
Abstract
Background:
Cranioplasty is a commonly performed reconstructive procedure to restore cranial integrity in patients with acquired skull defects after strokes, traumatic brain injury, and tumors, among other diagnoses. Given the procedure’s high complication rate and extensive perioperative planning, patient education is critical for informed decision-making. The American Medical Association (AMA) recommends that online patient education materials (OPEMs) be written at a sixth grade reading level to ensure equitable access to health information. Despite this, OPEMs for surgical interventions frequently exceed these recommendations. This study characterizes the readability and availability of English and Spanish-language OPEMs for cranioplasty.
Methods:
The top 20 English (“cranioplasty”) and Spanish (“craneoplastia”) OPEMs from Google searches were analyzed. English OPEMs were assessed using Flesch Reading Ease (FRE), Fry Graph (FG), Simple Measure of Gobbledygook (SMOG), and Gunning Fog Index (GFI). Spanish OPEMs were analyzed using Fernández-Huerta Reading Ease (FHRE), Gilliam-Peña-Mountain Grade Level (GPM), Spanish Orthographic Length (SOL), and Índice de Legibilidad de Flesch-Szigriszt (INFLESZ).
Results:
No OPEMs met the recommended sixth grade reading level. Among Spanish OPEMs, 55% (11) were written at the high school level and 45% (9) at a college level. Conversely, 35% (7) of English OPEMs were written at the high school level and 65% (13) at the college level. When adapted analog indices were compared across languages, Spanish OPEMs were on average easier to read than English OPEMs. No US healthcare institutions had Spanish OPEMs for cranioplasty and Spanish OPEMs were underrepresented among first-page search results (50%) relative to English OPEMs (70%).
Conclusions:
OPEMs for cranioplasty are written above recommended readability levels in both English and Spanish. Despite the United States’ large Spanish speaking patient population, no U.S. healthcare institutions currently have Spanish OPEMs for cranioplasty.
Introduction
Cranioplasty is a commonly performed reconstructive procedure used to restore cranial integrity in patients with acquired skull defects following stroke, traumatic brain injury (TBI), and other conditions.1,2 In addition to the procedure’s essential neuroprotective effects, cranioplasty plays a pivotal rehabilitative role in improving patients’ quality of life through correcting significant cranial deformities. 1 Despite its necessity, the procedure carries a disproportionately high complication rate, often cited between 15% and 40%.2,3 The procedure is further complicated by the wide range of available implant materials and the multidisciplinary care it requires across multiple surgical and rehabilitative specialties. 4 Consequently, patients undergoing cranioplasty must process and navigate large amounts of medical information throughout perioperative and recovery periods, underscoring the need for accessible and understandable health information.
Health literacy, according to the U.S. Department of Health and Human Services’ (HHS) Healthy People 2030 initiative, is defined as an individual’s ability to find, understand, and utilize information and services to make appropriate health-related decisions for themselves and others.5,6 In the United States, approximately 90 million individuals demonstrate limited health literacy and understanding of medical information. 7 Among patients receiving surgical care (perioperative to postoperative) across various surgical specialties, nearly one-third demonstrate limited health literacy, 8 which is associated with delays in seeking appropriate care, longer length of stay, increased post-acute care needs, poorer adherence to pre- and post-operative instructions, and psychological well-being.8-10 As a result of this increased utilization of healthcare resources, limited health literacy is estimated to add between 106 and 238 billion USD annually to U.S. healthcare costs. 8
Because patients often need to process complex medical information beyond clinical encounters, digital health technologies and online resources can be an effective way to improve health literacy among patients.11,12 Approximately 40% to 80% of medical information directly provided by healthcare practitioners is forgotten by patients after consultations. 13 As a result, online patient education materials (OPEMs) serve as an effective, widely accessible resource to improve health literacy, patient engagement, and overall health outcomes; utilized by approximately 58% of adults.14,15 To ensure equitable access to healthcare information, the American Medical Association (AMA) recommends that OPEMs be written at a sixth grade reading level.16,17 However, various studies have demonstrated that many existing surgical and medical OPEMs are written well beyond the suggested reading level,18,19 potentially widening the disparities in access to understandable medical information.
This concern is especially relevant for Spanish-speaking Hispanic populations in the United States, who represent the second-largest ethnic group, with 68 million people. 20 Hispanics in the US have lower rates of health literacy, especially among patients who preferentially speak Spanish,21,22 with approximately one-third reporting having limited English proficiency. 23 In this context, a lack of Spanish OPEMs and the high readability thresholds required to understand existing English and Spanish OPEMs can serve as a deterrent to online health information seeking among Hispanic populations, potentially worsening health outcomes.24-26 Thus, the primary objective of this study is to characterize the current state of the readability and accessibility of English and Spanish-language OPEMs for cranioplasty.
Methods
In this cross-sectional study, a Google search from a patient perspective using the single search terms “cranioplasty” (English) and “craneoplastia” (Spanish) were conducted on January 5th, 2026. Google Trends analysis comparing alternative search terms (“cirugía de reconstrucción craneal,” “reconstrucción del cráneo”) and English lay terms (“skull reconstruction,” “cranial reconstruction”) confirmed “craneoplastia” and “cranioplasty” as the highest-volume search terms over the past 5 years, supporting their selection for this study. The use of a procedure-specific medical term is also consistent with prior online surgical readability studies and is intended to approximate patient search behavior.27,28 To minimize personalization bias, all searches were performed in Google Chrome’s incognito mode with location services disabled and browser cache and cookies cleared. For the Spanish OPEM search, Google’s language settings were adjusted to Spanish (Estados Unidos), while the English OPEM search was conducted under English (United States) language settings.
