
Abstract
Despite men’s health playing a significant role in the well-being of infants, children, and women, there is a gap in maternal and child health research which more broadly considers men’s health as a component of family’s and community’s overall well-being and for the sake of men’s own health and well-being, particularly from the perspective of men with marginalized identities, such as Black men, and community members. Therefore, our community-based participatory research study aimed to explore what community members perceive as protective and risk factors for the general health of men in a low-income community using a generic qualitative approach with focus groups and thematic analysis. We identified six protective factor themes (health behaviors, economic stability, expected male responsibilities, healthcare engagement, social network, and faith, spirituality, and driving forces), as well as six risk factor themes (health behaviors, impact of mentorship, experience of driving forces, healthcare avoidance, mental health concerns, and systemic bias, racism, and social inequity). There are actionable steps public health practitioners and policymakers should prioritize, including addressing structural barriers to men’s health, such as by combating discrimination and increasing access to healthcare, removing barriers to mental health care, and creating opportunities for increased social support. These strategies can give way to greater opportunities for men to engage in protective behaviors that can both improve their health across the life-course and positively impact the health of mothers, infants, children, and communities.
Keywords
Introduction
Men and fathers have an important influence on infant and child health outcomes, maternal health outcomes, family health, and overall community health.1–3 Father’s/men’s health can have positive direct and indirect impacts on maternal and child health through family planning, enhanced paternal biologic contributions, improved reproductive health practices and outcomes for women, and improved capacity for parenthood/fatherhood.3,4 For children and adolescents, father involvement is associated with improved socioemotional development and academic achievement and fewer behavior problems. 5 A study using nationally representative data found significantly greater odds of poor physical and mental health among children of fathers with poor physical and mental health, 6 directly speaking to the relationship between father’s and children’s health outcomes. Furthermore, male partners provide social support and may reduce stress-related problems in pregnancy. 7
Due to the important role men play in maternal and child health, there has been a greater focus recently in public health research and practice to enhance paternal involvement and include males in maternal and child health programs,8,9 particularly in lower-income African American neighborhoods, where disparities in maternal and child health outcomes are the most pronounced. Therefore, men’s health in these communities must be nurtured and supported. We suggest a life-course, multi-level approach to maternal and child health to improve father and male involvement. Community-based organizations that previously focused primarily on improving the health of mothers and children have expanded to focus on men’s health and father involvement. 2 REACHUP, Inc. is a 501c3 not-for-profit organization providing healthy start services in a historically underserved area of Tampa, FL, USA.2,10,11 REACHUP utilizes a strengths-focused, community-based, multi-level approach to improve male involvement, family resilience, and community capacity.2,11 REACHUP focuses on improving men’s and father’s health and well-being through programs that provide leadership and mentorship and enhance self-esteem, health, and well-being.2,11,25 A study of REACHUP 24/7 fatherhood involvement program reported that many men who participated in this program identified as grandfathers, uncles, and family friends, which indicated that male involvement programs can have benefits for men who are not biological fathers but who take on paternal roles. 2
Recent research that came from the women’s preconception health movement has expanded the fatherhood paradigm to create a focus on men’s roles in preconception health and health care to improve maternal and child health outcomes and men’s own health and well-being. 4 This focus on men’s preconception health means focusing on men’s health prior to a partner’s pregnancy and throughout their entire life. 4 Research in this area is currently very limited and is still primarily focused on how men influence women’s and children’s health. 4 The life-course approach is a valuable framework for maternal and child health that can be used to conceptualize how men’s (as much as women’s) life-course health impacts maternal, infant, and child health and now men’s own health and well-being. 4 This represents a paradigm shift in the maternal and child health field to a focus on improving men’s health for both reproductive outcomes and the sake of nurturing men’s own health. 4 For example, Kotelchuck and Lu 4 presented a men’s maternal and child health life-course model to conceptualize men’s overall health risk and protective factors; whereas Davis et al. 12 suggested that including men in maternal and child health services presents a unique opportunity to provide men with preventative health information they may otherwise be missing. Moreover, one of the Healthy People 2030 goals is to “improve health and well-being for men” as men have shorter life expectancies and are at higher risk for many serious diseases than women. 13
Most current studies, however, still present the outlook that male involvement is a contributing variable to maternal and child health outcomes, rather than seeing male health as a component of a family’s and community’s overall well-being. Studies that look at men’s health are often comparing the gendered roles between men and women, rather than openly looking at all components of men’s health.14–16 Additionally, there are gaps in the research concerning the impacts of systemic bias on men’s health or health disparities men, and particularly marginalized men, face. 17 Though there are expected intersectional relationships among sex, gender, race, ethnicity, and male health, 18 it is important to investigate the perceived hindering and enabling factors that affect men’s health independent from women’s health.
However, though it is important to investigate men’s health independent of its relationship to women’s and children’s health, it is also important to gather community input because sex-specific health does not exist in a silo.
