
Abstract
Given COVID-19’s disproportionate impact on populations that identify as Black, Indigenous, and People of Color (BIPOC) in the United States, researchers and advocates have recommended that health systems and institutions deepen their engagement with community-based organizations (CBOs) with longstanding relationships with these communities. However, even as CBOs leverage their earned trust to promote COVID-19 vaccination, health systems and institutions must also address underlying causes of health inequities more broadly. In this commentary, we discuss key lessons learned about trust from our participation in the U.S. Equity-First Vaccination Initiative, an effort funded by The Rockefeller Foundation to promote COVID-19 vaccination equity. The first lesson is that trust cannot be “surged” to meet the needs of the moment until it is no longer deemed important; rather, it must predate and outlast the crisis. Second, to generate long-term change, health systems cannot simply rely on CBOs to bridge the trust gap; instead, they must directly address the root causes of this gap among BIPOC populations.
Introduction
It is widely recognized that COVID-19 has disproportionately affected minoritized populations, particularly Black, Indigenous, and People of Color (BIPOC) communities in the United States, with Hispanic, Black and American Indian and Alaska Native (AIAN) people having higher hospitalization rates, as well as being twice as likely to die from COVID-19, as White individuals. 1 Despite substantial improvements in COVID-19 vaccination equity over the past few years, it remains critical to understand the factors that led to vaccination inequities for BIPOC communities at the start of the vaccine rollout, which have persisted now that booster doses are available to protect against emerging coronavirus variants. 2
Both access barriers 3 and earned mistrust of health systems and health institutions by racially and ethnically minoritized populations have contributed to inequities in COVID-19 vaccination rates.3–5 Widespread low confidence in COVID-19 vaccines among BIPOC communities has led to renewed attention on the perceived lack of trustworthiness of healthcare and health institutions. To bridge this consequential trust gap, there have been calls for health institutions and systems to work with community-based organizations (CBOs) such as local non-profits that address housing, food insecurity, and other community needs, in order to leverage the trust these CBOs have built with communities to promote vaccination. For example, both the US Department of Health and Human Services Office of the Assistant Secretary for Preparedness and Response and the Center for Diseases Control and Prevention’s recommendations for promoting health equity during COVID-19 call for engaging with CBOs and leaders from BIPOC communities in order to facilitate communication with minoritized populations.6,7 However, as health systems increase investment in, and draw on the expertise and experience of, these organizations in reaching underserved populations, it is crucial to highlight broader lessons on trust so that they can be applied to a range of public health challenges.
In this commentary, we offer two key lessons learned about the importance of trust for health equity and provide recommendations for health systems and institutions to consider as they plan future public health initiatives. These lessons are informed by our involvement in the U.S. Equity-First Vaccination Initiative (EVI), a one-year initiative funded by The Rockefeller Foundation(April 2021-April 2022) that supported hyper-local and community-led strategies to reduce racial and ethnic disparities in COVID-19 vaccination among BIPOC populations in five U.S. cities.
