
Abstract
A central component of the Public Health 3.0 model is building partnerships between local public health departments and other community organizations/stakeholders, including public and private hospitals, as a means of promoting data sharing, service coordination, and collective action. Evidence suggests that such partnerships remain challenging and infrequent. This qualitative study used in-depth interviews to identify barriers and facilitators to building effective collaboration between local health departments (LHDs) and hospitals. We purposively recruited LHD officials (n = 12) across the United States. A directed qualitative content analysis of the interview transcripts revealed five barriers and five facilitators to building effective collaboration between the two entities. Perceived barriers included competition, inconsistent participation and engagement, communication breakdown, time constraints, and lack of financial and human resources. Perceived facilitators included finding common ground, well-established relationships, aligning and leveraging resources, open communication, and leadership commitment. Findings highlight challenges and opportunities to promote effective collaboration between LHDs and hospitals.
Keywords
Introduction
The United States (U.S.) has made noteworthy progress in improving its population’s longevity and quality of life over the past century through improved health infrastructure, strategic public health interventions, and advanced medical care.1–3 Despite these generally positive trends, a recent Commonwealth Fund report notes that, although U.S. health care spending outpaces other wealthy nations by a wide margin, the country trails its peers in life expectancy while having the highest rates of maternal/infant mortality and deaths from avoidable/treatable conditions. It also has the highest rate of people with multiple chronic conditions and an obesity rate that is approximately double the global average. 4 Several of these key health metrics have worsened in the wake of the COVID-19 pandemic; for instance, U.S. life expectancy declined approximately 2.7 years between 2019 and 2021, the largest 2-year decline since 1921–1923. 5 Furthermore, there continue to be considerable health disparities –– that is, differences in incidence, prevalence, mortality, burden of disease, and other adverse health conditions –– that negatively impact specific U.S. populations, including the poor and racial/ethnic minorities. 6 Mounting evidence demonstrates that many of these inequities worsened during the COVID-19 pandemic.7–9
In light of these continued challenges and a desire to “ensur[e] that everyone in America can achieve an optimal and equitable level of health” (p. 1), 2 scholars and practitioners have advocated for a new approach to public health practice described as “Public Health 3.0.” This approach is differentiated from Public Health 1.0 –– which encompassed the formation of the modern public health system in the late 19th and early 20th century and was characterized by scientific advances in disease etiology and prevention (e.g., vaccines) –– and Public Health 2.0, which DeSalvo et al. 2 argue originated with the Institute of Medicine’s landmark 1988 report The Future of Public Health and resulted in a (re)defining of a “a common set of core functions, and public health practitioners develop[ing] and implement[ing] target capacities and performance standards for governmental public health agencies at every level” (p. 3). Building from past successes and identified limitations associated with these prior eras, proponents of the Public Health 3.0 model have called for efforts to broaden public health practice beyond traditional functions and programs; in particular, they have advocated “work[ing] across sectors to address social, environmental, or economic determinants of health” (p. 3). 2
A central component of the Public Health 3.0 model is building partnerships between local public health departments (LHDs) and other community organizations/stakeholders, including public and private hospitals, as a means of promoting data sharing, service coordination, and collective action.1–3 This aligns with two Institute of Medicine reports that call for improving collaboration between public health and healthcare systems to improve efficiency, effectiveness, and better health outcomes. 10 The Affordable Care Act (ACA) also made provisions for nonprofit hospitals to complete community health needs assessment (CHNA) and invest in community health, providing an opportunity for collaboration between LHDs and non-profit hospitals. 11 The ensuing decade has brought a growing emphasis on the need to build better collaborations between local health departments and hospitals. LHDs play an important role in providing essential public health services to vulnerable populations and addressing the needs of their local communities, but many have been constrained by limited resources, which has compromised their effectiveness.12,13 Cultivating successful collaboration between LHDs and hospitals can facilitate greater investment in the community, more efficient use of resources, and improved coordination of population health efforts, especially in resource-constrained environments. 14
To promote collaboration between local health departments (LHDs) and hospitals, some states in recent years have sought to encourage voluntary collaboration between LHDs and nonprofit hospitals around CHNA, while some have provided guidelines or enacted laws to make collaboration around CHNA compulsory.15–18 Recent studies have found that collaborative relationships between LHDs and hospitals have consistently led to improved health outcomes in surrounding communities.19–21 For example, Isehunwa et al. 20 found that high levels of collaboration between LHDs and hospitals on CHNAs was associated with lower rates of self-reported poor health and a decrease in premature mortality. Another study found that collaboration between LHDs and substance use treatment centers was associated with lower county-level drug-induced mortality. 21