As such, although we know that men play a significant role in maternal and child health, we know much less about the specific risk and protective factors that affect the health of men in low-income communities. To improve men’s health and father involvement, we need to focus on men’s overall health and well-being. The majority of studies have focused on perspectives from women and mothers; few studies have focused on men’s perspectives on pregnancy and maternal, infant, and child health.19,20 Quinn et al. 20 in a qualitative study of men’s perspectives on Black infant mortality, suggested that future research should focus on perspectives of community members on protective factors for improving community health. Although Quinn and colleagues 20 examined men’s perspectives on maternal and child health, we found no studies that examined community perspectives on men’s health in the context of maternal and child health. Since little is known about marginalized communities’ perspectives on culturally relevant ways to improve men’s health, this study used community-based participatory research (CBPR) and the life-course perspective to examine community residents’ perspectives of men’s risk and protective health factors in a low-income community of color in Tampa, FL. Our study aimed to explore what adult community members perceive as risk and protective factors for the general health of men in their community. By using a CBPR approach, we were able to elicit shared perspectives of men’s health from community members living in marginalized communities. Men’s health within this study was part of the larger project which examined risk and protective factors of community members within the target community at all life stages, including women, children, adolescents, and older adults in the community.
It is important to note that, although the original project was fully participatory and Community Advisory Board (CAB) members and academic researchers made all decisions together at planning, collection, and analysis stages, the current study is a sub-analysis of qualitative data from the original project, so it is less participatory than the original, larger study.
This sub-analysis of four focus groups were analyzed by two primary independent coders (second author and third author) who were not involved in the original project. A third researcher (first author) who was also not involved in the original project, led the writing of the manuscript. Author sixteen, who was also not involved in the original study, also assisted with writing the manuscript. This process was supervised by the fourth author, who has been involved in the project since the beginning and was mentoring the new authors (students at the time of the analysis and writing) on this sub-analysis. Although the first four authors and the sixteenth author completed the majority of work on this sub-analysis, they were in contact throughout the process with the remaining authors, including the original academic researchers (fourth author, fifth author, sixth author, and last author) and all of the original community advisory board members (seventh author, eighth author, nineth author, tenth author, eleventh author, twelfth author, thirteenth author, fourteenth author, and fifteenth author).
We presented the initial themes and preliminary results to several members of the CAB for member check validation, and several rounds of refinement by those CAB members were made for this study. We also shared the drafts of this manuscript with the entire CAB for input. We recognize that our qualitative analysis was less participatory than the original study; however, it was not feasible for us to ensure the same level of engagement as during the larger project, which was conducted several years ago, but all original academic and community researchers are authors on this manuscript and involved in this sub-analysis/sub-project.
Methods
This generic qualitative study utilizes data generated from a larger mixed methods CBPR project titled, “Toward Eliminating Disparities in Maternal and Child Health Populations.” The larger study’s efforts were funded by the National Institute on Minority Health and Health Disparities through an R24 grant on ‘‘Community-Based Participatory Research” (Award#: 5R24MD8056-02). Full details outlining the larger study’s specific methodology have been previously described elsewhere.10,21–23,26 For the larger CBPR project, participants were recruited from target urban communities within Hillsborough County, FL, USA. The larger study was built upon an existing 20-year community-academic partnership between REACHUP and the University of South Florida (USF).23,24 REACHUP is a community-based 501(c)3 non-profit organization in Tampa, FL with the mission of providing services and support to mothers and children within their community. REACHUP and USF have collaborated extensively in CBPR initiatives and projects that have contributed to positive maternal and child health outcomes within their community.3,23–25 Employing a CBPR approach, study staff created a Community Advisory Board (CAB), which consisted of eight active community members living within our target communities and who represented the racial and ethnic diversity of the community. CAB members were community leaders nominated by REACHUP, many of whom had worked on previous CBPR projects and had extensive expertise in community engagement.24,25
CAB members served as gatekeepers between the academic research team and the larger community. In the larger project, in order to ensure equal participation among community members and academic researchers, the entire team of academic and community researchers (CAB members) participated in CBPR training sessions, bi-weekly project meetings, and completed a human subjects protection course. CAB members fully participated in the conceptualization of the study and the process of creating the overall aims and sub-aims of the project. The data collection instruments (focus group questioning guide) were designed and refined by CAB members and the CAB led the recruitment of participants and conducted the focus groups. Details about the development of the CAB and their qualifications have also been described in more details in previously published manuscripts from this project.10,21–23,26
Purposeful sampling was used in the larger study; trained community members recruited participants through word of mouth, emails, flyers, social media, and social networks. Purposeful sampling aims to specifically target individuals who are knowledgeable and experienced within the phenomenon of interest. 27 This sampling strategy seeks to elicit information-rich discussion as to obtain the most information about the inquiry of interest. 28 Within the larger project, trained community members conducted 10 focus groups with participants. All focus groups were audio recorded and transcribed verbatim by a trained community member. To maintain confidentiality, any identifiable information such as name and age was removed from the transcript.