8
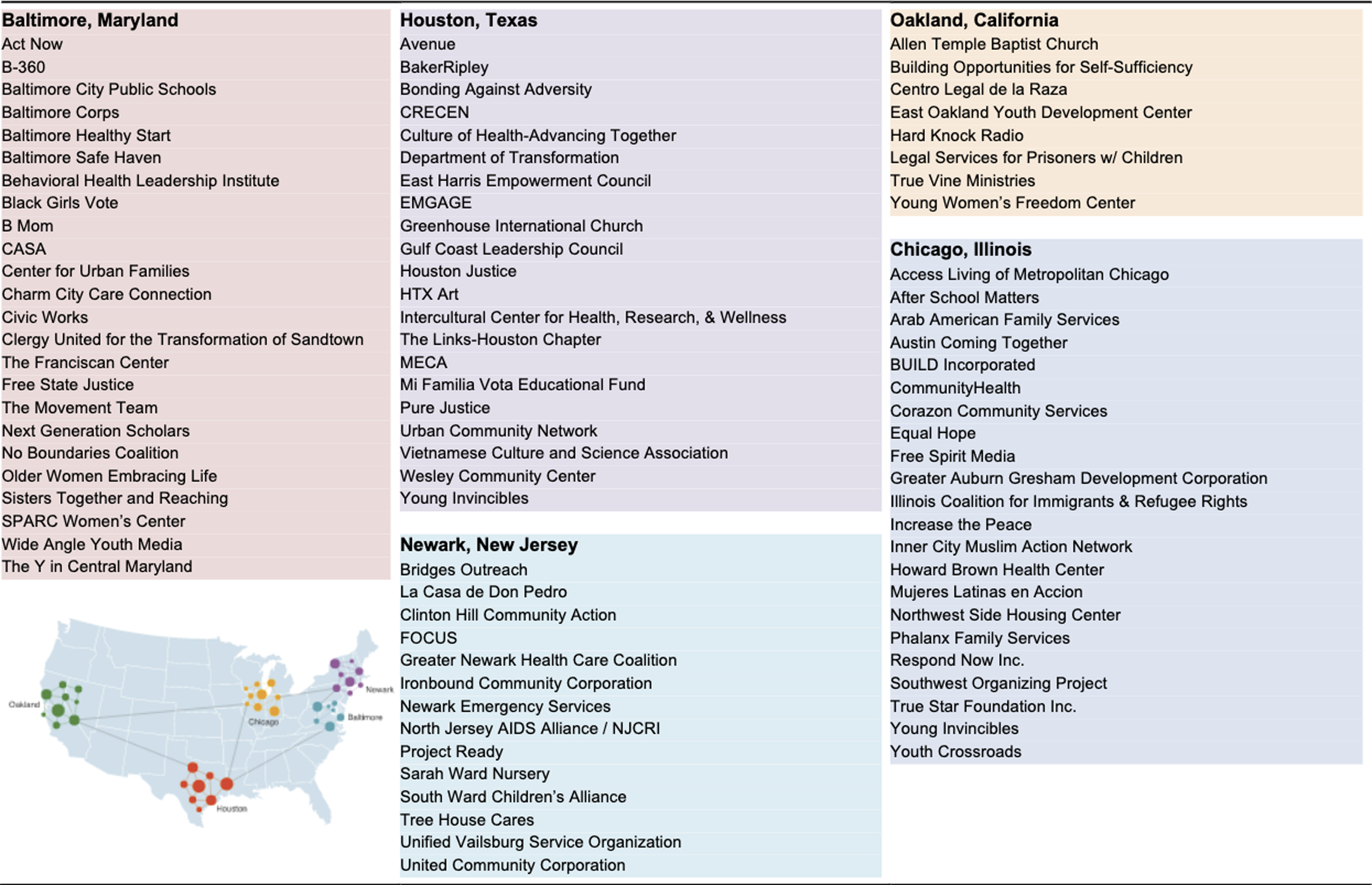
As learning partners in this initiative, we worked collaboratively to support CBOs with research insights relevant to their efforts to promote equitable vaccination in minoritized communities. Nearly 100 CBOs were engaged in the EVI, including faith-based organizations, youth development organizations, and service providers that addressed housing, food insecurity, and other health-related social needs (Figure 1).
9
Most of these organizations were not part of the public health sector as traditionally defined, but they were able to quickly transition to confront their communities’ COVID-19-related needs, harnessing relationships and engaging trusted voices to share trustworthy and accessible information about the COVID-19 and break down barriers to accessing vaccines.
10
Community Based Organizations within the U.S. Equity First Vaccination Initiative. Note: Reproduced from previously published report.
9
Below, we discuss two key lessons on trust derived from this initiative. First, trust cannot be “surged” on demand to meet the needs of the moment until it is no longer deemed important; rather, it must predate and outlast the crisis. Second, to generate long-term change, health systems cannot simply rely on CBOs to bridge the trust gap; instead, they must directly address the root causes of this gap among BIPOC populations.
