
Abstract
Purpose:
We present a patient with an optic nerve infarct after a recent medial orbital wall fracture. The suspected mechanism was a transient orbital compartment syndrome or localized air bubble in the orbital apex, as the patient presented with pain in the affected eye, with sneezing as a potential trigger.
Observations:
A 66-year-old male presented to the outpatient ophthalmology clinic with persistent left eye pain and swelling. Four days prior, a fall led him to the emergency department (ED), where computed tomography (CT) showed a left medial orbital wall fracture. Initial visual acuity was 20/20 and 20/40. Intraocular pressure (IOP) was 9 and 22 mmHg in the right and left eyes respectively. There was mild limitation of left eye supraduction and infraduction. Repeat CT demonstrated orbital emphysema, and he was given a methylprednisolone dose pack and strict sinus precautions. Fifteen hours after the clinic visit, nearly 5 days after his fall, he presented to the ED with left eye pain and with no light perception (NLP) in the left eye, an IOP of 26, non-reactive pupil with a left afferent pupillary defect, and near complete ophthalmoplegia. He reported sneezing multiple times overnight. He received IV steroids and underwent emergent lateral canthotomy with superior and inferior cantholysis of the left eye, after which IOP was 19 in that eye. He remained NLP, and Magnetic Resonance (MR) imaging demonstrated an ischemic infarct within the optic nerve.
Conclusions and importance:
While rare, vision loss can occur as a complication of orbital emphysema (OE). Providers may consider recommending patients check their vision after any Valsalva inducing event. Possible interventions for OE, if vision-threatening, include emergent cantholysis and needle decompression.
Introduction
Orbital emphysema (OE) with and without visual compromise in the context of orbital trauma and sneezing has been documented in the literature.1,2 OE after trauma suggests an orbital wall fracture with direct communication between the paranasal sinuses and orbit, with air forced in through a pressure gradient. 3 A pathological connection between sinuses and orbit combined with an event that rapidly increases pressure, such as a sneeze, can lead to complications if the tissues at the fracture site create a ball-valve mechanism, not allowing the air to escape. 3 We present a rare case of optic nerve infarction after medial orbital wall fracture that may have been related to a sneeze-induced compressive optic neuropathy leading to severe vision loss in a patient with OE.
Case Report
A 66-year-old man presented to an outside emergency department (ED) for eye pain after a fall. Pertinent medical history includes obstructive sleep apnea (OSA), hypertension, diabetes mellitus, and coronary artery disease. He was not using his Continuous Positive Airway Pressure (CPAP) machine. Computed tomography (CT) head showed a comminuted fracture of the left medial orbital wall with pre-septal and post-septal air throughout. Eye movements were full. The patient was discharged with antibiotics and recommended to follow-up with outpatient ophthalmology.
Four days after discharge, the patient presented to the ophthalmology clinic endorsing left eyelid pain and swelling since the fall. Visual acuity (VA) was 20/20 in the right eye and 20/40 (pinhole to 20/25) in the left eye while intraocular pressures (IOP) were 9 and 22 mmHg respectively. Pupils were equal, round, and reactive, with no relative afferent pupillary defect (APD). Extraocular movements were full in the right and mildly limited in supraduction and infraduction in the left. Confrontational visual fields were full. On slit lamp exam, there was significant periorbital edema with crepitus, trace chemosis, and patchy subconjunctival hemorrhage in the left eye. Dilated fundus exam was unremarkable.
A CT maxillofacial scan without contrast was ordered as the outside CT was unavailable. He was prescribed a methylprednisolone dose pack for periorbital edema and counseled on return precautions and sinus precautions, including strict no nose blowing for 3 weeks. Follow-up was scheduled for 4 days later. The CT scan (Figure 1) showed a left medial orbital wall fracture, associated extensive intraorbital, periorbital, left facial, and deep cervical soft tissue emphysema, and mild proptosis. No intraorbital hematoma was seen. CT findings and return precautions were discussed with the patient over the phone.