The focus groups were all conducted by trained community members and used semi-structured questioning guides. Informed consent was obtained, and $20 incentives were provided (an amount deemed acceptable and non-coercive by the CAB) to each participant. The focus groups were composed of English-speaking adult community members. The questions of interest within the focus group discussion included (1) For adult men in this community, what makes it difficult for them to be at their best health?; and (2) For fathers/men in this community, what would you say help them maintain their health? Only responses and discussion to these two questions were analyzed. We chose to use a generic qualitative approach because it allows for the exploration of participants’ firsthand experiences and is flexible and well-suited for research questions that are pragmatic in nature.29,30 We conducted thematic analysis using inductive coding. 31 We chose thematic analysis because it is a flexible approach that can lead to a rich analysis of the perspectives of community members. 31 First, two independent coders (who were not involved in the original, larger CBPR project) familiarized themselves with the data, reading over the transcripts several times. Next, they hand coded the transcripts sentence-by-sentence and organized their codes into higher order themes, categories, and subcategories using Excel to organize their findings. Upon conclusion of the individual review, the two coders discussed and negotiated until agreed upon themes, categories, and subcategories were identified. In instances where the two coders could not come to consensus, a third researcher from the team was asked to serve as the tiebreaker. The coders worked toward inductive thematic saturation, meaning they coded until no new codes or themes emerged from the data. 32 Upon the finalization of themes, categories, and subthemes, the two coders collaborated to provide operational definitions for each item.
Aligned with CBPR methodology, the final themes, categories, and subthemes from the initial analysis were shared with members of the CAB, where further feedback was obtained regarding the refinement of themes, language and operational definitions. The original two researchers then reconciled CAB feedback with the original analysis, thus resulting in the final themes, categories, and subthemes along with their operational definitions. This process was completed several times to ensure a thorough understanding of the CAB members’ feedback, and the CAB members reviewed and approved the final results presented in this manuscript. All authors (including all of those from the larger project as well as the four authors who led the sub-analysis, who were not involved in original project) edited and approved the qualitative findings, manuscript drafts, and the final version of this manuscript. This original study was reviewed and approved by the University of South Florida IRB (IRB#: Pro 00010288) and the sub-study was later approved by the University of Florida IRB (#IRB202000540).
Results
The original project collected sociodemographic data across the 10 original focus groups, with a total of 78 community members participating across the 10 groups. Since this is a sub-analysis, we were not able to collect demographics for these four focus groups. We provide this information for the entire project, but unfortunately, we are unable to provide it for the four focus groups as the original project collected demographic information across the entire sample. Across the entire project, 43.6% of participants were 41 and older, 46.1% were 19–40, and 10.3% were 12–18 years old. Additionally, 61.3% of the participants across the entire sample were female and 79.5% were not Hispanic or Latino. Over 61% of the participants were Black and 25.6% were white, with the remaining being other.
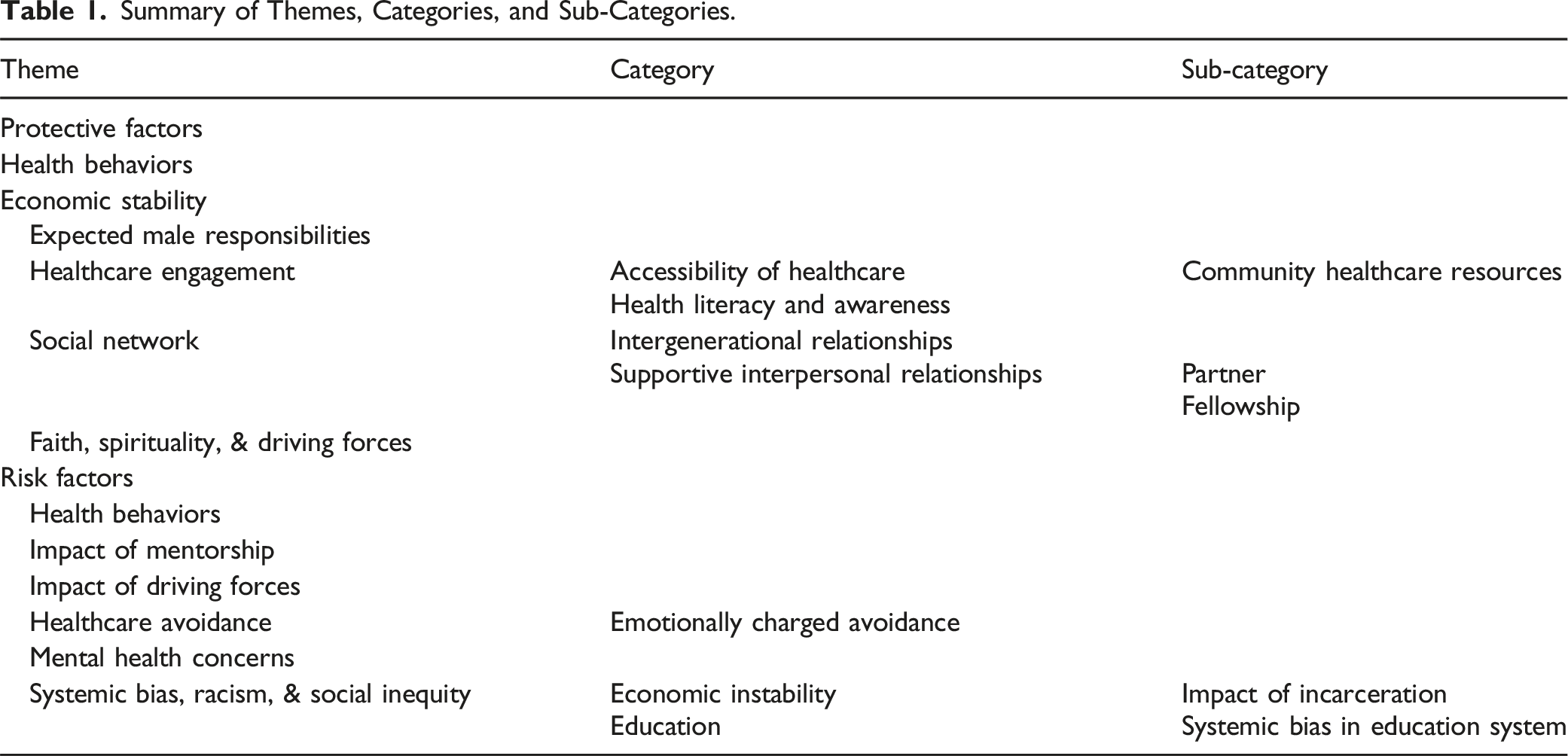
Summary of Themes, Categories, and Sub-Categories.
Protective Factors
Health Behaviors
The first theme identified was ‘Health Behaviors.’ This theme depicts actions (e.g., diet, exercise, smoking cessation and regular healthcare access) that positively affect an individual’s health. One participant overtly described these behaviors as beneficial or protective over one’s health, “Exercising and, you know, eating right, stop smoking,” while another participant discussed a variation of physical activity that would serve as a protective factor, “However, if you go to the community basketball court, you do see a lot of our brothers out there, and that’s exercise, that’s their Sunday routine where they go out and they play a few courts and, you know, they’ll do whatever and that’s their exercise for the week. You know?”
