
Abstract
Orbital fractures are among the most common forms of craniofacial trauma and present significant diagnostic and therapeutic challenges because of the orbit’s complex anatomy and the potential for long-term functional and aesthetic sequelae. This review synthesizes current evidence regarding the evaluation, imaging, management, and complications of orbital fractures, with emphasis on evolving treatment paradigms and ongoing areas of controversy. A PubMed® literature review was conducted using search terms related to orbital fracture anatomy, physical examination, imaging, conservative management, surgical intervention, antibiotics, and complications, with emphasis placed on contemporary studies. Clinical assessment remains central to management, particularly evaluation of visual acuity, globe position, ocular motility, diplopia, and infraorbital sensation, while high-resolution computed tomography continues to represent the diagnostic gold standard for characterization of fracture morphology, soft tissue herniation, and muscle entrapment. Current evidence increasingly supports selective rather than routine operative intervention, emphasizing functional deficits such as persistent diplopia, clinically significant enophthalmos, extraocular muscle entrapment, and vision-threatening complications over fracture size alone. Urgent repair remains indicated in cases of oculocardiac reflex, orbital compartment syndrome, or pediatric trapdoor fractures. Advances in transconjunctival approaches, image-guided navigation, biomaterials, and patient-specific implants have improved reconstructive precision and reduced postoperative morbidity, although controversy persists regarding operative timing, implant selection, and the routine use of prophylactic antibiotics for fractures communicating with the paranasal sinuses. Postoperative complications, including diplopia, infraorbital nerve dysfunction, retrobulbar hematoma, eyelid malposition, enophthalmos, and implant-related morbidity, continue to influence clinical outcomes despite advances in care. Overall, contemporary management increasingly favors an individualized, multidisciplinary, and evidence-based approach tailored to patient symptoms and functional outcomes, while future prospective studies with standardized outcome measures are needed to clarify unresolved management questions and establish more consistent treatment algorithms for orbital trauma.
Introduction
The orbit is a complex, 3-dimensional structure, often described as pear-shaped with the optic nerve forming the stem. The bony orbit contains the globe, nerves, vessels, lacrimal gland, extraocular muscles, tendons, fat, and connective tissue. 1 It is composed of 7 bones, arranged into 4 walls. The orbital floor consists of the maxillary, zygomatic, and palatine bones. The medial wall is formed by the frontal process of the maxilla, lacrimal bone, orbital plate of the ethmoid bone (lamina papyracea), and sphenoid body. 2 The lateral orbital wall is comprised of the zygomatic bone and greater wing of the sphenoid, while the orbital roof is formed by the orbital plate of the frontal bone and the lesser wing of the sphenoid. 1
The orbit’s location and lack of protective soft tissue make it susceptible to traumatic injury. Fractures can involve any orbital wall, with an orbital blowout fracture referring to a fracture of an orbital wall with an intact orbital rim. 3 Common causes of orbital fractures include blunt trauma from physical assault, mechanical falls, motor vehicle collisions, sports injuries, and occupational accidents, with the most frequent mechanism varying across demographic groups. 4 Isolated orbital fractures account for 4% to 16% of all facial fractures, whereas orbital involvement is seen in 30% to 40% of facial fractures.3,5,6 The incidence of orbital fractures has been increasing in recent years and is more common in men than in women, most frequently occurring in the second and third decades of life.3,7-10 From 2006 to 2017, the incidence of orbital floor fractures rose by 47%. During this period, assault remained the most frequent mechanism and increased only modestly, whereas fractures resulting from falls more than doubled. Because falls occur disproportionately in older adults, one proposed explanation for this rise is the concomitant growth of the population aged at least 65 years. 10 A more recent analysis of National Electronic Injury Surveillance System data from 2013 to 2022 similarly demonstrated increasing orbital trauma rates across all age groups, with the steepest growth observed in elderly adults who were most often injured by household or fall-related mechanisms. 11 Together, these data suggest that demographic shifts and fall-related mechanisms are major contributors to the rising incidence of orbital fractures, underscoring the growing need for targeted safety and prevention efforts in elderly populations.
The primary goals of orbital fracture management are to restore orbital contour and volume and to correct any functional deficits in a safe and effective way.12,13 Despite extensive research on orbital trauma, significant variability remains in how patients are evaluated and managed, including differences in assessment, indications and timing for surgical repair, and the prediction and prevention of postoperative complications. Existing reviews often emphasize isolated aspects of orbital trauma, but few integrate recent evidence across workup, treatment strategies, and complication profiles. This review aims to synthesize current data in these areas to clarify unresolved questions and support consistent, evidence-based clinical decision-making.
