
Abstract
Local health departments (LHDs) play a leading role in eliminating health inequities as they proactively identify and address barriers to optimal health within the community they serve. This study evaluated a Midwestern County LHD’s commitment, collaborations, and capacity to advance health equity in their organization. A total of 81 employees completed the online survey (response rate = 51%) and 12 among randomly selected employees completed the qualitative interviews (31.5%). More than 75% of participants reported that all departments had explicit work plans and 50% had a strong capacity to address social determinants of health. Almost 50% of the participants reported strong internal collaboration, but less than 25% indicated that no external partners were involved during the program planning process. Finally, a few participants identified the need for increased diversity in leadership and expressed the importance of quality training and feedback.
Keywords
Introduction
Advancing health equity is increasingly emphasized as a central goal of public health practice. 1 Governmental institutions, including national, state, tribal, and local public health systems, play a critical role in providing equitable opportunities and resources for all people to pursue optimal health.2,3 In particular, local health departments play an essential role in eliminating health inequities as they are expected to proactively identify, understand, and address barriers to health in their communities. 4 However, the 2017 Public Health Workforce Interests and Needs Survey (PH WINS) reports that in the next 5 years almost half the public health workforce may leave their organizations due to issues such as inadequate pay, lack of advancement, workplace environment, job satisfaction, and lack of support. 5 Hence, building a skilled public health workforce to promote health and address health inequities requires a deeper evaluation of a comprehensive assessment of their organizational capacity.
The efforts of health departments to address health equity requires an internal assessment of capacity, infrastructure and policies, as well as an external assessment of programs, resources, and services provided to the communities. 6 Active examination of internal organizational capacity and staff competencies requires all employees to understand the challenges and opportunities within their organization that build their internal capacity and strengthen their external collaborations. However, capacity assessment is reported to be often neglected, and program development and performance evaluations within organizations prioritized. 7 Despite the availability of diverse assessment tools to measure the effectiveness of health equity initiatives, there is a concurrent need to understand the necessary conditions and capacities that strengthen and support health equity action. 7
Organizational capacity, in the context of addressing health equity, refers to an organization's ability to facilitate, support, and implement strategies to promote equitable health outcomes for all individuals in the community. Capacity building represents a strategic methodology to enhancing these abilities of the organization itself as well as the staff. 7 Although organizational capacity is acknowledged as a critical determinant of public health system performance, the assessment of capacity is reported to be often neglected in preference for program development and evaluation. 7 The initial step in this process is to quantify the current capacity measures including the organizations’ policies, practices, and priorities.
Hence, the aims of this mixed methods study at a local health department (LHD) were to (a) quantitatively assess the baseline measures of their organizational commitment, collaborations, and overall capacity to address health inequities in the work they do in the community, and (b) qualitatively appraise the strengths and areas of improvement with respect to their institutional capacity to address health inequities. This introspective examination of current capacity could allow the health department to strategically align its resources, streamline processes, and foster a culture of effective collaborations, thereby improving their readiness to address health inequities.
Methods
A midwestern County LHD in collaboration with the local University institution in Ohio conducted this health equity assessment in summer of 2022. Approval from the Institutional Human Research Protection Program (#01448) was obtained to conduct this assessment.
The Bay Area Regional Health Inequities Initiative (BARHII) toolkit was used as a framework to develop the current baseline health equity assessment with a mixed-methods approach. 8 BARHII, a collaboration of 11 local health departments in the greater San Francisco Bay area developed the organizational self-assessment for addressing health inequities toolkit. The development of the self-assessment tools was informed by an extensive review of public health and organizational development literature, as well as a review of existing organizational and cultural competency assessment tools by the BARHII committee members. The toolkit aims to help organizations identify their current capacity, skills, and areas that need improvement to promote health equity initiatives.
Overall, the mixed methods approach was used here to gather both quantifiable data as well as descriptive, more in-depth information to provide comprehensive findings regarding the organization’s capacity to address health equity. Additionally, the mixed-methods approach is important to establish a solid, comprehensive baseline assessment for the organization to build future subsequent assessments as highlighted by Creswell and Hirose. 9
Quantitative Methods
Survey Development
Staff survey instrument within the BARHII toolkit was reviewed as a framework to adapt and develop the assessment survey. The final adapted survey consisted of six sections, the first five sections adapted from BARHII toolkit, which assessed the institutional commitment, infrastructure support, and community engagement to address health equity and SDOH at the LHD. These sections were as follows: (i) demographics; (ii) organization’s mission, strategic planning, program planning and design; (iii) collaboration within the programs and departments; (iv) collaboration with external partners and policy makers; and (v) working with the local communities. The sixth section consisted of newly developed items related to changes experienced during the COVID-19 pandemic by the organizational workforce. Thus, this survey provided an organization-wide picture of attitudes, practices, competencies, and structures that indicated a capacity to address health equity at the LHD.
