
Abstract
Black and Latina cisgender and transgender women who use substances face adverse sexual and reproductive health (SRH) outcomes due to intersecting forms of discrimination and limited access to high-quality SRH services. Insufficient research has explored healthcare providers’ views and experiences related to delivering SRH care to multiply marginalized women, especially the role of training in shaping their attitudes and practices. Using purposive sampling, we conducted online, in-depth interviews with 20 SRH care providers in Massachusetts and Rhode Island in August-November 2023 to elucidate how their training influenced their provision of SRH care to Black and Latina cisgender and transgender women who use drugs and identify the strategies they used to address the limitations of their formal training. Using intersectionality-informed thematic analysis, we found that most providers expressed dissatisfaction with their clinical education, which failed to address how racism, transphobia, and substance use stigma simultaneously influenced SRH outcomes and care. Further, many reported that the training needed to provide high-quality SRH care to Black and Latina cisgender and transgender women who use drugs largely occurred outside of their formal education, but that burnout, time constraints, and lack of reimbursement undermined their ability to obtain additional training and deliver tailored care. Providers also described how their professional and personal backgrounds influenced their practices and noted that specialized SRH education, working in person-centered care settings, and sharing social identities with patients facilitated their provision of high-quality SRH care to Back and Latina women who use drugs. Medical and nursing programs should incorporate training on intersectional discrimination and facilitate the enrollment of students with multiple minoritized social identities to advance SRH equity and justice.
Keywords
Introduction
Sexual and reproductive health (SRH) services, including the delivery of SRH information and the provision of sexually transmitted infection (STI), HIV prevention, gynecological cancer screening, and pregnancy-related care, are vital to the physical and mental health of all women in the United States (U.S.).1–5 However, negative experiences with SRH care providers can limit access to needed SRH information and care among socially and economically marginalized groups of women.4,6 In particular, Black, Latina, and other women of color face notable barriers to accessing high-quality SRH services as a result of interpersonal and institutional racism and xenophobia in healthcare settings, which in turn decreases their likelihood of engaging in regular SRH care and increases their risk of experiencing poor SRH outcomes.7,8
Moreover, transgender women, especially those from racialized backgrounds, experience elevated levels of transphobia during SRH care encounters, which in turn undermines the quality of the care they receive.9–11 Additionally, cisgender and transgender women who use substances also face substance use stigma from SHR care providers, which can result in high rates of unwanted pregnancies, abnormal Pap tests, HIV, and hepatitis C in these populations.9,12–17 Of note, women who experience multiple forms of discrimination and stigma, including racism, xenophobia, transphobia, and substance use stigma, may face particularly pronounced barriers to receiving high-quality SRH information and services from providers, which may result in especially elevated rates of adverse SRH outcomes, such as STIs and maternal mortality, in these multiply marginalized populations.6,7,18–23
Adequate education and training on the unique social experiences and health needs of marginalized groups of women, including women of color, transgender women, and women who use drugs, can better prepare SRH care providers to provide high-quality services to multiply marginalized patients, such as Black and Latina cisgender and transgender women who use drugs.21,24–26 However, physicians and nurses receive little formal education or training to prepare them to understand or meet the SRH care needs of these multiply marginalized populations.18,26,27 Indeed, medical and nursing education devote limited curricular time to learning about substance use disorders and harm reduction strategies.18,28–30 For example, the average medical school devotes 12 hours of curricular time to substance use disorder prevention and treatment, and most nursing programs do not include any curricular time on these topics.18,29,31 For some medical students and residents who lack clinical exposure to patients who use substances, their perceived preparedness and willingness to treat substance use disorders decrease as they advance beyond their formal medical education.18,28,30
Transgender women who use substances have healthcare needs that differ from those of cisgender women, such as gender-affirming care; yet, formal healthcare training often does not adequately prepare medical professionals to care for this population.26,32 Knowledge about the provision of healthcare to transgender and gender-diverse people varies widely due to the lack of a standardized health curriculum on transgender and gender-diverse health needs across medical education programs. 33 For example, in a nationally representative survey of residency programs in the United States (n = 61), only 51% of programs offered education on transgender health. 34 Moreover, gaps in transgender healthcare training are particularly evident in nursing education. As Yu et al. emphasized in their systematic review, nursing curricula have historically lacked structured content on health of lesbian, gay, bisexual, transgender, queer, intersex, asexual, and other sexual and gender minoritized (LGBTQIA+) populations, including the unique SRH needs of transgender individuals. 35
Indeed, despite expressing a strong desire for inclusive training, the vast majority of U.S. nursing students reported not receiving formal education on sexual orientation, gender identity, and health during their training, which in turn rendered them unprepared to adequately care for LGBTQIA+ patients. 36 The lack of culturally competent nursing education perpetuates medical distrust among transgender patients, nearly one-quarter of whom reported in the 2015 U.S. Transgender Survey that they had to teach their providers about their health needs. 9 Limited medical and nursing education training on the healthcare needs of transgender and gender-diverse people results in knowledge gaps among healthcare providers in relation to the provision of high-quality, respectful, and non-stigmatizing care—including SRH services such as HIV prevention, STI treatment, and anal cancer screening.10,11,26,35
The SRH needs of Black and Latina women who use substances are unique and differ from those of White women as a result of gendered racism in the healthcare system in particular and society in general. 7 However, medical schools have often failed to incorporate lessons on anti-racist communication, explicit and implicit racial bias, and the effects of interpersonal, institutional, and structural racism on healthcare and health outcomes within the training of healthcare providers, resulting in the medical mistrust among Black, Latine, and other communities of color.21,27,37
Additionally, race is still erroneously conceptualized as a biological risk factor for diseases rather than a social or political construct in medical education, which furthers the pathologization of communities of color.38–40 Of note, one study hypothesized that the pathologization of race as a risk factor has contributed to racial biases among medical professionals. 40 Other studies have also shown that, in nursing and medical education, there are few opportunities to discuss institutional racism and racialized health disparities.38,41 For example, more than half of family medicine residency programs in the U.S. do not offer a formal curriculum on racial justice in relation to health and healthcare, which in turn undermines healthcare providers’ ability to deliver high-quality, culturally relevant care, including SRH care, to Black and Latina women.27,40
While prior studies have identified gaps in formal provider education related to the health needs of distinct marginalized groups, current literature does not address how this education prepares healthcare providers to treat patients who hold multiple marginalized identities. Of note, few studies have examined how SRH care providers deliver SRH information and services to Black and Latina cisgender and transgender women who use drugs in particular. Moreover, research ascertaining healthcare providers’ training, or lack thereof, in providing SRH care to patients who experience racism, sexism, cisgenderism, and substance use stigma is scant. Thus, in order to address these gaps in the scientific literature, we conducted a qualitative research study to understand SRH care providers’ views on, approaches to, and experiences with delivering SRH care to Black and Latina cisgender and transgender women who use substances, with particular attention to the role of their clinical training. Additionally, we sought to identify the strategies providers used to supplement their formal training to better meet the SRH care needs of Black and Latina cisgender and transgender women who use drugs.