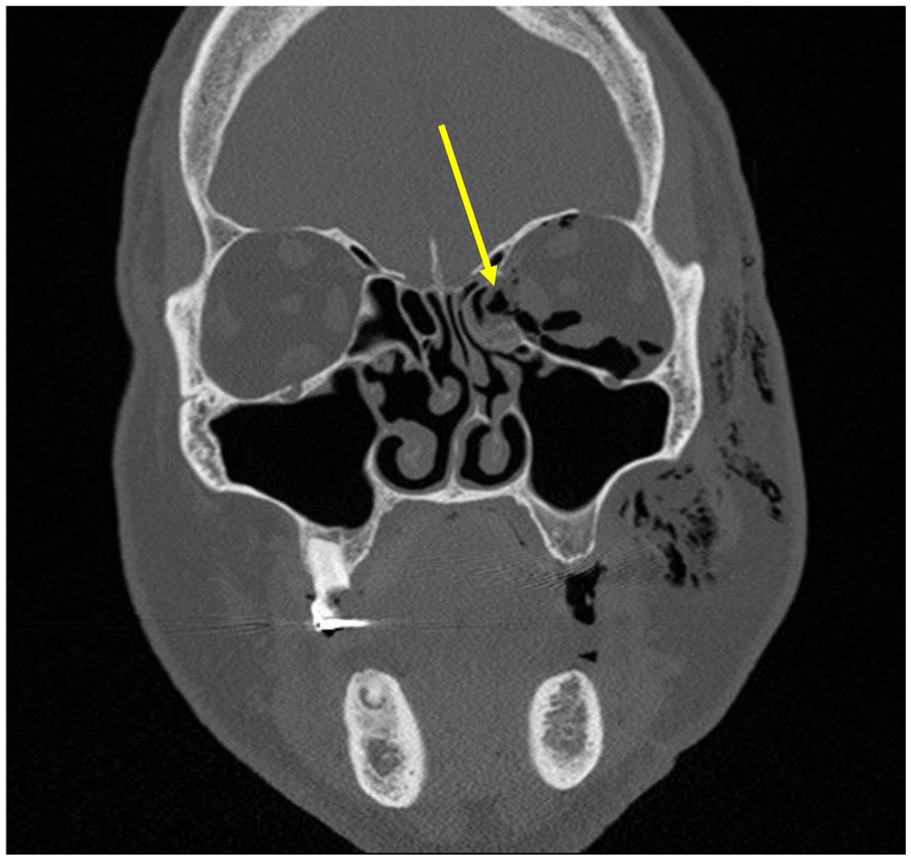
Initial CT scan of the orbits and sinuses after clinic visit showing left orbital emphysema and medial orbital wall fracture (yellow arrow).
Fifteen hours after the clinic visit, nearly 5 days after his fall, he presented to our ED for blurry vision in his right eye (the eye unaffected by injury) and pain in his left eye. He reported sneezing multiple times overnight. He was given IV methylprednisolone 125 mg. In the right and left eyes respectively, VA was 20/30 and NLP, and IOP was 21 and 26. His left pupil was non-reactive with a left relative APD, and his left eye demonstrated near-complete ophthalmoplegia. There was significant edema with crepitus on palpation, though the lids remained relatively soft and easy to open. His left eye showed moderate chemosis and diffuse injection. Dilated fundus exam was unremarkable. The patient was unaware of vision loss in his left eye until his eyelid was manually elevated by the ophthalmologist.
The patient was given an additional dose of 125 mg IV methylprednisolone and underwent emergent lateral canthotomy with superior and inferior cantholysis. His IOP improved to 19. He was admitted and given 1 g of IV methylprednisolone once a day for 2 more days. The patient remained NLP in the left eye. Dilated fundus exam was normal, without a cherry red spot or optic nerve edema. Magnetic resonance imaging (MRI) orbit with and without contrast a few hours post-canthotomy/cantholysis showed extensive intra-orbital and periorbital emphysema with mild stretching and lengthening of the left optic nerve and loss of the normal optic nerve sheath T2 signal. Two days post-canthotomy/cantholysis, MRI, MR venography (MRV), and MR angiography (MRA) of the brain and orbits were performed. MRI demonstrated an ischemic infarct within the midportion of the left optic nerve (Figure 2A), corresponding with an area of T1 hyperintensity on prior MRI orbit. On MRA, there was enlargement of the proximal left ophthalmic artery with the distal portion not visualized (Figure 2B). On MRV, the left ophthalmic vein was not visualized, and so a thrombus could not be ruled out. On the patient’s last follow up visit 11 months later, the vision remained NLP in the left eye and diffuse optic disk pallor was documented.
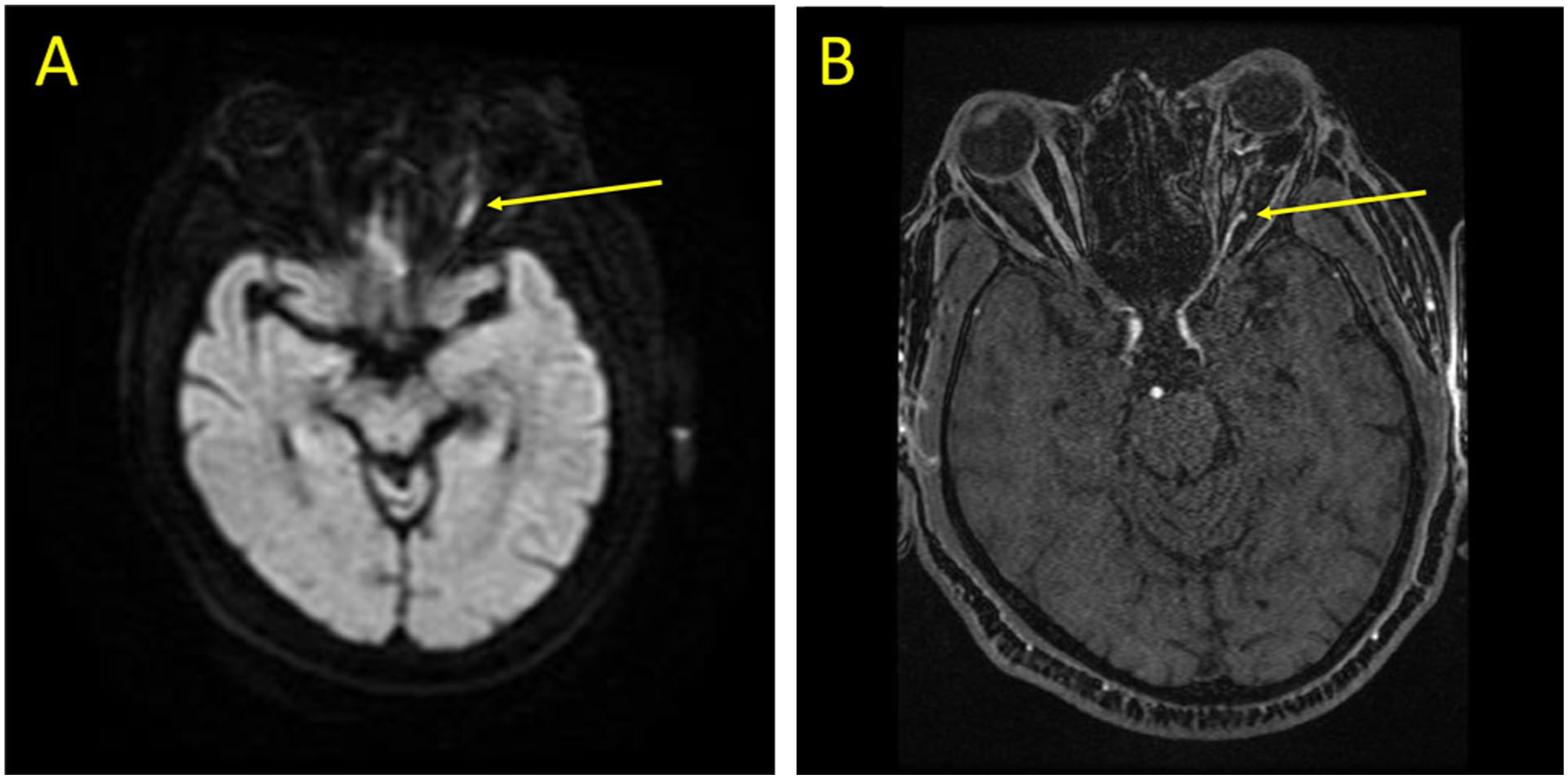
MRI brain with DWI (A), showing thinned left optic nerve with bright mid-portion and MRA brain (B) showing left ophthalmic artery only visualized to the mid portion of the optic nerve.
Discussion
