
Abstract
Background:
Endoscopic repair of craniosynostosis has emerged as a common surgical option due to its minimally invasive nature and safety profile. However, its indications related to patient age necessitate early diagnosis and referral, potentially exacerbating access disparities among socioeconomically and racially marginalized populations. To evaluate demographic, socioeconomic, and hospital-related factors influencing the utilization of endoscopic versus open craniosynostosis repair in a national inpatient cohort.
Methods:
A retrospective analysis was conducted using the National Inpatient Sample (2018-2021). Patients undergoing craniosynostosis repair were categorized by surgical approach (endoscopic vs open). Demographic, socioeconomic, and hospital characteristics were compared using chi-square tests and binary logistic regression.
Results:
From a sample of 1099 patients, 183 (16.6%) underwent endoscopic repair. Endoscopic patients were significantly more likely to be under 1-year-old, White, privately insured, and from high-income zip codes (P < .001 for all). Endoscopic procedures were more frequently performed at private, not-for-profit hospitals (P = .029), and less frequently at government, nonfederal hospitals (adjusted P = .048). Disparities persisted in a subgroup analysis of patients under 1 year.
Conclusion:
Significant racial, socioeconomic, and institutional disparities exist in access to endoscopic craniosynostosis repair in the United States. These disparities persist even among clinically eligible patients, suggesting systemic barriers in early diagnosis and referral. Efforts to expand equitable access must address both social determinants and structural healthcare inequities to ensure timely, optimal care for all patients.
Introduction
Craniosynostosis affects approximately 5.9 in 10 000 live births globally, with a wide spectrum of clinical manifestations and sequalae including abnormal cranial morphology, intracranial hypertension, and neurodevelopment impairment. 1 Surgical intervention remains the gold standard for treatment, typically performed within the first year of life to leverage the malleability of the infant skull and minimize long-term sequelae.2-4 Traditionally, open cranial vault remodeling has been the mainstay of surgical correction, but the introduction of endoscopic-assisted repair in the late 20th century has provided a less invasive alternative for eligible infants. Endoscopic techniques are associated with certain perioperative advantages compared to open repair, including decreased operative time, reduced intraoperative blood loss, lower transfusion rates, and shorter hospital stays; esthetic outcomes are comparable between approaches when postoperative helmet therapy compliance is maintained.5-12 These benefits have led to a growing preference for endoscopic approaches in eligible patients, particularly in high-volume academic centers with the necessary expertise and infrastructure.
However, the efficacy for endoscopic-assisted suturectomy falls with increasing age, necessitating surgical intervention before 6 months of age in patients with sagittal synostosis and 3 to 4 months in other synotoses.13-18 This narrow window for intervention necessitates early diagnosis and referral to a pediatric craniofacial specialist—steps that are not equitably accessible to all patients. Numerous studies have highlighted that children from socioeconomically disadvantaged backgrounds, those with public insurance, and those from racially and ethnically marginalized groups are more likely to experience delays in diagnosis and treatment.19-22 These delays often push patients beyond the age threshold for endoscopic repair, leaving open surgery as the only viable option, despite its increased risks and longer recovery. Additionally, structural barriers such as limited access to specialty care, geographic distance from craniofacial centers, parental language barriers, and inadequate prenatal or pediatric screening exacerbate the likelihood of late presentation in these populations. As a result, disparities in the utilization of endoscopic versus open craniosynostosis repair may not reflect differences in clinical eligibility, but rather broader systemic inequities in healthcare access and delivery.
The consequences of these disparities extend beyond the surgical procedure itself. Delayed open repair of craniosynostosis has been linked to higher rates of complications, increased need for revision surgery, and potentially poorer neurodevelopmental and psychosocial outcomes over time.23-27 Moreover, families of children undergoing open repair often face increased financial burdens due to longer hospital stays, extended recovery periods, and higher associated costs of care. 9 These financial and emotional strains are magnified in low-income families, contributing to a cycle of disadvantage that begins with unequal access to timely and effective treatment. While isolated studies have examined specific demographic or institutional factors influencing surgical approach, comprehensive national data evaluating the intersection of race, socioeconomic status, and hospital characteristics remain limited. The present study explores this gap by utilizing the National Inpatient Sample (NIS), a large, all-payer inpatient database, to assess demographic, socioeconomic, and hospital-related predictors of surgical approach in craniosynostosis management. By doing so, this study aims to identify modifiable factors contributing to disparities in surgical treatment of craniosynostosis and inform targeted interventions to promote equity in pediatric craniofacial surgery.