Materials and Methods
Sampling and Recruitment
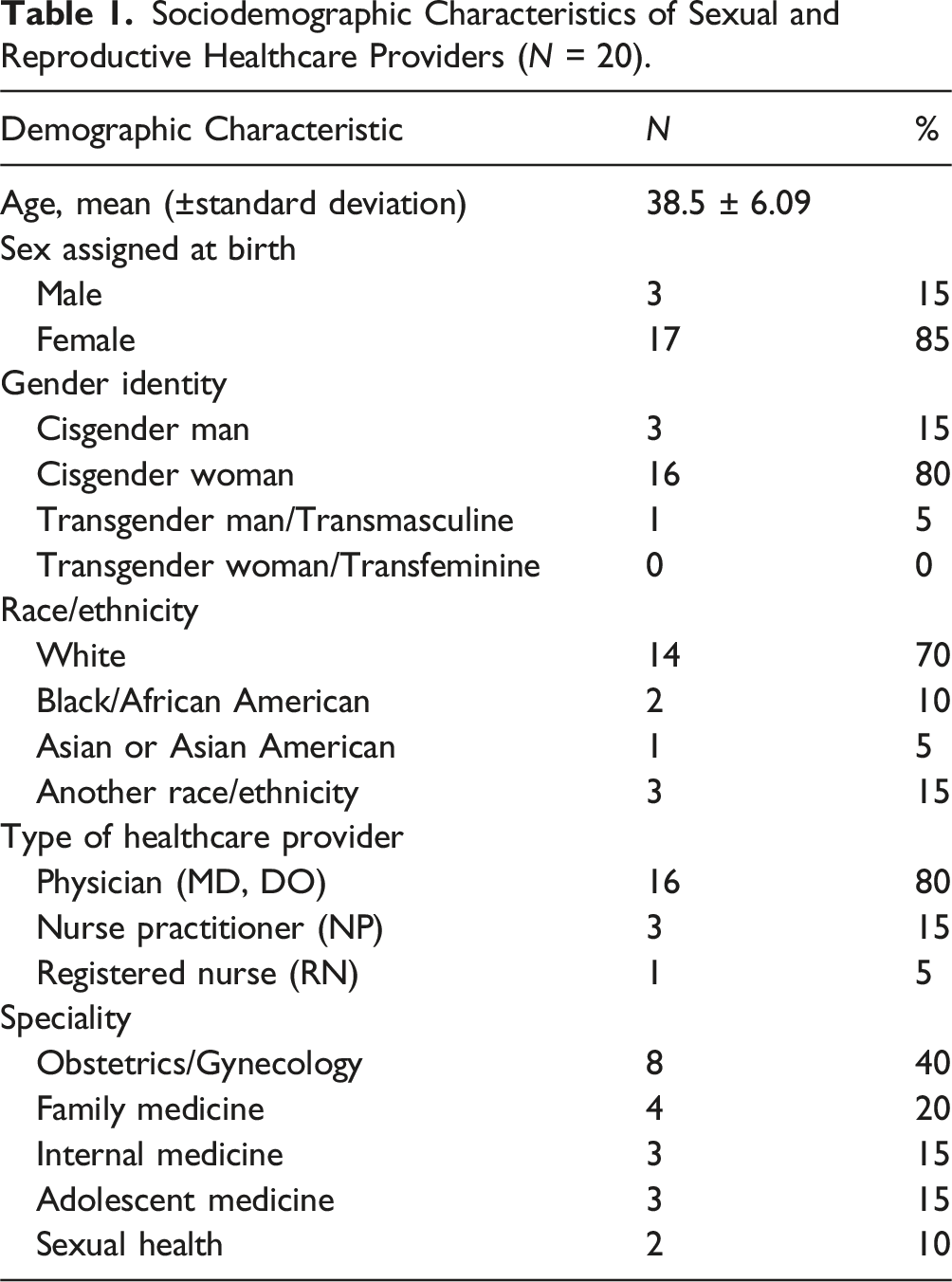
The research team employed purposive and snowball sampling to select 20 healthcare providers delivering SRH care in Massachusetts or Rhode Island.42,43 We identified potential participants, along with their contact information, through our professional networks and by accessing the publicly available websites of clinics, community health centers, hospitals, and academic medical institutions. Eligibility criteria for participation were: being a practicing healthcare provider, including a physician, nurse practitioner, or physician assistant; working in either Massachusetts or Rhode Island; having provided SRH care, including but not limited to cervical cancer screening, contraceptive care, and HIV/STI testing and prevention, to patients within the last year; and speaking English.42,43 Providers did not need to have any particular professional specialty or have prior experience treating people with substance use disorders to be eligible for our study. We used maximum variation sampling to intentionally select providers from a range of specialties, including but not limited to obstetrics and gynecology, internal medicine, adolescent medicine, and family medicine, to capture a diverse range of training experiences relevant to SRH care. 42 To increase the breadth of perspectives, we also sought diversity in providers’ professional roles, years of clinical experience, race/ethnicity, and gender identity. Finally, we used quota sampling to ensure the inclusion of physicians (i.e., MD, DO), nurse practitioners (NPs), and registered nurses (RNs) in our sample in order to explore similarities and differences in views, experiences, and training among these different provider types. 44 Of note, given the range of training and practice experiences that physicians have in SRH care, we intentionally oversampled this provider type so as to capture a broad range of physicians’ professional experiences. Specifically, we sought to generate a sample comprising 75% (n = 15) physicians and 25% (n = 5) NPs and RNs, which our existing sample approximates with 16 physicians, three NPs, and one RN.
Data Collection
We conducted semi-structured interviews (N = 20) with eligible participants to learn more about their views, experiences, and training in providing SRH care to Black and Latina cisgender and transgender women who use substances. Interviews were conducted between August and November 2023 via Zoom by two interviewers with training in public health and qualitative research methods using a semi-structured interview guide. The interview guide addressed a range of topics, including healthcare providers’ views, experiences, and training related to delivering SRH care to Black and Latina cisgender and transgender U.S. women who use drugs. Prior to their interview, each participant completed a brief demographic questionnaire. Interviews were conducted in English, lasted, on average, 56 minutes, and were recorded via Zoom for transcription and data analysis. Audio recordings were then transcribed using the NVivo transcription service. 45 All Zoom recordings were securely stored, and transcripts were reviewed against recordings for accuracy. Participants received a $100 Amazon gift card for their participation. All research activities were approved by the Human Research Protection Program (HRPP) at Brown University. All participants provided verbal consent at the start of their interview after a comprehensive discussion of the informed consent form.