Website Data Collection and Classification
Webpages were included for analysis if they were publicly accessible OPEMs related to cranioplasty and contained more than 100 words relevant text. Webpages were excluded if they were scientific articles, resources intended for healthcare providers, social media posts, or required paywall access. The first 20 eligible OPEMs webpage results were included in the readability analysis. OPEMs were further classified by author/source type (eg, hospital system, private clinic, health information platform, medical manufacturer, or other).
Readability Analysis
For each included webpage, relevant text was extracted and prepared for readability assessment using established document-cleaning procedures consistent with the CMS Toolkit for Making Written Material Clear and Effective 29 and the University of Arkansas for Medical Sciences (UAMS) Center for Health Literacy guidance. 30 English Language OPEMs were evaluated using the Flesch Reading Ease (FRE), Fry Graph (FG), Simple Measure of Gobbledygook (SMOG) Index, and Gunning Fog Index (GFI). FRE calculates readability on a 0 to 100 scale, with higher scores indicating easier readability, whereas FG, SMOG, and GFI generate grade-level estimates, with higher scores reflecting increased reading difficulty. Spanish-language webpages were analyzed using the Fernández-Huerta Reading Ease (FHRE; an adaptation of the English FRE test), Gilliam-Peña-Mountain Grade Level (GPM; an adaptation of the English FG test), and Spanish SMOG (SOL; an adaptation of the English SMOG Index), with the Índice de Legibilidad de Flesch-Szigriszt (INFLESZ) included as an additional Spanish readability measure. Each readability index incorporates objective text metrics, including word count, sentence length, character count, syllables per word, and number of complex words, to estimate reading difficulty. All readability analyses were performed using Readability Studio 2024 and an online readability tool (Legible). 31 The formulas for each readability index can be found in Supplemental Table 1. Statistical analyses were performed using Graphpad Prism 10 and were primarily descriptive. Comparisons across languages and source types were conducted descriptively using the analogous readability indices.