The Role of CBOs in Bridging the Trust Gap
Before COVID-19 vaccines became widely available, the impact of the ongoing erosion of trust in institutions among BIPOC populations was evident in myths that were propagated about the nature and effects of the SARS-CoV-2 virus. For example, the “Black immunity” myth early in the pandemic incorrectly stated that Black people were less likely to become infected with the virus. 11 Likewise, a related myth claimed that there were no COVID-19 infections in Africa, and another asserted that 5G, (fifth-generation technology for mobile networks) caused COVID-19. 12
As vaccines became available, a history of poor treatment in conjunction with the historical and contemporary ramifications of the complex system of policies and practices that reinforce racial inequity (structural racism) 13 led many BIPOC communities to be suspicious about the COVID-19 vaccines and the efforts to promote vaccination. Healthcare in the United States historically has been shaped by racism, with prominent scientists and medical doctors furthering eugenics. 14 Today, racism continues to perpetuate conditions that put people of color at increased risk for occupational exposure to COVID-19, with inconsistent protections. 15 For example, long term care workers, a disproportionate number of whom are racially and ethnically minoritized, were deemed “essential” workers, but unlike doctors and nurses, were not prioritized for personal protective equipment. 16 In addition, BIPOC populations continue to experience worse access to care 17 and lower quality care. 18 Therefore, those same health systems and institutions that are promoting and delivering COVID-19 vaccines encounter a trust gap that hinder their efforts to increase vaccination rates in communities that experience disproportionate morbidity and mortality from the pandemic. 19
CBOs that work with and in their communities to address health care and health related social needs have built social capital through longstanding relationships, providing a wide range of services and filling gaps in access. These organizations have established trust through rich, authentic relationships, and sustained efforts at meeting the dynamic needs of their communities. Just as patients benefit from continuity of care from a primary care provider, 20 CBOs offer community members continuity of trust through sustained engagement, services, and advocacy during routine times, not just during periods of crises. It has been posited that CBOs operate as non-elected political representatives, authentically representing the interests of lower-resourced communities with government administrators and private funders. 21 Recently, health systems’ efforts to engage with CBOs have yielded promising results. For example, a partnership launched in 2015 between the University of Illinois Hospital and the nonprofit Center for Housing and Health was associated with reductions in emergency room visits and healthcare costs. 22
As the country navigates the ongoing COVID-19 pandemic, some CBOs have benefited from increased recognition of the importance of their work and their position in communities, which has led to increased funding and stronger partnerships with local health institutions. For instance, in response to health inequities created by COVID-19, over the course of one year, a San Francisco Bay Area coalition of community partners and researchers and two local health departments administered over 40,000 COVID-19 tests and 30,000 vaccinations to individuals in BIPOC communities at high risk for COVID-19. These partners ascribed their success both to shared leadership and the fostering of a long-term partnership that will promote health equity beyond the pandemic. 23
Through multi-sector partnerships such as these, CBOs have been able to promote equitable vaccination and healthcare access during the pandemic in large part because they are trusted voices with deep knowledge of their communities. The nearly 100 CBOs that comprised the EVI, for example, worked to mitigate barriers to vaccination through a variety of strategies that included sharing accessible information, arranging transportation, and helping community members with language barriers navigate the healthcare system. 9 These CBOs employed strategies that were important both for the focused goal of increasing vaccination rates and for the broader goal of the EVI, which was to demonstrate how to strengthen the U.S. public health system as a whole.9,24
However, the recent intensification of efforts to engage CBOs in public health efforts should be properly contextualized within a landscape of unequal power dynamics, where engagement between CBOs and health institutions has been temporary, contingent upon funding, and consequently, shallow. 25 In becoming better integrated with health systems and institutions, CBOs gain access to resources, clinical expertise, and legitimacy from more powerful institutions that they may have been deprived of before. 25 These resources are crucial for them to build, strengthen, and sustain their programs, to develop additional capacity, and to rigorously evaluate their outcomes. 25
As the organizations who participated in the EVI shared with us, CBOs need stable and flexible funding, not an influx of resources that then recede when the acute crisis is over. Thus, it is critical to ensure that even as CBOs are supported as they bridge the trust gap during this crisis, they are not called on and then forgotten as the pandemic wanes, diminishing their resources to address persistent inequities in the social determinants of health within their communities. Rather, sustained investment in these productive partnerships with CBOs will serve to strengthen cross-sectoral relationships and build more resilient systems, increasing crisis preparedness and equity for the most minoritized. 26
Furthermore, recommendations to engage with CBOs in reaching minoritized communities implicitly recognize the problematic trust gap but often do not explicitly call for health systems and institutions to work toward becoming more trustworthy themselves. Engaging with CBOs without concerted efforts from health systems and institutions to authentically earn the trust of their communities would be at best, insufficient, and at worst, exploitative of CBOs and the communities they serve. Thus, it is imperative that health systems and institutions take the appropriate steps to demonstrate their trustworthiness rather than being perceived as outsourcing it for expediency.