Data Analysis
All interview transcripts were uploaded to Dedoose for team-based coding and analysis. 46 We used an intersectionality-informed, template-style thematic analysis approach to develop a hierarchical codebook that incorporated both inductive and deductive codes.47–49 Deductive codes were informed by the research literature on SRH care among Black and Latina women who use substances as well as by intersectionality, an analytical framework that postulates that the lived experiences of Black women and other multiply marginalized populations are shaped by multiple forms of discrimination, including but not limited to racism, sexism, and classism. 50
Two independent coders (who also served as the study’s interviewers), a White cisgender man and a White cisgender woman with backgrounds in SRH, harm reduction, sexual and gender minority health, and health equity and training in qualitative public health research, collaboratively developed an initial codebook based on four transcripts. They then independently coded the remaining transcripts, with 20% (n = 5) coded by both analysts to ensure coding consistency.47–49 Throughout the coding process, the coders iteratively refined the codebook to more effectively reflect the data in the interviews.48,49 Additionally, the coders compared their double-coded transcripts and resolved coding discrepancies through discussion and consensus.48,49
Guided by intersectionality, the coders created an analytic matrix of key coded excerpts from the transcripts organized by code and provider type (i.e., MD/DO, NP, or RN), specialty, race/ethnicity, and gender identity to facilitate subgroup comparisons of participants’ views, experiences, and training based on these social identities and professional roles.50,51 We used the matrix to develop robust themes and sub-themes by clustering codes, making comparisons across participants, and engaging in team-based discussions to further refine themes and sub-themes.47–49 Coders utilized memo writing throughout the coding and theme development process to keep track of emerging themes and iteratively develop robust themes and sub-themes that captured all of our data.47–49
Reflexivity Statement
As researchers, we acknowledge that our social identities, professional backgrounds, and personal values and experiences affect the research process, including data collection, analysis, and theme formulation. Thus, we acknowledge that both interviewers’/coders’ positionalities as White, cisgender public health researchers who do not provide SRH care to Black and Latina cisgender and transgender women who use substances influenced our findings. To elucidate how their positionality shaped the data collection and analysis process, the interviewers/coders engaged in regular memo writing and ongoing conversations with other members of the study team, who held strong commitments to racial, gender, social, and health justice and included individuals with minoritized sexual orientation, gender, and racial/ethnic identities. Regularly engaging in these reflexive practices facilitated the elucidation of beliefs, perceptions, and assumptions that could influence the collection and interpretation of data and theme development among the interviewers/coders, who kept their assumptions in mind throughout the research process.
Results
Participant Characteristics
Sociodemographic Characteristics of Sexual and Reproductive Healthcare Providers (N = 20).
Themes and Sub-themes
Theme 1: Formal healthcare provider education in sexual and reproductive health and harm reduction fails to adequately address multiple forms of discrimination and stigma and their intersections
Overall, SRH providers reported deficient experiences regarding their healthcare training on intersectional approaches to stigma and discrimination. Participants consistently noted that their formal education tended to address discrimination and substance use stigma inconsistently and rarely considered how multiple forms of discrimination intersected in the context of healthcare. These gaps left many providers feeling unprepared to recognize or respond to the specific SRH experiences and care needs of patients who face multiple forms of stigma and discrimination related to race/ethnicity, gender identity, and substance use (Figure 1). Thematic map of providers’ views, experiences, and training related to the provision of sexual and reproductive healthcare to Black and Latina cisgender and transgender women who use substances.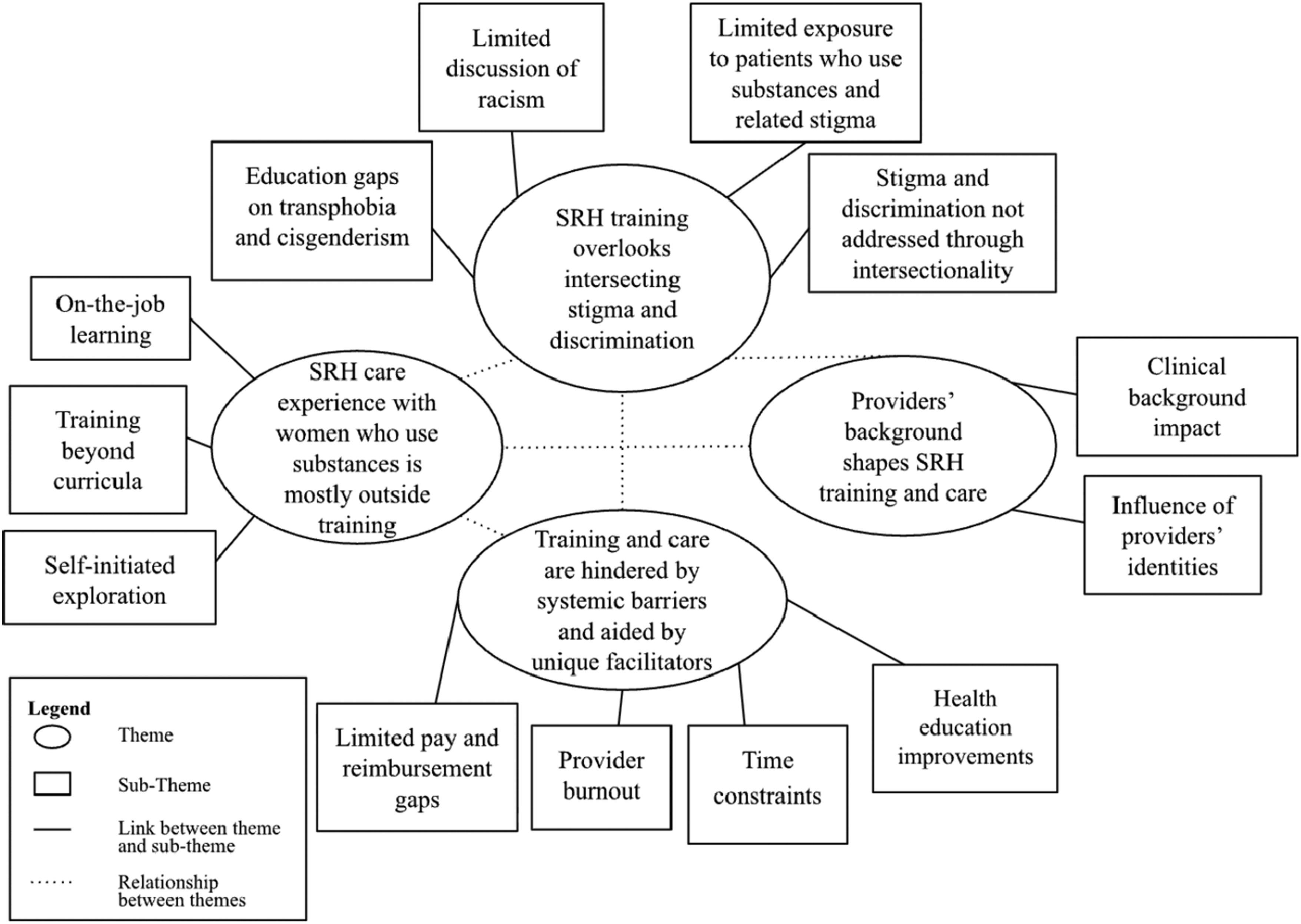
Inadequate discussion of racism in formal healthcare provider education
Many SRH care providers indicated that while race was mentioned throughout their formal education, it was framed as a biological difference rather than as a social or political construct. For example, in referring to training on race in formal medical education, an internal medicine physician, a White woman, said: “Race was not discussed as a risk factor or there was no formal education on that. In fact, race was probably taught… as a biological difference between people” (Participant ID 007). Another provider, an adolescent medicine physician, a White man, also explained: “I don’t think it was super explicitly talked about” (Participant ID 001). Various providers described how, while racialized health disparities were mentioned in their formal education, racism, the root cause of those health disparities, was ignored. For instance, a sexual health nurse, a White man, discussed: “It was very just factual… not really like diving into the why of these disparities, but more just like there’s disparities here” (Participant ID 003). Some providers also expressed frustration when racism was not named as a reason for racialized health disparities. One obstetrics and gynecology (OB/GYN) physician, a Black woman, said: “So I think back when I was in medical school, we were still teaching things like race as a risk factor… but now we don’t teach that because it’s not true, right? It’s not race, it’s racism” (Participant ID 014).