Economic Stability
A second protective factor identified was ‘Economic Stability,’ defined as access to financial resources, quality housing and food, and stable employment with an acceptable wage that improve one’s ability to maintain positive health behaviors. This theme embodied community members’ belief that by obtaining economic stability, largely discussed in terms of employment, there would be a distal effect of men having the opportunity to tend to their health. One participant depicted this by stating, “And so they got to have jobs. They need jobs. That’s what they need so they can go to work just like everybody else and then they can pay their bills and then they can make better choices, you know?”
Expected Male Responsibilities
In addition to the previously stated themes, ‘Expected Male Responsibilities’ was an emergent theme that specifically noted gendered protective factors. This theme entails cultural expectations of males to be the leader and provider in their households. One community member noted, “I think that the man should be in a leadership position, and if he’s doing right toward that woman, then that’s going to be healthy for the family, and then the woman going to respect him more.” This theme highlights the perceived benefits of feeling respected by family and community members for men who hold these roles, as well as the broader benefits to his family and those he is able to guide and provide support for.
Healthcare Engagement
The fourth identified theme was ‘Healthcare Engagement,’ which contains two additional categories and one sub-category. ‘Healthcare Engagement’ encompasses active participation in one’s healthcare and factors that enable them to do so. One community member stated, “You know, before men didn’t look at the fact that they have cancer just as much as women do. So I know a lot of men who go and get their checkups, you know,” demonstrating one aspect of engagement. Within this theme, ‘Accessibility of Healthcare’ was noted as a category, which describes factors that promote an individual’s ability to obtain healthcare, including but not limited to financial resources and health insurance coverage. One community participant shared their experience observing men seeking healthcare through their local offices, “I actually have county insurance myself, and I’ve seen men come to the county office that I go to, and they…whether they have insurance or not, they come in and they see the doctor. I’ve seen men that just come pay. And that’s been a big deal. Black men. It’s been a big deal to me to see that, you know, it’s just been amazing.” This quote draws attention to potential differences in insurance coverage for men of color, as well as possible barriers or hesitations that may have limited them from accessing healthcare in the past. Within ‘Accessibility of Healthcare’ a sub-category was developed to note the prevalence of ‘Community healthcare resources.’ This sub-category encompasses formal community resources that are currently present and provide direct healthcare or access to health services. One example provided by a participant was, “Anyone that does not have insurance can go to the Christian Judeo Clinic and they will wait on you whether you have insurance or not.” Another participant discussed additional local services that assisted in accessibility to healthcare efforts, “Because there’s many places that offer free care and have been for many years like the Shriners and the Lions Club and…” The final emergent category under ‘Healthcare engagement’ is ‘Health Literacy and Awareness,’ operationalized as knowledge and recognition related to an individual’s own physical and mental health. One participant expressed their individual health literacy and awareness by stating, “I got hurt and everything and that made me aware of myself and my…all my medical attention. You know, you need to take a look out on this part of your body, you need to make sure this is okay….I explained as I went on to different guys and stuff, what you need to do to maintain your body, maintain all your medical and everything, check each body part, not just one part, your whole body.” The entirety of the ‘Healthcare Engagement’ theme demonstrates a shared effort from individuals and the community, thus providing a multi-faceted protective factor.