Methods
A review of publications related to orbital fractures was conducted via a PubMed® search of “orbital fracture AND (anatomy OR physical examination OR imaging OR conservative management OR surgical intervention OR antibiotics OR complications).” Due to the return of thousands of articles, titles were sorted by date, more recent first, and then screened based on relevant terminology. Once information became overly repetitive, review was halted. Conflicting evidence was evaluated individually and all aspects incorporated with comment on strength of support. Additional studies were pulled as necessary from in-text citations.
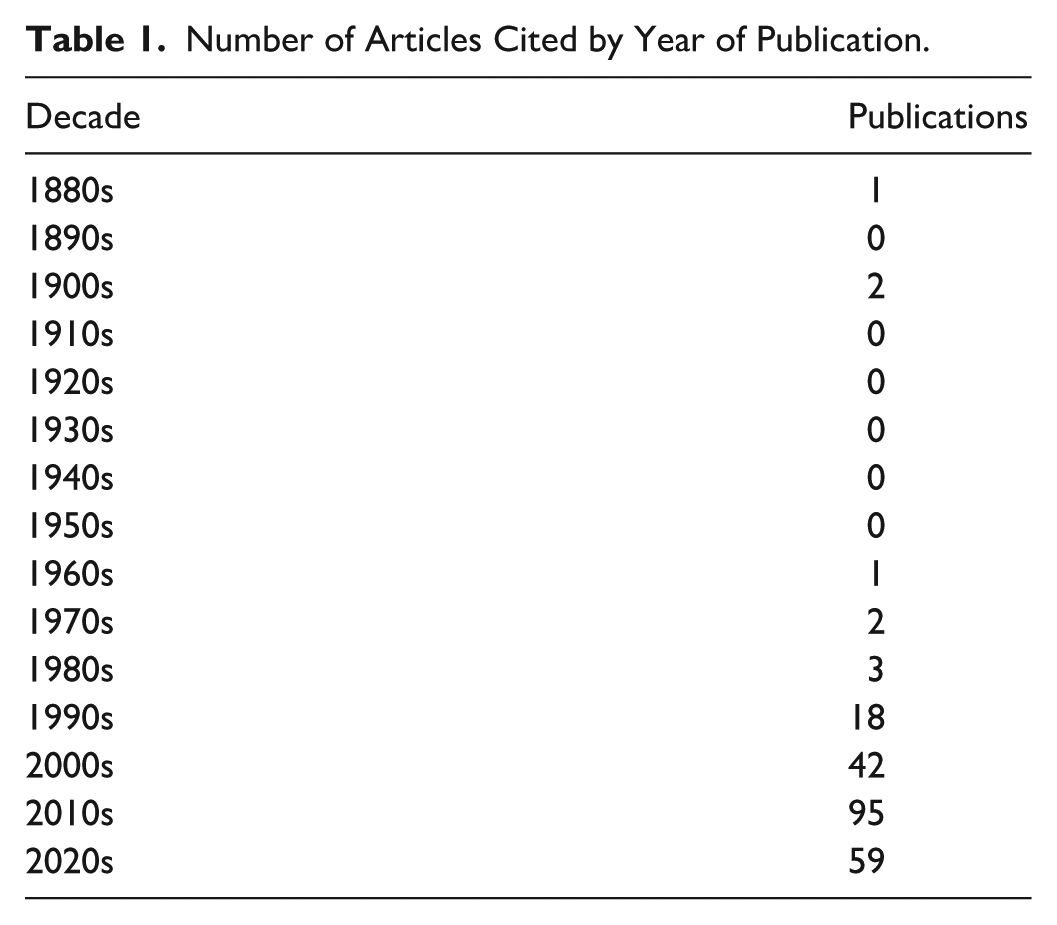
Publication years for articles cited ranged from 1886 to 2025, with the majority coming after 2020 (Table 1). Older articles were only used in instances of historical significance or high citation rates.
Number of Articles Cited by Year of Publication.
Workup
Physical Examination
A thorough physical examination is essential in evaluating suspected orbital fractures, guiding imaging decisions, and establishing the urgency of management. Key elements include visual inspection, globe measurements, palpation, assessment of ocular motility, acuity analysis, and sensory testing.