Lack of provider healthcare education on gender identity and transphobia
With regard to transphobia, participants noted that there was a distinct lack of education on the unique health needs of transgender individuals. For example, a family medicine nurse practitioner, a White woman, communicated: “The only thing we learned about was post-exposure prophylaxis… and there wasn’t the emphasis on… gender identity. None of that stuff really played a role in my education” (Participant ID 010). Most participants recalled how there was a failure to address transgender health at all. For instance, an OB/GYN physician, a White woman, explained: “Definitely—I never felt like we talked about transgender health at all” (Participant ID 018). Similarly, an internal medicine physician, a White woman, said: “I don’t think gender identities were at all addressed in that realm” (Participant ID 007). Due to the lack of LGBTQIA+ health education as a whole, lessons on transphobia rarely came up in providers’ descriptions of their healthcare education.
Limited training on substance use treatment, prevention, and stigma
Our data also revealed a gap in how substance use treatment, prevention, and stigma were addressed in SRH providers’ training. Referring to how substance these issues were rarely covered in formal provider training, a sexual health registered nurse, a White man, recalled: “I don’t think at any point in my nursing program, harm reduction was even mentioned” (Participant ID 003). Another participant, an OB/GYN physician, a White woman, expressed similar sentiments about her residency training on substance use treatment and prevention: “Sadly zero [training opportunities], which is something I’m really working on. Very, very minimal. It’s not a part of the standard design of residency training, substance use” (Participant ID 006). Moreover, an OB/GYN resident, an Asian/Asian-American woman, discussed how this lack of exposure to substance use treatment and prevention education has generated bias among providers: “I’m thinking about… the lack of familiarity. I think that you can have providers who… make judgments about patients, but even like providers who are open and willing to talk to patients, I think it can still be very challenging” (Participant ID 012). Another provider, an internal medicine physician, an Asian-American man, reiterated this concern, expressing discomfort in providing medication-assisted treatment due to gaps in his own medical education: “Specifically, medication for opioid use disorder and things like that… I never got any formal training. I don’t feel comfortable doing it” (Participant ID 004).
Failure to address multiple forms of discrimination and stigma using an intersectional lens
Providers reflected on how the intersection of racism, transphobia, and substance use stigma was rarely addressed in the context of their healthcare training. For example, a family medicine nurse practitioner, a White woman, reported that her program “never” addressed intersectionality (Participant ID 010). Similarly, a family medicine physician, a White woman, noted that lessons incorporating intersectionality were “somewhat minimal” in her medical education (Participant ID 020). Similarly, an OB/GYN physician, a White woman, reiterated that “even the concept of intersectionality, I don’t think it really had come up until after I was out of residency” (Participant ID 018). In particular, providers explained that when their training covered issues of race, gender identity, and substance use, they did so in siloed ways that failed to make connections among these social determinants of health. Indeed only a few providers reported receiving training that discussed how racism, cisgenderism, and substance use stigma simultaneously undermined SRH outcomes and care among Black and Latina cisgender and transgender women who use drugs in unique and compounding ways. As a result, providers often had to rely on their own initiative or practical, on-the-job experience to address the SRH care needs of these and other multiply marginalized patients in ways that attended to the multiple forms of discrimination and stigma they faced in society in general and the healthcare system in particular.
Theme 2: Providers primarily acquired knowledge and experience delivering sexual and reproductive health care to Black and Latina women who use drugs outside of formal education
Participants reported that they acquired knowledge on and experience with providing SRH care to Black and Latina cisgender and transgender women who use substances outside of their formal healthcare education, including through “on-the-job” learning and by seeking additional training on their own time (Figure 1).
Professional “on-the-job” interactions with Black and Latina women who use substances helps fill gaps in formal training
When asked about providing SRH care to Black and Latina cisgender and transgender women who use substances, most participants emphasized that “on-the-job” clinical interactions was essential for developing knowledge and skills not addressed in formal curricula. For example, when discussing prenatal care, contraception counseling, or management of STI risk among patients with substance use histories, one family medicine physician, a White woman, explained: “So much of the learning is done in… a clinical setting. So I guess… most of the training was in the hospital, in the clinic, you know, based on the patient that you’re seeing” (Participant ID 020). Similarly, a primary care and sexual health nurse, a White woman, said: “In general, most of my knowledge came outside of my actual NP program” (Participant ID 002). Moreover, a family medicine nurse practitioner, a White woman, explained how her professional experiences helped increase her comfort level treating patients who use substances: It was like… baptism by fire. Right? Because you’re having all these patients who, you know, are either in acute withdrawal or I mean, yeah… [working in] addiction… it made the whole thing more approachable, less scary. And just a normal part… of my line of questioning and my treatment for these patients (Participant ID 010).
In the context of SRH care for Black and Latina women who use substances, providers also highlighted the value of consulting colleagues, including with regard to strategies for integrating substance use considerations into contraception management, STI screening, and prenatal care for patients with a history of substance use. For instance, an OB/GYN physician, a White woman, discussed: “I learned a lot from my addiction medicine colleagues that I’ve been able to bring to our department” (Participant ID 006). Similalry, an OB/GYN physician, a White man, mentioned: “We have meetings where these issues are discussed every single month. What can we do better? What’s not working? And every month we find, you know, deficiencies. That’s how we get better” (Participant ID 005). Further an OB/GYN physician, a White woman, said: “We have different spaces created to talk about challenging cases. I think it is challenging emotionally or just logistically, and that is helpful” (Participant ID 019).
Providers seek additional training on approaches to sexual and reproductive health care for Black and Latina women who use drugs outside of their formal training
Outside of their formal education, providers reported furthering their knowledge of providing SRH care to Black and Latina cisgender and transgender women who use substances by attending supplemental lectures, workshops, and medical specialty conferences. For example, a family medicine physician, a White woman, discussed how “[the] annual conference, [for the] American Academy of Family Physicians (AAFP), [where] there are talks on substance use and treatment” and going to “talks post-residency on PrEP actually given by our community health center” helped her improve her delivery of SRH services to diverse groups of people who use substances (Participant ID 008). Similalry, referring to how she learns new knowledge and skills pertaining to the provision of SRH care to Black and Latina women who use drugs, an adolescent medicine physician, a Black woman, said: I go to the Centers for Disease Control (CDC) STI conference… the National Association of Pediatric Gynecology… and then we have an adolescent medicine national conference called the Society for Adolescent Health and Medicine (SAHM), and they do a lot of workshops and training (Participant ID 013).
