
Abstract
Introduction:
Unilateral lambdoid synostosis (ULS) is the rarest form of single-suture craniosynostosis, producing characteristic posterior cranial asymmetry. Although typically described as an isolated defect, recent studies suggest that adjacent minor sutures may also exhibit premature fusion. The purpose of this study is to evaluate the degree of suture fusion and frequency and impact of minor suture involvement in patients with ULS.
Methods:
A retrospective review of 50 patients with ULS computed tomography (CT) scans was performed to assess the degree of lambdoid suture fusion (complete, upper 2/3, lower 2/3) and minor suture involvement. Three-dimensional CT scans were used to determine the impact on craniometric measurements.
Results:
The lambdoid suture fusion distribution was 36% complete, 40% upper 2/3, and 24% lower 2/3. Minor suture synostosis was found in 16% of patients with ULS. The minor sutures involved included 8% with occipitomastoid suture synostosis and 12% with posterior intraoccipital suture synostosis. All patients demonstrated cranial asymmetry, ipsilateral posterior fossa deflection, ipsilateral inferior skull base, and significantly anterior ipsilateral deviation of the petrous ridge, external acoustic meatus, midface, and articular fossa. No significant difference was found in any measurement based on the degree of suture fusion or minor suture involvement.
Conclusions:
The degree of lambdoid suture fusion and minor suture involvement did not significantly impact the degree of craniofacial malformations in ULS. Minor suture involvement was observed in 16% of patients, with posterior intraoccipital suture synostosis being most common.
Introduction
Unilateral lambdoid synostosis (ULS) is the least common form of single-suture craniosynostosis, characterized by occipital flattening, skull base torsion, and compensatory mastoid and facial changes.1-4 The extent of suture fusion in craniosynostosis may play a role in determining the severity of cranial deformity.5,6 Partial fusion may allow limited compensatory growth across the remaining patent suture, resulting in milder craniofacial malformations. In contrast, complete fusion could possibly restrict growth across a larger segment of the posterior vault which may result in a more pronounced deformity among patients with ULS.
Although traditionally regarded as an isolated deformity, recent imaging and morphometric analyses have suggested additional involvement of minor sutures adjacent to the fused lambdoid suture.7,8 Minor suture synostosis, defined as premature fusion of secondary sutures such as the occipitomastoid (OM) or posterior intraoccipital (PIO) sutures, has emerged as an underrecognized feature in both syndromic and non-syndromic craniosynostosis.7-14 These sutures play an important role in cranial base morphology, and their early fusion may accentuate posterior vault deformity or influence compensatory growth patterns.15-17 However, the frequency, distribution, and clinical significance of minor suture fusion in lambdoid craniosynostosis remain poorly characterized.
Identifying patterns in the extent of lambdoid suture fusion and the presence of minor suture involvement could improve our understanding of the pathophysiology of lambdoid craniosynostosis and help explain the variability in clinical presentation and outcomes observed among affected patients. The present study aims to characterize how the extent of lambdoid suture fusion and the prevalence of minor suture involvement in patients with ULS impact the severity of craniofacial malformations. By elucidating these associations, we aim to improve the precision of diagnostic classification and inform targeted surgical strategies for posterior vault deformities.
Methods
A retrospective review of pre-operative 3-dimensional computed tomography (CT) scans of patients diagnosed with ULS between 2010 and 2025 was performed. Approval was obtained from the University of Texas Southwestern Medical Center Institutional Review Board. Patients with syndromic diagnosis, other involved sutures, or any other craniofacial conditions were excluded. All CT scans were reviewed by a pediatric neuroradiologist (TNB) to evaluate the degree of lambdoid suture involvement (Complete, Upper 2/3, Lower 2/3) and for minor suture involvement.
Our group previously described all measurements performed in the current study to evaluate cranial and facial malformations in patients with ULS.3,4 Three-dimensional CT images were rendered using Mimics 26 (Materialise NV, Belgium), and craniometric evaluation was performed utilizing the in-built measurements in 3-Matic (Materialise NV, Belgium) software (Figure 1). To account for age-related variability within the cohort, craniofacial asymmetry was quantified using asymmetry ratios. 4 All ratios were calculated as the contralateral side measurements divided by the ipsilateral side measurements. All images were first registered in the Frankfort horizontal plane.