Weekly meetings were held with administrators from the LHD to identify the department’s areas of interest for evaluation. Face validity of the final survey instrument was established by the expert review of the survey by six faculty at the academic institution. The final survey on Qualtrics was further tested by six members of the evaluation research team for functionality and accessibility. The instrument consisted of 39 items with a readability level at 8th grade, assessed using the Flesch-Kincaid test.
Measures
Contact with the Community in Their Role at the Health Department
The survey respondents were asked if they directly interact with the community residents in their current role at the health department. Those who answered “yes” were categorized as “direct community-contact employees,” and those who selected “no” as “indirect community-contact employees.”
Perceived organizational commitment to address health inequities was measured using a subscale with five items, (i) working with external partners, policymakers, and community members, (ii) demonstrating commitment at the staff level, (iii) placing strategies to advocate for public policies, (iv) having program level work plans with explicit strategies, and (v) demonstrating commitment at the organizational level. Each item was measured as “no”, “moving in that direction,” and “yes.” The total score on this subscale ranged from 5 to 15, with higher scores indicating greater perceived commitment. The Cronbach’s alpha for this subscale was 0.85.
Commitment to Address Health Inequities in Mission, Vision, Values, and Strategic Plans
The responses to the survey items inquiring if the organizational commitment is reflected in (i) mission statement, (ii) vision statement, (iii) values, (iv) organizational strategic plan, and (v) program level strategic plan was recorded as “yes,” “no,” and “don’t know.”
Type and Role of External Partners
Survey respondents were asked to select from a list of the type of external partners and a list of the role of such partners. Additionally, respondents also had the option to select the “other” option and type their responses.
Trusting Relationships with External Partners and True Representation of Interests and Needs by the External Partners
On a 5-point Likert scale ranging from “Strongly disagree” to “strongly agree,” the survey respondents stated if they believe the organization has a trusting relationship with external partners and if they believe these external partners truly represent the interests and needs of the local community residents.
Familiarity with the Community Subscale
Being responsive to the needs of the community being served is one of the key elements of organizational capacity to address social determinants of health (SDOH). Hence, the survey respondents were asked about their familiarity with the community they serve using four items assessed on a 5-point Likert scale ranging from strongly disagree to strongly agree. The total score ranged between 4 and 20. This subscale had a Cronbach’s alpha of .88.
Internal Collaborations
The opinions of survey respondents about internal collaborations within the organization between programs and departments to address health inequities were assessed using six items. The responses were recorded on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree.”
Ability to Support Work Subscale
This subscale consisted of six items about the ability of LHD to support work addressing social determinants of health and health inequities. The responses were recorded as “no,” “moving in that direction,” and “yes.” The total score on the subscale ranged between 6 and 18, with higher scores indicating positive perceptions towards LHD’s ability to support work addressing SDOH and health inequities. The Cronbach alpha coefficient was 0.87.
Perceived Capacity Subscale
This 6-item measure assessed respondents’ perceived capacity of the LHD to address social determinants of health and health inequities on a 3-point scale, “no,” “moving in that direction,” and “yes.” The potential range of this scale was 6 to 18, with a higher mean score representing higher perceived capacity of the organization. The Cronbach alpha coefficient was 0.96.
Sampling and Data Collection
After an initial invitation email from the Health Commissioner to all employees, the Qualtrics survey link was distributed via email to all 153 then-current staff at the LHD. Data were collected during the summer of 2022. Five reminders were sent, including four from the evaluation team and one from the Health Commissioner. In total, 81 employees completed the survey yielding a response rate of 53%.
Analysis
SPSS-version27 was utilized to conduct all statistical analyses. Detailed descriptive statistics were performed using frequency and percentages.
Qualitative Methods
Interview Guide Development
The interview questions were initially developed by the academic research team using BARHII staff-level and management-level interview guides as a framework. These initial drafts of interview questions for direct and indirect community-contact employees were then reviewed for feedback by the LHD representatives. Finally, the collective team of academic researchers and LHD representatives together created the final version of the instruments in a group meeting. Next, the lead researcher conducted one training session consisting of a mock interview with the researcher who conducted the final interviews. The interview guide for the direct community-contact employees and in-direct community-contact employees inquired regarding commitment, capacity and community engagement to address health equity in the following topic areas: vision mission and value statement; strategic planning process; cultivating organizational culture of learning and professional development; value cultural and linguistic diversity; participatory and transparent decision-making process community capacity building efforts; streamlined administrative processes and funding; staff knowledge of community issues and resources; and workforce development (Appendix A).
Interviews were utilized to gain insight into the participant’s subjective experience of working at the organization during the COVID-19 pandemic. This approach allowed the interpretations of employees of the LHD to guide understanding of their experience and the meaning that is assigned to their experience. Face validity of the final interview guide was established by the expert review of six faculty at the academic institution.