Moreover, in discussing the provision of high-quality SRH care to people of color and transgender and gender diverse patients, a family medicine physician trained in obstetrics, a White woman, said: I’ve learned a lot in my own training in trans healthcare. And so that, you know, I’ve been to workshops… and training about taking care specifically to be thoughtful about how we’re taking care of patients who are people of color, trans, gender diverse, all those different pieces. And I would say that’s much more of an emphasis on that (Participant ID 017).
Another provider, a family medicine nurse practitioner, a White woman, described gaining specific skills in providing comprehensive SRH care, including to marginalized women who use drugs, through ongoing training in contraceptive methods, noting that: “I’ve done continuing education in order to provide, you know, like long term reversible contraception and you know, a lot of continuing education in that area just because it’s an interest I have” (Participant ID 010).
Providers addressed gaps in their formal sexual and reproductive health care training through self-initiated learning
While formal healthcare education provided a foundation, participants emphasized that their ability to provide high-quality SRH care to Black and Latina women who use substances relied heavily on not only experiential learning and continuing education but also self-directed research. In particular, several participants described engaging in self-initiated learning that included reviewing literature on the structural barriers to SRH care among marginalized populations and learning about culturally-appropriate approaches to SRH care among Black and Latina women who use substances. For example, an internal medicine physician, an Asian-American man, said: It’s been reviewing data, in my role in public health, and really looking at trends and advocating, first off, just to capture the data so that we can even look at trends. And it’s been by choice, by seeking out educational training sessions, by asking community members for feedback and for insights and thoughts, approaches (Participant ID 004).
Moreover, a sexual health registered nurse, a White man, explained: “Frankly, I’ve just learned a lot on my own just through researching and reading online about like what other cities might do or what other organizations might do with regard to harm reduction” (Participant ID 003).
Theme 3: The provision of high-quality sexual and reproductive healthcare to Black and Latina women who use drugs is undermined by systemic barriers and enhanced by intersectional, person-centered, and strcturally-competent care approaches
In addition to the lack of formal training they received regarding the provision of SRH care to Black and Latina cisgender and transgender women who use substances, which undermined their personal ability to effectively do so, SRH care providers faced systemic barriers that inhibited their pursuit of additional, informal training opportunities and undermined their capacity to provide high-quality SRH care to these multiply marginalized populations. In contrast, participants reported that using intersectional, person-centered, and structurally-competent approaches helped improve their delivery of SRH sertices to Black and Latina women who use drugs (Figure 1).
Healthcare provider burnout
Many providers mentioned burnout as a barrier to pursuing additional training and deliving high-quality SRH care to Black and Latina cisgender and transgender women who use drugs. When discussing some of the challenges providers he faces in adequately caring for these multiply marginalized patients, an adolescent medicine physician, a White man, said: “Burnout is huge, let’s put it that way” (Participant ID 001). Importantly, several participants noted that caring for Black and Latina women who use substances can intensify feelings of burnout, as providers must balance complex medical needs, overlapping SRH concerns, and the multiple stigmas these patients experience. Culturally-appropriate care often requires more time and labor, which providers described as being more taxing than serving non-marginalized patients. An OB/GYN resident, an Asian/Asian-American woman, expressed this sentiment: “Providers are burnt out, they’re seeing four patients every hour and it’s hard to remember to do all that stuff for every single patient” (Participant ID 012). One provider, a physician practicing as an OB/GYN, a Black woman, also expressed frustration with the sheer amount of patients she is expected to care for, underscoring that: “It burns the providers out. And then we feel awful because we have patients that we take care of for the whole pregnancy, and then they come in labor and we don’t have a bed” (Participant ID 014).
Lack of time to acquire additional knowledge and training
In addition to burnout, providers reported that they often lacked the time to obtain additional training on delivering high-quality SRH care to Black and Latina women who use drugs during work hours. For example, in expressing that she is so pushed for time that she has to finish her responsibilities outside of regular hours, an internal medicine physician, a White woman, expressed: “You spend a lot of time just seeing patients and finishing up your responsibilities with the phone calls and everything else after that. There’s always that time push” (Participant ID 007). A family medicine physician, a White woman, reiterated the struggle with time constraints during the work day, articulating that: “I think that would probably be something that at this point I would have to seek out on my own, like through medical conferences, online lectures, articles. I don’t have structured learning time in my daily work anymore” (Participant ID 016). Another provider, an OB/GYN resident, an Indigenous woman, said that even when there are educational resources readily available, there is still the barrier of time: “I think it’s hard. I think it’s great, like if we have a list of recommended readings. But I think the reality is that most people are so busy that unless it’s part of something they’re going to be asked to do at work, it’s not going to get done” (Participant ID 015). Moreover, several participants also mentioned that their high patient loads and short clinic visits also undermined their ability to provide multiply marginalized patients who use drugs with SRH care that attended to all of their social and medical needs.
Health insurance reimbursement barriers
Most participants discussed issues with healthcare financing that created barriers to providing high-quality SRH care to Black and Latina women who use substances. Providers noted that they faced notable difficulties in obtaining reimbursement for treatments that sought to address the complex needs of marginalized women who use substances because their appointments often involved multiple, overlapping health and social needs that do not neatly fit into standard billing models. For instance, one appointment might include prenatal care, substance use counseling, and social service referrals, each of which requires additional time that was not adequately compensated. For example, an OB/GYN physician, a White man, said: “Take a patient and see them as many times as possible. And that’s how you make your money… With this population, we have to address every issue… at one time. And it’s a whole shift in philosophy on how you take care of patients” (Participant ID 005). Another provider, an OB/GYN resident, an Asian/Asian-American woman, reflected on the lack of education on the financial hurdles of medicine for providers, mentioning that: You don’t necessarily know until you get more experience in the field, like what medication requires authorization from insurance, what steps an insurance company forces you to go through before landing on the appropriate management for the patient, and what the patient wants… I think that’s challenging (Participant ID 012).
Improvements to healthcare education in relation to the provision of care to Black and Latina women who use substances
Several SRH providers mentioned that, in recent years, medical education had been slowly improving with regard to meeting the SRH care needs of Black and Latina cisgender and transgender women who use substances. For example, when referring to overall changes in healthcare education throughout time, a primary care and sexual health nurse practitioner, a White woman, explained: “I think that only in the last couple of years… have I really seen a sort of a change in the way that we are talking about some of these topics. I think it’s the same with gender and identity and pronouns and race and ethnicity” (Participant ID 002). Similarly, an internal medicine physician, a White woman, reiterated positive changes in medical education over time, stating that: “Really over the past decade or so and really going back into academia has redefined race as a social construct and has informed my perspective on treating patients” (Participant ID 007).
A few providers also mentioned positive aspects of their recent formal training experiences. In discussing transgender healthcare, an adolescent medicine physician, a White woman, who went to medical school abroad, said that: “I had formal training in, like a gender inclusive clinic giving, like gender affirming hormones, there was like, both hands on teaching on that and formal education about that” (Participant ID 011). Another provider, an OB/GYN resident, an Indigenous woman, mentioned that: “We do have a lot of intersectionality as it pertains to caring for our patients, which is important” (Participant ID 015). Although some programs have evidently made efforts to improve their curricula, gaps clearly remain in many healthcare training programs across the U.S.