Methods
Patient Selection
The present study retrospectively reviewed data from the National Inpatient Sample (NIS), part of the Healthcare Cost and Utilization Project (HCUP), from 2018 to 2021. The NIS is the largest publicly accessible all-payer inpatient database in the United States, capturing discharge data from approximately seven million hospitalizations annually across 48 states and the District of Columbia, representing around 98% of the U.S. population. 28 Patients included in the analysis were identified using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes corresponding to craniosynostosis diagnoses, as well as ICD-10 Procedure Coding System (ICD-10-PCS) codes for surgical interventions related to craniosynostosis (Appendix A). Cases were categorized based on surgical technique into endoscopic/percutaneous and open approaches. This study was deemed exempt from review by the institutional review board.
Variable Collection
Demographic variables included patient sex, age at admission (<1, 1, 2, 3, 4, ≥5), race (White, Black, Hispanic, Asian or Pacific Islander, Native American, other, missing), primary payer status (Medicare, Medicaid, private, self-pay, missing), and median household income for patient zip code (Q1: 0-25th percentile, Q2: 26th-50th percentile, Q3: 51st-75th percentile, Q4: 76th-100th percentile). Key cohort and hospital characteristics included hospital bedsize (small: 1-49 for rural, 1-99 for urban, nonteaching, 1-299 for urban, teaching; medium: 50-99 for rural, 100-199 for urban, nonteaching, 300-499 for urban, teaching; large: 100+ for rural, 200+ for urban, nonteaching, 500+ for urban, teaching), hospital location/teaching status (rural, urban nonteaching, urban teaching), and hospital control (government, nonfederal; private, not-for-profit; private, investor owned). Frequencies and means were calculated as appropriate.
Data Analysis
All analyses were performed using IBM SPSS Statistics, version 29.0. National estimates were produced using NIS-provided sampling weights, accounting for complex survey design. Group comparisons of categorical variables were evaluated with Pearson chi-square tests. Binary logistic regression was used to evaluate differences in hospital size, hospital location/teaching status, and hospital control between surgical approaches, adjusting for demographic characteristics that showed significant variation between groups. Statistical significance was determined using a 2-tailed P value threshold of .05.
Results
A total of 1099 patients who underwent surgical treatment for craniosynostosis were identified from 2018 to 2021, including 183 who underwent endoscopic procedures and 916 who underwent open repair (Table 1). Overall, 35.1% of the patients were female and 67.9% were under the age of 1 year. Most patients were also White (51.8%) and on Medicaid (50.0%). Included hospitals mostly had large bedsizes (62.6%), were in urban, teaching environments (98.7%), and were private, not-for-profit (88.8%). Statistically significant demographic, socioeconomic, and hospital-related differences were observed between the 2 groups:
Demographic Variables for Endoscopic and Open-Approach Craniosynostosis Groups, Univariate Analysis.

Demographic Characteristics
Patients undergoing endoscopic repair were significantly younger, with 100% under the age of 1, compared to only 61.5% in the open group (P < .001). No patients older than 1 year received endoscopic surgery. Of the endoscopic patients, 67.8% were White compared to 48.6% in the open group (P < .001), and significantly fewer endoscopic patients identified as Asian or Pacific Islander (0% vs 3.3%, P = .013). Endoscopic patients were more likely to have private insurance (60.1% vs 37.7%, P < .001) and less likely to be insured by Medicaid (34.4% vs 53.2%, P < .001). Patients undergoing endoscopic repair were also more likely to reside in zip codes within the highest income quartile (37.2% vs 24.6%, P < .001) and less likely to reside in areas corresponding with the lowest income quartile (12.6% vs 22.1%, P = .004).