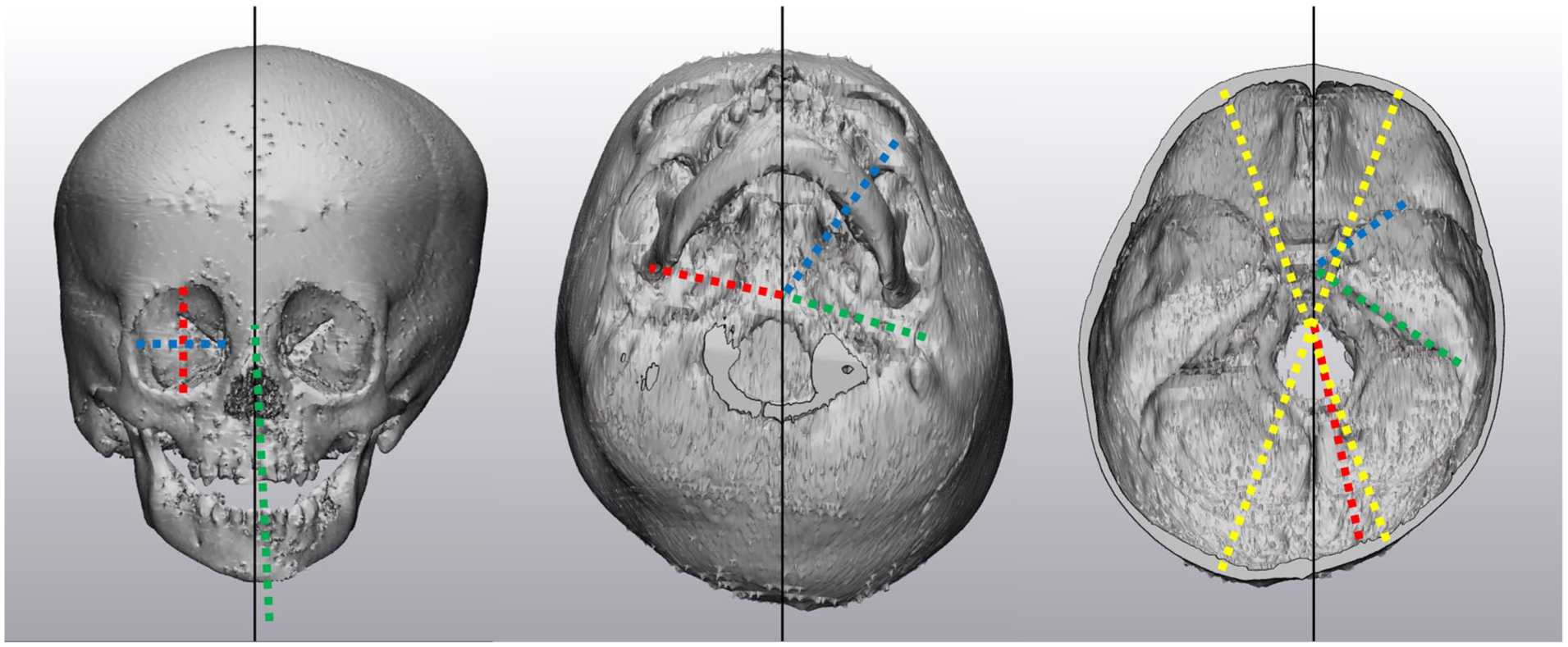
Unilateral lambdoid synostosis craniometric measurements. Left: Orbital height (red), orbital width (blue), and chin deviation (green). Middle: Articular fossa angle (red), midface angle (blue), and external acoustic meatus (green). Right: Cranial asymmetry index (yellow), posterior fossa deflection angle (red), lesser wing sphenoid angle (blue), and petrous ridge angle (green).
Cranial asymmetry index was calculated as the difference between the lengths of the contralateral side distance and ipsilateral side distance at thirty degrees from midline, divided by the contralateral side distance, multiplied by 100 (Figure 1). The posterior fossa deflection angle was defined as the angle formed between the midline and the deviation of the foramen magnum. The skull base angle was measured as the difference from the horizontal line at the most inferior ipsilateral side occiput and the line intersecting the inferior contralateral occiput. The petrous ridge, lesser wing sphenoid, external acoustic meatus, midface asymmetry, and articular fossa angles were measured as the deviation of from these listed landmarks and the midline defined through the glabella and sella turcica. Orbital height and width ratios were calculated as the contralateral side divided by the ipsilateral side. Nasal and chin deviation were measured as the angle deviation from the vertical midline defined through the glabella and anterior nasal spine.