While the exact etiology of the optic nerve infarct in this patient is not possible to determine, it is possible that the sneeze may have caused an extreme, transient pressure spike that infarcted the nerve before settling to 26 mmHg. A venous thrombus could not be ruled out, but sudden severe vision loss would be less likely with venous thrombosis and there were no retinal findings to suggest venous congestion. It could also be an independent ischemic event, but that is less likely. Aspects of the case that support the suspected mechanism being a transient orbital compartment syndrome or localized air bubble in the orbital apex is the patient presenting with pain in the affected eye with sneezing as a potential trigger. On arrival to the ED, he did not have very high IOP and the eyelids were easily opened, but he did have significant ophthalmoplegia.
Studies have found an association between OE and medial wall fractures, with OE more common in medial wall and combined medial wall-floor fractures compared to floor fractures alone.4,5 The medial wall connects to the ethmoid sinus, which is smaller than the maxillary sinus and more likely to involve air trapping. 4 Although OE is often benign and self-limiting, OE in the setting of medial wall fractures may warrant additional caution and close monitoring. 3 Management of vision-threatening OE involves urgent needle decompression and/or lateral canthotomy and cantholysis.6-8 In this case, since lateral canthotomy and cantholysis alone led to sufficient IOP reduction, needle decompression was not pursued. It may have been reasonable to pursue needle decompression, particularly if an air pocket to target had been visualized on imaging, but with the improved IOP, this was not pursued.
A key takeaway from this case is that for patients with OE, serial, frequent vision, and IOP checks may lead to early detection and timely intervention. Although there is no evidence in the literature to support performing a needle decompression for everyone with OE on initial presentation, it could be considered in cases with potential higher risk such as those with significant emphysema, EOM restriction, and medial wall involvement. Beyond nose-blowing precautions, providers may also consider asking patients to assess their vision after any Valsalva-inducing event. Additionally, while CT is the imaging modality of choice in orbital trauma, MRI can play a role in assessing and localizing any vascular complications secondary to OE. 1 In cases of vision loss like our patient, MRA and MRV may also provide important prognostic information, such as the potential for visual recovery.
Footnotes
Acknowledgements
None.
Ethical Considerations
IRB approval was not required for this manuscript. Informed consent to publish this report was obtained from the patient and no personally identifying information was included.
Consent to Participate
Informed consent to publish this case has been obtained, though the patient requested that no photographs of his face be included. This report does not contain any personal identifying information.
Author Contributions
All authors (MA, NM, CMM, HAS) attest that they meet the current ICMJE criteria for authorship.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon reasonable request to the corresponding author.