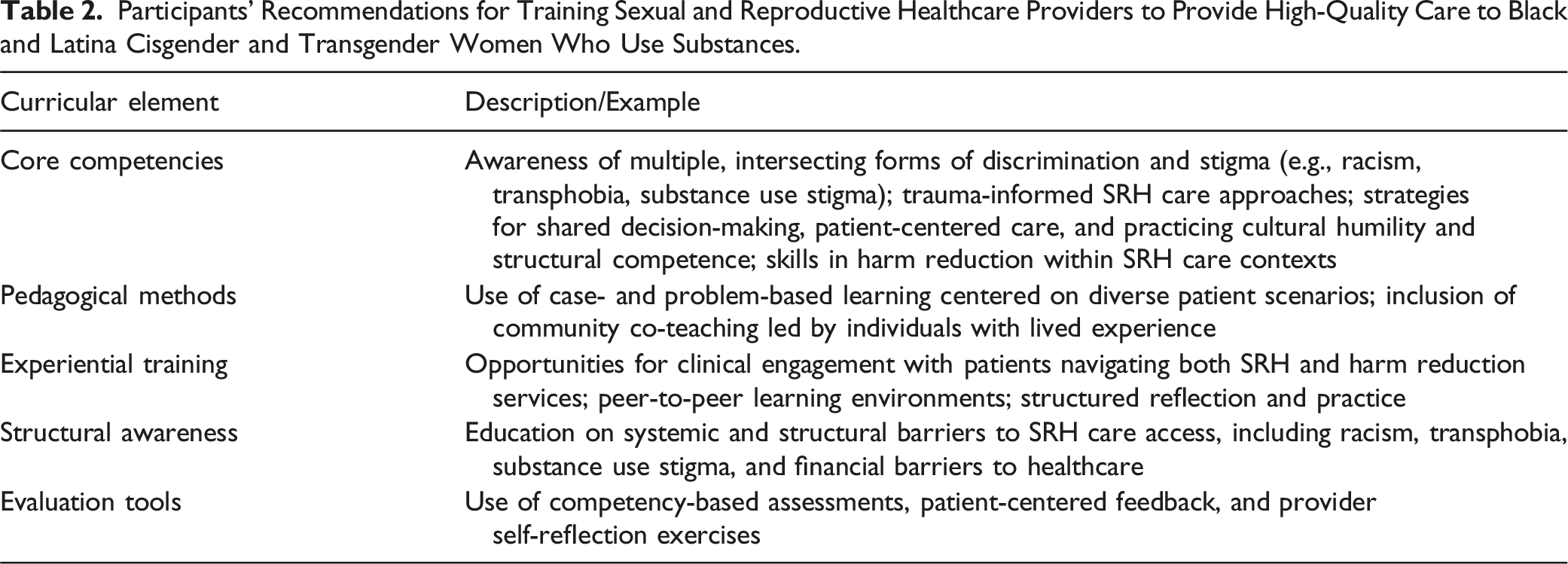
Participants’ Recommendations for Training Sexual and Reproductive Healthcare Providers to Provide High-Quality Care to Black and Latina Cisgender and Transgender Women Who Use Substances.
Theme 4: Providers’ professional and personal backgrounds and clinical context shape their training on and provision of sexual and reproductive healthcare to Black and Latina women who use drugs
Throughout the interviews, participants highlighted the unique aspects of their professional and personal background, as well as the clinical contexts in which they work, that influenced their approach to the provision of SRH to Black and Latina cisgender and transger women who use substances. In particular, we found that providers with OB/GYN or SRH professional backgrounds, who worked in clinical settings with large populations of patients who use drugs or that emphasized person-centered care, and providers with marginalized racial/ethnic and gender, identities reported feeling better prepared to provide high-quality SRH care to Black and Latina cisgender and transgender women who use drugs. Conversely, providers in clinical specialties or settings with limited SRH and harm-reduction training or working in environments where stigma toward substance use or HIV was prevalent described facing significant challenges in providing equitable care (Figure 1).
Impact of professional background and clinical context on the provision of sexual and reproductive healthcare to Black and Latina women who use substances
Subgroup analyses by healthcare provider type revealed differences in training experiences. Of note, physicians often reported greater exposure to formal SRH care education addressing substance use, whereas nurse practitioners emphasized experiential and self-directed learning. Similarly, providers in OB/GYN specialties were more likely to report training regarding providing SRH care to marignalized women and women who use drugs compared to internal medicine or family medicine colleagues. For example, in discussing how being an OB/GYN differs from other specialties regarding training on the provision of SRH care to women who use drugs, an OB/GYN physician, a White woman, explained: I think it depends on which residency program you train at, but I think that sexual and reproductive health [is] embedded in what you do as an OB/GYN… Every patient you encounter, you’re talking about not only their past medical history of pregnancies, sexually transmitted infections… but then you’re also screening patients routinely, talking about harm reduction, contraception practices, safe sex practices (Participant ID 018).
Another provider, a primary care and sexual health nurse practitioner, a White woman, also reflected on the unique aspects of her professional background, saying that: Because of the women’s health degree, or certification, I have a little bit more of a background in sexual health, because then… another nurse practitioner or just an adult health provider, because a lot of young women who present to gynecology providers, a lot of their needs are on sexual health (Participant ID 002).
Multiple providers also mentioned that differences in education among clinical staff have generated challenges in working with different marginalized populations. More specifically, in referring to the education of nursing staff, an OB/GYN physician, a White woman, explained: “There’s definitely differences I feel in their sort of understanding of substance use disorder in the chronic disease framework and trauma-informed care… like all those things seem to be kind of unfortunately like a notch below kind of where I see most of our midwives in obstetrics” (Participant ID 006). Another provider, an OB/GYN resident, an Asian/Asian-American woman, reflected on differences in the nursing population itself, explaining that: My coworkers and my co-residents are fairly diverse, but the nursing population that we work with is not, and I think that in communication with the nurses… some of the concerns that they expressed to me as a provider sometimes seem to be rooted in racist beliefs about the patient (Participant ID 012).