All measurements were performed in duplicate by 2 authors and assessed for inter- and intra-observer reliability using Cohen’s Kappa analysis with strong reliability (k = 0.82; k = 0.83). Two-tailed t-test analyses were performed using SPSS version 29 (IBM Corp., Armonk, NY). Different degrees of lambdoid suture involvement (Complete, Upper 2/3, and Lower 2/3) were compared. Patients with minor suture synostosis were compared to those without. Statistical significance was determined at a value of P < .05. Pearson’s correlation coefficient was used to assess the relationship between age at CT imaging and craniometric measurements.
Results
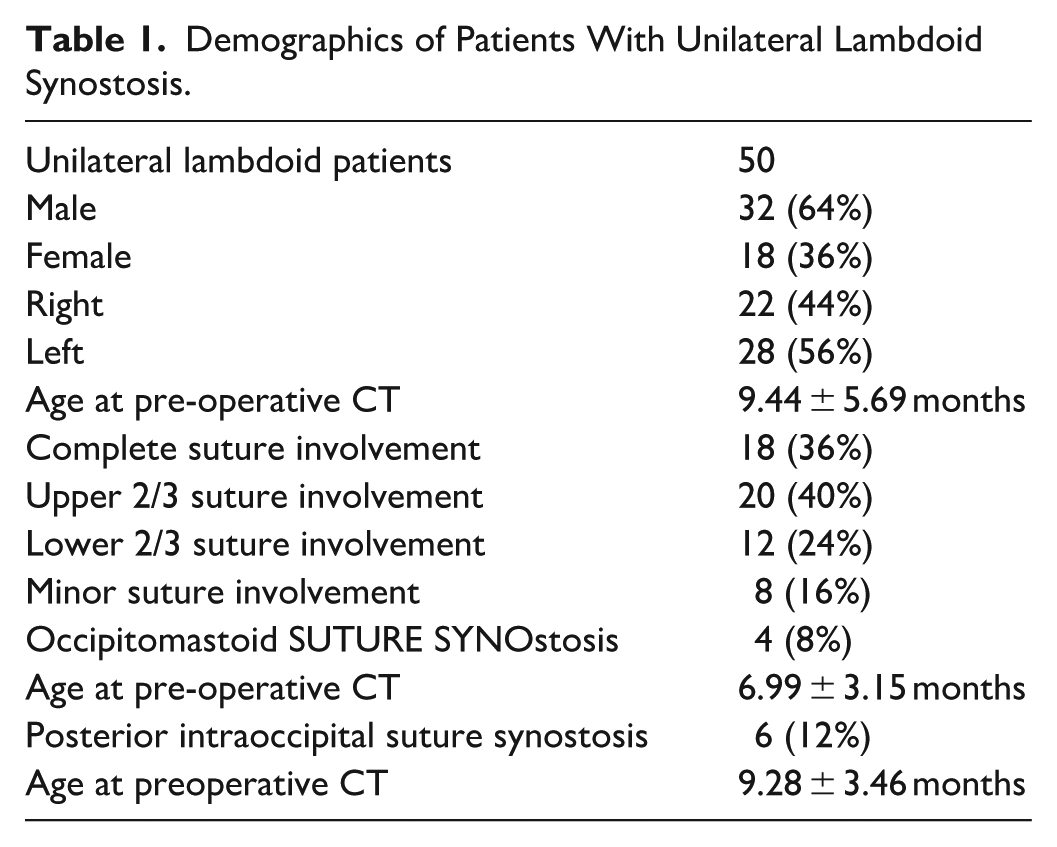
A total of fifty patients with ULS were identified (Table 1). The patients were predominantly male (64%) and had left-sided lambdoid suture involvement (56%). The distribution of suture involvement included 36% complete, 40% upper 2/3, and 24% lower 2/3. Involvement of minor sutures was identified in 16% of patients overall. 8% of the cohort displayed occipitomastoid suture synostosis, and 12% showed posterior intraoccipital suture synostosis. Two of these patients had fusion of both sutures. No involvement of the petro-occipital, anterior intraoccipital, spheno-occipital, or any other minor suture synostosis was identified. There was no association found between the degree or location of suture fusion and minor suture synostosis.