Social Network
‘Social Network,’ defined as a community system of personal relationships and social engagements/interactions, was one of the more commonly discussed themes among community members. Participants expressed the importance of positive relationships for men to achieve good health. One community participant stated, “That’s the good mind settlin’ point to have, when you know you got support from your family or from some friends or whatever, if you don’t have any family, it goes around or, you know, whatever.” As described by this participant, both family and friend support were prevalent among discussion, thus leading to the development of two categories: ‘Intergenerational Relationships’ and ‘Supportive Interpersonal Relationship.’ ‘Intergenerational Relationships’ represent the perceived importance of males demonstrating positive health and life behaviors for their children, families or others that expand across generations. One male participant specifically expressed, “And we as men, the more we help those along the way coming behind us to get character I think would be the greatest that we could give to them.” This demonstrates an external motivation to serve as a role model to other men within their community. In addition, another participant expressed how men demonstrating positive health behaviors provides a sense of positive modeling for community youth, “And a lot of times if our men are doing positive things and healthy things for themselves, then our children certainly want to mimic what they see daddy doing, whether it’s a boy or girl.” Ultimately, this category depicts the desire and achievement of passing along healthy ideals to others. Though similar, the meaning captured in this theme reflecting the intergenerational role males may play as mentors within their family and community was identified as distinct by the members of the CAB to that of the theme ‘Supportive Interpersonal Relationships’, which is defined as relationships that offer tangible and emotional support and encourage or enable positive health behaviors. This category is further broken down into two sub-categories: ‘Partner’ and ‘Fellowship.’ ‘Partner’ depicts relationships with family and partners that offer tangible and emotional support and encourage or enable positive health behaviors. One participant stated, “Also, too, that woman in your life, your wife, your girlfriend, whoever, she needs to support her man. That’s right. She need to push her man, make her man feel good about himself, let him know he’s the best in whatever he’s doing.” Comparatively, ‘Fellowship’ is community relationships with males or other peers that offer tangible and emotional support and encourage or enable positive health behaviors. A participant suggested, “I think like a men’s support group with, you know, to be able to talk to other men with similar health issues or, you know, just to be able to relate.” The ‘Supportive Interpersonal Relationship’ category, as further defined by the sub-categories, demonstrates the desire and need for multiple avenues and relationships of support to be successful at achieving good health.
Faith, Spirituality, & Driving Forces
The final protective factor theme identified was ‘Faith, Spirituality, & Driving Forces’ which represents internal and external factors that encourage an individual to engage in positive behaviors, including motivation related to family and religious/spiritual drivers. One participant summarized this theme by stating, “If you got a strong motivator, that motivator going to push you to do, you know what I’m saying, what you destined to do, you’re going to do it. You know what I’m saying?”
Risk Factors
Health Behaviors
Parallel to the protective factor of ‘Health Behaviors,’ participants outlined that ‘Health Behaviors’ can also serve as a risk factor that hinders achieving good health. This was defined as actions (e.g., smoking, poor nutrition, limited physical activity) that negatively affect the individual’s health. One participant outlined specific behaviors that could negatively impact health, “When they out there doing things they shouldn’t be doing. Well, that’s probably what I would say make them [unhealthy]…Well, drugs, that [they] take… Not eating right. Not getting the proper rest.” In addition, one participant described a decrease in a health behavior, “Because a lot, especially the Black men, they don’t exercise like they used to.” This statement indicates a belief that Black men specifically may have fewer opportunities to engage in exercise than they have in the past.
Impact of Mentorship
‘Impact of Mentorship,’ or the role of guidance from an individual outside of one’s family that can provide support and advice on issues such as health and professional development, was discussed by a handful of participants. One participant overtly stated that there is a lack of mentoring, “But there’s not enough positive mentoring or role model in the community.” In contrast, one participant defined the changing role of mentorship within a professional domain, “You [previously] had doctors, lawyer, teachers in the community. Right now there’s no… It’s hard to find. I’m not saying there’s no, but it’s hard to find that. And you don’t have to be a professional to be a role model. But it’s hard to find that in the community.” Participants felt that without guidance from predeceasing figures, they were at an increased risk of poor health outcomes.