Inspection may reveal characteristic signs such as periorbital ecchymosis, eyelid swelling, and hematoma—common indicators of orbital trauma.14,15 Subconjunctival hemorrhage is frequently observed; while often benign, it can obscure more serious underlying pathology.16-19 A complete ophthalmologic examination should be performed, including evaluation of the anterior chamber for hyphema and dilated fundus examination of the retina to assess for associated intraocular injury, which may necessitate urgent ophthalmic intervention, medical management, and/or delay of operative fracture repair depending on severity and risk of visual compromise.20,21 Patients should also be assessed for superior orbital fissure syndrome (involvement of cranial nerves III, IV, V1, and VI), which may present with ophthalmoplegia, ptosis, diplopia, and loss of corneal sensation, often accompanied by pain and sensory deficits in the upper face.22-24
Globe positioning, analyzed relatively between sides, is a fundamental aspect of the exam. 25 Enophthalmos, reflecting posterior displacement of the globe, typically suggests disruption of the orbital floor or medial wall.26,27 Conversely, exophthalmos, or protrusion of the globe, may signal retrobulbar hemorrhage or the presence of orbital emphysema.28-30 A difference greater than 2 mm between eyes is associated with clinical significance.26-30 To calculate globe position, one can use an exophthalmometer, such as that created by Hertel, which measures the distance from the lateral orbital rim to corneal surface, 31 or by Naugle, which uses the superior and inferior orbital rims as reference. 32 Gross examination, in which the patient tilts the head backward and the examiner looks through a worm’s-eye view, is nevertheless the preferred method to these devices in the emergency setting due to ease and quickness. 33 Although interpretation of exophthalmometry is limited when baseline positions are unknown, repeat measurements are telling of pathological progression. 34 Intraocular pressure should also be measured with a tonometer when globe rupture has been excluded, as elevated pressure may indicate orbital compartment syndrome or retrobulbar hemorrhage requiring urgent intervention.35-38
Palpation of the orbital rim and zygomatic arch can uncover step-offs or crepitus, pointing toward fractures involving the orbital floor or the zygomaticomaxillary complex. 39 Facial asymmetry and deformities of the infraorbital rim are also important findings.40-42 The presence of crepitus and periorbital emphysema should raise concern for communication with the paranasal sinuses, supporting the suspicion of a floor or medial wall defect.43-45
Evaluating extraocular movement is a critical component of the exam.46,47 Forced duction, in which topical anesthetic is applied to the eye followed by passive movement of the conjunctiva with forceps, can distinguish between paresis and mechanical restriction. 48 Restriction in upward gaze often reflects entrapment of the inferior rectus muscle or orbital fat herniation through a blowout fracture.49-51 Vertical diplopia is a classic indicator of muscle entrapment and should prompt urgent imaging and possible surgical referral. 52
Visual acuity must be assessed in all patients to identify potential optic neuropathy or globe injury.53-55 A relative afferent pupillary defect may signal optic nerve involvement. 53 Pupil asymmetry or reactivity abnormalities could indicate intraocular trauma or globe rupture. 55 Hirschberg was the first to describe a corneal light reflect test to check for ocular alignment, whereby the examiner shines a light source into the eyes and observes if reflection location is equal. 56
Finally, sensory testing over the infraorbital nerve distribution, including the cheek, upper lip, and upper gingiva, can reveal hypesthesia or anesthesia.57-60 These findings are frequently associated with orbital floor fractures involving the infraorbital canal, but can be due to swelling, meaning that a well-documented baseline to track recovery is crucial.61,62
Given the often subtle nature of some presentations, a high index of suspicion should be maintained. While clinical findings can strongly suggest the presence of an orbital fracture, definitive assessment requires imaging, most commonly high-resolution computed tomography (CT), to delineate the full extent and complexity of the injury.
Imaging
Imaging is central to confirming the diagnosis and characterizing the severity of orbital fractures. While the physical exam provides initial direction, high-resolution CT remains the imaging modality of choice due to its superior ability to define both bony and soft tissue anatomy.
CT scans offer fine detail that allows for precise evaluation of orbital walls, extraocular muscles, and potential globe or intracranial injury.63-65 Thin-slice axial and coronal images are particularly effective in identifying fractures of the orbital floor and medial wall—the most commonly affected areas. 66 Coronal reconstructions are especially valuable in detecting so-called trapdoor fractures that potentially incarcerate orbital contents.67,68 This pattern is more frequently seen in pediatric patients.69-71
CT can reveal signs of increased orbital volume, such as herniation of fat or muscle, and may demonstrate orbital emphysema, an indicator of communication with adjacent sinuses.64,72-75 Other findings such as extraocular muscle entrapment, retrobulbar hemorrhage, and optic canal involvement are critical for determining the need for urgent surgical intervention.74,76-78 In “pure” blowout fractures, where the internal orbital wall is affected without rim involvement, CT can help distinguish isolated orbital injuries from more complex midfacial trauma.79-81 Entrapment of the inferior or medial rectus muscles may be visualized directly or inferred through changes in contour, fat stranding, or displacement of adjacent structures.49,82,83
Three-dimensional reconstructions derived from CT data are increasingly used for complex cases when multiple and/or comminuted fractures significantly distort normal anatomy.84-88 They can enhance preoperative planning and provide valuable intraoperative reference in reconstruction procedures.89-91
Magnetic resonance imaging has a limited role in the acute setting due to suboptimal bone resolution and susceptibility to motion artifact.73,74,92-94 Nonetheless, it may be useful when optic nerve injury, muscle ischemia, or vascular complications such as carotid-cavernous fistula are suspected but not clearly identified on CT. 95 Traditional radiographs are now largely obsolete due to their poor sensitivity and limited diagnostic utility. 75 Ultrasound can serve as a cost-effective alternative with the added advantage of no radiation exposure.96-98 Regardless, these modalities serve minimal functions in acute evaluation.
