
Abstract
Background:
Microtia is a congenital defect of the external ear, ranging from structural auricular deficiency to anotia, and is frequently associated with hearing impairment. Its prevalence varies geographically, with notably higher rates reported in high-altitude regions of Ecuador. However, clinical, and anatomical comparisons between isolated and familial microtia in Ecuador remain limited.
Objective:
To analyze the demographic, clinical, and anatomical characteristics of Ecuadorian patients with microtia, emphasizing differences between isolated and familial cases.
Methods:
A cross-sectional observational study was conducted in 2024, including 146 patients with confirmed microtia. Patients were classified as isolated or familial according to family history. Demographic, clinical, anatomical, and audiological variables were collected. Minor auricular findings, including auricular nodules, preauricular sinus, Darwin tubercle, and prominent ear, were recorded separately as associated anatomical observations and were not considered diagnostic criteria or severity indicators. Data were analyzed using descriptive statistics, chi-square, and Mann-Whitney tests, and multivariate logistic regression.
Results:
Median age was 10 years (IQR 8-14), with no significant age differences between groups. Isolated microtia was more frequent in males than familial microtia (72.32% vs 52.94%; P = .034). Familial cases showed more Grade 1 right-ear microtia (26.7% vs 11%; P = .003), whereas isolated cases more commonly presented Grade 3 microtia. Left auricular nodules, or mamelons, were significantly associated with isolated microtia (P = .024; OR = 8.07; 95% CI: 1.05-62.24).
Conclusion:
Isolated and familial microtia showed distinct demographic and anatomical patterns. Auricular nodules were associated with isolated microtia but should be interpreted as associated anatomical findings, not diagnostic or severity markers.
Highlights
High-Altitude Prevalence: Microtia shows a markedly higher prevalence in Ecuador, particularly in high-altitude regions, supporting an association between geographic factors and increased disease occurrence.
Sex Distribution and Severity: Isolated microtia was more frequent in males and was more often associated with severe defects, particularly Grade 3 microtia, whereas familial cases showed a more balanced sex distribution and more commonly presented milder forms, especially Grade 1 microtia.
Auricular Nodules as Associated Findings: Left auricular nodules, or mamelons, were significantly associated with isolated microtia, with affected patients being approximately 8 times more likely to present this finding than familial cases. These nodules should be interpreted as associated anatomical findings, not as diagnostic criteria, or markers of microtia severity.
Distinct Anatomical Patterns in Familial Microtia: Familial microtia was characterized by less severe auricular defects and a higher proportion of recognized genetic syndromes, highlighting the importance of family history assessment and genetic evaluation.
Clinical Implications: Differentiating isolated from familial microtia has practical implications for clinical evaluation, anatomical characterization, genetic counseling, audiological follow-up, and individualized treatment planning.
Introduction
Microtia is a congenital anomaly of the external ear with heterogeneous clinical presentation and variable prevalence across populations.1,2 In Ecuador, previous studies have reported a comparatively high burden of microtia, particularly in high-altitude regions, suggesting that geographic and environmental conditions may contribute to increased disease occurrence.3,4 Ecuadorian cohorts have also shown characteristic clinical patterns, including unilateral involvement, right-sided predominance, male predominance, and frequent hearing impairment, although severity and associated findings may vary among patients.5,6
Beyond geographic factors, social and healthcare-related disparities may influence the recognition, evaluation, and follow-up of patients with microtia, especially in rural and underserved communities.7,8 Recent evidence supports that microtia is a multifactorial condition in which genetic susceptibility, environmental exposures, maternal factors, and developmental mechanisms may interact during craniofacial formation. 9 Clinical and phenotypic studies further emphasize the importance of detailed anatomical characterization, including laterality, degree of auricular deficiency, external auditory canal status, associated anomalies, and audiological profile.10-13
Microtia may occur as an isolated defect or as part of broader congenital anomaly patterns. High-altitude exposure has been proposed as a potential contributor to congenital anomalies in Ecuador, although its specific relationship with microtia severity remains uncertain. 14 Syndromic and craniofacial conditions, including Treacher Collins syndrome, branchio-oto-renal spectrum disorders, hemifacial microsomia, and other congenital external ear anomalies, may include microtia or overlapping auricular findings.15-18 Therefore, distinguishing isolated from familial or syndromic cases is essential for accurate clinical classification, family history assessment, and genetic counseling.
The interpretation of minor auricular findings also requires careful distinction. Some external ear variants or associated findings may coexist with microtia but should not necessarily be considered part of the microtia spectrum.19,20 This distinction is particularly relevant when comparing isolated and familial cases, because overclassification of common auricular variants may affect phenotype definition and bias genotype-phenotype correlations. Current genetic and environmental evidence supports the need to refine clinical subgroups and evaluate how inherited susceptibility, developmental pathways, and external exposures contribute to microtia heterogeneity.21-25
Ecuadorian populations provide a unique context for studying congenital anomalies because of their substantial genetic heterogeneity and admixture. Studies in Amerindian Kichwas, Mestizos, and Afro-Ecuadorian descendants using STR and SNP markers have demonstrated Native American, European, and African ancestral contributions.26,27 More recent genomic analyses describe Ecuador as a highly structured tri-hybrid population, with ancestry patterns varying by ethnicity and geography.28,29 This population structure may influence susceptibility to congenital anomalies and could help explain differences between isolated and familial microtia in high-prevalence regions.
This study aims to analyze the demographic, clinical, and anatomical characteristics of Ecuadorian patients with microtia, with emphasis on identifying differences between isolated and familial cases. By characterizing these patterns, the study seeks to improve clinical classification, support individualized evaluation, and guide future research on genetic, environmental, and population-specific factors influencing microtia development.
Methods
Study Design
This study employed an epidemiological, cross-sectional, and observational design.
Participants
Patients with a confirmed clinical diagnosis of microtia were recruited during 2024. Individuals who had not attended a follow-up visit within the previous year were eligible for inclusion. Recruitment was conducted through a word-of-mouth call disseminated by medical students affiliated with the institution. Patients of both sexes and diverse ethnic backgrounds were included. Participants were classified into 2 groups: isolated microtia and familial microtia, based on family history criteria detailed below.