Experience of Driving Forces
The internal and external catalysts that encourage an individual to partake in a specific task or behavior or ‘Experience of Driving Forces’ was discussed among community members. One participant stated, “Men are just that way, they just… They don’t want to just… They don’t just take the initiative to do stuff.” Another participant provided further context as to what they believed caused a hinderance to motivation, “And in the community, it’s a lot of the Black men want fast money and don’t want to do the, you know, education wise, they don’t want to go to school and, you know, … get their education.” This quote suggests there may be negative perceptions specific to Black men’s driving forces; these perceptions may not accurately reflect Black men’s lived experiences and have the potential to lead to further bias or stigma.
Healthcare Avoidance
‘Healthcare Avoidance’ depicts when an individual intentionally keeps away from medical care. This was a recognized action by both men and women within the focus group discussions. One participant noted, “As men, as a whole, we don’t like to go to the doctor, so therefore we ignore lots of things.” Another expressed, “I think there’s certain situations that most men will not… A lot of men don’t go to the doctor, and I think a lot of men need to have some therapy done.” Interestingly, this theme had a category emerge that was relatively prevalent as to why men avoid healthcare: ‘Emotionally-charged Avoidance.’ This category is defined as when an individual intentionally steers away from medical care due to feelings such as fear and denial of their health status. One participant stated, “I was thinking, because when you asked that question, I was thinking about my husband, and I think for him it’s denial.” Another participant shared that they thought men were scared of potential diagnoses, “And they’re scared. A lot of them are scared to go and find out what’s wrong with them because they might get a bad answer like a…well you got cancer, you got prostate cancer.”
Mental Health Concerns
‘Mental Health Concerns’ was identified as constructs that negatively affect an individual’s mental state and/or well-being. One participant summarized the overall potential impact of a culmination of negative influences, “How are you going to help somebody, you’re not even helping yourself, you know, speak some word that they might be able to hear to help them balance with their society. You understand?” Participants discussed stress and a lack of social support as they pertained to mental health. Specifically, participants expressed the need for relationships that offer tangible and emotional support. As described by one participant, “If you got a strong motivator, that motivator going to push you to do, you know what I’m saying, what you destined to do, you’re going to do it. You know what I’m saying?”
Systemic Bias, Racism, and Social Inequity
The final risk factor theme was ‘Systemic Bias, Racism, and Social Inequity,’ which contains several categories and subcategories. This theme represents the biases such as systemic racism, discrimination, and classism that impose barriers in attaining desired health. These barriers often manifest in terms of income, employment, and financial stability, as well as limited ability to engage in personal development due to one’s current social network and environment. These barriers disproportionately affect racial and ethnic communities. One participant stated, “So the hindrance is that we really don’t have anybody saying I’ll to take care of you, so we’re waiting for the system to do it…The system is not going to do it.” Two categories were further identified within this theme: ‘Economic Instability’ and ‘Education.” ‘Economic Instability’ represents the reciprocal of the identified protective factor theme of ‘Economic Stability.’ Specifically, it is the challenges to accessing financial resources, quality housing and food, and stable employment. A conversation among participants depicted this: “Because when a man is employed, he feels like he’s up there, you know, and that he can contribute to the family, community or whatever. But when he’s not employed, he doesn’t really contribute to anything. Then like she said, it’s a stressful thing on a man.” “And then if you, if you’re not employed, you ain’t even thinking about none of this stuff that’s wait, wait, way, way, you got to pay anything…You can't afford it.”
This category had an emergent subcategory of ‘Impact of Incarceration.’ This subcategory depicts the obstacles that accompany a record of imprisonment and/or legal charges in obtaining economic stability, often compounded by systemic racism and structural inequality. One participant stated, “Well, we got… Okay. A lot of our young men have felony records and things like that where a job is difficult to find” and another added, “They can’t get a job to feed the family because they’re locked in a bigger system now.”
The second category, ‘Education,’ is defined as challenges to achieving a desired level of formal education. One participant shared that they believe lack of education is a root cause of poor health, “But I think it was really because of lack of education and a fear and, of course, you know, all the other things that everybody else said, but just a lack of education, that’s all.” In addition, one participant expressed the delayed consequences of not acquiring formal education on one’s health, such as, “not being [having] good insurance or not having the jobs.” This category also had an emergent subcategory: ‘Systemic Bias in Education System.’ This subcategory illustrates institutional practices and/or norms that often hinder students of color compared to their White student counterparts. A community members stated, “When we used to get in a fight at the school, they’ll take us in the office, maybe give us 3-day suspension or something, but a kid fighting now, he got a battery charge and he’s going to a court, at seven and eight and nine-years-old he’s going to a court.”
Discussion
This research explored what adult community members, including men, perceive as risk and protective factors for the general health of men in their community by using a CBPR approach grounded by the life-course perspective. While prior maternal and child health research has largely focused on how men impact women’s and children’s health, 4 this research more broadly examined men’s health and included the perspectives of members of a low-income community of color. Through focus groups, we identified six themes for protective factors (healthy behaviors, economic stability, expected male responsibilities, healthcare engagement, social network, and faith, spirituality, and driving forces), and six themes for risk factors (health behaviors, impact of mentorship, experience of driving forces, healthcare avoidance, mental health concerns, and systemic bias, racism, and social inequity). Ultimately, this research illuminated the barriers that men and Black men face in particular in achieving protective factors which make it difficult to avoid risk factors for their health and well-being.