Sampling and Data Collection
Thirty-eight employees were randomly selected using a random number generator from the list of 153 LHD staff and invited to participate in the qualitative study. Finally, six direct community-contact and six indirect community-contact employees consented to participate in the study and completed the key interviews. SignUpGenuis.com, an online platform, was utilized to schedule the interviews. The interviews were conducted after consent was obtained by an academic research team member and recorded on both Sonix (10 interviews) and WebEx (2 interviews) online platforms, each lasting for 40-60 min. Ensuring confidentiality, all employees were encouraged to speak openly regarding their experiences working at the LHD.
Analysis
Interviews were transcribed verbatim, and all identifying information was removed to protect confidentiality. Two researchers reviewed and independently coded each transcript. 10 Using text analysis, deductive coding was applied to categorize them into themes and sub-themes. 11 Codes developed from the data analysis allow the researcher to determine the range of issues discussed and their meanings. Initial codes developed were re-analyzed and refined throughout the data analysis phase. Key themes were extracted from the final codes, and illustrative quotes were selected and analyzed. 11 Deductive thematic analysis was then conducted related to organizational characteristics and workforce competencies as described in the BARHII toolkit. Additional themes were included as they emerged during data analysis.
Results
Quantitative Results
Majority of the survey respondents were program staff (46%), followed by those in administrative positions (23%). A significant proportion of the respondents were direct community-contact employees (75%) while 20% were indirect community-contact employees. Close to half of the participants (48%) had >10 years of experience working in the field of public health, and about 42% have been working at the LHD for >10 years.
Organizational Commitment to Address Health Inequalities
Organizational Commitment to Address Health Inequalities Among LHD Employees.
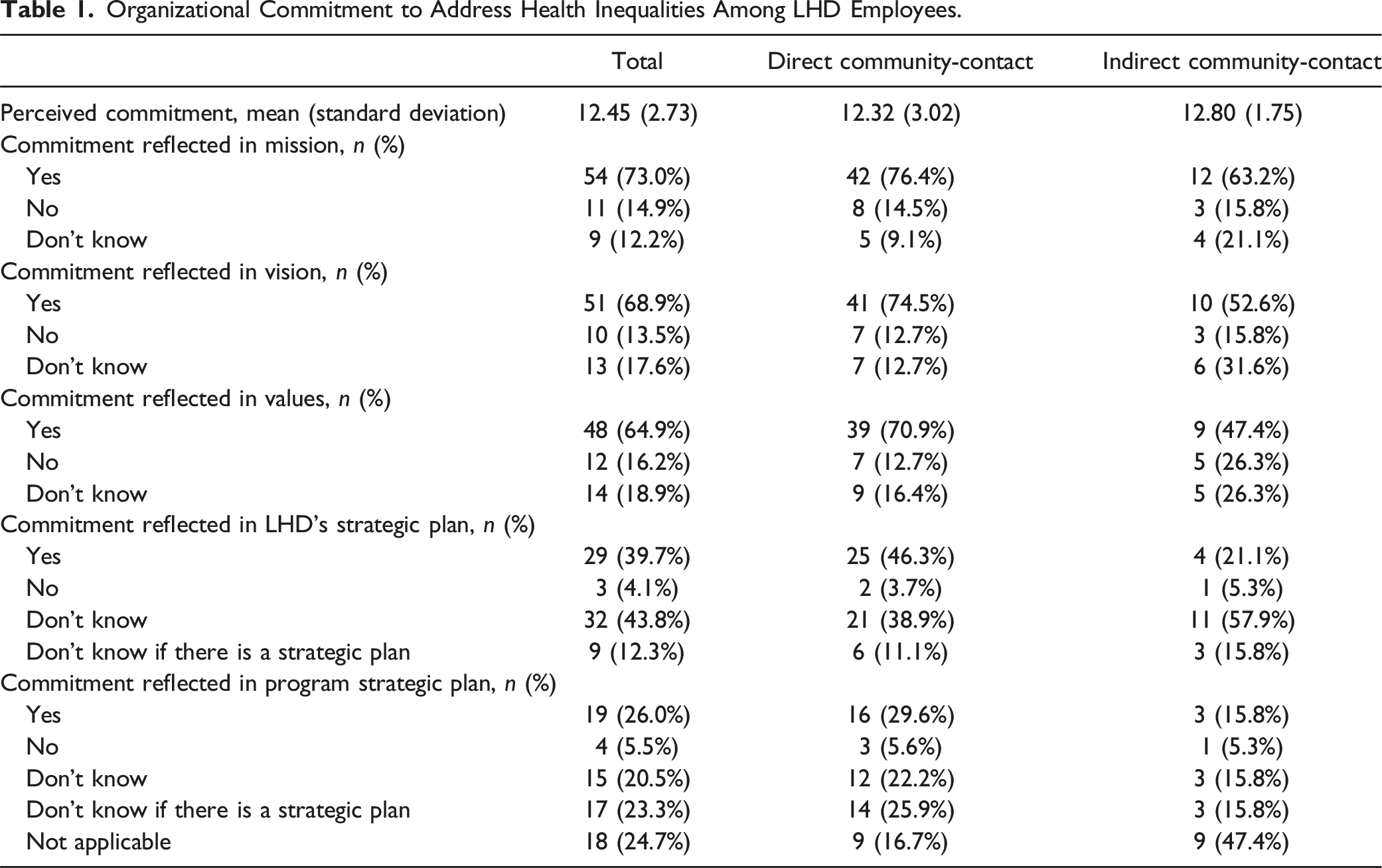
Most respondents expressed that LHD's mission (73%), vision (69%), or core values (65%) reflect the organization's commitment to addressing health equity, with less than 20% indicating an unfavorable view. Only 40% of the survey participants agreed that the LHD's strategic plan includes an explicit commitment to addressing health inequities. A significant proportion (48%) said that they are unaware of such a plan or there is no strategic plan for their department.