Lastly, providers discussed how the unique aspects of the clinical contexts in which they worked influenced their provision of SRH care to Black and Latina cisgender and transgender women who use substances. For example, a nurse practitioner, a White woman practicing primary care and sexual health, discussed how working in a healthcare institution in which a large proportion of the patient population used drugs helped her feel better prepared and equipped to provide high-quality SRH care to Black and Latina cisgender and transgender women who use drugs. She explained: “I’m not in a place where, like, I get an occasional person who’s using substances, needs sexual health, identifies like [as] a Latino trans female, right? Like I’m in a place where, like, those are the patients that I’m seeing all the time” (Participant ID 002). Another provider, an OB/GYN resident, an Indigenous woman, reflected on how the person-centered culture of her clinic positively influenced her provision of SRH care to women who use drugs with minoritized racial/ethnic and/or gender identities: “The culture of where we work is so patient-centered, it’s so advocacy forward that I feel like if I want to know more about a topic, I can just shoot an email to someone and then they’ll send me like a million different resources, which is awesome” (Participant ID 015). In contrast, multiple providers described the challenges they faced in providing high-quality SRH care to Black and Latina cisgender and transgender women who use substances as a result of pervasive substance use and HIV stigma in the clinical settings in which they worked. For instance, referring to the provision of medication-assisted treatment, a family medicine nurse practitioner, a White woman, said: “My current clinic is a little antiquated, where certain providers are like, I don’t touch those patients. And refuse to prescribe it [Suboxone]… I have like three providers who don’t do Suboxone or just refuse at my current job, and I’m just like- I don’t understand that” (Participant ID 010). One participant, an OB/GYN physician, a Black woman, also described how she has had to educate and challenge other providers to ensure the provision of high-quality SRH care for marginalized patients: [There was] a patient with HIV where the nurses wanted to disclose that to the partner… [that] was probably my first real interaction with people who, you know, not bad physicians, but just had very different training. You know, I worked more with the nurses and with the residents, you know, teaching them about my patients, teaching them about like - this is - this is her life story. Like, I know you see her as a snapshot, but this is her backstory. Don’t let her die (Participant ID 014).
Impact of providers’ social identities and lived experiences on the provision of sexual and reproductive healthcare to Black and Latina women who use substances
Many SRH providers reflected on how their social identities and related lived experiences have impacted the way they provide care to marginalized groups of women who use substances. Specifically, in discussing how the identities they share with (some) marginalized patients have helped them connect with their patients, a sexual health registered nurse, a White man, mentioned: “I think my lived experience is that I’m a white trans-masculine person and I definitely present as queer… I think people, especially gender minorities, you know, there is kind of like an instant comfort and connection that naturally sort of happens during the visit” (Participant ID 003). Another provider, an OB/GYN resident, an Indigenous woman, expressed similar sentiment, saying that: “My own background is one of lower socioeconomic status and being a person of color, so I think that is a little bit more automatically easy to relate to” (Participant ID 015).
Other White and cisgender providers discussed how their lack of shared minoritized social identities with the marginalized patients they see has required a more intentional effort to further educate themselves on the unique needs of Black and Latina cisgender and transgender women who use substances in particular. In discussing identity discordance, an OB/GYN physician, a White man, said: “There’s the real-life experience of learning how to do reproductive healthcare. Especially doing it as a man. It takes a special type of training, like figuring out getting people to trust… a lot of it is just experience” (Participant ID 005). Another provider, an adolescent medicine physician, a White woman, reiterated that: [As] a cis het white woman … I’m discordant in identity for a lot of my patients that we’re talking about… I feel like I educate myself to make myself the best provider that they can deal with within that identity. I imagine that they prefer a more congruently identified person who is also educated (Participant ID 011) (Figure 1)
Discussion and Conclusions
Our study aimed to understand SRH care providers’ views and experiences regarding their training in relation to their provision of care for Black and Latina cisgender and transgender women who use substances. Using an intersectional-informed thematic analysis approach, we found that SRH care providers faced significant challenges in obtaining adequate training on the specific experiences and needs of Black and Latina cisgender and transgender women who use substances. Specifically, we found that the vast majority of participants lacked training addressing how multiple forms of discrimination and stigma and discrimination, including racism, transphobia, and substance use stigma, simultaneously shape the SRH needs and care of Black and Latina cisgender and transgender women who use drugs, and that, in turn, providers needed to supplement their training through professional experience and clinical interactions to adequately meet the SRH care needs of these multiply marginalized patients. Viewed through an intersectional lens, medical and nursing training that fails to address the SRH care experiences of groups of women experiencing racism, transphobia, and substance use stigma reflect larger structural inequities in the healthcare system and society more broadly, in which the social, economic, and healthcare needs of multiply marginalized people are often ignored.52,53
Additionally, our findings illuminate that SRH provider training varied in relation to both their professional and personal backgrounds. For instance, the specialty of the provider and the unique qualities of different training programs influenced their preparedness, or lack thereof, to meet the SRH care needs of Black and Latina cisgender and transgender women who use substances. SRH care providers also mentioned that systemic barriers in the clinical contexts in which they worked, including healthcare provider burnout, a lack of time, and the private insurance reimbursement model, also restricted their ability to pursue additional training on the unique SRH care needs of marginalized patients and their capacity to adequately address their overlapping social and health needs.
Multiple studies have shown that Black and Latina cisgender and transgender women who use substances face negative SRH care experiences as a result of discriminatory and stigmatizing interactions with providers.7,14,17,54,55 In one such study, researchers highlighted that those with mutliple marginalized social identities, such as African-American LGBTQIA+ persons, face lessened shared decision-making and heightened discrimination in healthcare settings. 56 Our findings extend this literature by demonstrating that these negative experiences are shaped not only by explicit and implicit bias but also by systemic issues in medical and nursing education, which often fails to address racism, transphobia, and substance use stigma altogether, let alone in conjunction52,53
Our findings regarding how medical and nursing professionals seek to enhance their knowledge of and skills in providing care to marginalized patients outside of formal curricula align with prior studies.18,21,26–30,32,37 However, the existing literature rarely situates gaps in provider training within an intersectional framework that captures how multiple forms of discrimination and stigma converge to simultaneously influence provider preparedness and patient experiences or attends to the unique and specific SRH care needs of Black and Latina cisgender and transgender women who use drugs in particular.
Our study works to address these gaps by highlighting the failure of healthcare education to adequately prepare SRH care providers to provide high-quality care to Black and Latina cisgender and transgender women who use substances. Providers’ professional backgrounds, clinical practice contexts, and social identities intersect with these systemic training gaps, in turn influencing how providers engage with multiply marginalized patients and navigate trust-building in clinical interactions. Further, current research has articulated that clinical interactions with patients who hold marginalized social identities and positions is vital to the reduction of bias and the development of skills in treating patients with overlapping social and healthcare needs, like those who are socially and/or economically marginalized or use substances.18,24,28,30
Our study contributes to current research by presenting evidence that clinical engagement with marginalized patients not only fills gaps in healthcare but occurs predominantly outside of formal medical and nursing education. Clinical exposure not only supplements formal education but is structured by first-hand experience relevant to providing high-quality care to multiply marginalized patients, including learning to navigate racism, transphobia, cisnormativity, and substance use stigma simultaneously. Lastly, our study suggests that SRH care providers’ personal commitment to continuing their education is critical for seeking out training opportunities beyond formal curricula. This finding highlights a notable disparity between providers who have a personal interest in furthering their education for the betterment of care provision to marginalized women who use substances and those who do not.