Despite these documented benefits, facilitating collaboration between LHDs and hospitals remains a challenge. Singh and Carlton 22 report, for example, that less than one-third (28%) of LHDs were collaborating at high levels on CHNA efforts with hospitals. Similarly, Cramer et al. 19 reported that––although strong LHD-hospital collaboration was associated with positive individual health behaviors, including lower smoking, higher consumption of vegetables, and more intense exercise––only about 22% of LHDs were involved in well-established collaborations. Few studies have explored barriers and facilitators to effective collaboration between LHDs and hospitals, especially from the perspective of LHDs. Erwin’s extensive review of LHD performance 23 as well as studies on the organization of LHDs and other public health agencies, 12 including the collaboration between public health and primary care, 24 are older and therefore do not contain recent investigations of a rapidly evolving public health environment. Valaitis et al. 25 qualitatively examined organizational factors that influence effective collaborative efforts between primary care and public health in Canada. Their study is relevant but does not address the specific organizational and operational aspects of LHDs in the U.S. 25
The array of current public health concerns, including ongoing COVID-19 outbreaks, the opioid epidemic, worsening mental health issues, and chronic health conditions, underscore the need to promote effective collaboration between LHDs and hospitals, both of which are critical actors within the public health and healthcare system. 26 Improving community health through such collaborations appears to hinge on implementing CHNA recommendations. For instance, Cronin et al. 27 found that many hospitals do not formally implement strategies to address opioid misuse following a CHNA despite having the resources to support community-based efforts to prevent opioid misuse. Conversely, Montoya et al. 28 demonstrated that highly coordinated collaboration among local public health officials and hospitals led to reduced asymptomatic COVID transmissions and improved outbreak control within nursing homes. Furthermore, studies by both Cramer 19 and Isehunwa 20 indicate that advanced levels of collaborative activities between LHDs and hospitals were pivotal to creating improved public health outcomes in the community and fostering greater degrees of preventive health measures.
The framework for this study is based on the Collective Impact (CI) model, which has been shown to provide an integrative framework for organizing diverse stakeholders into an effective team to address complex problems.29–32 The CI model, originally developed by Kania and Kramer, 33 focuses on five conditions that are usually present in systems-level collaborations and how those conditions can lead to greater system-wide progress. CI has been used by a wide array of stakeholders to address challenges in public health, education, and environmental degradation, among others.29,30,34,35 CI’s five conditions are helpful for evaluating the strengths and weaknesses of inter-agency collaborations, even if they are not explicitly engaged in using the CI model.
Acknowledging that no one organization is solely responsible for resolving a systemic problem, CI describes the five conditions that make it possible for diverse stakeholders, including a mix of public and private entities, to effectively collaborate and create positive systemic impact. According to the CI model, the five conditions of collective success are: (1) A “common agenda” with primary goals that are mutually agreed upon by the collaborating agencies; (2) “shared measurement systems” so that organizations may efficiently transmit meaningful data to each other; (3) “mutually reinforcing activities” that recognize the diverse gifts of participants and invite a variety of activities, all of which contribute to the overarching vision; (4) “continuous communications” among partners to build trust and reinforce strong relationships; and (5) a “backbone support organization” with adequate staff and resources to ensure that the collective activities are sustained and managed effectively.30,33
Using the CI model, this qualitative study explores the perceived barriers and facilitators to effective collaboration between LHDs and hospitals from the perspective of LHD administrators. As contemporary public health challenges evolve, this information will be useful for those seeking to improve LHDs and stimulate more successful collaborations between LHDs and hospitals.
Methods
Approach
All manuscript authors have extensive training in and experience with qualitative methodology. Drawing from this expertise, we chose a data collection and analysis approach grounded in the interpretive perspective –– that is, focusing on how participants use language to describe and make sense of their lived experiences.
Study Participants
Using a purposive sampling strategy, we recruited and conducted in-depth interviews with 12 LHD officials in 2018. The 2016 Profile Study of the National Association of City and County Health Officials (NACCHO) was utilized to identify LHDs collaborating with a hospital on one or more CHNAs as a proxy for LHD-Hospital collaboration. 20 We also attempted to include LHDs from higher-performing and lower-performing communities using data from the 2017 County Health Rankings, which identified the percentage of adults with poor or fair health, the average number of poor mental health days per month, the average number of poor physical health days per month, the years of potential life lost rate per 100,000, and premature age-adjusted mortality rates per 100,000 in each local community. High performers were communities with a “high” ranking on all five outcomes, as designated by the County Health Rankings, while low performers were communities with a low ranking in at least one of the five outcomes, in addition to not having any high ranking in any of the five outcomes.
From a sampling frame of about 296 LHDs reporting some form of collaboration with nonprofit hospitals around CHNA (statistically sampled by NACCHO to describe their levels of collaboration around CHNA based on eight activities), 40 LHDs were randomly selected taking into consideration those that had detailed contact information available through their respective websites and other publicly available sources. An initial email was sent to all 40 LHDs; after receiving no response, phone calls were made to 34 LHDs (i.e., those with available phone contact information). Of those contacted via telephone, five LHDs’ directors/administrators declined to participate, four LHDs’ directors/administrators initially showed interest in participating but subsequently could not be reached or did not agree to interview, and 14 LHDs did not answer their phone call. In instances where we were unable to reach an LHD via telephone, we followed up at least three times before removing them from our list of potential participants.