Collaboration with the Community
More than one in four respondents (26%) indicated that no external partners were involved in the program planning process at the LHD. The most frequent types of external partners identified by the respondents were public agencies (46%), community-based organizations (42%), community members/residents (38%), and non-profit organizations (36%). When inquired about community stakeholders' specific roles in the LHD’s program planning and delivery, a striking 40% of participants perceived that the community stakeholders play no role. In comparison, another 40% of respondents thought that the community leaders, residents, and organizations contributed their input at the beginning of the program planning process.
The survey respondents reported the organization collaborates a lot with external partners, particularly for (i) food security that impacts health inequity (40%), (ii) early childhood development and education (30%), and (iii) community safety and violence prevention (25%). On the other hand, a significant proportion of participants reported no external collaboration for: (i) community economic development (56%), (ii) land-use planning (44%), and (iii) availability of quality affordable housing (42%).
There is a significant gap between the number of survey respondents (63%) who agree or strongly agree that external partners truly represent the interest and needs of the community and those who agree or strongly agree (51%) that the LHD has trusting relationships with external partners (Figure 1). Local Health Department and External partners.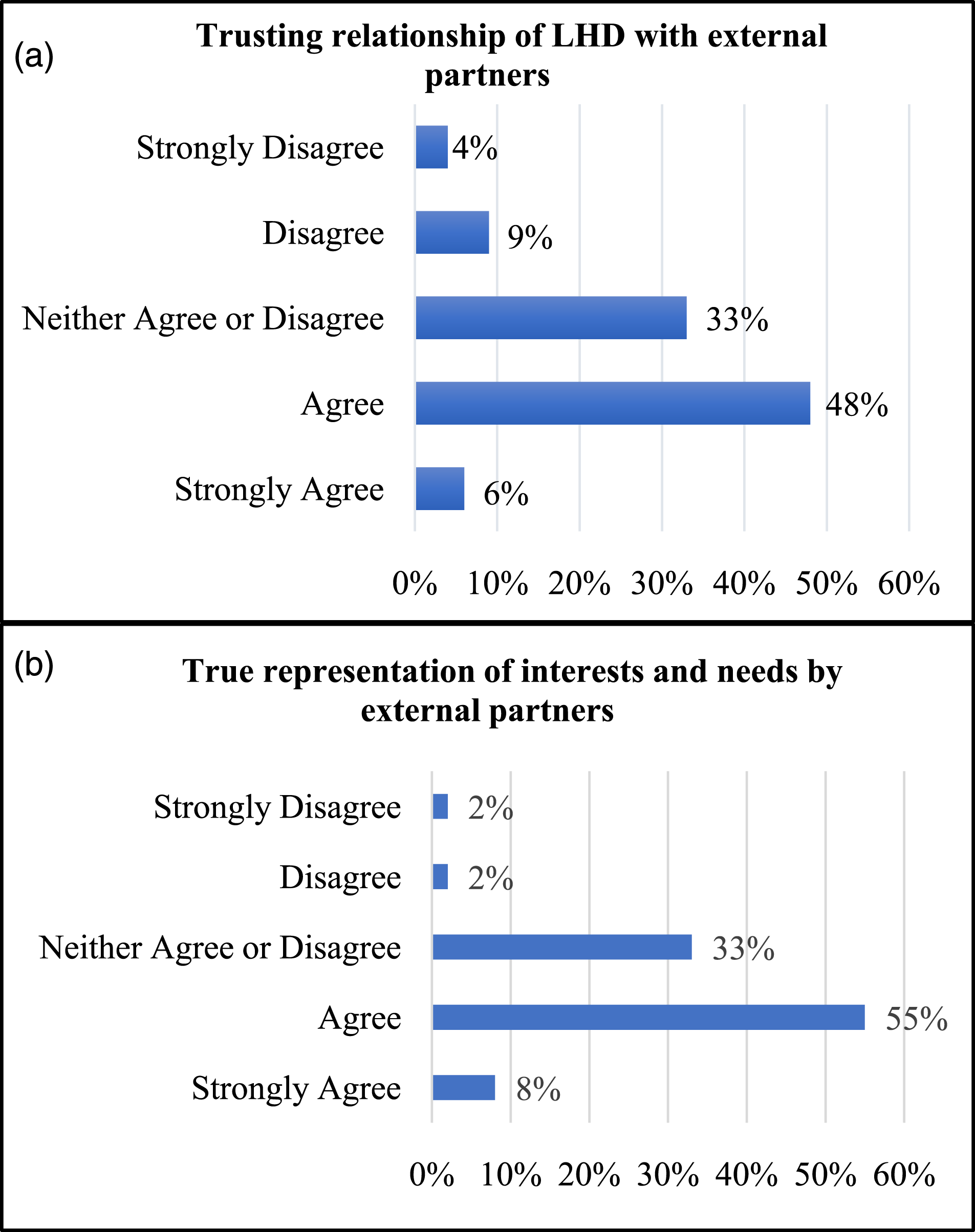
Organization Capacity to Address SDOH and Health Inequities
Familiarity with the Community
Seventy percent or more survey respondents reported overall good familiarity with the community, specifically its (i) demographic composition (87%) (ii) major health inequities affecting the residents (77%), and (iii) information sources to help identify and learn about chief concerns in the community (73%). However, 10% of participating staff expressed the most unfamiliarity with the strength and resources of the community they serve.
The difference in mean familiarity score between direct community-contact (M = 15.87) and indirect community-contact employees (M = 16.0) was not statistically significant (t(57) = 0.169, p = .87).
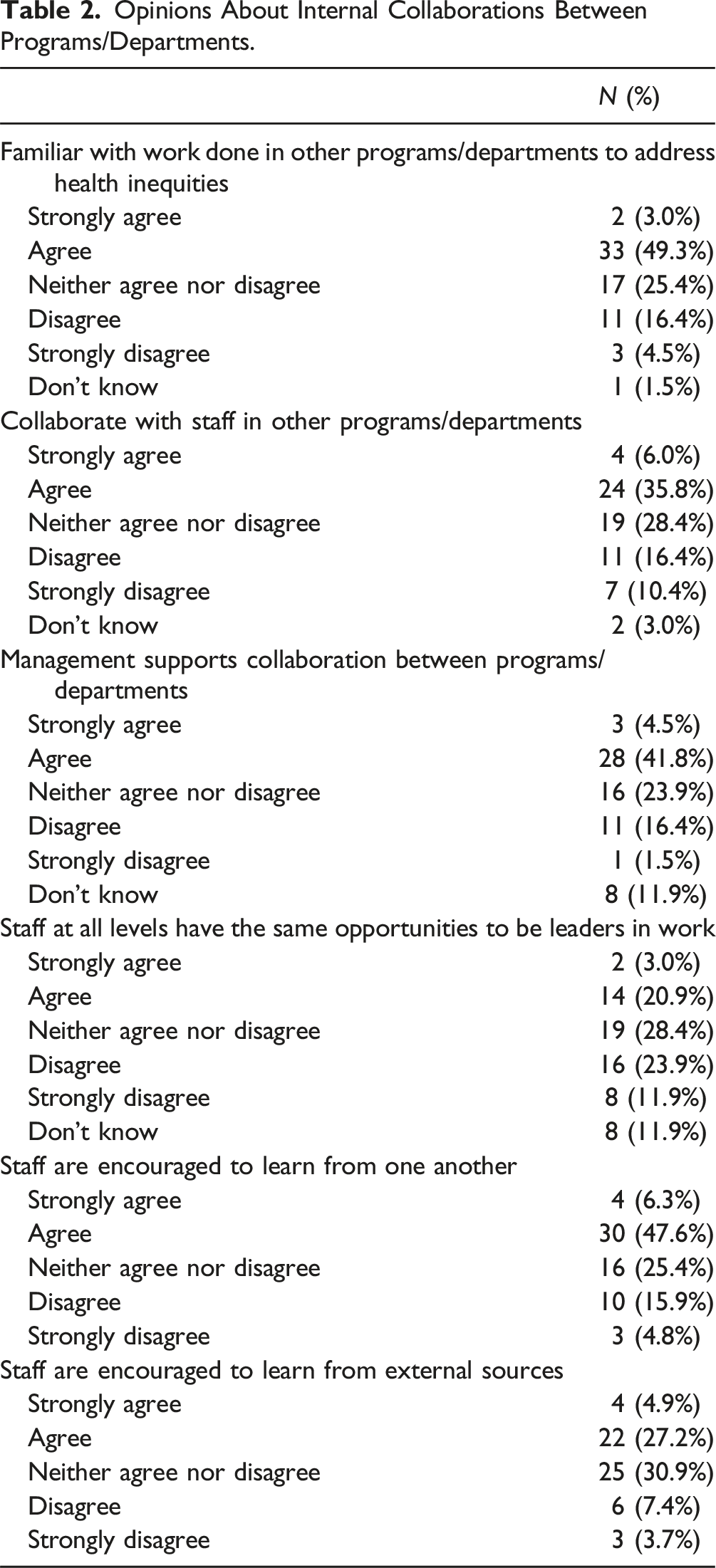
Internal Collaborations
Opinions About Internal Collaborations Between Programs/Departments.