Variables
Collected variables included demographic data (age, sex), clinical characteristics (type of disability, use of hearing devices, and type of device), and associated risk factors. Anatomical variables included laterality of microtia involvement (left, right, or bilateral), degree of microtia, external auditory canal status (normal, stenosis, or absence), ear implantation (normal or low ear placement), and phenotypic classification. Minor auricular findings, including auricular nodules (mamelons), preauricular sinus, Darwin tubercle, and prominent ear, were recorded separately as associated anatomical observations and were not used as diagnostic criteria for microtia or as indicators of microtia severity.
Measurements
A standardized anatomical examination of the external ear was performed for each participant to document microtia laterality, severity grade, external auditory canal status, ear implantation, and associated minor auricular findings. Minor auricular findings were recorded separately and did not modify the classification of microtia grade or phenotype.
Bias: To minimize observer bias, all medical examinations were conducted by experienced specialists in Plastic Surgery, Medical Genetics, and Audiology.
Study Size: n = 146
Quantitative Variables
Audiological evaluations were conducted by licensed audiologists or speech-language therapists. Hearing assessment protocols were selected according to patient age and cooperation level, following standard clinical practice.
Statistical Methods
Data were analyzed using RStudio© and IBM® SPSS® Statistics version 29. Qualitative variables were summarized using frequencies and percentages, while quantitative variables were described using medians and interquartile ranges (IQR).
Normality of continuous variables was assessed using the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to compare median ages between groups, and the chi-square test or Fisher’s exact test (when appropriate) was applied to categorical variables, including sex, type of disability, and hearing device use. A P < .05 was considered statistically significant. Multivariate logistic regression analysis was performed to identify independent predictors of microtia type (isolated vs familial), including age, sex, type of auditory disability, hearing device use, family history, microtia grade, presence of auricular nodules, and phenotypic classification.
Definitions
Isolated Microtia: Cases in which microtia affects 1 or both ears without a documented family history of microtia, without associated congenital syndromes, and with no other affected relatives.
Familial Microtia: Cases in which 1 or more first-degree relatives, including parents or siblings, are affected, or when at least 2 relatives across generations, such as grandparents, uncles, aunts, or cousins, have a confirmed diagnosis of microtia.
Degree of Microtia: Microtia severity was classified according to standard clinical grading. Grade 1 microtia was defined as a mildly small ear with recognizable anatomical landmarks, sometimes referred to as a constricted ear. Grade 2 microtia was defined as a partially formed auricle with an absent or stenotic external auditory canal. Grade 3 microtia corresponded to a peanut-shaped auricle with external auditory canal atresia. Grade 4 microtia was defined as complete absence of the auricle, or anotia.
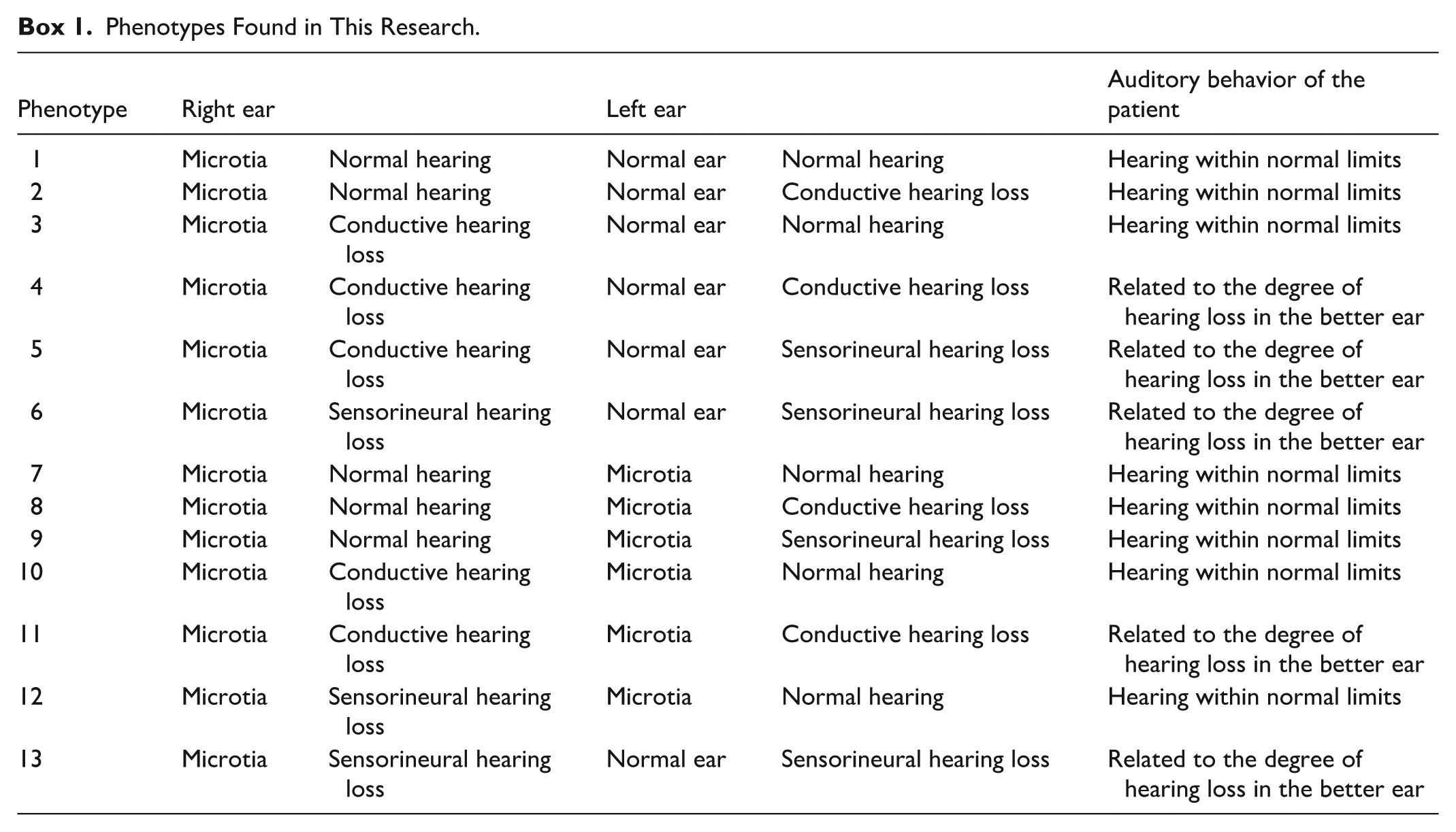
Phenotypes: Phenotypes were defined based on the combination of auricular morphology and audiological profile of each ear, as detailed in Box 1.