Procedures
This study was approved by the Institutional Review Board at the University of Memphis. Eleven telephone interviews and one onsite interview were conducted by the first author, who was a graduate student trained in qualitative research at the time of the interviews and who had no prior relationship with any of the study participants. An interview guide was developed using the Collective Impact (CI) model (see Appendix 1). 33 Each interview lasted approximately 25–45 minutes and was audio recorded. Field notes were taken during the interviews. Prior to the interview, the first author reviewed the informed consent document with participants, explaining the study’s purpose as well as privacy and confidentiality protections. The first author ensured participation was voluntary and addressed participant questions as they arose. Interviews proceeded after obtaining verbal informed consent.
Data Analysis
Interview audio recordings were transcribed; the transcriptions were double-checked against the recordings for accuracy by the first author. Transcripts were then imported into NVivo 12 and coded by the first author using a process informed by directed qualitative content analysis. 36 The a priori theoretical constructs were derived from the five Collective Impact conditions (i.e., a common agenda, shared measurement systems, mutually reinforcing activities, continuous communication, and backbone support organization). 34 Preliminary coding proceeded by analyzing meaning units, or quotes, grouping the quotes under the a priori categories, writing summaries of each group, and establishing codes based on the group summaries. Multiple preliminary codes were generated. The first author and senior author together compared, merged, and organized the initial codes using the constant comparative method.37,38 Next, the corresponding author and another senior author grouped the preliminary codes into categories, further abstracting the data from the a priori constructs. 36 Data were further analyzed inductively to examine the transcripts for emergent categories that might constitute new, stand-alone categories unanticipated in the deductive analysis. 35 No new categories were identified in that process. Disagreements were resolved through discussion among the first author, corresponding author, and other senior authors. To ensure the trustworthiness of the data, debriefing and field notes were used for confirmation or corroboration of study findings. 39 To enhance the rigor of the findings, a summary of the results was sent to participants to check for accuracy and to minimize researcher bias. 39
Findings
Characteristics of the LHD Participants and Organizations (N = 12) Included in the Study.
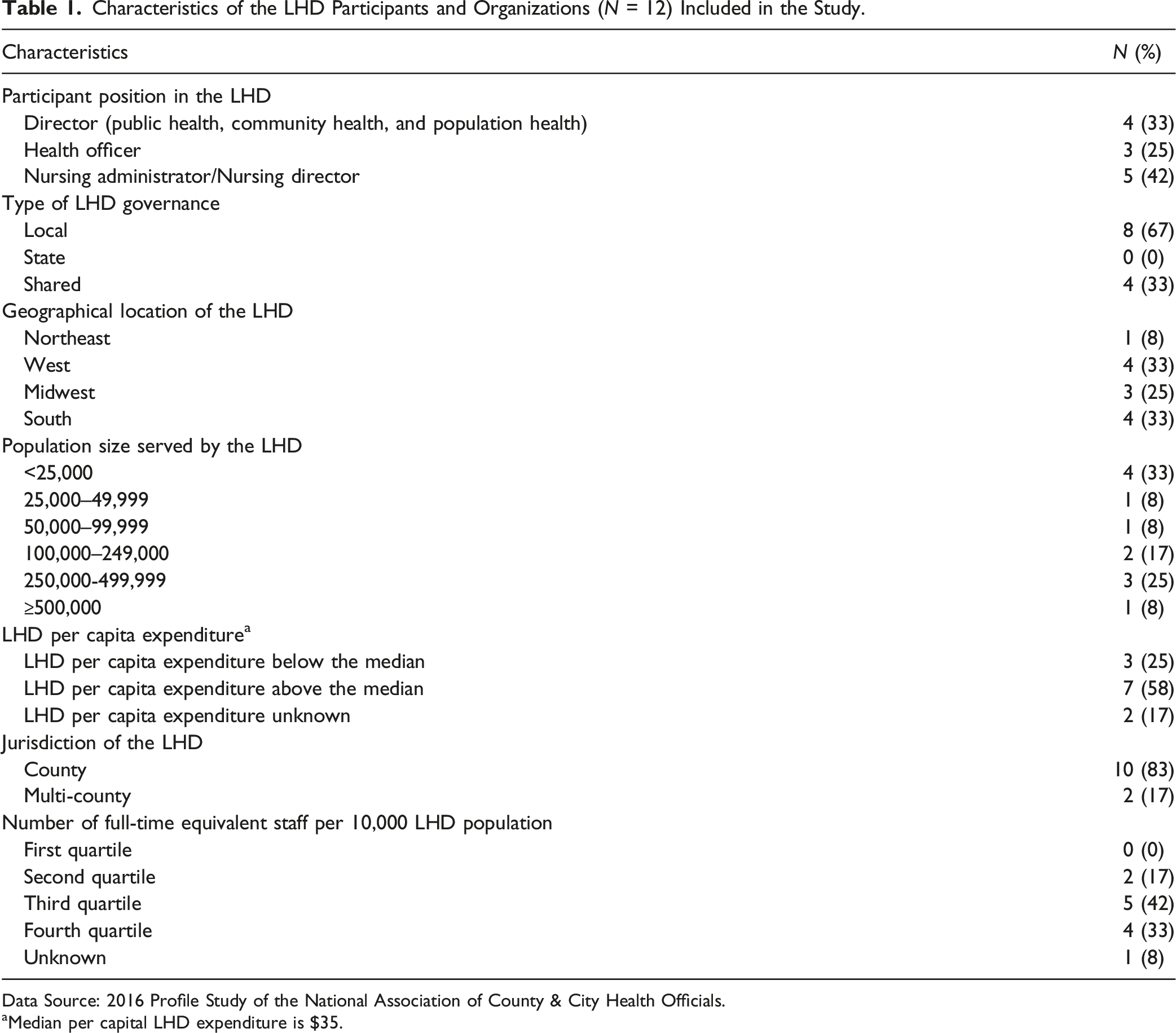
Data Source: 2016 Profile Study of the National Association of County & City Health Officials.
aMedian per capital LHD expenditure is $35.
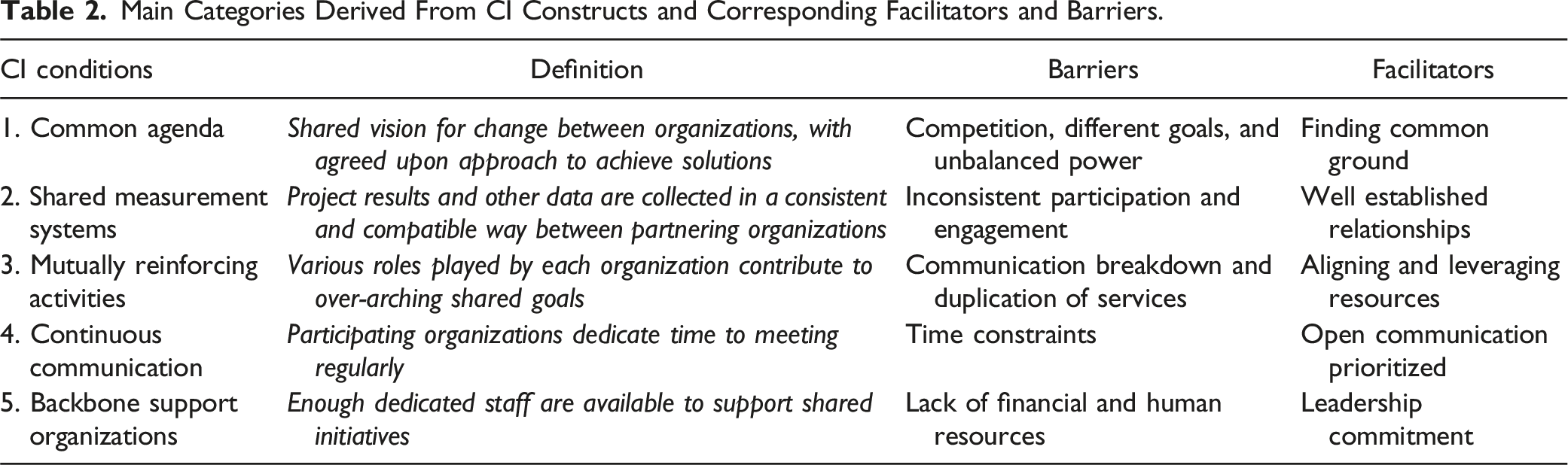
Main Categories Derived From CI Constructs and Corresponding Facilitators and Barriers.
Barriers to Effective Collaboration Between LHDs and Hospitals
Although all LHD officials reported that they were involved in collaborative relationships with hospitals to address community health needs and improve outcomes, they also shared some challenges to effective collaboration.