Demographics of Patients With Unilateral Lambdoid Synostosis.
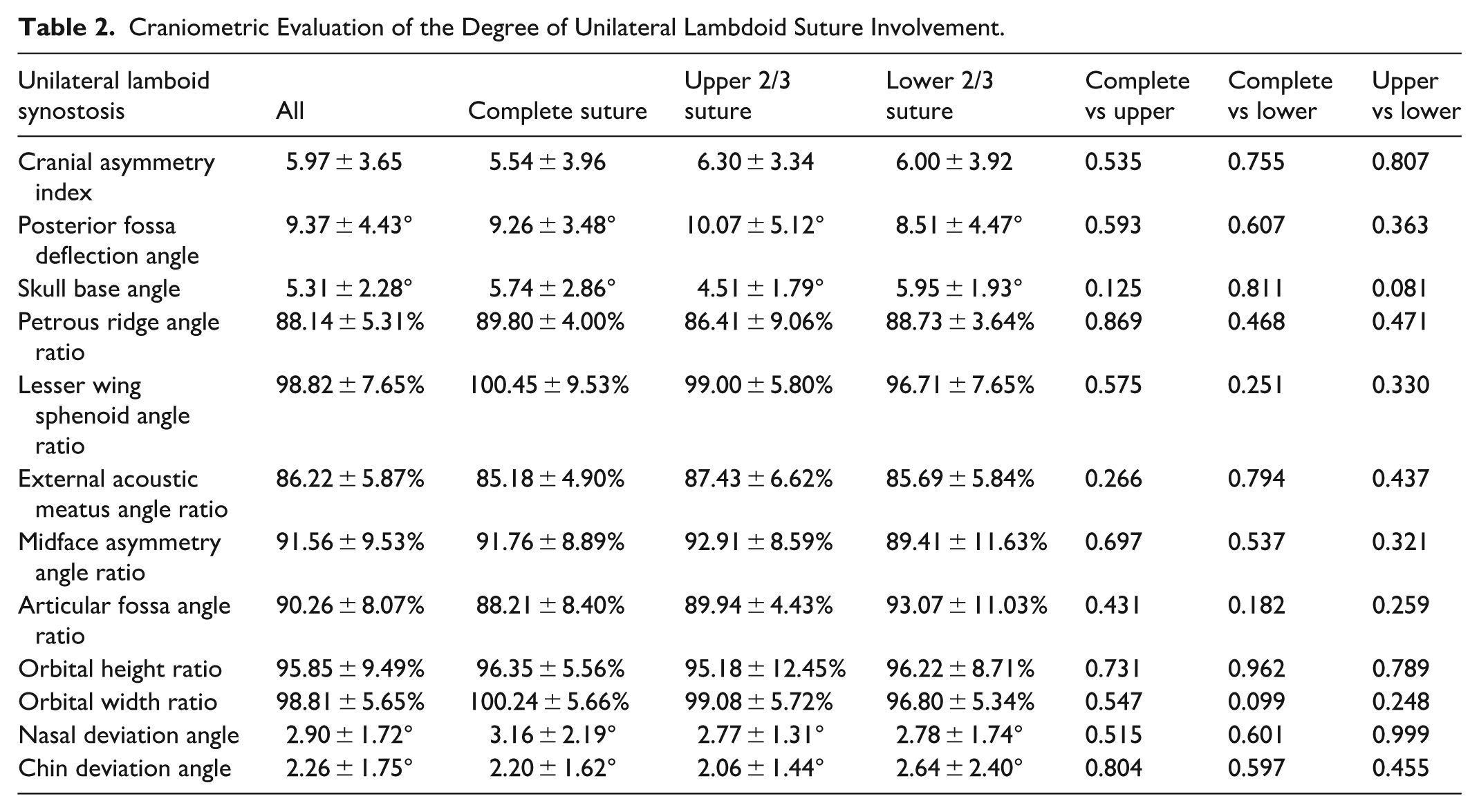
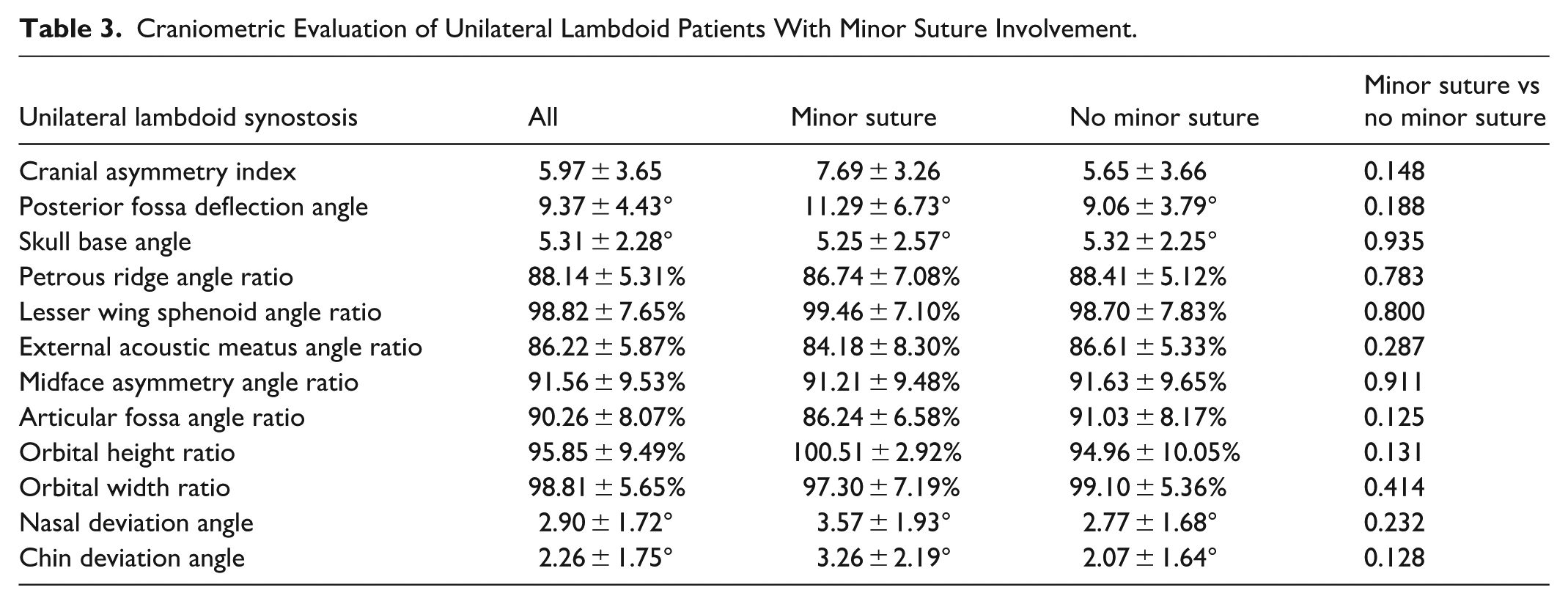
All groups demonstrated significant cranial asymmetry index scores (Table 2). The posterior fossa was deflected between 8 and 10 degrees to the ipsilateral side in all groups. The skull base was deviated inferiorly on the ipsilateral side between 4 and 5 degrees compared to the contralateral side. The petrous ridge was significantly more anteriorly deviated on the ipsilateral side (P < .001). The lesser wing of the sphenoid angle did not demonstrate a significant difference between the 2 sides. The external acoustic meatus was significantly more anteriorly deviated on the ipsilateral side in all groups (P < .001). Both the midface and articular fossa of the mandible were significantly more anteriorly deviated on the ipsilateral side (P < .001; P < .001). Orbital height and width did not differ significantly between sides. The nose and chin were found to deviate towards the contralateral side, each by between 2 and 3 degrees. No significant difference was found in any craniometric measurement based on the extent of lambdoid suture involvement (Table 2) or presence of minor suture involvement (Table 3). No moderate or strong correlation was found between age at CT and any craniometric measurements (r < 0.3).
Craniometric Evaluation of the Degree of Unilateral Lambdoid Suture Involvement.
Craniometric Evaluation of Unilateral Lambdoid Patients With Minor Suture Involvement.