Ability to Support Work Addressing SDOH and Health Inequities
Half of the participants (50%) indicated that the LHD is open and responsive to community stakeholders’ feedback on its work, while 42% reported the organization is moving in that direction. The greatest need was identified by participants in the areas, where 41% specified that there are no strategies in place to minimize barriers to community participation, and 22% specified that the LHD does not make deliberate efforts to build the leadership capacity of community members to advocate on issues affecting SDOH.
Overall, the direct community-contact employees had more positive opinions that LHD’s ability to support work addressing SDOH through strategies and deliberate efforts in the community (M = 13.89), compared to indirect community-contact (M = 10.43), and the differences were statistically significant (t(24) = 2.68, p = .01)
Perceived Capacity to Address SDOH and Health Inequities
Overall, the participants indicated affirmative opinions toward the capacity of the LHD to address SDOH and health inequities. About two-thirds of the respondents (65%) believed that the LHD creates and distributes oral and written information appropriate for the community's cultural, linguistic, and literacy needs. The two most frequent areas of concern were (i) setting standards and expectations for how they work with the community (18%), and (ii) assessing the work against these preset benchmarks (19%). Overall, the direct community-contact employees had a higher mean on this subscale, indicating higher perceived organizational capacity (M = 14.48), compared to indirect community-contact employees (M = 12.20), although the difference was not statistically significant (t(28) = 1.16, p = .26).
Qualitative Results
Themes, Sub-themes and Quotes From Qualitative Key Interviews With LHD Employees.
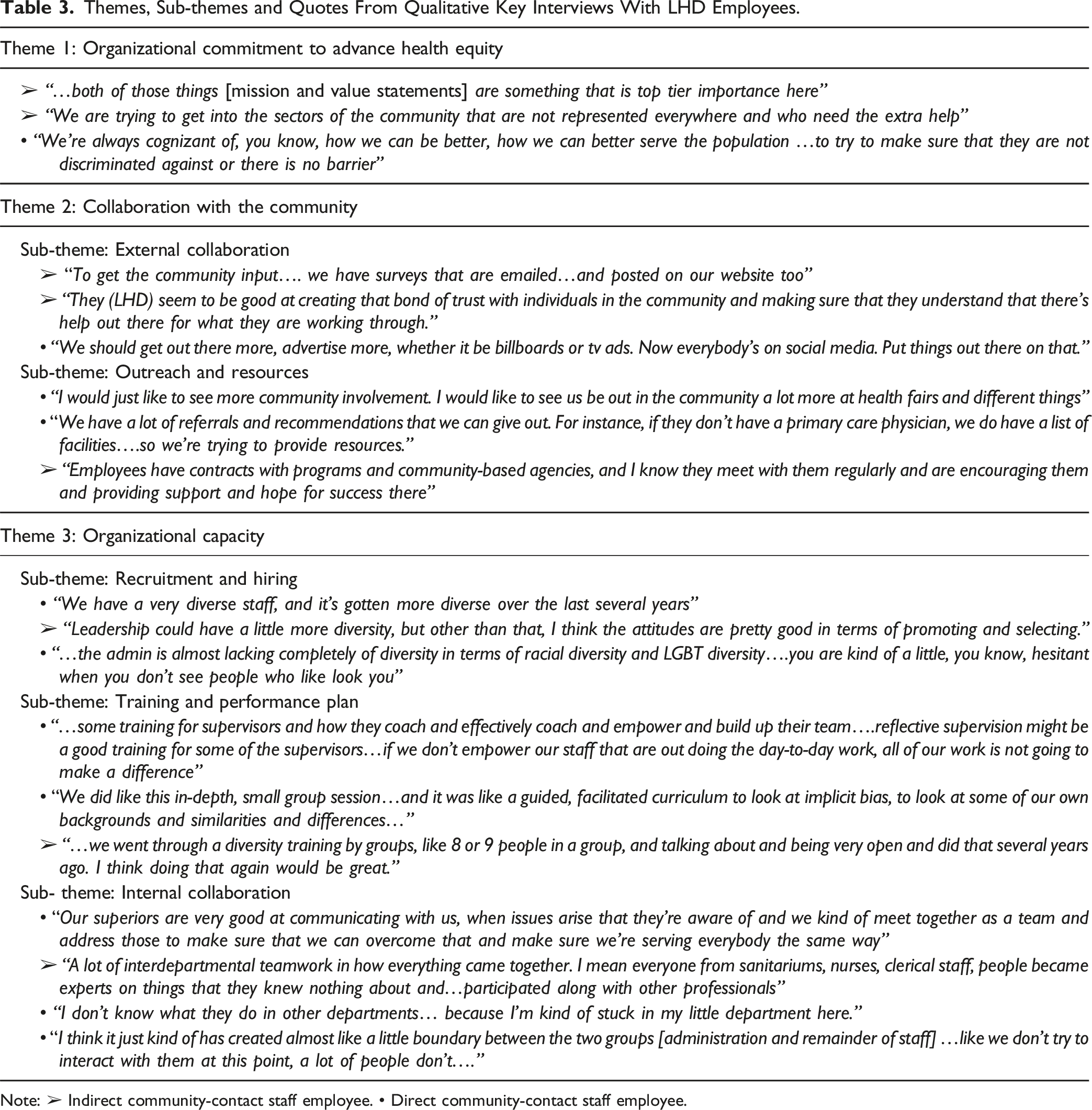
Note: ➢ Indirect community-contact staff employee. • Direct community-contact staff employee.
Theme 1: Organizational Commitment to Advance Health Equity
Most of the direct and indirect community-contact employees reported that their organization’s vision, mission, and values statements demonstrate a commitment to advance health equity. One participant emphasized the expansion of diverse community programs to better serve the community. One direct community-contact employee elaborated that funding decisions are also aligned to their institutional commitment to support the needs of vulnerable community members.
Theme 2: Collaboration with the Community
Two sub-themes were identified including external collaboration, and outreach and resources.
Sub-theme: External Collaboration
Most direct and indirect community-contact employees reported that the organization maintains a strong commitment to foster true community partnerships by promoting regular community meetings and building connections with all community-based agencies. One indirect employee shared that open communication is actively pursued by conducting community surveys via emails and posting them on the website. Multiple employees emphasized the critical role of building trust and forming long-term relationships, in addition to maintaining existing relationships with community partners.
Sub-theme: Outreach and Resources