Phenotypes Found in This Research.
Type of Disability: The type of disability was defined according to the official evaluation issued by the Ministry of Health, which provides certification of disability type and percentage.
Associated Minor Auricular Findings: Minor auricular findings were recorded as associated anatomical observations and were not considered diagnostic criteria for microtia or part of the microtia spectrum. These findings included Darwin tubercle, a congenital prominence located on the posterior margin of the helix; preauricular fistulae or sinuses; prominent ears, also referred to as protruding ears, characterized by abnormal auriculocephalic angles without tissue deficiency; and preauricular nodules or mamelons, which represent remnants of embryonic auricular hillocks. Darwin tubercle, prominent ear, and preauricular sinus were documented separately because they may coexist with microtia or represent common anatomical variants, but they were not classified as forms of microtia. Preauricular nodules or mamelons were analyzed as associated auricular findings because of their potential relevance to external ear development (see Figure 1).
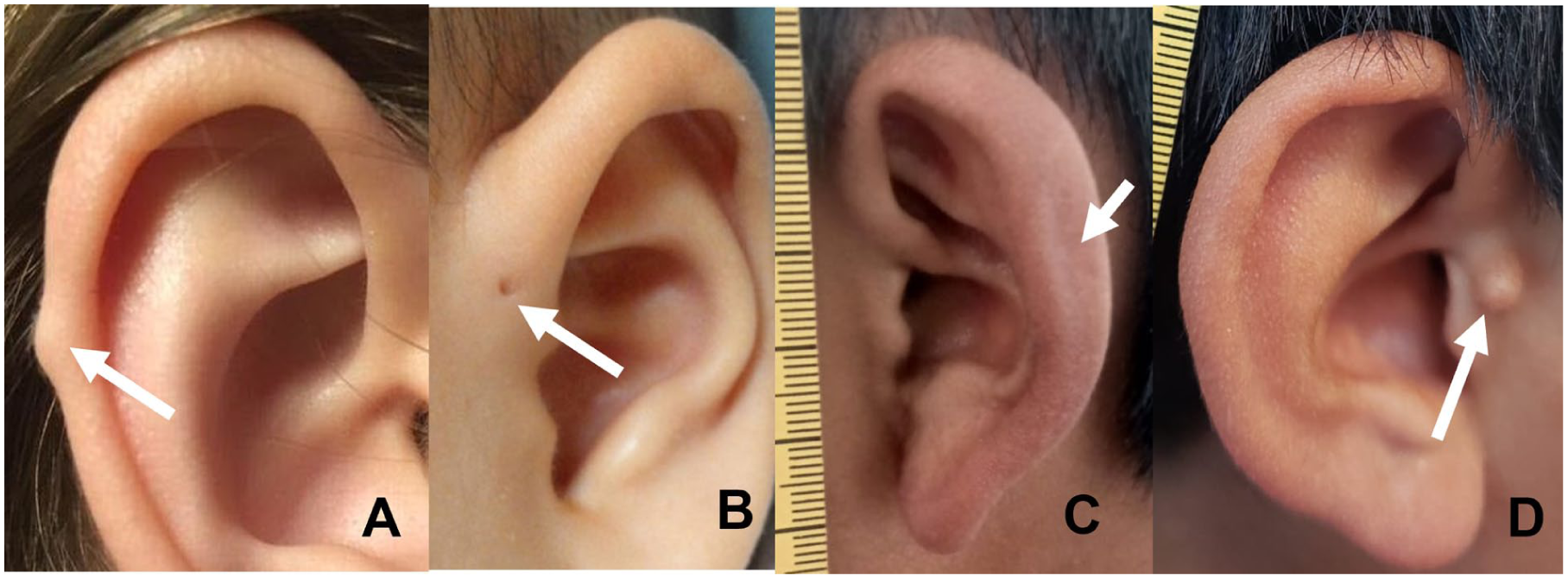
Minimal auricular anomalies representing the mildest end of the microtia spectrum. (A) Darwin tubercle, with the arrow indicating the focal thickening/projection along the superior helix. (B) Preauricular fistula or sinus, with the arrow indicating the small pit anterior to the auricle. (C) Prominent ear, also known as protruding or cup ear, with the arrow indicating the increased outward projection of the auricle. (D) Preauricular nodule or mamelon, with the arrow indicating the accessory soft-tissue nodule located anterior to the ear.