How Can Health Systems Bridge the Trust Gap With Minoritized Populations?
Figure 2 depicts an overarching framework to bridge the trust gap that health system leaders, healthcare institutions and healthcare providers, could consider adopting. It identifies three broad approaches, taking responsibility for building trust, understanding both historical and contemporary reasons for mistrust, and addressing root causes of the trust gap, and suggests potential strategies within each. These suggested steps are not meant to be exhaustive but constitute a promising starting point for more robust and concrete plans that stakeholders can tailor to their own contexts. Antecedents of Mistrust and Proposed Strategies to Build Trustworthiness. Note: This figure is informed by authors’ synthesis of articles33,36–41 on the roots of vaccination inequity and effective strategies for engaging BIPOC populations, including RAND’s report
9
on lessons learned from participating as a learning partner in the EVI.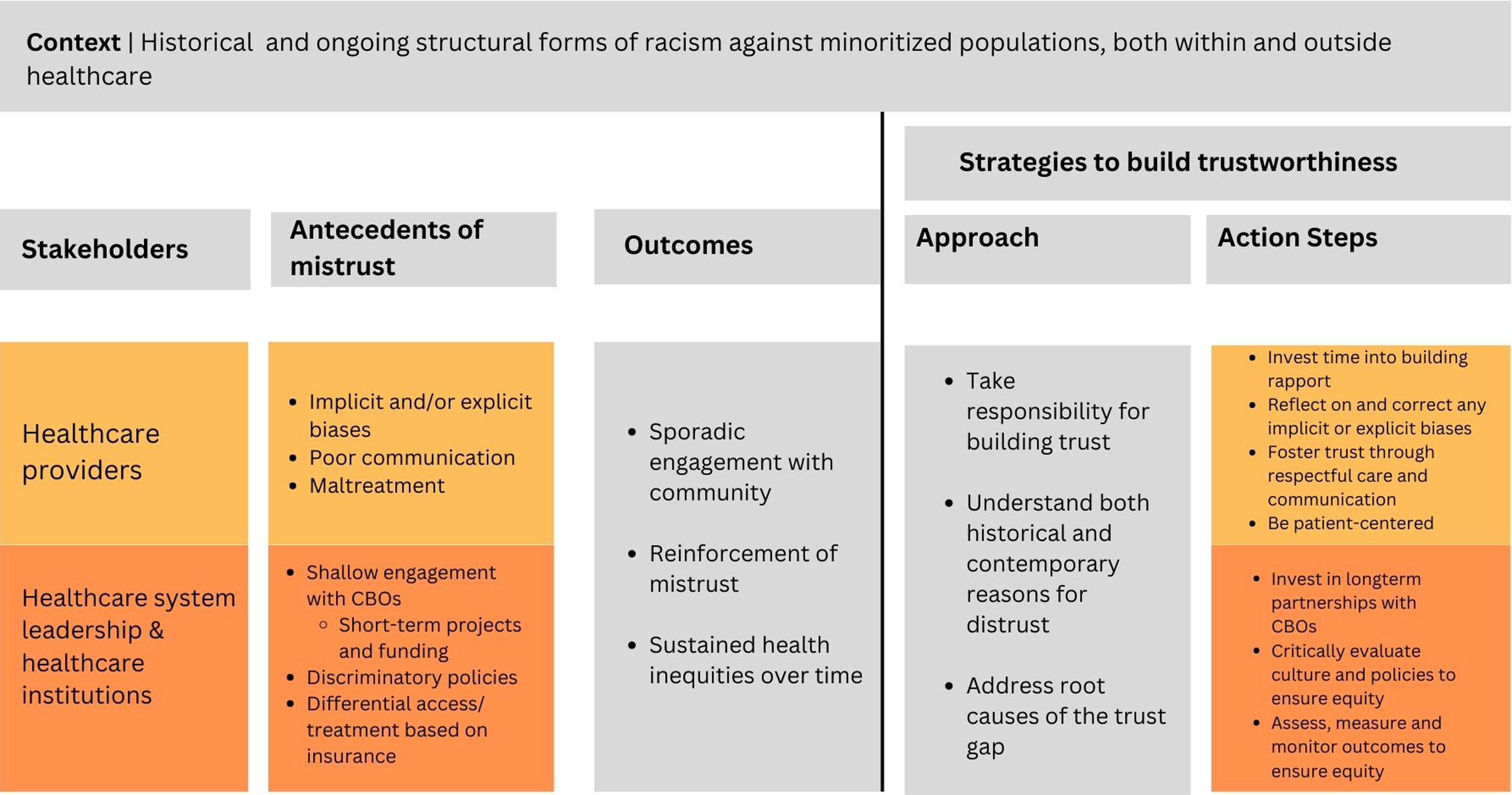
To be effective, these approaches should be grounded in bell hook’s ethic of love, which involves care, commitment, trust, responsibility, respect, and knowledge of self and the other. 27 Hooks also encouraged that individuals learn the truth about how interlocking systems of domination operate, learn to look critically both inward and outward, and learn love in the context of community.27,28
Applying these principles to the context of health equity and trust, stakeholders should begin by having a relational outlook on trust that centers the humanity of BIPOC populations. Grounding health promotion efforts in the humanity of these communities, stakeholders should ensure a robust understanding of how racism directly impacts health inequities, critically reflect on their work and their impact in relation to others and seek to demonstrate care and commitment in their engagement with communities they serve.
Below, we elaborate on the approaches and strategies in Figure 2, describing our framework for health system leadership, healthcare providers, and healthcare institutions to strengthen their trustworthiness.
Approaches to Building Trustworthiness
Take Responsibility for Building Trust
First, trust is too often discussed in a way that places the onus on community members to have trust, thus framing mistrust as a deficiency on the part of BIPOC populations. Instead, efforts to address mistrust should begin with acknowledgement that the responsibility should be placed on the shoulders of stakeholders across the health sector who participate and work within racist systems that continue to produce inequitable outcomes, to become deserving of the community’s trust.