Results
To identify 20 English OPEMs for cranioplasty, the top 28 Google search results for the search term “cranioplasty” were analyzed. Of these, 8 webpages were excluded due to being scientific articles (5), social media content (1), content tailored to healthcare professionals (1), and having <100 words (1). The included OPEMs originated from a variety of sources, including hospital systems (9), private clinics (9), health information platforms (1) and Wikipedia (1). In contrast, reaching the same 20 Spanish OPEM threshold necessitated screening the first 47 Google search results. Of these, 27 webpages were excluded due to being scientific articles (14), social media content (7), content tailored to healthcare professionals (4), having <100 words (1), and being unrelated to cranioplasty (1). The included OPEMs originated from a multitude of sources ranging from health information platforms (9), hospital systems (1), private clinics (7), medical manufacturers (2), and Wikipedia (1) (Figure 1). Of the Spanish-language OPEMs, 6 originated from Mexico, 3 from Spain, 2 from Argentina and India, and 1 from Venezuela, Ecuador, Belgium, and South Korea. For 3 Spanish OPEMs, country of origin could not be determined from the website. Among the English-language OPEMs, 17 originated from the United States and 2 from the United Kingdom. Country of origin could not be determined for 1 English-language OPEM. Notably, no US healthcare institutions with a Spanish OPEM for cranioplasty were identified (Supplemental Figure 1).
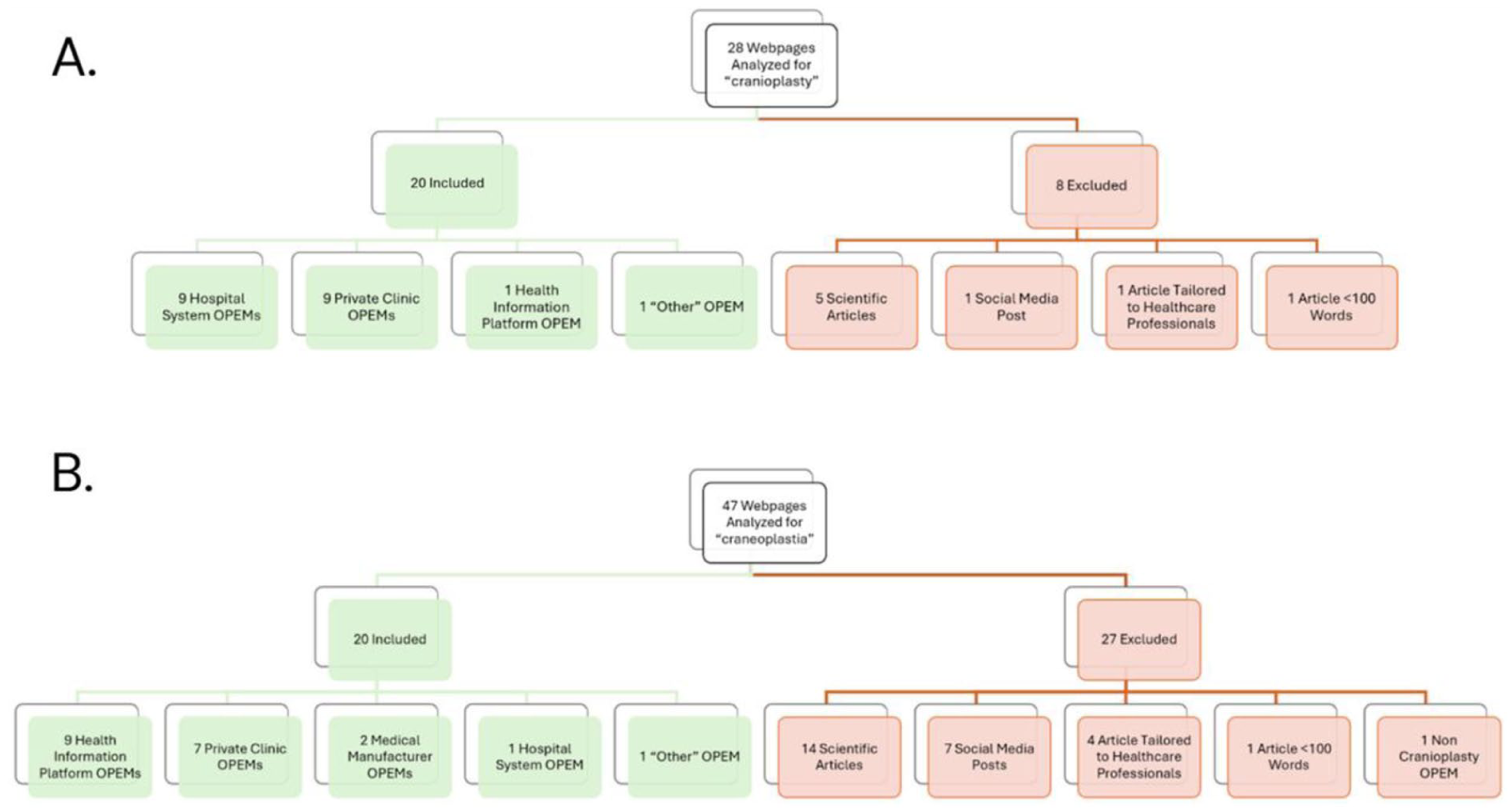
(A) Hierarchical flow chart depicting the webpages yielded from the English search term “cranioplasty” and (B) Hierarchical flow chart depicting the webpages yielded from the Spanish search term “craneoplastia.”
Among the first page of search results for craneoplastia returned by Google, only 5 online patient education materials (OPEMs) were identified. The remaining results included scientific articles (3), social media posts (1), and articles intended for healthcare professionals (1). In contrast, the first page of English-language search results yielded 7 OPEMs, with the remaining results consisting of scientific articles (2) and social media posts (1).