Results
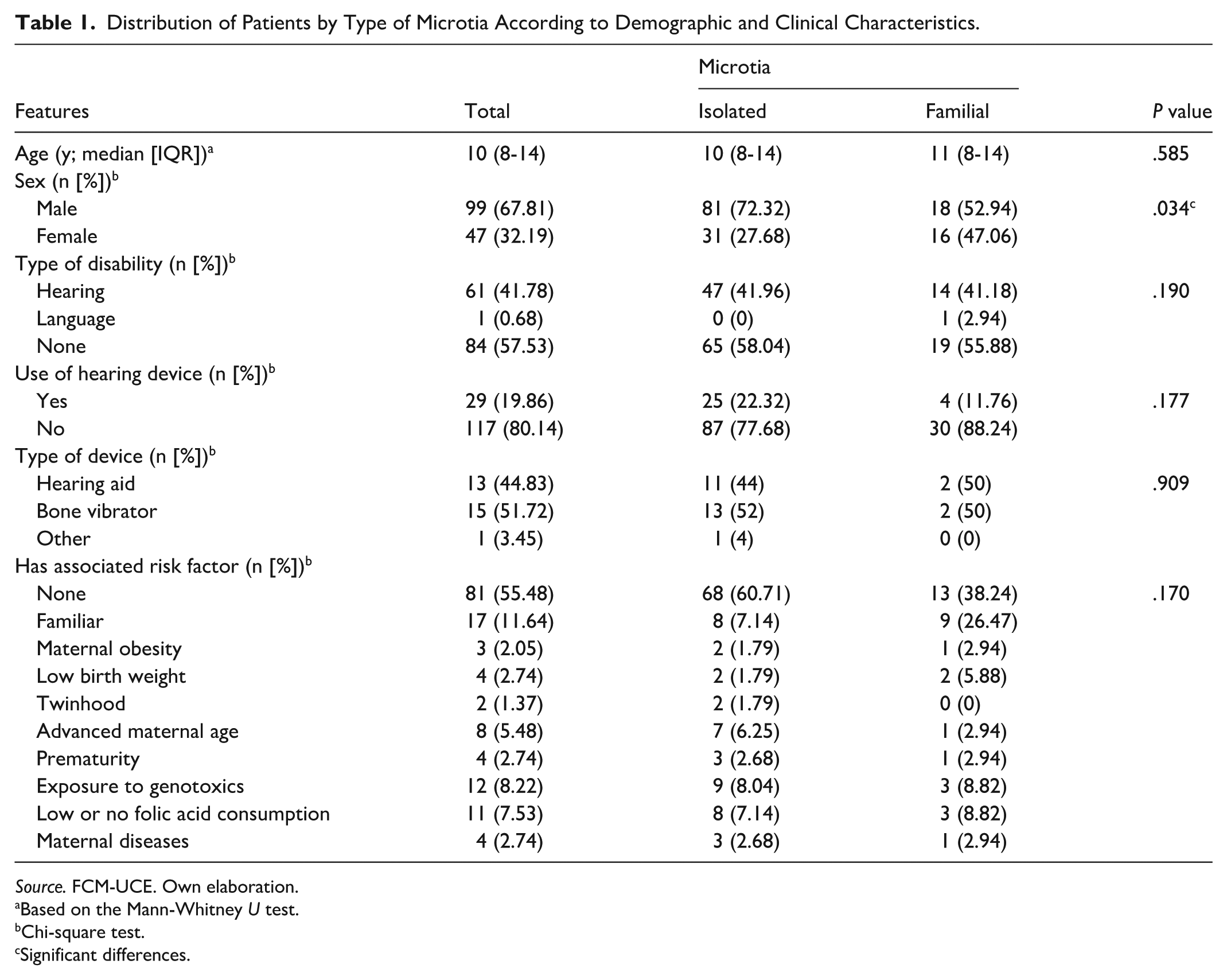
Table 1 summarizes the distribution of patients according to demographic and clinical characteristics by microtia type. Table 2 presents the anatomical characteristics stratified by isolated and familial microtia. Box 1 describes the phenotypic classifications identified in the study, and Table 3 shows the association between the presence of auricular nodules (mamelons) in the left ear and microtia type. All patients underwent complete clinical and audiological evaluation, and no cases were excluded from the analysis.
Distribution of Patients by Type of Microtia According to Demographic and Clinical Characteristics.
Source. FCM-UCE. Own elaboration.
Based on the Mann-Whitney U test.
Chi-square test.
Significant differences.
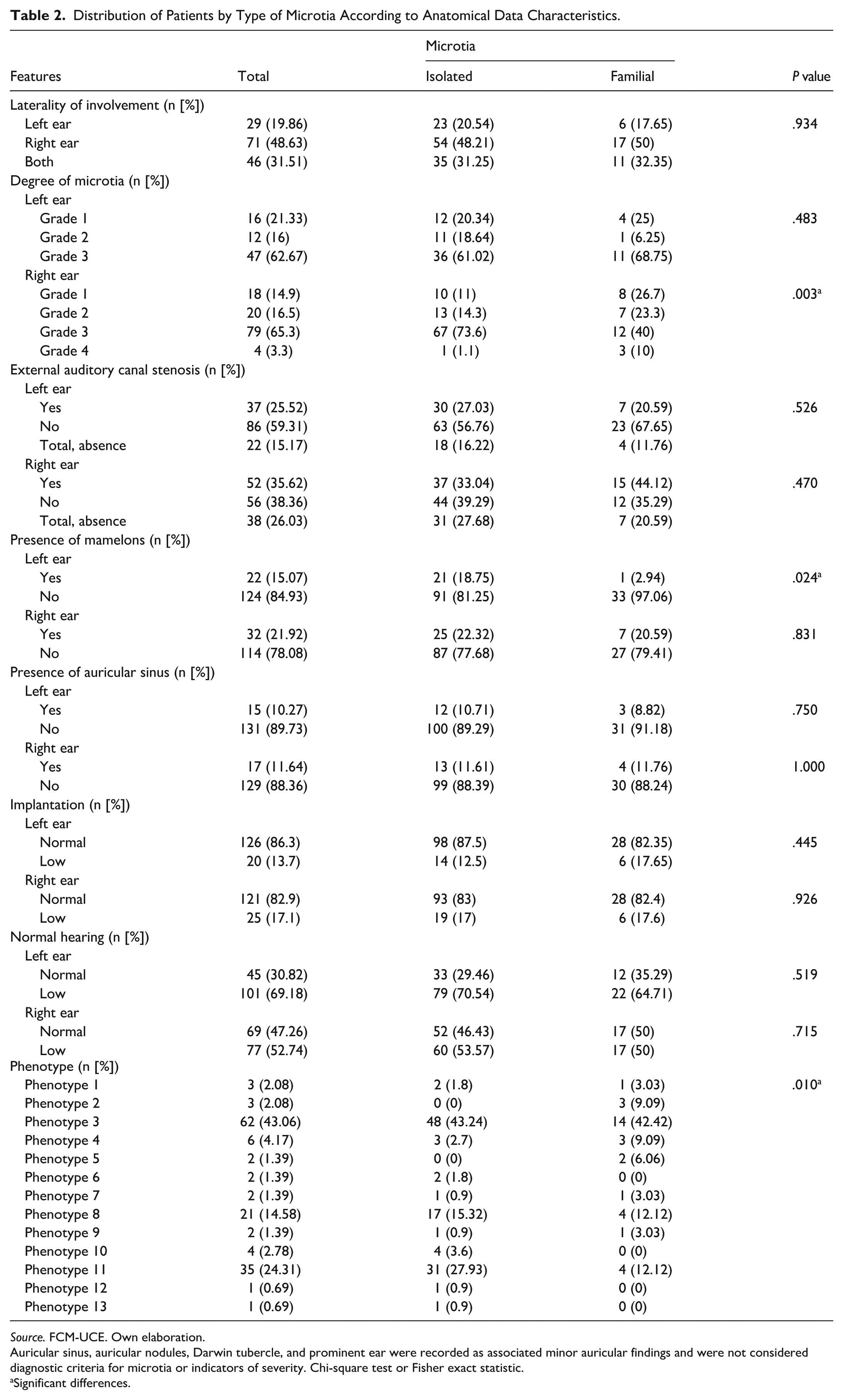
Distribution of Patients by Type of Microtia According to Anatomical Data Characteristics.