Explicitly Acknowledge Both Historical and Contemporary Reasons for Distrust
Secondly, health systems leadership, healthcare institutions, and healthcare providers should recognize not only the historical but also the contemporary reasons for mistrust. Mistrust is steeped in the history of the brutalization of BIPOC bodies, including the often-cited Tuskegee syphilis experiment, the non-consensual use of Henrietta Lacks’ cells 29 and the violation of enslaved peoples' bodies for research. These historical factors work in tandem with contemporary realities to reinforce mistrust. 30 While the Tuskegee experiment may play a role in some Black people’s hesitancy to participate in clinical trials or take up a new vaccine, various other factors are significant, including systemic racism, well-documented poorer health outcomes among BIPOC populations, lower quality treatment by healthcare providers, and discriminatory experiences both inside and outside of health care settings.30,31 In the face of these prevailing realities, mistrust is a rational outcome of systemic racism, discrimination and inequitable treatment that occurs every day in clinics, emergency departments, hospitals, and anywhere people of color seek care.32,33
Address the Root Causes of the Trust Gap
Finally, it is important that health systems and institutions understand that trust is deeply integrated into the everyday interactions that people have with health systems. For example, there is evidence of pervasive implicit and explicit bias among healthcare providers.34–36 These biases contribute to unequal treatment and lower quality care for racially and ethnically minoritized individuals. 36 Interactions that are marred by biases crystallize perceptions and attitudes that BIPOC populations have toward healthcare institutions. Mistrust cannot be viewed as a mere hurdle to be overcome in promoting behavior change (e.g., to get vaccinated against COVID-19). Instead, all relevant actors need to create more opportunities to listen to the voices of minoritized people, and to communicate in a way that emphasizes respect and fosters agency. For example, one of the CBO partners in the EVI reported that even for some community members who did not trust the safety and efficacy of the vaccine and ultimately did not decide to get vaccinated, they appreciated the respectful and non-judgmental discussions they had with CBO representatives about their concerns.