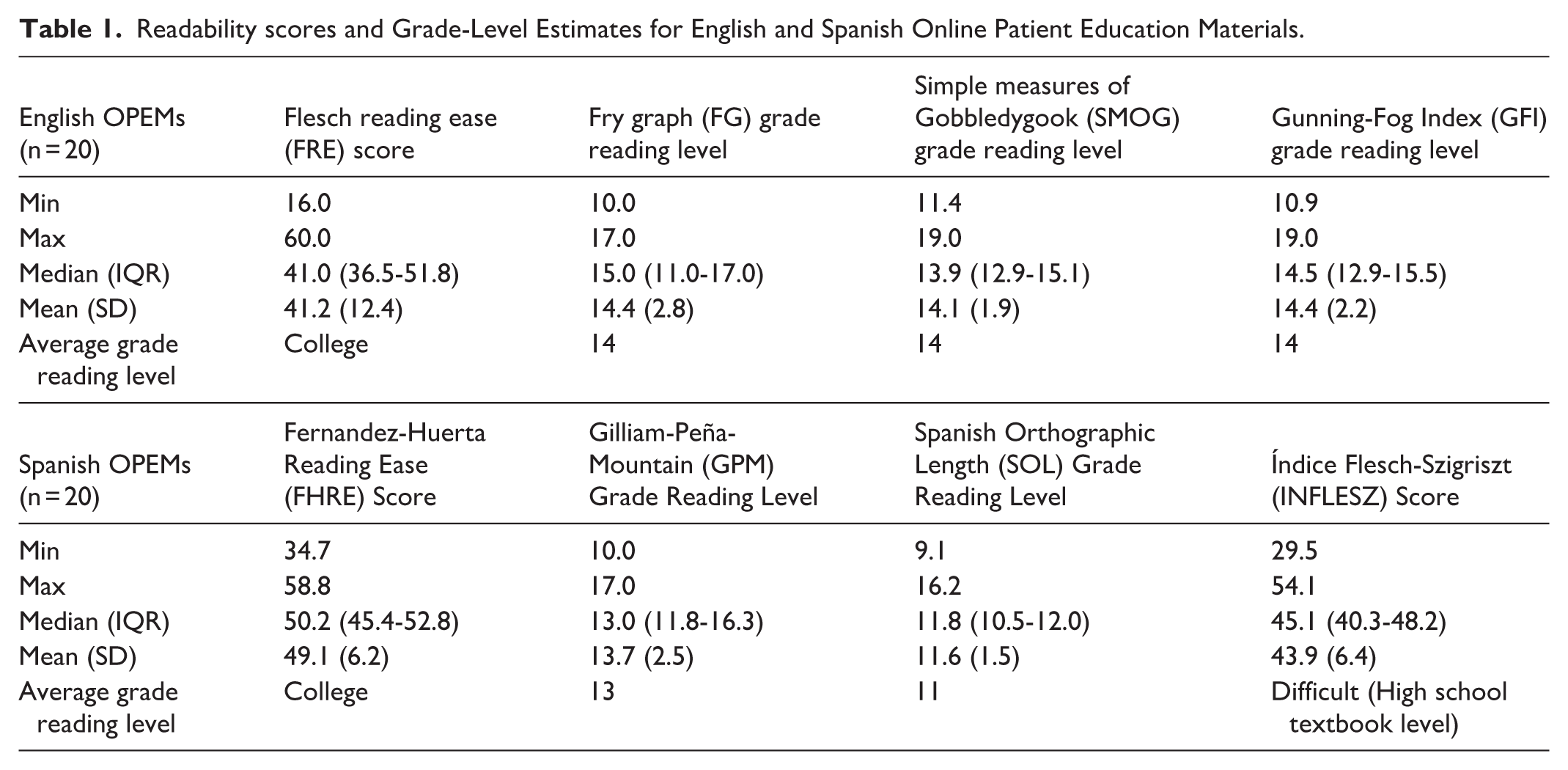
No English or Spanish OPEMs met the sixth-grade reading level recommendation. Among the English-language OPEMs, 5% (1) were written at a 9th to 10th grade level, 30% (6) at a 11th to 12th grade level, 20% (4) at a 13th to 14th reading level, and 45% (9) above the 15th grade level. Among the Spanish-language OPEMs, 20% (4) were written at a 9th to 10th grade level, 35% (7) at a 11th to 12th grade level, 40% (8) at a 13th to 14th reading level, and 5% (1) above the 15th grade level. Median readability metrics across all English and Spanish OPEMs demonstrated that materials were written well above recommended patient reading levels. For English OPEMs the median FRE score was 41.0 (IQR 36.5-51.8), corresponding to a college reading level. Median grade-level reading estimates were 15.0 (IQR 11.0-17.0) for the Fry Graph (FG), 13.9 (IQR 12.9-15.1) for SMOG, and 14.5 (IQR 12.9-15.5) for the Gunning-Fog Index (GFI). Spanish OPEMs demonstrated similar poor readability. The median Fernández-Huerta Reading Ease (FHRE) score was 50.2 (IQR 45.4-52.8), corresponding to a college reading level, while median grade-level reading estimates were 13.0 (IQR 11.8-16.3) for the Gilliam–Peña–Mountain (GPM), and 11.8 (IQR 10.5-12.0) for the Spanish Orthographic Length (SOL). The median INFLESZ score was 45.1 (IQR 40.3-48.2), corresponding to text written at the high school textbook level (Table 1).
Readability scores and Grade-Level Estimates for English and Spanish Online Patient Education Materials.
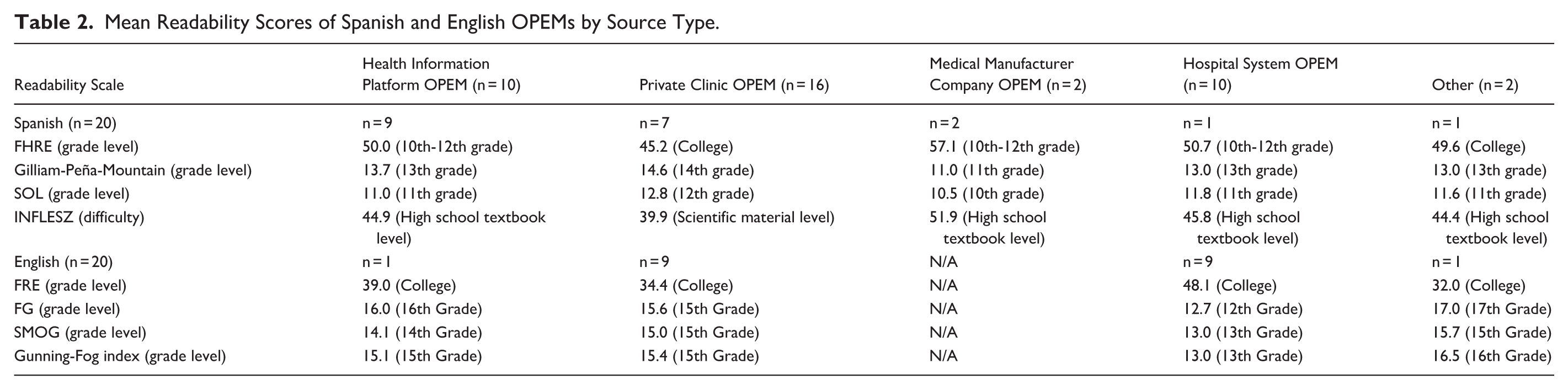
Among Spanish-language OPEMs, readability varied slightly across source categories, with private clinic materials (n = 7) demonstrating the highest average grade-level estimates (GPM 14.6;SOL 12.8), while medical manufacturer materials (n = 2) demonstrated the lowest average grade-level estimates (GPM 11.0; SOL 10.5). In contrast, among English-language OPEMs, private clinic materials (n = 9) had the highest average grade-level scores (FG 15.6; SMOG 15.0; GFI 15.4), while hospital system materials (n = 9) demonstrated lower average grade-level estimates (FG 12.7; SMOG 13.0; GFI 13.0; Figure 2; Table 2).