Hospital Characteristics
Endoscopic procedures were more likely to be performed at private, not-for-profit hospitals (93.4% vs 87.9%, P = .029; Table 2). In the adjusted binary logistic regression analysis, treatment at private, not-for-profit hospitals was significantly associated with undergoing endoscopic surgery (OR = 2.41, 95% CI: 1.19-4.33, P = .013), whereas treatment at government, nonfederal hospitals was inversely associated (OR = 0.45, 95% CI: 0.21-0.99, P = .048; Table 3). Hospital bed size and teaching status were not significantly associated with surgical approach after adjustment (P > .05).
Hospital Characteristics for Endoscopic and Open-Approach Craniosynostosis Groups, Univariate Analysis.

Hospital Characteristics for Endoscopic and Open-Approach Craniosynostosis Groups, Binary Logistic Regression Analysis.

Subgroup Analysis of Patients Under 1 Year of Age
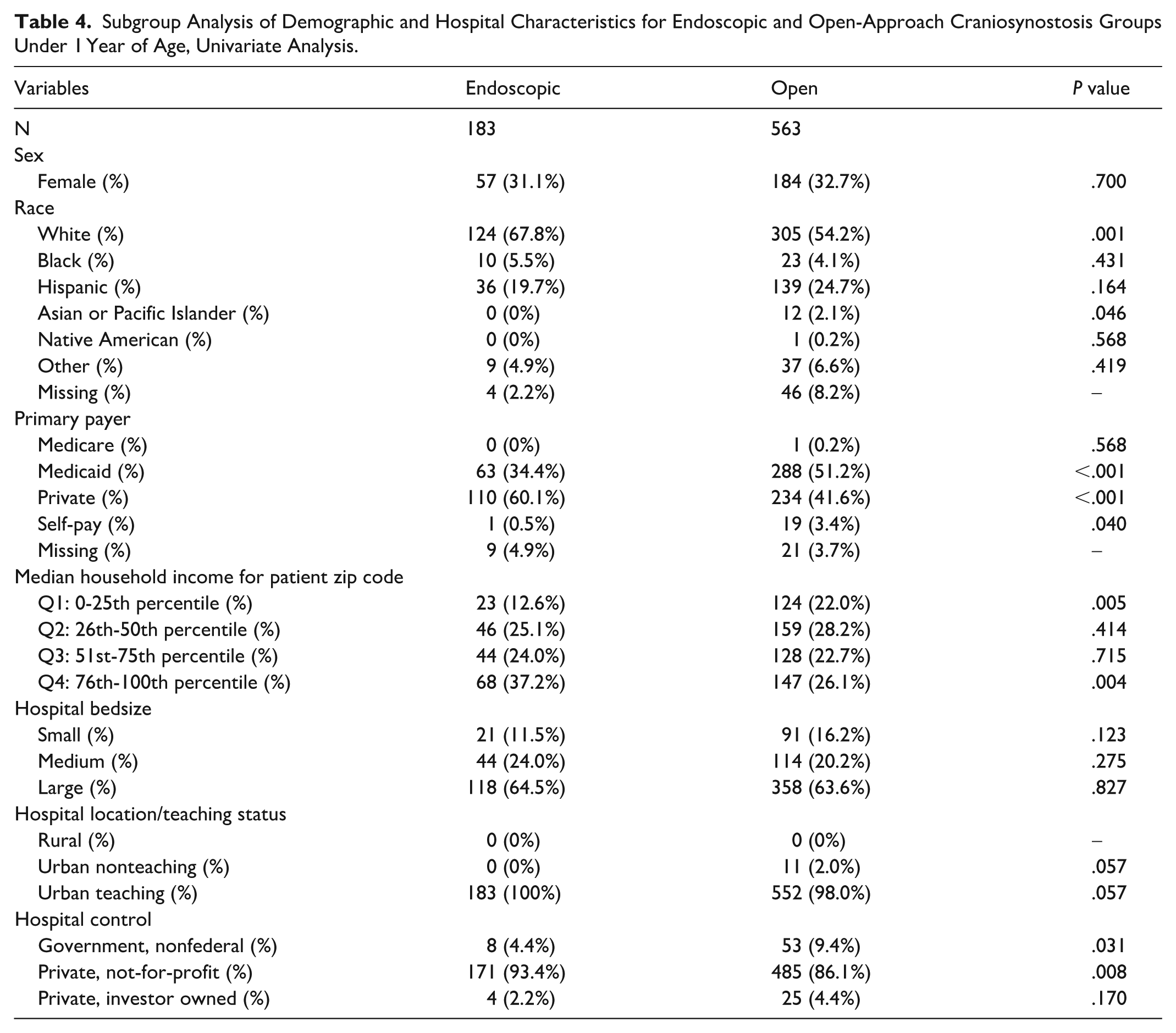
In the subgroup analysis of patients under 1 year of age (n = 746), White patients comprised a significantly larger portion of the endoscopic group compared to the open group (67.8% vs 54.2%, P = .001; Table 4), while patients of Asian or Pacific Islander descent were underrepresented (0% vs 2.1%, P = .046). Endoscopic patients were more likely to have private insurance (60.1% vs 41.6%, P < .001) and less likely to have Medicaid (34.4% vs 51.2%, P < .001). Patients residing in zip codes associated with the highest income quartile were more likely to undergo endoscopic repair (37.2% vs 26.1%, P = .004), and those in the lowest quartile were underrepresented (12.6% vs 22.0%, P = .005). Hospital control remained a significant factor in this subgroup. Endoscopic procedures were more commonly performed at private, not-for-profit hospitals (93.4% vs 86.1%, P = .008), while patients treated at government, nonfederal hospitals were more likely to undergo open repair (9.4% vs 4.4%, P = .031).
Subgroup Analysis of Demographic and Hospital Characteristics for Endoscopic and Open-Approach Craniosynostosis Groups Under 1 Year of Age, Univariate Analysis.
Discussion
The use of endoscopic approaches to manage craniosynostosis has steadily increased in recent years, rising from 3.8% in 2013 to over 13% in 2019. 