Beyond interpersonal interactions that can help provide evidence of trustworthiness, structural racism needs to be redressed within health systems and institutions. Hospitals and clinics that primarily serve racially and ethnically minoritized communities still experience resource constraints and staffing issues that have outlived the legality of segregation. 37 Likewise, some healthcare institutions continue to offer differential access and treatment based on insurance status 38 -- a discriminatory approach that also affects racially and ethnically minoritized communities. This is particularly important in light of empirical findings that irrespective of satisfaction with care, mistrust is higher in lower income individuals, who are disproportionately from racially and ethnically minoritized populations. 39
Suggested Strategies for Key Stakeholders
Healthcare Providers
In light of the historical and contemporary reasons for distrust discussed above, healthcare providers should lead with respectful care and communication that foregrounds the agency and voices of the communities they serve.40,41 Stanford University’s Presence 5 framework for antiracist communication recommends the following: self-reflection on identity and bias, attentive listening that is sensitive to racism and its effects, explicit conversations about goals and care with patients, acknowledgement of patients’ story, and being aware and responsive to patients’ emotions. 42 In addition, we echo the American College of Physicians’ recommendation for healthcare professionals to have a strong knowledge base on screening for and addressing social determinants of health for individuals placed at higher risk. 43 Finally, healthcare providers are responsible for critically examining preconceived notions and explicit or implicit biases they might hold about racially and ethnically minoritized individuals. Becoming aware of biases is the first step in moving toward correcting harmful mindsets, providing equal care to all patients and demonstrating trustworthiness.
Health System Leadership and Healthcare Institutions
For health system leadership and healthcare institutions, a suggested strategy for showing care and commitment is investing in long-term partnerships with CBOs. These partnerships will serve as a foundation of sustained commitment to the wellbeing of the communities and will go a long way in demonstrating trustworthiness. We echo previous calls in the literature for these to be equitable, mutual partnerships 44 that focus not only on health, but on nutrition, housing and other social determinants of health. 45 Doing so demonstrates care for the community and reflects the trustworthiness of these health systems. Healthcare institutions in particular, should critically examine the impact of their organizational policies and culture with attention to how these policies and cultures serve to either disrupt or reinforce racist structures. Unless structures themselves are challenged, individuals, even well-intentioned ones, will continue to participate in systems that reproduce racist outcomes and foster mistrust and distrust among minoritized people. Suggested steps to promote trust and equity include providing education and training for all healthcare professionals in implicit bias and cultural humility as well as ensuring diversity through equity-focused recruitment practices for these professionals.
Finally, robust data should be collected and consistently monitored by health systems and institutions, and health outcomes measured across racial and ethnic groups in order to expose and address existing health inequities. 46
Conclusion
The COVID-19 pandemic has re-centered the importance of trust in pursuing health equity. As CBOs become more integrated with local health systems in efforts to leverage their built trust with the community, it is important that these relationships are supported over the longer term. The influx of resources to these organizations should likewise continue beyond the pandemic, building the capacity of these organizations to expand programming and better serve underserved populations. Furthermore, this investment in CBOs cannot be used as an alternative to a rigorous, sustained effort by those same health systems to earn and maintain the trust that is so crucial for health equity. Stakeholders across the health sector should be mindful of how their actions and inactions serve to build or further threaten trust. Finally, healthcare systems and institutions should dismantle policies and organizational cultures that reinforce structural racism. If these systems do not proactively demonstrate their trustworthiness, trust will continue to be actively eroded, and the next public health crisis will find trust in healthcare systems and institutions more lacking than ever.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible by generous financial funding from The Rockefeller Foundation (10976). The findings and conclusions contained within are those of the authors and do not necessarily reflect positions or policies of The Rockefeller Foundation