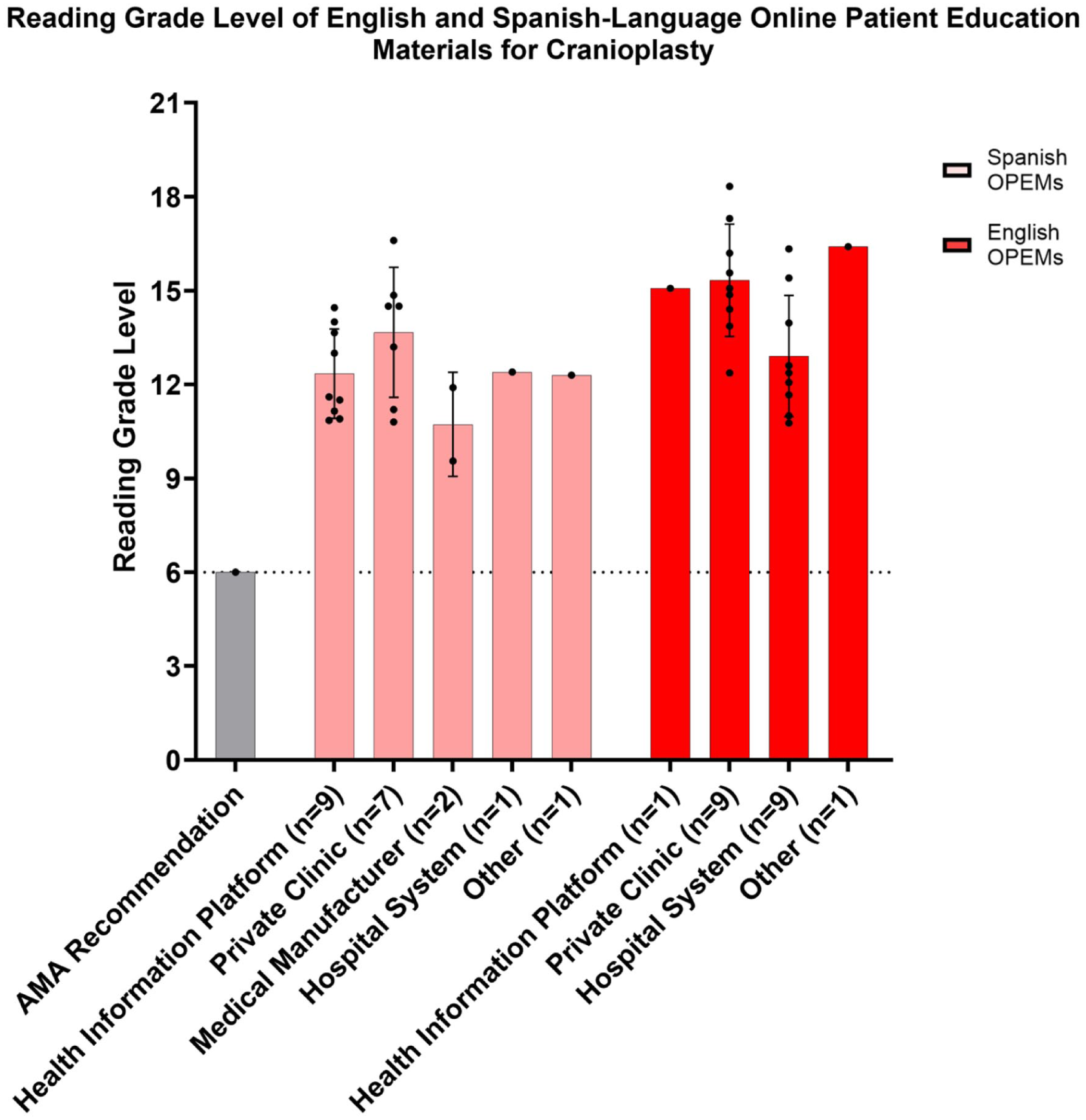
Reading grade level of Spanish and English-Language OPEMs for cranioplasty. The Spanish average grade level for each OPEM was calculated using the average of the Spanish Orthographic Length (SOL) and the Gilliam-Peña-Mountain (GPM) reading tests. The English average grade level for each OPEM was calculated using the average of the Fry Graph (FG), Simple Measures of Gobbledygook (SMOG), and Gunning-Fog Index (GFI).
Mean Readability Scores of Spanish and English OPEMs by Source Type.
Exploratory cross-language comparison across all analogous readability indices suggested that Spanish-language OPEMs may be easier to read than English-language materials, as reflected by lower Spanish grade-level scores for the SOL/SMOG pairing (11.6 vs 14.1) and GPM/FG pairing (13.7 vs 14.4), and higher readability ease scores for the FHRE/FRE pairing (49.1 vs 41.2; Figures 3 and 4).