Competition, Different Goals, and Unbalanced Power
Establishing a common agenda between collaborative agencies is the first condition of the Collective Impact model. Study participants reported that the history of relative isolation between public health and healthcare systems—with different missions, goals, and objectives—is a challenge for establishing a common agenda with local hospitals: We clearly have a different mission. We approach our work differently and we haven’t leveraged our power. We are not historically viewed as equal at the table as a result of that. It is really trying to level that playing field. (LHD Official 4)
LHD officials described how finding the right balance between different goals and objectives was difficult; they did, however, report progress had been made in this area. They also felt that hospitals had more power and influence because of access to more resources: We don’t want to be in competition with the hospital. We are a non-profit organization, and we don’t want to step on their toes. I am not sure that they don’t step on ours because they really don’t provide anything that we essentially provide. (LHD Official 7)
Inconsistent Participation and Engagement
The second condition of CI addresses the critical need for collaborating agencies to consistently share information in formats that are mutually useful. Study participants indicated that a lack of consistent participation and involvement in shared projects or initiatives made it difficult to develop mutually useful information exchange processes. Although participants acknowledged having good working relationships with their counterparts, there were still concerns about how to ensure consistent participation and engagement between LHDs and hospitals. For instance, one LHD official expressed, “Getting them to consistently participate in the meetings and have them lead some of the work groups have been a challenge.” (LHD Official 6)
Another LHD official stated, “The data that is included in their (hospital) very sophisticated electronic health record is just not made very available to us as public health for population management like for opioid overdoses or for any other conditions that they may be seeing arise.” (LHD Official 3)
Communication Breakdown and Duplication of Services
A diverse group of stakeholders is one of the most important components of the CI model; in particular, the model highlights the need to acknowledge each organization’s capacity to perform separate but “mutually reinforcing activities” to achieve success. Although some necessary overlap exists in services provided by LHDs and hospitals, several participants identified program/service duplication as a concern; in many instances, they attributed this overlap to communication breakdowns. For example, one nursing administrator from a lower-performing community stated: I think sometimes we work on the same problems, and we do that separately. … Probably just a lack of knowledge really at the hospital of what we do here at the health department. And probably us not reaching out to them like we should to let them know what we do. Same as us for them. I don’t really know what they have or who they have out there working on prevention and health education and stuff like that in the community. I guess we don’t have that direct line because nobody has ever asked. We haven’t asked them; they haven’t asked us. (LHD Official1)
Additionally, another LHD director stated: One of the things that initially was an issue and something that we have continued to keep an eye on is to ensure that we are not duplicating services. People get really protective of their work arena. (LHD Official 11)
Time Constraints
Continuous communication, the fourth requisite of CI, is designed to support collaboration while building trust between stakeholders. Respondents identified time constraints as the most relevant barrier to maintaining regular contact with local hospitals. Participants attributed time constraints to several factors, including lack of staff, competing interests, and insufficient planning. For many, finding time to attend meetings or participate in a project with hospitals was difficult and put a strain on how effectively they could perform. One LHD official described the challenge as follows: It’s just, you know, it takes time. Relationship building takes time. And you have to work on it, and you have to maintain it and you have to nurture those relationships so that you can continue to work together and have a positive effect collectively. (LHD Official 6)
Another LHD official stated: Sometimes, I guess the challenge may be that they are busy, and they may not always have the staffing to participate in some of our community partnership meetings that we’ve had. That has been a challenge at times, just getting them to the table sometimes for some of the meetings that we have. A lot of it is that they are busy, and we understand that. (LHD Official 5)
Lack of Financial and Human Resources
The CI model describes a strong “backbone” of financial and staff support as a necessary condition for effective collaboration. If partnering organizations are underfunded or have limited staff to dedicate time to the larger collaboration, this condition is unachievable. In the present study, LHD officials described how a lack of sufficient funds and reductions in budgets affected their ability to recruit staff and dedicate their time to collaborative endeavors. Although some received small grants and other funding from hospitals or other sources for collaborative projects, most participants explained that the lack of financial and human resources compromised the sustainability of their projects. For example, one LHD nursing supervisor recounted: You know when you don’t have the funding to be able to hire a new person to do a new project, then your project does not have a good foundation to continue. I think that is the biggest challenge. When you start something for the community, our goal is to be able to continue that for years. That is the challenge; it is almost impossible to think that you can do that with budget cuts and staff. (LHD Official 3)
Facilitators of Effective Collaboration Between LHDs and Hospitals
Study participants who reported effective collaboration with hospital partners identified several factors that helped facilitate healthy collaboration. As in the previous section, these observations aligned with conditions outlined in the CI model.