Source. FCM-UCE. Own elaboration.
Auricular sinus, auricular nodules, Darwin tubercle, and prominent ear were recorded as associated minor auricular findings and were not considered diagnostic criteria for microtia or indicators of severity. Chi-square test or Fisher exact statistic.
Significant differences.
Relationship Between Mamelons in the Left Ear and Microtia Type.
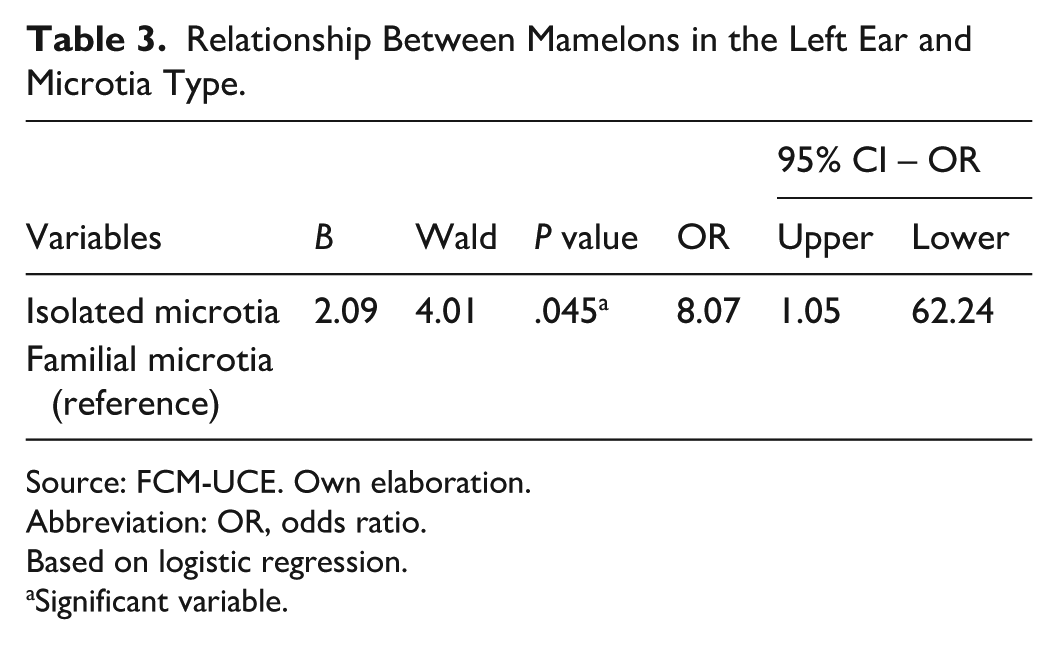
Source: FCM-UCE. Own elaboration.
Abbreviation: OR, odds ratio.
Based on logistic regression.
Significant variable.
Demographic and Clinical Characteristics
The median age of patients with microtia was 10 years (IQR 8-14), with no statistically significant difference between isolated and familial cases (P = .585). Sex distribution differed significantly between groups (P = .034), with a higher proportion of males among isolated microtia cases (72.32%) compared to familial cases (52.94%). Overall, 41.78% of patients presented with hearing disability, with no significant difference between isolated and familial microtia (P = .190). Hearing device use was reported in 19.86% of patients and was more frequent in isolated cases (22.32%) than in familial cases (11.76%); however, this difference was not statistically significant (P = .177). No significant differences were observed in the type of hearing device used, including hearing aids, bone vibrators, or other devices (P = .909). Several potential risk factors were evaluated, including family history, maternal obesity, low birth weight, multiple gestation, advanced maternal age, prematurity, exposure to genotoxic agents, low or absent folic acid supplementation, and maternal illnesses. Although a positive family history was more frequent in familial cases (26.47%) than in isolated cases (7.14%), the overall distribution of risk factors did not differ significantly between groups (P = .170). Among familial microtia cases, 17.65% were associated with a recognized genetic syndrome.