Clinical guidelines consistently support early CT evaluation in any patient with signs of orbital trauma, particularly when diplopia, globe injury, decreased vision, enophthalmos, or periorbital emphysema are present. Early imaging ensures appropriate triage and expedites surgical referral when necessary.
Treatment
Conservative Management
While certain orbital fractures require surgical repair, many cases can be managed conservatively with close monitoring and supportive care. Non-operative management is typically appropriate in the absence of clinical features such as extraocular muscle entrapment, significant bony displacement, enophthalmos exceeding 2 mm, persistent diplopia in primary gaze, evidence of globe or optic nerve injury, or involvement of more than half of the orbital floor.58,59,77,99-109 There is, however, some discrepancy between ophthalmology and plastic surgery standards in that plastic surgeons generally intervene early for enophthalmos and large bony defects.110-112
Patients managed conservatively should be followed closely to detect delayed complications, including diplopia, enophthalmos, or restrictions in ocular motility.69,113-115 Re-evaluation is often recommended within 7 to 10 days, as initial swelling may mask symptoms that become more apparent with time.77,104,116-118 Follow-up examinations should include reassessment of visual acuity, globe position, and ocular alignment.55,113,119,120 Serial photography and exophthalmometry can be helpful for documenting changes in globe position over time.71,90,121,122
Symptom management plays a key role in conservative care.123,124 Cold compresses during the first 48 hours can help reduce swelling, and head elevation may further alleviate periorbital edema. 30 Pain is typically managed with acetaminophen or nonsteroidal anti-inflammatory drugs, although the latter should be used cautiously in patients with associated hemorrhage.123-127 Short-term nasal decongestants may be beneficial, especially in medial wall or floor fractures, to reduce sinus congestion and the risk of secondary infection.58,128-130 Importantly, patients should be instructed to avoid nose blowing for at least 10 to 14 days to prevent retrograde air insufflation into the orbit, which could lead to orbital emphysema.28,131-134 Activity modification is also important.78,124,125,129 Patients should avoid strenuous exertion, heavy lifting, and contact sports for 4 to 6 weeks.77,124 Air travel may be contraindicated in the presence of orbital emphysema, given the potential for gas expansion at altitude.131,134-137 Protective eyewear is advisable during recovery to prevent further injury.138,139
Most patients with small, non-displaced orbital fractures recover well without surgery. Many regain their premorbid statuses if medical recommendations are adhered to. However, a subset may require delayed surgical correction if functional or cosmetic issues persist.
Surgical Intervention
Surgical management is indicated when an orbital fracture is expected to result in functional impairment or significant cosmetic deformity. The decision to operate is based on clinical findings, imaging results, and patient-specific factors. Timing is carefully considered, balancing the need for urgent intervention against the benefits of delayed reconstruction once edema has subsided.
Urgent surgery, typically within 24 to 48 hours, is reserved for high-risk cases that would otherwise result in long-term visual impairment and possible hemodynamic instability.107,108 Entrapment of extraocular muscles, particularly the inferior or medial rectus, may result in ischemia and dysfunction if not promptly addressed.99,102,103,105,109 The presence of an oculocardiac reflex, manifested by bradycardia, nausea, vomiting, or syncope, further underscores the need for immediate surgical release. 101 Similarly, elevated intraocular pressure concerning for orbital compartment syndrome constitutes an ophthalmologic emergency and may necessitate immediate lateral canthotomy and cantholysis to prevent irreversible vision loss.35,140-142 These examination findings—particularly marked motility restriction with pain and a positive forced duction test—serve as key decision points in contemporary management algorithms, prompting urgent operative intervention regardless of fracture size or radiographic appearance.124,125,143,144
Delayed surgical repair, usually performed within 1 to 2 weeks, is appropriate in cases of persistent diplopia (especially in primary gaze) or enophthalmos greater than 2 mm.58,77,100,104,106 Fractures involving more than 50% of the orbital floor or those with defects larger than 2 cm2 are also more likely to result in late enophthalmos and hypoglobus and are often treated surgically to prevent progressive deformity.58,59 Nevertheless, more recent studies claim that defects of 1 to 2 cm2 necessitate surgery,145,146 whereas other evidence has found that even large fractures do not cause late sequelae. 147 Accordingly, a strategy of careful observation with delayed repair only if clinically significant enophthalmos develops has gained acceptance, challenging the older dogma of routine early intervention solely to prevent a theoretical future deformity.124,148
Surgical approach is selected based on fracture location, surgeon expertise, and the need to preserve cosmesis.149-152 The transconjunctival approach is frequently preferred for its minimal external scarring and excellent exposure of the orbital floor and medial wall.153-156 It also has the advantage of being readily combined with a transcaruncular incision to allow simultaneous access for reconstruction. 157 Subciliary and subtarsal incisions provide good visualization but carry higher risks of complications such as scleral show and ectropion, particularly in older patients.158-160 Endoscopic endonasal techniques offer a minimally invasive alternative for medial wall fractures and allow concurrent management of sinonasal pathology, though they require specialized training and instrumentation.161-163