Community members emphasized the importance of men engaging in a variety of healthy behaviors (e.g., diet, exercise, smoking cessation) and avoiding parallel behaviors that could negatively impact their health (e.g., poor nutrition, limited physical activity, and smoking). However, this requires creating the conditions for men to be able to partake in healthy behaviors by addressing systemic barriers, such as fear of police brutality, which may prevent Black men from accessing leisure spaces for physical activity, 33 neighborhood poverty and racial residential segregation, which can lead to unequal access to healthy food options, 34 high rates of incarceration which preclude Black men from living full, healthy lives both during and after incarceration, 35 and healthcare access disparities, as Black men are less likely to have health insurance and report discrimination by healthcare providers.36,37 Investing in communities and addressing these political determinants of health 38 is a vital first step in breaking down structural barriers for men to participate in healthy behaviors. Instead of solely focusing on efforts to promote individual behavior change, upstream solutions can lead to more sustainable outcomes (ODPHP, n. d.). 39 Indeed, while participants brought attention to the less healthy behaviors of men in their community, public health professionals and programs should seek to highlight and combat the root causes of these behaviors to avoid victim-blaming. Further, addressing these larger structural issues is important to maternal and child health, as it leads to improved opportunities for not only men but families and the community. 40
A key component of confronting structural barriers that prevent men from engaging in protective health behaviors is addressing economic stability. For example, community members stressed the value of employment on men’s health while also shedding light on the ways in which systemic racism hinders men from accessing financial resources, housing, food security, and options for work. The value placed on economic stability for men intersects with the gendered protective factor of expected male responsibilities discussed by community members. Interestingly, while community members discussed expected male responsibilities as a protective factor, research shows that strict norms of masculinity can worsen men’s health.15,41,42 Men living in low-income communities may find it challenging to meet this expectation of providing for their households while simultaneously navigating systemic poverty and the ongoing impacts of racism on their economic stability. Indeed, while community members identified the experience of driving forces as a potential risk factor for men’s health, it may be more likely that men are facing chronic stress from racism and its associated poor mental health outcomes, which can diminish their willingness and motivation to operate within a biased system. This coupled with the expectation to meet gendered roles related to employment despite unequal opportunities43–46 may collectively perpetuate the current status of negative health outcomes among this population. To increase possibilities for economic stability, public health and maternal and child health professionals should work toward both improving educational and employment prospects for men with marginalized identities, including combating employment discrimination and addressing poor mental health that can result from ongoing oppression.
Healthcare engagement also emerged as a protective factor for the health of men. Men’s low rates of health-seeking behaviors have been well-documented and can be attributed to factors such as embarrassment, anxiety, and distress, endorsement of traditional masculinity norms, regarding symptoms as minor or insignificant, and weak communication with healthcare providers. 47 Many participants discussed that men in their community do seek out healthcare, including within community resources that may offer free or low-cost care; however, others commented on men’s reluctance to see doctors due to factors such as fear of potential diagnoses. Black men face additional unique obstacles to healthcare and health-seeking behaviors, such as socioeconomic status, racism and distrust of the medical system, having a criminal record, and certain social networks or religious and spiritual beliefs. 48 Community organizations, public health departments, and policymakers can promote healthcare engagement among men and Black men in particular, through strategies such as raising awareness of health disparities men face, holding health fairs within disadvantaged communities, and advocating for increased healthcare coverage for marginalized populations. 48 Bolstering men’s healthcare engagement can also lead to healthier families and communities, as men with improved physical and mental health may have increased capacity as parents and partners,3,4,7 and men’s health is correlated with the health of their children. 6
Working toward improved healthcare engagement must also include mental health services, as community members identified mental health concerns as a risk factor for men resulting from stress and a lack of social support. Black men face several health disparities related to mental health, including discrimination and racism leading to poor mental health,49,50 personal and structural obstacles to seeking out mental health care,51,52 and stigma surrounding seeking mental health services. 53 In addition, research has shown that compared to women, Black men are less open to seeking professional help, 53 and that men hold more negative attitudes toward mental health services than women. 47 Thus, future efforts to improve the mental health of men should include interventions across the social-ecological model that aim to break down individual, interpersonal, community, and structural barriers to mental health care utilization. To increase potential for success, these interventions must consider the role of racism and minority stress on Black men’s mental health. These interventions can also be beneficial by improving opportunities for culturally competent individual and family counseling within communities.