Finding Common Ground
A “shared agenda” is the first requisite of CI. Several participants described how finding common priorities helped to facilitate collaboration with local hospitals. Finding common ground was described in several ways. For instance, one participant described how they have come to accept the relationship as give and take. Another participant pointed out that making the other sector aware of their role was a critical piece to having a good working relationship: “We work more and actually help them understand the role that public health has. We are not in competition...They have a role, and we have a role, and we work together.” (LHD Official 6)
Another LHD official stated: “Finding those common places where the hospital system is interested in trying to improve the health of their patient and we are interested in trying to improve the care of their health community and seeing where those overlap.” (LHD Official 8)
Well-Established Relationships
According to the CI model, once a common agenda is found, seeking out ways to share results and data between organizations is another necessary step toward systems-level partnership. To this end, participants described how having a good relationship with providers in the hospital made it easier to achieve cooperation, including the sharing of data and other resources: I guess in my personal view I worked for the hospital for many years. I think that has been helpful to the collaboration. They know me personally, and I work here. They kind of know where I am coming from, so I think that is helpful when we are in a small community and the relationship I kind of have that already built. (LHD Official 3)
Another LHD official stated: It is very hard to be able to pay for the quality IT services that we need to secure our data. So, the hospital stepped up and we actually contract with the hospital, and they provide the expertise [to] our IT staff and then we pay the hospital, but they maintain the level of expertise that we need. So that has been marvelous. As well as through our electronic health record. They have given us such a substantial discount on our EHR, so we are able to share data that way through EHR with the hospital. (LHD Official 2)
Aligning and Leveraging Resources
The recognition of the importance of each partnering organization’s strong points, appreciation of the team’s diversity, and engagement in “mutually reinforcing activities” are crucial to elevating collaborative capacity. Some LHD officials described how they were able to build a strong collaboration with their region’s hospital by reaching a mutual understanding of each other’s strengths: “They are a very good partner for us, very valued. We’ve been able to use each other’s strengths and build off each other…We have been able to build those partnerships so that we can work together.” (LHD Official 8)
Participants noted that, although administrative priorities differed between LHDs and hospitals, the process of and outcomes resulting from a jointly conducted CHNA can help align priorities between the two organizations. From their perspective, this alignment was critical to forming action plans with the potential to improve community health. One participant explained that established CHNA collaboration enabled the quick pooling of resources to address the opioid crisis in their community: So, the opioid crisis here locally is not as profound as some other areas of the state. But once we made a decision, we needed to act before ours got as bad. It was very easy to call people to the table. Because we already have those relationships, and you are not trying to rebuild those relationships over time. (LHD Official 4)
Open Communication
CI’s emphasis on “continuous communication” recognizes that relationship-building between organizations requires spending time together on a consistent basis. LHD officials expressed how open communication had helped to facilitate collaboration between LHDs and hospitals. Specifically, LHD officials described taking an active role in initiating and ensuring an open line of communication; one LHD official related: We’ve got real open lines of communication. We keep in touch with each other and involve each other when we’ve got different meetings and outreach that we have going on. We try to make contact with them and keep that door open for us to be able to be together. (LHD Official 5)
LHD officials also described how maintaining regularly scheduled meetings provided an opportunity to keep abreast of changes in programs or services and address the service gaps identified. Although there were concerns about communication breakdowns in some instances, having an open line of communication made it easier to respond to feedback and changing circumstances while also maintaining rapport between the organizations: Because there is a set monthly meeting, and it gives us really good access to other services that we may or may not be aware of that are available because they are changing depending on the federal funding. …. We have worked with each other in different areas, and I just think it has a good personality to it, and we get along well. And I think we do a really good job of filling in the gaps what we discover and through those meetings. (LHD Official 11)
Leadership Commitment
The final condition of CI, “backbone support organization,” pertains to the organizational demands of maintaining collaboration. Even if some LHDs did not have high levels of funding or dedicated staff, participants expressed that, in their best experiences working with hospitals, LHD leadership managed to create a sustainable framework for collaboration by making sure that collaborative activities were implemented at each level and across organizational units: We have established relationships with them at the higher levels, administrative levels but also at lower levels … But to improve and expand those relationships, I started at the top and I went to the administrators, and I spoke with them and talked to them about how we can work together, and then it drizzled down. (LHD Official 6)
LHD officials also pointed out how organizational leaders, their backgrounds, and their level of commitment to LHD-hospital partnerships were crucial to facilitating collaboration. They believed that leadership was a major contributing factor to establishing successful collaboration, as another LHD official shared: It really depends on your hospital administration and the administration at your health department, whether they want to form that relationship or not. Right now, we’ve got some very good administrators at both hospitals that make it more easy for us to be able to work with them. (LHD Official 5)
LHD officials recognized how their own experiences helped establish collaborations with hospitals. One participant indicated that maintaining contacts from prior interactions with a hospital made it easier to reach out and engage in collaborative activities with that same hospital: “I worked at the hospital for 25 years before I came here, and I know a lot of the personnel that are still there, that helps tremendously.” (LHD Official 7)
Discussion
The Public Health 3.0 model has been championed as a mechanism for expanding traditional LHD functions and programs to better meet community needs. A central component of operationalizing this model is facilitating greater integrations between LHDs and private/public hospitals.1–3 To date, however, there is little evidence of any meaningful change in the number and/or quality of LHD-hospital partnerships across the U.S., which some have argued negatively impacted community-level responses to the COVID-19 pandemic.43,44 In order to better understand why such changes have not occurred and help encourage them in the future, the present study sought to identify some of the fundamental obstacles faced by LHDs seeking to better serve their community and establish working relationships with local hospitals; it also drew upon the CI model to investigate how LHDs and hospitals might use the components of effective collaborations to foster improved relationships.