Implant selection is a critical part of the reconstructive process.124,164-167 Autologous grafts, such as bone or cartilage, which are chosen based on fracture location and pattern to best match pre-injury structure, provide excellent biocompatibility but are limited by donor site morbidity and variability in shape.168-171 As a result, alloplastic materials are more commonly used.171-175 Titanium mesh remains a widely favored option due to its strength, flexibility, and compatibility with image-guided navigation systems.176-179 Porous polyethylene offers easy handling, soft tissue integration, and a low rate of complications.180-184 In growing pediatric patients, implant choice is particularly influenced by future skeletal development, with a preference for resorbable plates to avoid growth restriction or distortion, whereas autologous grafts may also be selected depending on defect characteristics and reconstructive needs.185,186 Resorbable materials like poly-L-lactic acid or polydioxanone sheeting may be suitable for small defects or children, though their structural support is limited over time.174,187 Emerging technologies such as patient-specific implants derived from preoperative CT data have shown promising results in complex or revision cases, offering precise anatomical restoration and improved surgical outcomes.167,188,189
Ultimately, surgical success depends on careful case selection, proper timing, and an individualized approach to technique, which may include intraoperative image guidance, and implant use. When performed appropriately, orbital fracture repair can restore function and appearance with excellent long-term results.
Antibiotics
The role of prophylactic antibiotics in orbital fractures remains a subject of ongoing debate. Fractures involving the orbital floor or medial wall may create direct communication between the orbit and paranasal sinuses, raising theoretical concerns for retrograde infection, including orbital cellulitis or abscess formation. While many clinicians prescribe antibiotics in this context, high-level evidence to support routine use is limited.190-194
The most commonly cited rationale for antibiotic prophylaxis is to prevent bacterial translocation from the sinuses, particularly in fractures that disrupt the lamina papyracea or involve maxillary sinus mucosa.192,193 Amoxicillin-clavulanate is often recommended as first-line therapy due to its broad spectrum of activity against typical sinus pathogens.195-197 Despite these theoretical benefits, multiple studies have failed to demonstrate a clear reduction in infection rates with antibiotic use in uncomplicated, non-surgical cases.190,191,194 In contrast, prophylactic antibiotics are more widely accepted in surgical cases, particularly those involving implant placement or sinus wall manipulation.198-202
In summary, while antibiotics remain commonly prescribed in the setting of orbital fractures with sinus involvement, current literature supports a selective, rather than routine, approach. Future prospective studies are needed to better define the risk-benefit profile and to establish standardized treatment protocols.
Complications
Orbital fractures can lead to a range of complications, whether managed conservatively or operatively. While some complications are a direct result of the initial trauma, others arise from surgical intervention.
Vision-Threatening Hemorrhage: Retrobulbar and Intraorbital Hematoma
Retrobulbar hematoma is one of the most feared complications of orbital trauma given its potential to cause permanent vision loss. A 2025 review of 2,149 patients with orbital fractures found a 1.3% incidence of retrobulbar hematoma. This incidence was higher in high-energy traumas, bilateral fractures, and orbital roof and rim fractures. 203 Intraorbital hematoma is more broadly defined than retrobulbar hematoma, but it poses a serious postoperative risk. In a series of 227 patients undergoing orbital fracture repair, intraorbital hematoma occurred in 0.9% of patients. 204 Another study of 153 blowout and orbitomalar fractures reported a 2% incidence of postoperative intraorbital hematomas, consistent with the low overall incidence of this complication. 205 Given the potential for rapid vision loss, surgeons should monitor closely for visual changes in the immediate postoperative period, and patients should be instructed to seek emergency evaluation if they experience any sudden change in vision after discharge. Retrobulbar hematoma can also cause superior orbital fissure syndrome, a rare complication of orbital fractures with incidence less than 1%.24,206
Infraorbital Nerve Paresthesia
Infraorbital nerve injury may result from trauma or surgical manipulation. Although the literature regarding infraorbital nerve damage following isolated orbital fractures is limited, a 2021 review of zygomaticomaxillary complex fractures reported infraorbital nerve dysfunction in 37.3% of cases, with orbital floor involvement and fracture line through the infraorbital canal as significant predictors. 207 Most cases of infraorbital paresthesia are transient, however, some patients develop persistent neuralgias. A small series of 9 patients reported symptom resolution after surgical decompression for persistent infraorbital neuralgia. The authors of this study propose that evidence of infraorbital nerve compression in a distorted bony canal may warrant operative decompression to prevent or improve neuralgia and chronic pain, even in the absence of other surgical indications. 208
Diplopia
The presence of diplopia is one of the primary indications for orbital fracture repair, but the incidence rates vary widely in the literature, ranging from 15% to 86%. 104 Persistent diplopia can result from prolonged delays in fracture treatment leading to slow recovery of ocular motility, extraocular muscle ischemia from prolonged incarceration, or injury to the inferior oblique muscle during operative approach. 204