29 This increase reflects the well-recognized, favorable operative profile of endoscopic treatment for craniosynostosis, which is prevalent in the literature. Compared to open surgery, previous studies have found significantly decreased operative times, lengths of hospital stays, and use of operative materials leading to superior perioperative outcomes for endoscopic techniques, including lower transfusion rates and reduced intraoperative blood loss.5,10,29-32 These perioperative differences, while meaningful, should be interpreted in the context of the additional burden of postoperative helmet therapy required following endoscopic repair, which carries its own demands in terms of family compliance, cost, and access to orthotist services. Studies also describe significantly lower total costs and complication rates associated with endoscopic repair of craniosynostosis. 7 It should be noted that these cost comparisons reflect hospital-level expenditures and do not account for the family-level financial burden of postoperative helmet therapy, including the costs of the helmet device, orthotist visits, and associated time and transportation demands, which may substantially offset hospital-level savings for families.
The present study evaluated access to endoscopic and open surgical approaches in the management of craniosynostosis, leveraging a large national database. The authors found that endoscopic procedures may be less accessible to craniosynostosis patients from marginalized backgrounds, as multiple demographic and socioeconomic disparities were revealed between patients undergoing endoscopic and open surgical treatment. Specifically, patients treated endoscopically were significantly more likely to have private insurance, be treated at private, not for profit hospitals, reside within zip scodes corresponding to the highest median household income quartile, and identify as White when compared to patients treated with open surgery. 33
These socioeconomic disparities are heavily corroborated by existing literature. Mozaffari et al found that patients treated by endoscopic craniectomy were more than twice as likely to reside in zip codes associated with the highest income quartile and have private medical insurance, while Stanbouly et al reported that those with private medical insurance were significantly more likely to undergo endoscopic repair compared to open surgery.34,35 The present study also found that patients treated by open surgery were significantly more likely to be insured through Medicaid compared to those treated endoscopically, which was also a finding reported by Stanbouly et al. These studies and many others highlight the fact that the harm of decreased access to endoscopic treatment for patients from marginalized backgrounds is further compounded by the perioperative advantages of endoscopic intervention, which, when accessible and supported by adequate helmet therapy compliance, may offer meaningful short-term clinical benefits compared to open surgery.