Anatomical Characteristics
Laterality of microtia involvement (left, right, or bilateral) did not differ significantly between isolated and familial cases (P = .934). Differences were observed in the severity of microtia, particularly in the right ear. While no significant differences were found in left ear microtia grading (P = .483), right ear grading differed significantly between groups (P = .003). Grade 1 microtia was more frequent in familial cases (26.7%) compared with isolated cases (11%), whereas Grade 3 microtia was more prevalent among isolated cases (73.6%) than familial cases (40%). External auditory canal stenosis was observed in 25.52% of left ears and 35.62% of right ears. No statistically significant differences were identified between isolated and familial microtia for left ear canal status (P = .526) or right ear canal status (P = .470). Associated minor auricular findings were analyzed separately from microtia grading and were not considered diagnostic criteria for microtia or indicators of microtia severity. A significant difference was observed in the presence of auricular nodules, or mamelons, in the left ear (P = .024). Mamelons were present in 18.75% of isolated microtia cases compared with 2.94% of familial cases. No significant difference was found for right ear mamelons (P = .831). Preauricular sinus was also recorded as an associated anatomical finding and did not differ significantly between isolated and familial cases in either the left ear (P = .750) or right ear (P = 1.000). Other anatomical variables, including ear implantation and auditory function by ear, did not differ significantly between groups. Regarding phenotypic classification, a statistically significant difference was observed for phenotype 1 (P = .010). Some phenotypes, such as phenotype 2, were observed exclusively in familial cases, although overall frequencies were low.
Logistic Regression Analysis
Multivariate logistic regression analysis demonstrated a statistically significant association between the presence of left ear auricular nodules and isolated microtia (P = .045). The odds ratio was 8.07 (95% CI: 1.05-62.24), indicating that patients with isolated microtia were more likely to present auricular nodules in the left ear compared to those with familial microtia.
The complete multivariate logistic regression model is presented in Table 4 and visually summarized in Figure 2. In this model, male sex was significantly associated with higher odds of isolated microtia (OR = 2.85; 95% CI: 1.11-7.34; P = .030), whereas positive family history was associated with lower odds of isolated microtia (OR = 0.14; 95% CI: 0.04-0.49; P = .002), consistent with its relationship to familial cases. Right-ear Grade 4 microtia was also associated with lower odds of isolated microtia (OR = 0.05; 95% CI: 0.003-0.82; P = .036). Left auricular nodules, or mamelons, remained significantly associated with isolated microtia (OR = 8.07; 95% CI: 1.05-62.24; P = .045). Other variables, including age, hearing disability, hearing device use, and most microtia grade categories, were not statistically significant in the adjusted model. Figure 2 illustrates the direction and magnitude of these associations, with odds ratios greater than 1 indicating higher odds of isolated microtia and values below 1 indicating higher odds of familial microtia. Auricular nodules were analyzed as associated anatomical findings and were not considered diagnostic criteria or indicators of microtia severity.
Multivariate Logistic Regression Model for Factors Associated With Isolated Microtia.
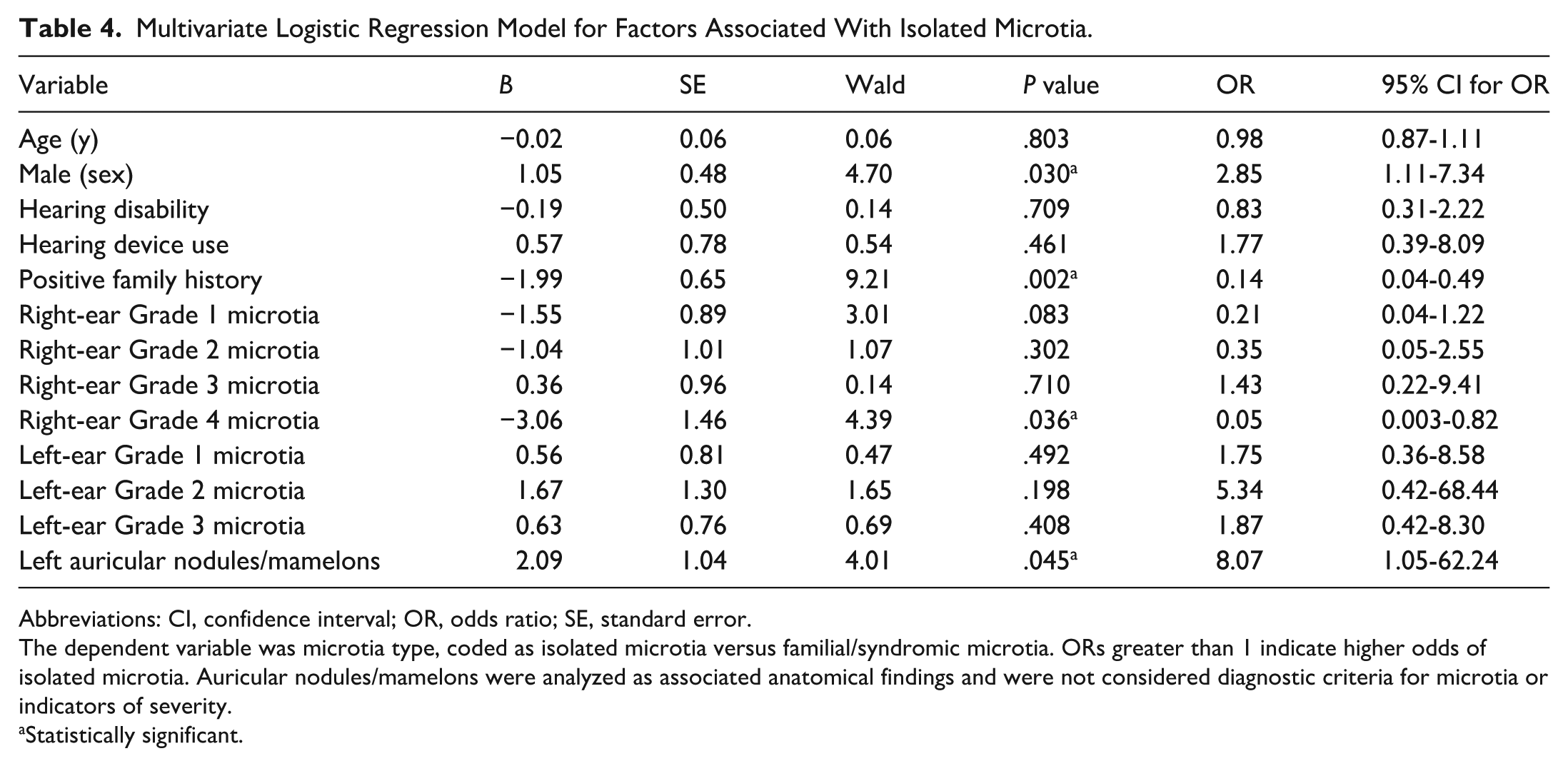
Abbreviations: CI, confidence interval; OR, odds ratio; SE, standard error.