Many direct community-contact employees stated that active engagement in the community is fostered through diverse activities such as health fairs, community events, providing clinical and non-clinical referrals, and health clinics for immunization and other screening needs. Few employees shared that increasing awareness of programs in the community is an important part of building community partnerships and shared the prominent role of community organizations in promoting health awareness resources. However, one direct community-contact employee shared more emphasis on community outreach is still needed.
Theme 3: Organizational Capacity
Three main sub-themes were identified including recruitment and hiring, training and performance plans, and internal collaboration.
Sub-theme: Recruitment and Hiring
All employees reported that their organization has actively engaged in hiring practices to create a diverse workforce, despite a high employee turnover. In addition, the recruitment strategies emphasize creating a diverse workforce that matches the diversity in the community. However, a few direct community-contact employees observed that diversity in leadership and administrative positions is significantly lacking, that may contradict the emphasis on diversity and inclusion to advance health equity as an important organizational value.
Sub-theme: Training and Performance Plan
Most direct and indirect community-contact employees reported that staff are supported in addressing health inequities through existing programs, staff discussions, and team meetings. These established infrastructures support open and comfortable communication with their supervisors. Most of the indirect community-contact employees shared that feedback from all staff members is actively pursued by conducting a yearly employee satisfaction survey. In addition, one indirect community-contact employee mentioned the use of assessments such as SWOT analysis with all employees and board members helps create transparency in all communications and develop strategic tools to address challenges. Multiple employees reported on the importance of creating efficient, streamlined administrative processes, for example, developing a succession plan to meet the challenges during crises such as the COVID-19 pandemic.
Many employees reported the need for additional training on important issues such as implicit bias, addressing the needs of vulnerable populations, and health disparities. Some direct community-contact employees stated attending training was further challenged during the pandemic. One indirect community-contact employee reported a lack of data sharing within the organization and with community partners as a challenge; however, efforts are ongoing to develop a data-sharing hub.
Sub-theme: Internal Collaboration
Most direct and indirect community-contact employees reported strong interdepartmental and intradepartmental collaboration and communication. Many expressed that a lot of effort was invested in building effective teams within the departments and with community members during the pandemic to meet the diverse needs of the community. Most employees shared that there was open and inclusive communication within the organization, and supervisors were mostly supportive. However, a few direct community-contact employees reported feeling disconnected and isolated in their work experience due to a lack of interaction with other employees and departments. In addition, one direct community employee reported lacking guidance and being hesitant in approaching senior administrators.