Given the present study’s findings of significant socioeconomic (insurance provider, hospital type, median household income by zip code) and racial disparities between patients undergoing endoscopic and open surgical treatment for craniosynostosis, these favorable outcomes for endoscopic repair are therefore less attainable for patients from marginalized backgrounds. One study by Wallace et al found that Hispanic patients had the highest rates of open operations, and that Hispanic and non-White patients experienced longer operative times and hospital length of stays relative to White/non-Hispanic patients, although this did not reach statistical significance. 22 Less favorable outcomes in craniosynostosis repair for patients from disadvantaged groups were also reported by many other studies, citing metrics such as higher complication rates, hospital charges, and blood transfusions, as well as longer operative times, anesthesia duration, and hospital length of stay.21,36
Given that the overwhelming majority of craniosynostosis procedures—particularly endoscopic repairs—are performed before 1 year of age, the present subgroup analysis of patients under 12 months provides critical insight into disparities that exist even when controlling for age eligibility. In this study, 100% of endoscopic cases occurred in patients under 1 year old, reflecting current treatment guidelines and surgical preferences that favor endoscopic intervention within the first 3 to 6 months of life due to optimal bone pliability and craniofacial growth patterns.7,37,38 By limiting the analysis to this age group, the persistence of racial, socioeconomic, and hospital-related disparities suggests that factors beyond clinical eligibility—such as access to specialized care, insurance coverage, and referral timing—may continue to drive inequities in the utilization of endoscopic techniques. These findings underscore the need for practitioner-level interventions, including increased education and outreach to referring pediatricians and community providers, to promote earlier recognition and referral for evaluation, which may help reduce disparities in access to endoscopic repair. Additionally, targeted educational outreach to primary care physicians, including those practicing in minority communities or from underrepresented backgrounds, may help facilitate earlier recognition and referral and mitigate disparities in access to endoscopic repair.
Surgeons performing open surgical repair for craniosynostosis patients >1-year-old implies that patients from low-resource settings without access to prenatal screening or specialized infant care may be at increased risk of being diagnosed with craniosynostosis at a later age, and hence ineligible for endoscopic repair. The systematic review by Amin et al showed that of the 8 studies that analyzed the effect of insurance status on diagnostic timeline, 7 reported that patients with Medicaid experienced delays in presentation and were significantly more likely to undergo surgery at an older age than those with private insurance. 39 Similarly, a study including over 3000 patients by Baker et al found that higher social vulnerability and certain racial groups are correlated with delayed craniosynostosis surgical repair. 40 Delayed diagnosis of craniosynostosis has also independently been associated with worse outcomes. In a study by Blum et al, minority racial and/or ethnic status was found to be a risk factor for delayed presentation and associated increases in incidence of open surgery, complication rates, operative time, hospital length of stay, and hospital charges. 36 More generally, older age at the time of craniosynostosis repair has also been linked to negative outcomes, including but not limited to increased need for revision, worse long term neurologic outcomes, and facial bone asymmetry plus associated sequelae (eg, ocular dystopia and strabismus).41-43 In addition, according to a study by Gandolfi et al, children from minority groups are at increased risk of delayed referral which may further exacerbate patient outcome disparities as a result of healthcare access disparities. 38
However, a few studies counter the findings herein of decreased access to endoscopic craniosynostosis repair for patients from disadvantaged backgrounds and the idea that outcomes may vary by socioeconomic and demographic status based on the precedent of delayed presentation among marginalized groups and subsequent older age at surgery. In a retrospective analysis including 474 patients, Rochlin et al detected no significant outcome disparities by socioeconomic status (household income quartile, insurance provider) or race. 44 A similar study by Brown et al concluded that socioeconomic factors including parental education, insurance type, household income, and referring physician type were not significant predictors of age at consultation for craniosynostosis repair, although a correlation was identified between race and age at consultation. 45 The existing literature outside of these studies as well as the present study support the finding that endoscopic procedures are less accessible to craniosynostosis patients from marginalized backgrounds, but other factors affecting access to craniosynostosis treatment such as primary language, transportation, distance to craniofacial care centers, and religious or cultural beliefs should be considered in future studies.