Social networks also offer a potential pathway to increase opportunities for men to engage in healthy behaviors and avoid risk factors for their health. Community members highlighted the importance of positive relationships for men, whether from family, friends, or partners. They also pointed to the benefits of intergenerational relationships, in which men can demonstrate healthy behaviors within their families and communities. However, the impact of mentorship also emerged as a potential risk factor, suggesting the need for improved opportunities for positive social relationships. Seeking out varied types of relationships may be especially important for men, who report benefiting from relationships with women that provide emotional support and relationships with other men, who provide instrumental support. 54 On the other hand, it is also important to address men’s potential barriers to accepting and providing emotional support from and for other men to increase opportunities for close and supportive relationships, as well as to remove the burden on women as sole providers of emotional care. For individuals with marginalized identities, increased levels of social support may also aid in combating the adverse effects of discrimination.46,55 One potential mechanism for social support, and another protective factor identified by community members, is religious involvement. Indeed, some research has shown that religious involvement can reduce the impacts of discrimination.56,57
Limitations
While this research addressed an important gap about community members’ perspectives on men’s health in the context of maternal and child health and for the sake of men’s own health and well-being, it is not without limitations. Due to the nature of qualitative research, the findings are not intended to be generalizable to other populations. However, we aimed for transferability within our work by providing a clear description of the study and how it is situated within the current body of literature, highlighting rich quotes to support our findings, and making connections between our findings and broader health disparities and systemic inequities. In this project, which is a sub-analysis of a larger data set, we cannot ensure theoretical saturation. We recommend that future researchers expand our findings by assessing the community perspective with more qualitative research to ensure that saturation is reached. There is also the potential for self-selection bias. Community members within the larger project with increased interest or investment in the research topic or within their community may have been more likely to participate. Furthermore, including all members of the community, rather than only men, may be considered a limitation of this study. Having the perspectives of all male groups could have revealed additional insights about risk and protective factors. For instance, some men could have been hesitant to share certain thoughts or experiences with women present. Additional research that focuses specifically on men’s perceptions of risk and protective factors for health may yield additional unique findings.
Although we conducted focus groups in Spanish as part of the larger study, we did not include the results of those focus groups in this paper, which is a limitation of this study. Further, while we monitored participants’ sociodemographic information to minimize overrepresentation from any particular group, it is possible that cultural or linguistic barriers could have influenced participation or responses. Since focus groups come with unique challenges such as groupthink, and social desirability bias, it is possible that participants expressed opinions they perceived as socially acceptable or withheld views they felt were socially unacceptable. Individual interviews on this topic would be helpful in the future to avoid these focus group challenges. As this research was part of a larger study, there were only two focus group questions related to men’s health included within this sub-analysis. A more comprehensive set of focus group questions could reveal other risk and protective factors for men’s health or add additional context to community members’ responses. The original project collected sociodemographic data across the 10 original focus groups, with a total of 78 community members participating across the 10 groups. Since this is a sub-analysis, we were not able to collect demographics for these four focus groups. Lastly, for this study, the data were analyzed by two primary coders who were not involved in the original project. However, as mentioned, we presented the initial themes and preliminary results to several members of the CAB for member check validation, and several rounds of refinement by those CAB members were made for this study. We also shared the draft of this manuscript with the entire CAB for input.
Conclusion
This research has important implications for promoting men’s health across the life-course, including facilitating men’s ability to practice health behaviors, improving their economic stability, enhancing opportunities for social and spiritual engagement, and increasing physical and mental healthcare access. As attention to the importance of including men within maternal and child health efforts continues to grow, listening to the voices of community members and men specifically offers valuable insight into what men need to improve their health and well-being. This is of particular importance in low-income marginalized communities that face disparities in maternal and child health outcomes and the impacts of structural oppression. Concentrating on understanding men’s risk and protective factors for health addresses a current gap in the maternal and child health literature on prioritizing nurturing men’s own health while adding to the research base on how their well-being can impact the health of mothers, infants, children, and communities. By seeking out upstream solutions to increase opportunities for men to practice behaviors that lead to improved health and reducing risk factors that prevent them from doing so, there is potential to both improve their health across the life-course and further their roles as key stakeholders in maternal and child health.
Footnotes
Acknowledgements
We thank the community, especially the Community Advisory Board members, and the staff from REACHUP Incorporated.
Author Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Lindsey M. King, Abraham A. Salinas-Miranda, and Hamisu M. Salihu, Roneé E. Wilson, Kenneth Scarborough, Estrellita “Lo” Berry, Deborah Austin, Richard Briscoe, Georgette King, Lillian Cox, Carrie Y. Hepburn, Evangeline Best, Conchita Burpee. Data analysis was performed by Sarah L. Collins and Gaia Zori. The first draft of the manuscript was written by Cary Carr, Lindsey M. King, Sarah L. Collins, and Gaia Zori and all authors reviewed and commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the National Institute on Minority Health and Health Disparities through an R24 grant on ‘‘Community-Based Participatory Research” (Award#: 5R24MD8056-02).
Ethical Consideration
This study was reviewed and approved by the University of South Florida IRB (IRB#: Pro 00010288) and then later approved by the University of Florida IRB (#IRB 202000540).
Consent to Participate
Informed consent was obtained from participants.
Consent for Publication
Participants signed informed consent regarding publishing their data.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.