Recent studies show the incidence of postoperative diplopia at approximately 20%, with most cases in patients who had diplopia preoperatively. 205 A recent series of 254 orbital fracture repairs shows that risk factors include preoperative enophthalmos, extraocular movement limitations, combined orbital floor and medial wall fractures, and defect size greater than 2 cm2 or displacement greater than 3 mm on CT scan. 209 The same authors created a validated risk calculator for postoperative diplopia that demonstrated excellent sensitivity (87.9%) and negative predictive value (95.8%), making it useful for ruling out postoperative diplopia. 210
Timing of repair is also critical to postoperative diplopia, with 1 study showing that surgery within 2 weeks of injury led to a higher resolution rate of diplopia compared to surgery after 2 weeks (58% vs 38.1%). 104 Although most studies suggest that timing and fracture characteristics are associated with postoperative diplopia, a 2017 retrospective cohort of 126 patients found that increased age was the only factor significantly associated with postoperative diplopia. 211
Enophthalmos and Exophthalmos
Enophthalmos may present immediately or in a delayed fashion due to soft tissue remodeling or fat atrophy. It is estimated to occur in 7% to 10% of patients treated nonoperatively, 212 though some report much higher rates. 213
While orbital volume expansion is a commonly cited mechanism for enophthalmos, soft tissue changes and geometric bony remodeling also contribute and there is no consensus on the most important predictors. One study found that orbital volume accounted for only 50% of post-traumatic enophthalmos. 214 Other studies identified defect size and herniated fat volume as the most significant predictors of enophthalmos215,216 or found no correlation between increased orbital volume and long-term enophthalmos. 27 Exophthalmos is rarer with a reported incidence of 5.5% postoperatively. 205
Eyelid Malposition
The risk of eyelid malposition varies with surgical approach, and risk is increased in older patients with lid laxity. Multiple retrospective series and systematic reviews agree that subciliary incisions are associated with higher rates of ectropion and scleral show. Incidence of ectropion ranges between 2.6% and 25% in subciliary groups and 0% and 4.4% in transconjunctival groups. Risk of entropion is higher in transconjunctival groups, with the incidence ranging from 2.5% to 6.6%.154,217-219 Overall, transconjunctival incisions have lower complication rates, but surgeons should be aware that this approach may require a lateral canthotomy for adequate exposure. 217
Complications of Medial Wall and Orbital Roof Fractures
Medial wall fractures can damage the nasolacrimal duct, resulting in postoperative epiphora. Recent literature examining epiphora as a result of orbital fractures is sparse, but a 2024 series of 227 repairs reported epiphora in 2 patients postoperatively (less than 1%). 204 It is important to maintain a high index of suspicion in fractures involving the medial orbital wall and lacrimal outflow tract to adequately treat or prevent epiphora. Additional complications of medial wall fractures include disruption of the medial canthal ligament, which may result in telecanthus if not identified and addressed. 2
Orbital roof fractures may result in cerebrospinal fluid leak and pneumocephalus, and carry a risk of serious intracranial complications including meningitis, brain abscess and encephalocele if not promptly identified and managed. Many cerebrospinal fluid leaks resolve with conservative measures such as head-of-bed elevation and activity restriction, but persistent or high-volume leaks may require neurosurgical intervention. Given the complexity of these injuries and their potential for intracranial involvement, the literature supports multidisciplinary management with neurosurgery. 107
Implant-Related Complications (Exposure, Migration, Infection)
Implant exposure, migration, and infection are uncommon but serious complications. In a 2024 review of 227 cases, 1.3% of patients experienced implant-related issues including infection, rejection, and exposure. 204 A separate retrospective study reported 2.3% of patients experienced pain or infection attributed to the implant, and 0.8% experienced immediate exposure. 205
In addition to exposure and infection, complication profiles can vary by implant type, making implant selection a clinical challenge. Proponents of titanium mesh implants point to their ability to bio-integrate with low extrusion and infection rates; however, their pro-inflammatory properties can result in the adhesion of orbital tissues to the implant, leading to eyelid retraction, diplopia or restriction of extraocular movements. This phenomenon is known as orbital adherence syndrome. 220 The incidence, pathophysiology and clinical significance of orbital adherence syndrome remain controversial. Some authors attribute postoperative motility restriction to titanium-induced fibrosis, while others argue adhesions occur with all implant types. Management of orbital adherence syndrome is difficult and often includes removal of the titanium implant and lysis of fibrotic tissue. To reduce this risk, multiple authors advocate for the use of smoother, more inert materials such as nylon foil implants rather than titanium mesh. 221 Others support the use of barriers that surround the titanium implants to prevent direct contact with orbital tissues. A 2019 retrospective study comparing titanium implants alone versus those covered with a xenogenic collagen membrane reported significantly lower rates of postoperative diplopia, extraocular movement limitation, and eyelid rigidity when a barrier was used. 222 Similarly, another retrospective study found that polyethylene coated titanium mesh implants had lower rates of postoperative diplopia than uncoated titanium implants. 223 Although larger studies are needed to validate these findings, barrier-coated titanium implants represent a promising strategy to reduce adhesion-related complications.