While the present study agrees with existing research on access to endoscopic versus open surgical craniosynostosis management, it is not without limitations. The heterogeneity of the database and sample, absence of data on syndromic status, lack of patient information on comorbid conditions, and unavailability of specific suture involvement information are limitations inherent to the NIS database, and future studies should utilize databases with a broader range of variables to allow for more nuanced analyses. As the NIS database only includes inpatient data and does not capture patients who may have undergone surgery in outpatient or ambulatory settings, there is potential for selection bias. Additionally, the endoscopic/percutaneous procedural category in this study was defined using ICD-10-PCS codes for percutaneous and percutaneous endoscopic approaches to skull excision, replacement, supplement, and repair. This category may encompass a heterogeneous group of minimally invasive techniques, including endoscopic strip craniectomy and potentially spring-assisted cranioplasty, which cannot be separately isolated within the NIS. Furthermore, helmet therapy following endoscopic repair is not captured in inpatient procedure coding and therefore cannot be confirmed or excluded at the patient level. Future studies utilizing operative databases with more granular procedural data would allow for subgroup analyses by specific technique and would enable assessment of helmet therapy utilization. The NIS also does not provide geographic identifiers below the broad census region level, precluding state- or metropolitan-level analyses that could reveal where disparities in access to endoscopic repair are most pronounced. Future studies utilizing state-level inpatient data or institutional registries are needed to characterize the geographic distribution of these disparities. Importantly, the NIS does not capture age at referral or age at diagnosis, only age at inpatient admission. As such, our interpretation that delayed referral contributes to the observed disparities in access to endoscopic repair is grounded in prior literature documenting later presentation among publicly insured and racially or ethnically marginalized patients, rather than directly measured in the present cohort.38-40 We were similarly unable to determine whether patients who underwent open repair were ineligible for endoscopic treatment due to late presentation or were unable to access it for other reasons. Future studies utilizing institutional or registry data with referral and diagnostic timelines are needed to confirm this mechanism. The present study was also limited by the fact that all patients undergoing endoscopic repair were less than 12 months of age. However, due to current treatment guidelines for craniosynostosis, data including patients undergoing endoscopic repair are not readily available for older patient cohorts. Finally, the study period was restricted to 2018 to 2021 which limits the ability to assess temporal trends in disparities. At the time of analysis and manuscript preparation, these were the most recent NIS data available. Although newer editions have since been released, they were not accessible during the study period, and longer-term studies will be required to determine whether the disparities identified here have changed over time.
Conclusion
The present study underscores the persistent disparities in access to endoscopic versus open surgical treatment for craniosynostosis in the United States. Despite the well-documented benefits of endoscopic repair—including reduced operative times, shorter hospital stays, and lower complication rates—patients from marginalized racial, socioeconomic, and insurance backgrounds remain significantly less likely to receive this advanced intervention. These disparities persist even when accounting for age eligibility, suggesting that non-clinical barriers such as delayed diagnosis, limited access to specialized care, and systemic healthcare inequities contribute to unequal treatment utilization. While some studies challenge the extent of these disparities, the weight of evidence—including the findings of this national cohort—points to a need for targeted strategies to promote equity in craniofacial care. Future research should explore additional barriers such as language, geographic access, and referral patterns, with the ultimate goal of ensuring that all patients, regardless of background, can access timely and optimal surgical care.
Footnotes
Appendix A
Ethical Considerations
Institutional Review Board approval was not required.
Consent to Participate
Consent to participate was not required for this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter J. Taub is a member of the Editorial Board of FACE and did not take part in the peer review or decision making process for this submission.
Data Availability Statement
The data is publicly available through the Agency for Healthcare Research and Quality’s Healthcare Cost and Utilization Project (HCUP) National Inpatient Database (NIS).