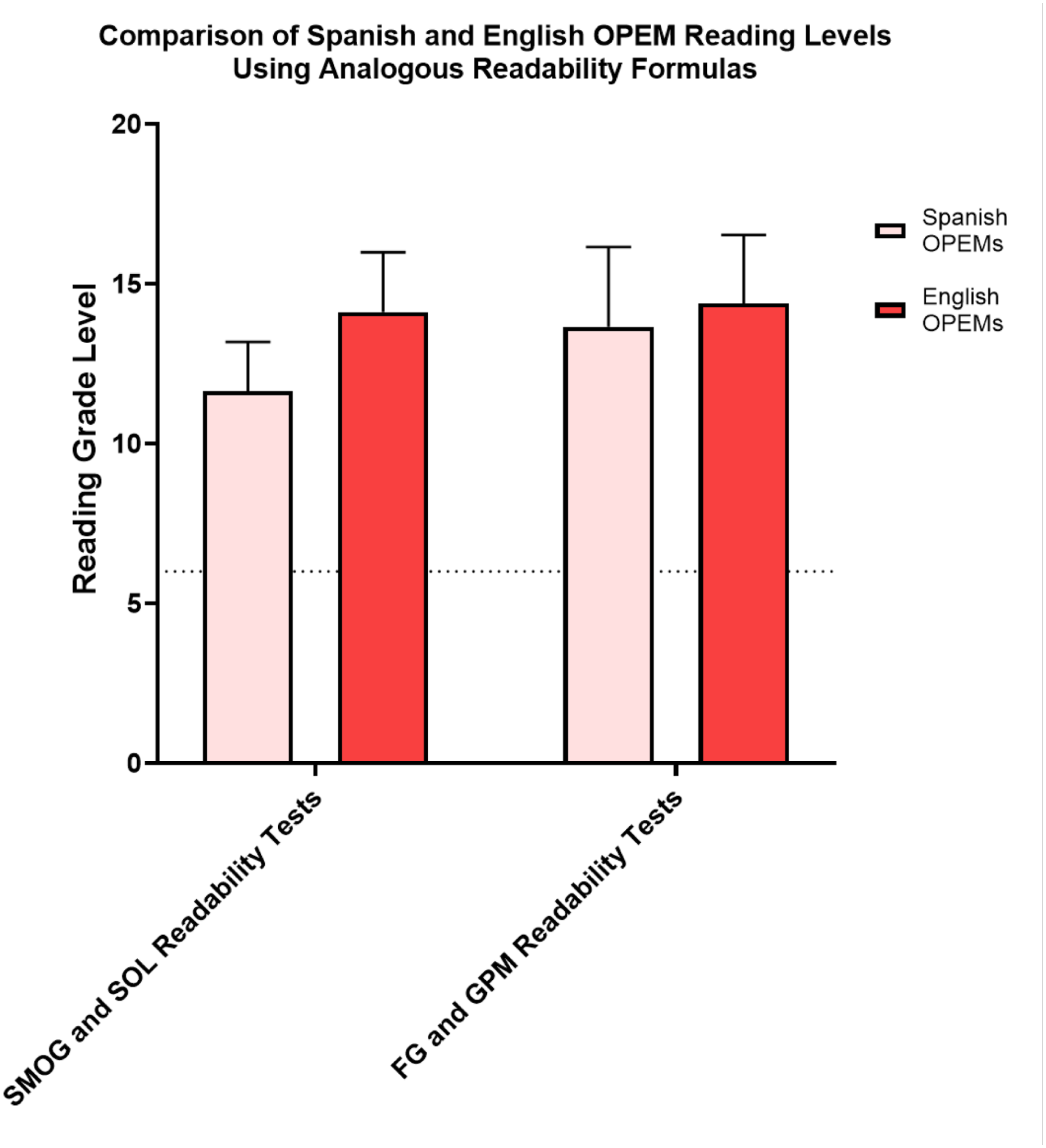
Descriptive comparison of Spanish and English OPEM reading grade levels using analogous readability indices (Spanish SOL vs English SMOG; Spanish GPM vs English FG).
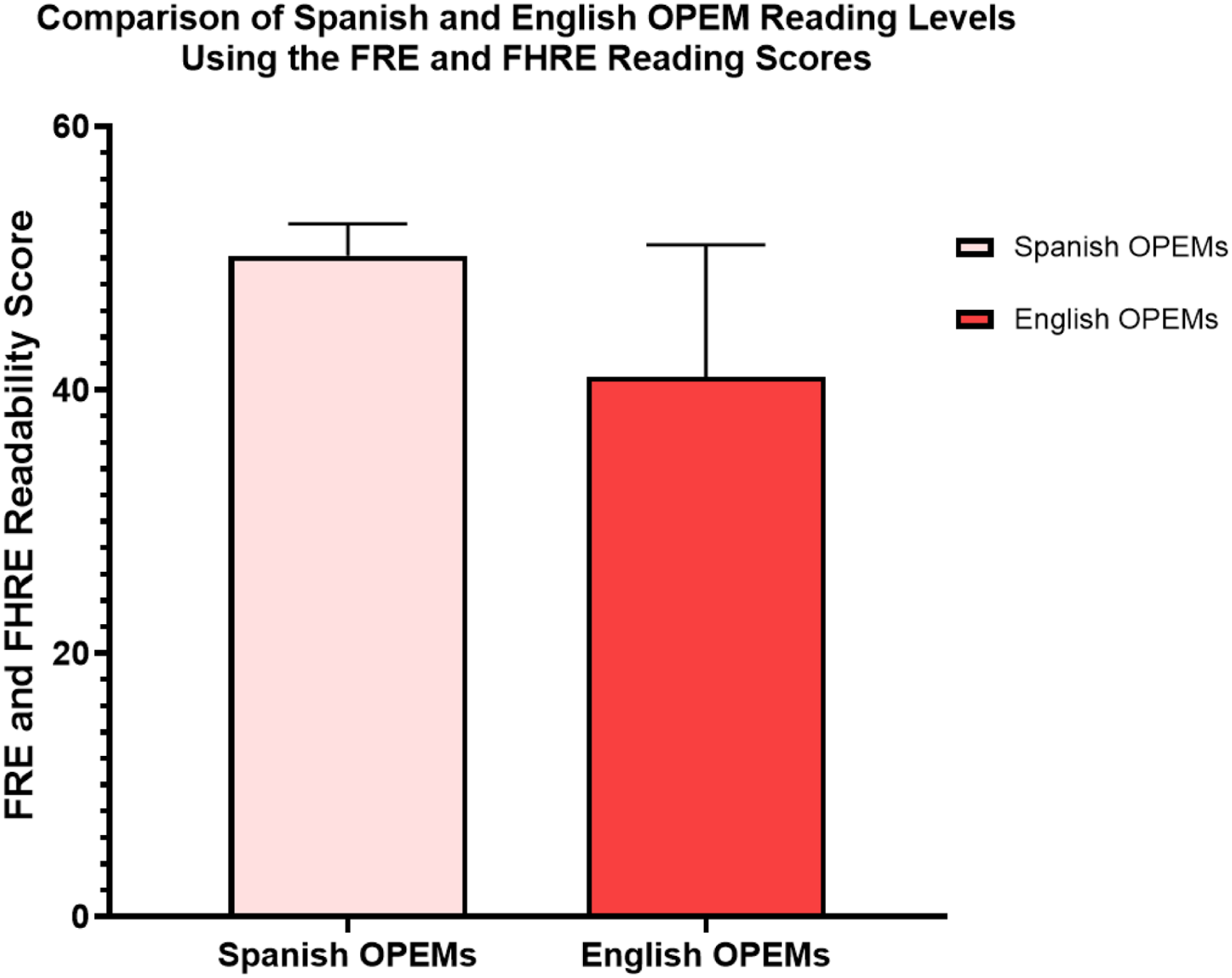
Descriptive comparison of Spanish and English OPEM readability ease scores using analogous readability indices (Spanish FHRE vs English FRE).
Discussion
In this cross-sectional analysis, our findings revealed that all English- and Spanish-language OPEMs for cranioplasty were written well above recommended readability thresholds, with no materials meeting the AMA’s suggested 6th grade reading level. 16 Readability analysis across multiple validated indices revealed that the existing English OPEMs for cranioplasty require a college reading level for comprehension, whereas Spanish OPEMs require a marginally lower, late high school level of literacy. Resources across both languages far exceed the average U.S. adult 7th to 8th grade reading level32,33 and are of particular concern based on national modeled estimates from the U.S. Department of Education suggesting that approximately 54% of U.S. adults read below a sixth grade reading level. 34 In addition to readability barriers, we identified a significant relative scarcity of Spanish-language online patient resources for cranioplasty. To obtain 20 Spanish OPEMs for analysis, 47 Google search results spanning the first 5 search result pages had to be screened. This is nearly double the 28 results screened to identify 20 English OPEMs, reflecting the lower overall availability of Spanish OPEMs for cranioplasty. This disparity was also evident within the first page of search results, where only 5 of the top 10 Spanish results for “craneoplastia” led to relevant OPEMs, compared with the English first page search that yielded 7 OPEMs. The relative scarcity of Spanish OPEMs may therefore preclude this population from accessing online educational materials, especially given that studies of web search behavior consistently find that over 97 % of all clicks occurred on results on the first page of search outputs. 35 Underscoring this, not a single U.S. healthcare institution was found to have a Spanish-language cranioplasty OPEM. This is of particular concern given the large and growing Spanish speaking population in the United States, where Spanish speakers represent the second-most spoken language in the U.S. and is spoken at home by 12.8% of all residents. 