Findings suggest that LHDs face difficulties establishing long-term, productive relationships with local hospitals where they can work together to fulfill common goals. In particular, they highlight a lack of consistent funding, and consequent understaffing, as detrimental to fulfilling larger project goals, mainly because personnel are limited in the time they can dedicate to collaborative efforts. On the other hand, LHDs who reported successful collaborations attributed their successes largely to well-trained leaders committed to building relationships with potential partners as well as to investing the time and energy necessary to effectively share resources essential to realizing the shared goal of improved community health.
Consistent with these findings, a recent practice report, authored by Brandert et al., 45 notes that “[w]ith the decline in numbers of state and local public health professionals in practice and the growing complexities of their work, the need for adaptive and collaborative leaders able to work across sectors to address community and system challenges has never been more apparent” (p. S210); the authors go on to highlight the importance of and positive outcomes associated with public health leadership institutes. This sentiment is also consistent with a recent article by Rukchart et al., 46 which reported the findings of a cross-sectional study that asked 410 public health leaders to rate the skills that were most important for new public health graduates as they transition into the professional world. The two highest ranked competencies were vision-grounded skills (i.e., the ability to understand/support an organization’s mission and vision) and collaboration skills (i.e., the ability to coordinate with others and work in a team). 46
Study results further indicate that LHDs and hospitals’ attempts to collaborate often fail to address basic conditions for building effective partnerships, as identified by the CI model. For example, while all participants indicated that they had actively collaborated with local hospitals, it was unclear that any of these partnerships had fulfilled the second CI condition (shared systems of measurement), complicating assessments of efficacy. Several LHD officials commented on how difficult it was to maintain regular communication between agencies, explaining that their hospital partners were “too busy” to commit to consistent meetings. Finally, data indicate that many LHDs lack the staff and funding to serve as backbone support (the fifth CI condition) for larger collaborative efforts. Although hospitals may be enthusiastic about working with local public health partners, study participants suggest hospitals do not lend their greater organizational structure to supporting collaborations with LHDs.
The CI conditions that were reported to be most effectively engaged were those pertaining to agencies with strong leadership committed to participating in the shared effort by engaging in “continuous communication” (the fourth CI condition). By undertaking ongoing efforts to build relationships with partners, these officials find common ground and are more likely to forge a “common agenda” (the first CI condition). Consistent with this study, a growing number of studies exploring collaborations between public health and healthcare systems in developed countries have identified leadership and management support as common conditions for successful collaboration.24,25,47,48 Studies, such as Scutchfield’s 49 work on public health agency capacity, the multi-level study by Cramer et al., 19 and the literature review by Erwin 23 suggest a positive association between organizational leadership within LHDs and improved performance outcomes. Our study also indicates that well-established relationships between LHD officials and hospital leaders is a critical component of effective LHD-hospital collaboration. Studies of organizations using the CI model to structure their collaborations show similarly high performance in public health and educational endeavors.31,32,35
While a growing number of collaborative initiatives exist between local health departments and hospitals,20,22,50 evidence indicates that it has been challenging to sustain this collaborative approach across communities in the U.S. 2 Our results demonstrate that a lack of financial and human resources may be a barrier to effective collaboration between LHDs and hospitals. LHD officials expressed how the lack of grants or other funding as well as budget and staffing cuts had negatively impacted the sustainability of their collaborative projects. Previous cross-sectional and prospective studies have found that LHDs with increased spending or higher budgets and staffing achieve better performance and outcomes.51,52
A contemporary example that supports many of the findings reported here is the COVID Positive Pathway –– “a practical collaboration between public health authorities, primary care practices, primary health networks, and hospital services” (p. 418) in the area surrounding Melbourne, located in the southeastern Australian state of Victoria. 53 Although a detailed description of the program is beyond the scope of this article, Lim and colleagues’ 53 findings suggest that –– by working across healthcare sectors to facilitate testing, provider education, contact tracing, and disease progression risk assessment –– the COVID Positive Pathway was able to meet the care of needs of approximately 80% of those testing positive for COVID-19 in the region via primary care and other community health organizations; this support allowed hospital services to be reserved for people with more severe illness or with risk factors for disease progression. Importantly, the authors argue the program’s success was facilitated by adequate, centralized funding, data-sharing among various entities, and an implementation process that “was refined iteratively at once or twice weekly meetings of all collaborators” (p. 414).