Discussion
ULS produces complex 3-dimensional cranial and cranial base asymmetries that can impact both posterior and anterior craniofacial structures.1-4 In this cohort, variation in the degree of lambdoid suture fusion, whether complete or partial, did not significantly affect the extent of craniofacial deformity. Similarly, minor suture involvement varied but was not associated with increased morphologic severity. These findings suggest that while ULS produces a consistent pattern of posterior and cranial base distortion, the overall degree of deformity may be driven more by the intrinsic growth mechanics than by the completeness of fusion or the involvement of adjacent minor sutures.
All patients demonstrated consistent cranial base torsion, anterior petrous ridge deviation, and anterior displacement of the ipsilateral midface and articular fossa, findings corroborated by prior 3-dimensional analyses of ULS.2-4 These findings reinforce the theory that ULS affects the cranial base, resulting in translational shifts and alterations in the facial skeleton. The absence of significant orbital or midfacial asymmetry differences between groups suggests that anterior compensatory changes occur uniformly once the posterior vault is affected, regardless of fusion extent or minor suture involvement.
Previous studies have proposed that variation in suture fusion may allow for residual growth across unfused portions, potentially leading to variations in phenotype in other forms of synostosis.5,6 However, our data in ULS did not demonstrate measurable differences in craniometric parameters across varying degrees of lambdoid fusion. This may indicate that once any segment of the lambdoid suture is fused, compensatory growth becomes similarly restricted along the posterior vault. Among the fifty patients in our cohort, 36% had complete suture fusion, which was similar to the findings by Boyaijan et al., who reported a 28.6% rate of complete fusion in 14 patients with ULS. 5
Minor suture involvement was present in 16% of patients, which may suggest that secondary sutures, especially in syndromic craniosynostosis, can exhibit premature fusion in association with primary suture synostosis.7-14 The 2 minor sutures identified were the PIO and OM sutures, which are part of a “lambdoid ring” that extends from the lambdoid sutures. While this structure appears analogous to the coronal ring seen in unilateral coronal synostosis, the presence of minor suture fusion did not produce additional measurable impact on craniofacial morphology.18,19 The PIO suture runs transversely along the posterior skull base, allowing flexibility during birth. It is believed to start fusing around 1 to 2 years of age and be completed by 4 to 7 years.11,16,20-22 In isolation, PIO synostosis has been shown to create a posterior malformation similar to ULS when the lambdoid suture remains patent.16,21,23 Mazzaferro et al. found that 1 of the 5 patients evaluated with ULS had PIO synostosis involvement. 7 The other involved minor suture that was found to be involved in our cohort was OM synostosis, which acts as a connection between the lambdoid and the PIO sutures. OM is believed to begin fusion around 5 years of age and be complete by 12 to 18 years.11,20,22 OM synostosis, in a mixed cohort of patients with synostosis, has been shown by Mizutani et al. to significantly impact the posterior fossa deflection angle; however, these findings were not observed in our ULS cohort. 8
The study is limited by the retrospective design and reliance on imaging obtained at a single preoperative time point. Longitudinal imaging could clarify whether the degree of suture fusion or minor suture involvement influences postoperative remodeling or surgical outcomes. Additionally, although this study represents one of the most extensive series of ULS patients analyzed, the relatively small number of cases limits power for subgroup analysis. While not available in the current study, the impact of the extent of suture fusion and minor suture involvement on Chiari malformations should be analyzed. Future studies incorporating automated shape modeling or finite element analysis may further elucidate how partial suture fusion or minor suture involvement contributes to local strain distribution and bone growth patterns. Lastly, patients with less severe ULS phenotypes may not be detected and therefore may not be represented or analyzed in the current study.
Conclusions
This study demonstrates that the extent of lambdoid suture fusion and the presence of adjacent minor suture synostosis do not significantly alter the craniofacial morphology associated with unilateral lambdoid synostosis. While minor suture involvement was relatively frequent, its impact on overall cranial shape is limited. These findings suggest that the hallmark deformity of ULS results primarily from the anatomic position of the fused lambdoid suture and its effect on posterior vault growth restriction, rather than the completeness of fusion or minor suture participation.
Footnotes
Ethical Considerations
This study was approved and followed the guidelines set by the University of Texas Southwestern Institutional Review Board (STU 032018-067).
Consent to Participate
Written consent was obtained following the guidelines set by the University of Texas Southwestern Institutional Review Board (STU 032018-067).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.