36 Coupled with the high clinical volume of cranioplasties in plastic and neurosurgical practices, the absence and poor visibility of Spanish-language resources may ultimately exacerbate existing health literacy issues within the Hispanic and Spanish-speaking population. Taken together, these findings highlight the significant digital barrier experienced by Spanish-speaking patients in accessing health information related to cranioplasty.
These findings are not limited to OPEMs for cranioplasty and fall in line with broader patterns of plastic surgery patients’ education materials being written well above recommended levels.27,28,37-39 For example, abdominoplasty and rhinoplasty English patient resources were found to average roughly 12th grade readability,27,28 while hand surgery and gynecomastia materials were observed to be written at around the 10th to 11th grade level.40,41 Similarly, there is a growing body of work analyzing issues in Spanish-language plastic and reconstructive surgery education materials.42-44 At the specialty-society level, Sathyanarayanan et al 44 reported that national plastic and reconstructive surgery organization websites frequently exceeded readability guidelines and lacked Spanish representation. It was found that both American Society of Aesthetic Plastic Surgeons (ASAPS) and American Society of Reconstructive Microsurgeons (ASRM) websites provided no Spanish educational materials, whereas over 92% of American Society of Plastic Surgeons (ASPS) materials were written in English. Similar to our findings, Spanish OPEMs from the ASPS websites were easier to read than the English OPEMs but were characterized by a significant lack of availability. This trend persists in procedure specific educational materials, where Doval et al 45 similarly reported a paucity of breast reconstruction Spanish OPEMs from US institutional and academic centers. Unsurprisingly, these findings were observed to transcend procedural educational materials, with Blount et al’s 46 evaluation of Spanish and English resources related to breast reduction insurance coverage identifying persistent readability barriers, underscoring more broad health-literacy implications for the Spanish-speaking population.