One of our participants’ most noted collaboration points between LHDs and hospitals was CHNA. Since the inception of the Affordable Care Act in 2010, nonprofit hospitals are required to perform CHNAs, and thus there is a growing body of research around CHNA projects. 20 Some states, like New York and Massachusetts, have taken additional steps to leverage the ACA provision by requiring or promoting collaboration between nonprofit hospitals and LHDs in CHNA processes.21,54 More recently, Ohio has encouraged LHDs to develop community health assessments (CHAs) and community health improvement plans (CHIPs) in collaboration with nonprofit hospitals. 54 Most of the relevant research indicates that collaborations between LHDs and hospitals on CHNAs are linked to improved community health outcomes.14,20,26,50 Bommersbach et al. 55 argues that conducting a CHNA, as well as funding mental health and substance use treatment and prevention efforts, are important opportunities for LHDs and hospitals to build lasting collaborations and make meaningful progress addressing their communities’ public health challenges.
Limitations
This study has a few important limitations. LHD officials are a challenging population to recruit, given their many responsibilities and obligations, which accounts for the small sample size (n = 12). We attempted to address this limitation by conducting detailed, in-depth interviews to obtain the richest data possible and engaging in member checking. While the sample size is small, it is consistent with other studies of hard-to-access populations.56,57 A further limitation was that the recruitment of participants came from primarily urban counties. No LHD officials from rural counties with <2500 population agreed to participate. Small communities have been underrepresented in similar studies, but there are efforts underway to bridge the urban-rural divide in health assessments and collaborations, 58 some focusing specifically on rural regions and other vulnerable populations.57,59 Additionally, although our sampling strategy distinguished between LHDs in high- and low-performing communities, the limited sample size prevented meaningful comparisons between these groups. Future research could explore this distinction more explicitly, especially in larger or more geographically diverse samples. Nonetheless, the results of this study may be transferable to similar urban counties as well as LHDs in urban counties with similar opportunities and challenges for hospital collaborations.
Implications and Conclusion
Given the public health emergencies presented by the concomitant rise in chronic health and infectious disease illnesses, the CI model’s approach to understanding the barriers and the facilitators to systems-level collaboration is critical to making greater strides in addressing the variety of public health threats. 30 Data from this study and others indicate that despite a growing recognition of the benefits of collaboration between LHDs and hospitals, systems-level collaboration remains limited and suboptimal. Results from this study suggest several contextual and organizational factors that may hinder successful collaborative efforts or motivate continuing successful alliances between LHDs and nonprofit hospitals. Results from this study also suggest the need for LHDs and hospitals to pursue more formalized collaboration and arrangements including service and resource sharing (i.e., of data and personnel), or joint programs and services to minimize duplication of services. 60 A previous observational study showed that while many LHDs are involved in simple exchange of information and regular meetings with hospitals, few are involved in more formalized written agreements or sharing of resources and personnel with hospitals. 61 Research on the impact of LHD-hospital collaboration around CHNA on population health is limited and should be further explored. It is our intent that the results of this study inspire greater exploration into the causes of collaborative failure, as well as both systemic and situational remedies for those breakdowns. Cross-sector collaboration is a necessary component of public health efforts, and their success or failure will affect population health for decades to come. Determining practical strategies for collaborative problem solving and improving synergy between LHDs and hospitals are critical steps toward the enhancement of community health outcomes.
Footnotes
Author Contributions
OI: Conceptualization, Data collection, Methodology, Formal Analysis, Writing, Validation, Project administration; SK: Conceptualization, Methodology, Writing; MS: Validation, Writing; CE: Validation, Writing, EC: Conceptualization, Methodology, Validation; PD: Validation, Writing, Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Appendix
(1) What is your role in your organization? (2) How would you describe if any, how your local health department collaborates with hospitals to improve the health of your community? Probe: How would you describe the strength of the collaboration between your health department and hospitals within your community? (3) What has helped to improve/ maintain the collaboration you have with your health department? Probe: Who are the major stakeholders? (4) What are some of the barriers your health department has had with regards to collaboration with hospitals? Probes: (a) What have been some of the challenges to maintaining effective collaboration or partnership? (b) How would you describe the challenges your health department has faced when it comes to collaboration with hospitals? (c) How would you describe the challenges your health department has faced when it comes to working with hospitals to improve population health? (5) How would you describe what has been accomplished because of your collaboration with your health department? Probe: How do you measure the success of your collaboration with your health department? (6) For our study, we are interested in learning more about experiences of conducting a community health needs assessment with nonprofit hospitals if one has been done. How would you describe the overall process? Probes: (a) How important do you think local health departments should collaborate with hospitals to conduct a community health needs assessment? (b) What was learned? (c) In your opinion, what are the benefits? (7) In what areas are you working with hospitals to improve population health? Probes: (a) In what ways are you working hospitals to address preventable hospital readmissions? (b) In what ways are you working with hospitals to care for the elderly? (c) In what ways are you working with hospitals to address the opioid epidemic? (d) In what ways are you working with the hospitals to improve community mental health? (e) Which other partners are you collaborating with in the community to improve health outcomes? (8) In what major area would you like to see more collaborative work between your hospital and your health departments? Probe: What is a major public health concern you think should be addressed in your community? (9) Is there anything else you would like to share with me?