Discussion
Despite substantial advances in imaging, biomaterials, and operative technique, the management of orbital fractures remains heterogeneous across specialties and institutions. This review (Figure 1) highlights that variability persists in nearly every stage of care, from initial assessment to operative timing and postoperative management. Although high-resolution CT has become the diagnostic standard and provides excellent characterization of bony and soft tissue injury, clinical decision-making still relies heavily on physical examination findings such as diplopia, enophthalmos, globe malposition, and evidence of muscle entrapment. Importantly, contemporary literature increasingly challenges several traditional management paradigms. Historically, large orbital floor defects were repaired preemptively to avoid delayed enophthalmos; however, more recent evidence suggests that fracture size alone may not reliably predict long-term functional or cosmetic deformity. Similarly, although enophthalmos has classically been attributed to orbital volume expansion, emerging studies demonstrate that soft tissue remodeling, fat atrophy, and complex geometric changes contribute substantially to globe displacement. These findings underscore the multifactorial nature of orbital fracture sequelae and support a more individualized management strategy that prioritizes clinical symptoms and functional outcomes over radiographic measurements alone.
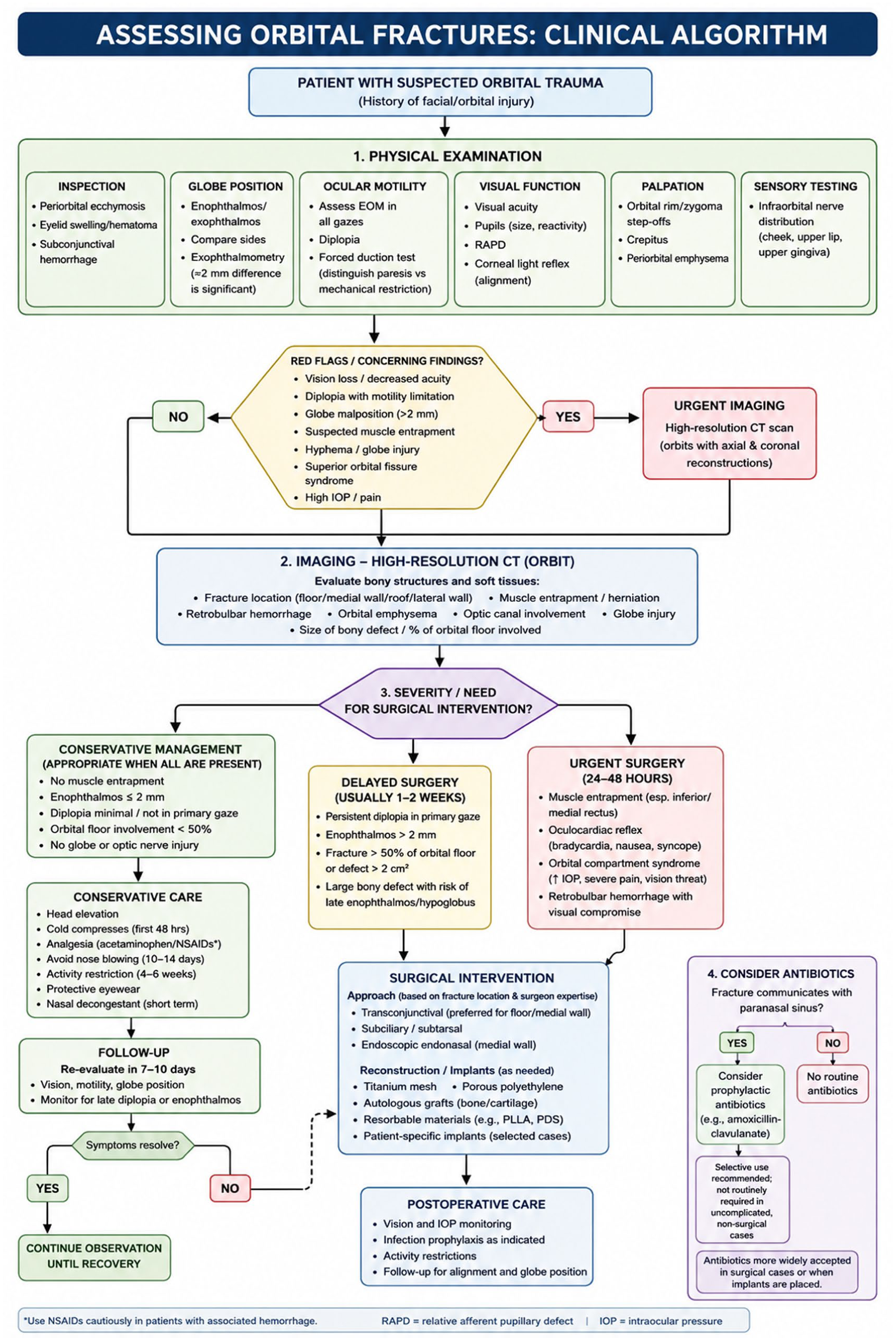
Clinical algorithm for assessing patients with suspected orbital fractures.