With the rapid expansion of internet access and advances in artificial intelligence, patients are increasingly turning to online resources to better understand their diagnoses and surgical options. 47
In this ever-evolving landscape, OPEMs serve a critical function: to provide accurate, accessible and procedure-specific information that supports informed consent, reinforces perioperative counseling, and promotes shared decision-making. High-quality OPEMs can not only explain indications, risks, benefits, and alternatives to surgery, but also guide patients through pre- and post-operative care in a manner that is understandable and actionable. 48 The need for effective OPEMs is underscored by robust evidence demonstrating that patients retain only a small fraction of the information delivered during clinical encounters. One study suggests that patients remember as little as 14% of medical information provided orally by physicians, 13 and recall is further diminished when patients are anxious, or confronted with complex surgical terminology. Effective OPEMs allow patients to revisit information at their own pace and clarify misunderstandings after the clinical encounter. Previous studies have shown that well-designed educational materials can improve adherence to postoperative instructions, enhance patient satisfaction, and improve quality-of-life outcomes.8-10,49 For patients with limited baseline health literacy, OPEMs may be especially impactful by reinforcing surgeon-delivered teaching and strengthening comprehension across the perioperative continuum. 50
Importantly, the quality and accessibility of language-specific OPEMs have direct implications for health equity. More than 20% of Americans speak a language other than English at home. 36 The Hispanic population, one of the largest and fastest-growing ethnic minority groups in the United States, is projected to comprise 28.6% of the population by 2060 and has among the lowest health literacy. 51 Inadequate availability of Spanish-language OPEMs, or materials written above recommended reading levels, risks amplifying existing disparities in comprehension, informed consent, and postoperative adherence. Given that health literacy is closely linked to patient satisfaction, complication rates, and hospital readmissions, inequities in OPEMs are likely to contribute to broader structural disparities in surgical care. Expanding the availability, cultural appropriateness, and readability of both English- and Spanish-language OPEMs represent a tangible opportunity to reduce these gaps.
Surgeons and healthcare institutions therefore share responsibility in shaping the arc of health literacy through the development of equitable, evidence-based OPEMs. However, improving readability must not come at the expense of medical accuracy. The challenge lies in balancing the feasibility of understanding with precision that ensures the nuance clinical details are conveyed in the AMA recommended grade reading levels. Emerging technologies offer additional opportunities for improvement. Notably, large language models such as ChatGPT have demonstrated early promise in generating patient-facing education content and enhancing readability in various specialties including dermatologic conditions and aortic stenosis OPEMs.52,53 When used judiciously and with professional oversight, artificial intelligence can streamline the creation of linguistically and grade-level appropriate reading materials in both English and Spanish. OPEMs represent a practical and scalable strategy to strengthen shared decision-making, enhance perioperative education, and promote equitable surgical care. By prioritizing readability and language accessibility, healthcare systems can transform patients from passive recipients of information into informed and engaged participants in their surgical care.
Our study is not without limitations. Firstly, our analysis focused on text-based readability indices and therefore did not account for alternative methods of communicating health information, such as images, diagrams, videos, interviews, or other multimedia components that may promote comprehension. Additionally, it must be acknowledged that commonly used readability indices frequently rely on proxies such as syllable count and word length. This may cause readability scores to be inflated due to the inherent complexity of medical terminology that may be necessary for patient understanding. Finally, OPEMs only represent one component of a broader list of resources used by patients to build health literacy. Patients may similarly rely on in-person medical counseling, printed handouts, and other educational materials provided by surgeons and healthcare teams during medical appointments.
Although Google Trends analysis supported the selection of “cranioplasty” and “craneoplastia” as the highest-volume search terms, patients may also search using lay terminology, which could yield different OPEMs not captured in the present study. In addition, our analysis was limited to Google, which despite accounting for 90% of global search engine usage, 54 does not capture all web-based health information. Future studies may incorporate multiple search engines, additional search terms, and repeated search dates to improve generalizability.
Conclusion
Although Spanish OPEMs were written at significantly lower reading levels than English OPEMs, all identified Spanish and English educational materials for cranioplasty well-exceeded the AMA’s recommended sixth grade reading level. Despite the United States’ large and growing Spanish speaking patient population, no U.S. healthcare institutions have Spanish OPEMs for cranioplasty. Spanish OPEMs also demonstrated lower overall availability and visibility in top search results compared to English OPEMs. To prevent worsening health literacy disparities and promote informed consent, healthcare institutions must prioritize the creation and revision of both Spanish and English OPEMs that adhere to AMA readability guidelines.
Supplemental Material
sj-docx-1-fac-10.1177_27325016261459568 – Supplemental material for Readability and Availability of English and Spanish Online Patient Education Materials for Cranioplasty
Supplemental material, sj-docx-1-fac-10.1177_27325016261459568 for Readability and Availability of English and Spanish Online Patient Education Materials for Cranioplasty by Satyam K. Singh, Alfred Wong, Amar Sahota, Junaid Ali and Kerry-Ann Mitchell in FACE
Footnotes
Acknowledgements
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Author Contributions
Conceptualization, S.K.S.; methodology, S.K.S and A.W.; project administration, S.K.S.; writing—original draft preparation, S.K.S., A.W., A.S., and J.A.; writing—review and editing, K.M.; supervision, K.M.; resources, S.K.S.; data curation, S.K.S., A.W., A.S., and J.A.; formal analysis, S.K.S.; All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All datasets, statistical outputs, and materials utilized in this study can be obtained upon reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.