The dependent variable was microtia type, coded as isolated microtia versus familial/syndromic microtia. ORs greater than 1 indicate higher odds of isolated microtia. Auricular nodules/mamelons were analyzed as associated anatomical findings and were not considered diagnostic criteria for microtia or indicators of severity.
Statistically significant.
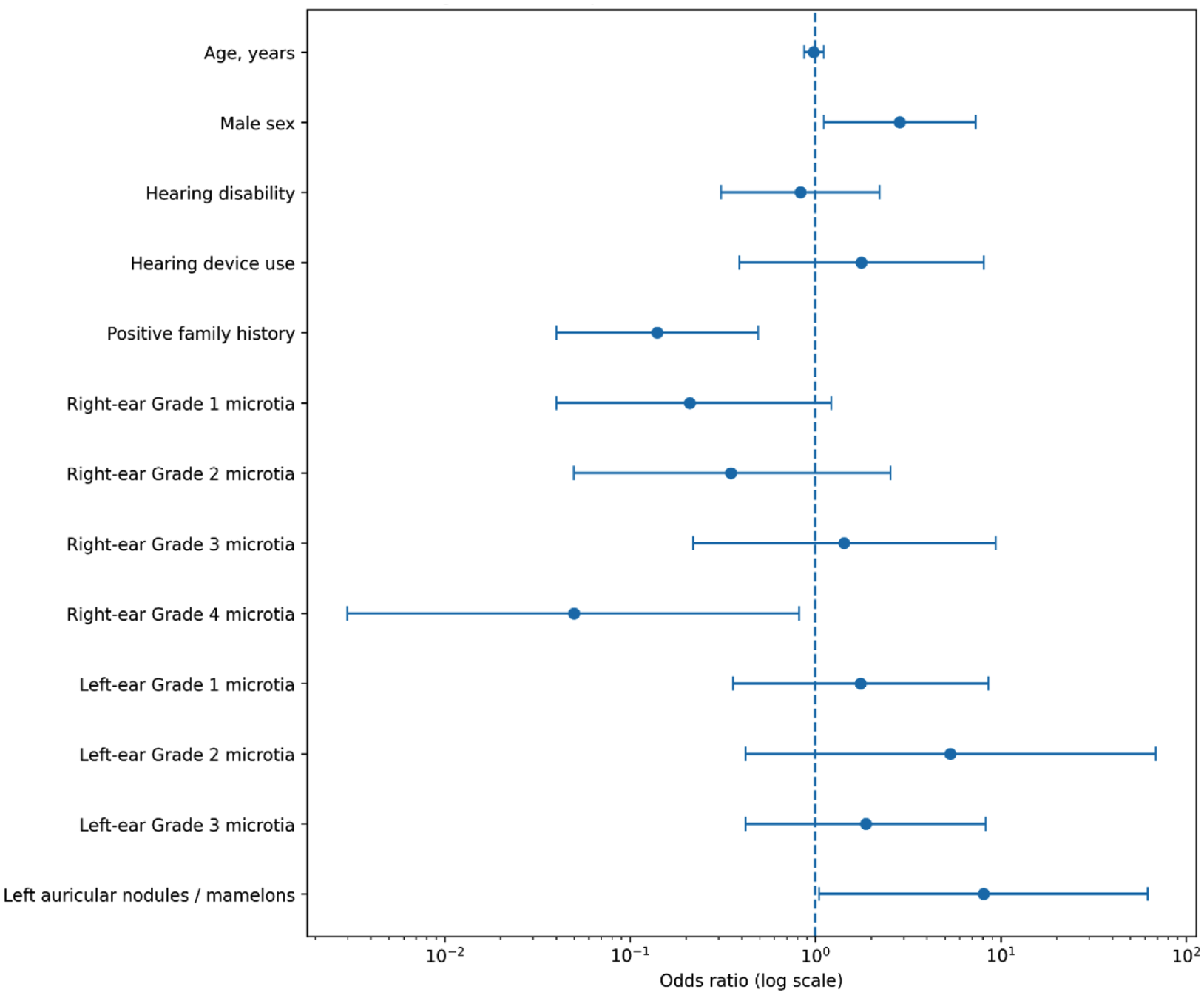
Forest plot of factors associated with isolated microtia. Odds ratios and 95% confidence intervals are shown for demographic, clinical, and anatomical variables included in the multivariate logistic regression model. Odds ratios greater than 1 indicate higher odds of isolated microtia, whereas values below 1 indicate higher odds of familial microtia. Auricular nodules, or mamelons, were recorded as associated anatomical findings and were not considered diagnostic criteria for microtia or indicators of severity.
Discussion
The present study provides a comprehensive analysis of the demographic, clinical, and anatomical characteristics of patients with microtia, distinguishing between isolated and familial cases in a high-prevalence population. The findings demonstrate clinically relevant differences between these subtypes, contributing to a better understanding of their potential etiological mechanisms and implications for diagnosis and clinical evaluation.
One of the most notable findings was the significant male predominance observed in isolated microtia cases. This sex disparity suggests a possible genetic or endocrine influence during embryonic development. Previous studies have proposed that craniofacial morphogenesis may be affected by sex-linked genetic factors or hormonal sensitivity, particularly involving retinoic acid signaling pathways. Although the present study was not designed to evaluate hormonal or molecular mechanisms, these findings support the need for future research exploring the role of sex-specific biological factors in auricular development.
Hearing impairment remains a major clinical concern in patients with microtia, regardless of subtype. Despite this, the overall use of hearing devices was low, particularly among familial cases. This may reflect differences in disease severity, access to specialized care, socioeconomic factors, or the presence of syndromic conditions that complicate rehabilitation. Although no statistically significant difference in hearing device use was observed between groups, these findings highlight the importance of improving access to early audiological assessment and individualized intervention strategies. Longitudinal studies would be valuable to assess the progression of hearing loss and the long-term benefits of early auditory rehabilitation.