Discussion
Organizational capacity largely determines an organization’s ability to function effectively and achieve goals. Capacity is a multifaceted concept and is impacted by aspects like organizational commitment and community collaboration. 12 In the current assessment of a LHD’s organizational capacity to address health inequities, both quantitative and qualitative results revealed two key aspects that needs immediate attention to further build their capacity, (i) having a skilled and diverse public health workforce, and (ii) engaging communities in all in all aspects of strategic planning, program planning and implementation. The quantitative data highlighted the high turnover rates and lack of diversity, particularly in leadership positions, reflecting national trends in public health departments. These findings were substantiated by qualitative insights from staff and leaders, who voiced concerns about the need for more diverse leadership and expressed the immediate need to address this issue. Moreover, the importance of community collaboration was revealed in the qualitative results, with staff emphasizing the value of community partnerships and outreach activities, a theme also presents in the quantitative assessment.
First, having a skilled and diverse workforce offers unique insights into ways of achieving health and is better equipped to meet the needs of communities being served. The Public Health Accreditation Board (PHAB) lists having a competent workforce and leadership as a standard requirement for health department accreditation, 13 which is threatened by high turnover rates. 14 Our study found high turnover rates within the organization following the national trends where LHDs lost 21% of their workforce from 2008-2019. 15 Such rates are attributed to the lack of competitive salaries for public health professionals. 5 Furthermore, notable pay disparities exist where employees of LHDs typically earn less than those at a state health agency, despite having equal credentials. 15 Job positions, such as data analysts, nurses, and epidemiologists, earn significantly more in the private sector than in LHDs that could also significantly impact turnover. 16
Fostering a diverse workforce at all levels is one of the important ways to build trust in the community in order to reach underserved and disadvantaged populations. The 2019 National Profile of Local Health Departments reported that less than 10% of top executives were a minority race/ethnicity, and the majority were
Skill and quality of leadership as well as staff perception of leadership support, have been found to be strong predictors of staff retention. 14 Our assessment revealed some participants feeling unsupported and in need of more guidance/supervision, which could have further fueled the ongoing issue of workforce turnover. In summary, addressing these growing threats to recruit and retain a skillful and diverse workforce is critical to building organizational capacity to address health inequities.
Finally, engaging in community-based participatory practice (CBPP) in all community efforts is another key element to building organizational capacity to advance health equity. CBPP is a collaborative approach that proposes equal involvement from community members, researchers, and other stakeholders along with the organization. 18 For LCDs to effectively serve their respective communities, they must be strongly committed to collaborate with the community in all aspects of program planning, implementation, and results dissemination to advance their health equity action plan.
This study had a few limitations. Firstly, this mixed method study reports the experiences of employees working at a Midwestern LHD, which may limit the generalizability of these results to the experiences of employees at LHDs serving other regions of the country. Another limitation of the study is response bias. As this study was conducted at the tail-end of the COVID-19 pandemic, so personal challenges experienced during time-period may have influenced the responses by the participants.
Conclusion
Minimal work has been done to address health inequities across the country due to the demand of time and budget. Based on resource limitations imposed it is difficult to address all SDOH domains at various levels. It is critical that health departments commit to conducting annual health equity assessments of their organizational capacity, commitment, and community engagement in addressing health inequities. As next steps, LHDs must consistently advance their efforts to tackle the structural factors impacting their capacity to address health equity including organizational policies, cultural competency, their ability to address social determinants of health, community engagement, and equity-centered training.
Health departments need to build diversity in leadership, as it is an essential step in demonstrating organizational commitment to improving its culture of equity. Also, efforts are needed to recruit and retain a highly skilled, diverse, and motivated workforce. This could be facilitated through a governmental commitment to pay fair and competitive salaries as well as constantly offering skill-building and training opportunities for the workforce. Finally, organizations truly committed to fostering health equity in their communities should prioritize community engagement in all their activities, such as strategic planning, program planning and development, and program implementation.
Supplemental Material
Supplemental Material - Assessing Organizational Capacity to Advance Health Equity: Mixed-Methods Approach at a Local Health Department
Supplemental Material for Assessing Organizational Capacity to Advance Health Equity: Mixed-Methods Approach at a Local Health Department by Shipra Singh, Mounika Polavarapu, Katharine Vallerand, Yashika Bhoge, and Krista McCarthy Noviski in Community Health Equity Research & Policy.
Footnotes
Acknowledgement
Local Health Department administration and staff.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Author Shipra Singh and Mounika Polavarapu received grant funding from Centers for Disease Control and Prevention through the Regional Health District (Toledo Lucas County Health Department) (Grant #207612) for this study.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.