The evolving evidence surrounding operative timing further illustrates the shift toward tailored decision-making. While urgent intervention remains essential in cases of muscle entrapment, oculocardiac reflex, orbital compartment syndrome, or vision-threatening injury, the optimal timing for less severe fractures continues to be debated. Several studies support repair within 2 weeks to improve recovery of ocular motility and reduce persistent diplopia, yet others suggest that delayed intervention may yield comparable outcomes in carefully selected patients. This discrepancy likely reflects the heterogeneity of fracture patterns, patient demographics, and outcome definitions across studies. Pediatric trapdoor fractures represent a particularly important exception, as prompt release of entrapped tissue is critical to prevent ischemic injury and long-term motility deficits. Advances in surgical technique have also refined reconstruction strategies. Transconjunctival approaches have largely supplanted subciliary incisions because of lower rates of ectropion and scleral show, while patient-specific implants and image-guided navigation offer increasingly precise restoration of orbital anatomy in complex fractures. Nevertheless, implant selection remains controversial, particularly regarding titanium-associated orbital adherence syndrome and the long-term performance of resorbable materials. Collectively, these developments demonstrate that successful orbital fracture management requires not only technical expertise but also careful patient selection and an appreciation of evolving evidence.
Another major finding of this review is the persistent lack of consensus in areas where high-level evidence remains limited, particularly regarding prophylactic antibiotics and predictors of postoperative complications. Although antibiotics are frequently prescribed for fractures communicating with the paranasal sinuses, available studies have not consistently demonstrated reduced infection rates in uncomplicated injuries managed nonoperatively. This discrepancy between common practice and evidence-based support highlights the need for prospective randomized studies capable of defining which patients truly benefit from antimicrobial prophylaxis. Likewise, postoperative complications such as diplopia, infraorbital nerve dysfunction, enophthalmos, eyelid malposition, and implant-related morbidity continue to present important clinical challenges despite advances in care. Recent efforts to develop predictive models for postoperative diplopia represent a promising step toward risk stratification and personalized treatment planning, but these tools require further external validation before widespread adoption. Overall, the current literature supports a multidisciplinary and patient-centered approach to orbital fracture management, integrating ophthalmology, plastic surgery, otolaryngology, and neurosurgery when appropriate. Future research should prioritize standardized outcome measures, prospective comparative trials, and long-term functional assessment to better define optimal management algorithms and improve both aesthetic and visual outcomes following orbital trauma.
Conclusion
Orbital fractures remain a complex and evolving challenge in craniofacial trauma care, requiring integration of meticulous clinical examination, high-resolution imaging, and individualized treatment planning to optimize functional and aesthetic outcomes. Contemporary evidence supports a selective and patient-centered approach in which operative intervention is guided not solely by fracture size or radiographic appearance, but by symptoms such as diplopia, enophthalmos, muscle entrapment, and visual compromise. Advances in CT imaging, minimally visible surgical approaches, biomaterials, and patient-specific implants have improved diagnostic accuracy and reconstructive precision, yet significant controversy persists regarding operative timing, implant selection, and the routine use of prophylactic antibiotics. Complications including persistent diplopia, infraorbital nerve dysfunction, eyelid malposition, retrobulbar hematoma, and implant-related morbidity continue to underscore the importance of careful patient selection, close follow-up, and multidisciplinary collaboration. As the incidence of orbital fractures continues to rise, particularly among elderly patients with fall-related injuries, future prospective studies with standardized outcome measures are needed to clarify unresolved management questions and establish more consistent evidence-based treatment algorithms.
Footnotes
Ethical Considerations
There are no human participants in this article and informed consent is not required.
Consent to Participate
All participants voluntarily provided information and signed an informed consent form.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter J. Taub and Devra B. Becker are members of the Editorial Board of FACE and did not take part in the peer review or decision making process for this submission.