The higher frequency of positive family history and recognized genetic syndromes among familial microtia cases reinforces the genetic basis of this subgroup. While prenatal and environmental risk factors were evaluated, their distribution did not differ significantly between isolated and familial cases, suggesting that environmental exposures may contribute similarly across both groups. However, the potential role of epigenetic mechanisms, such as DNA methylation influenced by maternal health or environmental exposures, cannot be excluded, and warrants further investigation through genomic and epigenomic approaches.
Anatomical analysis revealed significant differences in microtia severity, particularly in the right ear. Familial cases more frequently presented with Grade 1 microtia, whereas isolated cases were more often associated with severe deformities, especially Grade 3 microtia. These findings suggest that distinct developmental or pathogenic pathways may underlie these subtypes. Familial and syndromic cases may involve broader craniofacial developmental disturbances, whereas isolated cases in this cohort showed a greater tendency toward severe auricular structural deficiency.
A relevant finding was the association between auricular nodules, or mamelons, in the left ear and isolated microtia. Patients with isolated microtia were approximately 8 times more likely to present this associated anatomical finding than those with familial microtia. Importantly, mamelons were analyzed as minor associated auricular findings and were not considered diagnostic criteria for microtia or indicators of microtia severity. Their embryological origin has been related to the development of the auricular hillocks; therefore, their presence may reflect localized variation in external ear development. However, this finding should be interpreted cautiously and validated in larger cohorts before being considered useful for distinguishing isolated from familial microtia.
The multivariate logistic regression model further supports the existence of distinct clinical and anatomical profiles between isolated and familial microtia. Male sex remained independently associated with isolated microtia, reinforcing the possibility that sex-related biological factors may influence susceptibility or expression of non-familial forms. In contrast, positive family history was inversely associated with isolated microtia, as expected, confirming the validity of the clinical classification, and highlighting the relevance of systematic pedigree assessment. The association between left auricular nodules, or mamelons, and isolated microtia persisted after adjustment, suggesting that this finding may reflect localized variation in external ear development. However, mamelons should be interpreted cautiously as associated anatomical findings rather than diagnostic criteria or severity markers. The inverse association observed for right-ear Grade 4 microtia may reflect the small number of anotia cases and should therefore be interpreted with caution. Overall, these adjusted findings strengthen the need for detailed anatomical evaluation, careful family history documentation, and larger studies integrating genetic and population-ancestry data to clarify the mechanisms underlying isolated and familial microtia.
Other minor auricular findings, such as Darwin tubercle, prominent ear, and preauricular sinus, should not be interpreted as part of the microtia spectrum. In this study, they were documented separately as associated anatomical observations because they may coexist with microtia or represent common anatomical variants. Their presence did not modify microtia grading, phenotypic classification, or case definition. This distinction is important to avoid overclassification of normal or common auricular variants as microtia-related defects.
Overall, the phenotypic heterogeneity observed in this cohort supports the concept that microtia includes multiple subtypes with overlapping but distinct clinical and genetic characteristics. Previous studies have identified mutations in genes involved in branchial arch development and transcriptional regulation, further supporting the need for genotype-phenotype correlation studies. Experimental models, including patient-derived induced pluripotent stem cells, may offer valuable insights into the molecular mechanisms underlying auricular development.
Limitations
Several limitations should be acknowledged. First, although the sample size was relatively large for a single-center study, it may not fully represent the entire population of patients with microtia. Second, the non-random, clinic-based recruitment strategy introduces potential selection bias, as patients seeking care may differ from those who do not access specialized services. Third, the cross-sectional design limits causal inference and does not allow evaluation of disease progression or long-term outcomes. Additionally, some data, particularly family history and prenatal risk factors, were self-reported, which may introduce recall bias. Environmental exposures were not comprehensively assessed, and the familial microtia group included patients with heterogeneous genetic syndromes, potentially affecting internal comparability. Nevertheless, these limitations are common in observational studies of rare congenital conditions and do not diminish the clinical relevance of the findings.
Generalizability
The results of this study are likely applicable to other regions within Ecuador and, with caution, to populations with similar genetic backgrounds or environmental exposures. Given the high prevalence of microtia in high-altitude regions, these findings may be particularly relevant to Andean and other mountainous populations.
Conclusion
This study demonstrates distinct demographic, clinical, and anatomical differences between isolated and familial microtia. The male predominance and greater severity observed in isolated cases, together with the association between auricular nodules and isolated microtia, provide important insights into the heterogeneity of this condition. Importantly, auricular nodules were analyzed as associated anatomical findings and should not be interpreted as diagnostic criteria or indicators of microtia severity. These findings underscore the importance of detailed anatomical evaluation, genetic counseling, and individualized clinical assessment. Future research should prioritize genetic and epigenetic analyses, as well as longitudinal studies assessing auditory, developmental, and surgical outcomes. Improved understanding of microtia subtypes will enhance diagnostic precision and support the development of individualized treatment strategies, ultimately improving outcomes for affected patients.
Footnotes
Abbreviations
BOR – Branchio-oto-renal syndrome
CI – Confidence interval
IQR – Interquartile range
OR – Odds ratio
SE – Standard error
Ethical Considerations
It was granted by the Institutional Review Board (IRB) of the Universidad Tecnológica Indoamérica, coded UTI-DPS-IRB 027-2025, on May 23, 2025.
Consent to Participate
All participants voluntarily provided information and signed an informed consent form.
Consent for Publication
All participants voluntarily provided information and granted their permission for publication.
Author Contributions
FG.-A, FC, P.E.O.-C., G.A.-R., and H.V. developed the research protocol and design, data collection, statistical analysis, evaluation, data interpretation, critical analysis, discussion, writing, and final approval of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that supports this manuscript is and will remain stored by the authors; access to it will be made upon reasonable request.