Previous work has also suggested the importance of healthcare provider identity concordance, with some patients who hold marginalized identities expressing a preference for healthcare providers with the same racial or ethnic identity. 57 Despite this, other patients have noted that healthcare provider identity concordance can reproduce harmful power dynamics and is thus a hindrance to positive clinical interactions. 8 Of note, our study uniquely addresses the influence of providers’ social identities, lived experiences, and professional background on their provision of care for marginalized groups of women who use substances. Moreover, the present study situates these findings within an intersectional context, showing that identity concordance interacts with structural systems of oppression and institutional factors to shape trust, patient comfort, and shared decision-making. 8
The differences in training experiences, resulting from provider specialty and unique aspects of different healthcare training programs, impacted exposure to training on and experience with providing care to marginalized groups of women who use substances. Additionally, our study highlights how individual identity concordance or discordance led to a perceived heightened or lessened trust, respectively, between SRH care providers and marginalized groups of women who use substances. Importantly, increased trust between patients and providers can lead to greater patient comfort, better shared decision-making, and lessened negative interactions.56,58 Moreover, these factors converge to influence provider preparedness and patient experiences, reinforcing that intersectionality provides a critical analytic lens for addressing these dynamics and adequately meeting the SRH care needs of Black and Latina cisgender and transgender women who use drugs.52,53
Other researchers have emphasized the systemic barriers that healthcare providers face in continued training, such as provider burnout and inadequate compensation for furthering their education. 59 We add to this research by identifying the unique systemic barriers a that SRH care providers experience in relation to their provision of care to Black and Latina cisgender and transgender women who use substances.59,60 While burnout, time constraints, and inadequate compensation are widespread challenges across healthcare settings, providers in our study emphasized that these barriers became amplified in the context of providing SRH care to Black and Latina cisgender and transgender women who use substances in particular. This finding highlights the urgency for systemic reforms in providers' clinical work environments as well as private insurance reimbursement models a to allow SRH care providers to more effectively address the specific considerations associated with providing equitable SRH care to marginalized groups of women who use substances.
Our findings should be interpreted in the context of several limitations. First, our sample consisted of predominantly cisgender women SRH providers working in clinic settings. Thus, results may not be reflective of the training of SRH care providers who hold different gender identities and work in other formalized care settings. As a result, future research should recruit diverse participants with various gender identities working in a variety of care settings, including hospitals and federally qualified health centers. Second, interviews were conducted with providers in Rhode Island and Massachusetts. Therefore, results may not be applicable to providers in other geographic locations with different social and political contexts. Thus, more studies addressing SRH provider education are essential to account for differences in provider education among SRH providers in other parts of the United States.
Thus, our findings should be understood in light of the unique social and political environments of Massachusetts and Rhode Island. Both states have expanded Medicaid and invested in harm reduction infrastructure, which may have shaped provider experiences by offering broader coverage for SRH services, reimbursement for substance use treatment, and institutional support for harm reduction practices.61–65 Additionally, Massachusetts and Rhode Island have implemented racial equity initiatives in healthcare, including efforts to reduce maternal mortality disparities and increase access to culturally responsive care.66,67 Providers in our study may therefore have had more exposure to harm reduction approaches and equity-focused policies than peers working in more conservative states. Indeed, in settings where Medicaid expansion has not been adopted, harm reduction remains inconsistent, and racial equity initiatives are underdeveloped, SRH care providers may encounter even less structural support, fewer opportunities for training, and more institutional resistance to providing person-centered care to Black and Latina cisgender and transgender women who use drugs. Thus, future research that explores the views and experiences of SRH care providers working in more socially and politically conservative states ios needed.
Importantly, our findings underscore the need to implement interventions that incorporate LGBTQIA+ health and anti-racist communication into healthcare provider formal and ongoing education.21,26 For example, in one study, researchers developed a problem-based learning course to address gaps in LGBTQIA+ health competencies for fourth-year medical students. 26 After the course, participants demonstrated improvement in their preparedness to treat and comfort in working with LGBTQIA+ patients. 26 Another study improved a course on anti-racist communication, the Presence 5 for Racial Justice (P5RJ) curriculum, in clinical care.21,68 Providers who participated in the P5RJ survey demonstrated competency in discussing anti-racist communication practices; however, the survey’s small sample size is subject to self-selection bias and may have resulted in unstable estimates. 68 Future programs should build on these efforts to incorporate training on multiple, intersecting forms of stigma and discrimination and explicitly incorporating training on intersectionality as an analytic framework to inform how providers engage with racially, ethnically, and gender-diverse women who use substances.
Moreover, SRH care curricula should include information on harm reduction among racially, ethnically, and gender-diverse women who use substances. Given providers' widepsread accounts that their formal training fails to address these issues, it is imperative that formal SRH care curricula be explicitly designed to cultivate these competencies. Indeed, participants' reflections suggest that the absence of training on mutliple forms of discrimination and harm reducation in the context of SRH care constrains their ability to discern how discrimination and stigma undermine SRH outcomes in compounding ways and undermines their capactiy to build skills tailored to addresing the unique social and medical needs of Black and Latina cisgender and transgender women who use substances. Specifically, study participants expressed that medical and nursing competencies in SRH care should include recognizing and addressing intersecting forms of discrimination and stigma (e.g., racism, sexism, substance use, transphobia), practicing trauma-informed and person-centered communication, and engaging with harm reduction as an SRH approach. Participants suggested that effective methods for implementing these skills included case-based learning, community co-teaching with individuals with lived experience of substance use and marginalization, and reflection on providers’ biases.
Additionally, healthcare institutions should work to foster peer-to-peer learning on sexual and reproductive health and harm reduction topics using an intersectional, socially and historically contextualized approach in order to further provider learning beyond formal training. One study highlighted how exchange networks among practicing clinicians can also reduce gender and racial bias, resulting in more accurate treatment recommendations for patients. 69 Healthcare institutions should also work to hire more providers with shared social identities and lived experiences as Black and Latina cisgender and transgender women who use substances. 57 Lastly, policies and guidelines, such as Medicaid reimbursement and efforts to address racism in clinical settings, should be implemented in health care settings in order to support SRH care providers in delivering high-quality, person-centered, and structurally-competent SRH care to socially and econoimcally marginalized groups of women who use drugs.
Taken together, our findings underscore the urgent need for healthcare institutions, educators, and policymakers to integrate intersectional, person-centered, and structurally-competent approaches into both formal medical and nursing SRH care curricula and continuing education and ensure that providers work in institutional environments that support them in providing high-quality care to (multiply) marginalized patients. In particular, ensuring that provider training addresses the specific SRH care needs of Black and Latina cisgender and transgender women who use drugs in the context of racism, transphobia, and substance use stigam will better prepare SRH care providers to deliver care that is responsive to patients' needs. Of note, improving provider education in these ways is not only a matter of reducing individual provider bias but also a structural requirement for meeting the specific SRH care needs of multiply marginalized patients. Overall, the present study underscores that addressing discrimination and stigma at the intersection of race/ethnicity, gender identity, and substance use is both an educational and structural imperative. Implementing intersectional approaches to healthcare provider training and fostering supportive institutional policies and clinical environments for SRH care providers to deliver high-quality care are essential to advancing reproductive health equity and justice for all.
Footnotes
Acknowledgements
Thank you to the members of the 2023-2024 Sexual Health and Reproductive Experiences (SHARE) Lab for their invaluable feedback and collaboration. Additionally, we would like to thank the study participants for taking the time to share their valuable knowledge and thoughtful reflections during this project.
Author Contributions
Eli Wasserman: Writing - Original Draft - Data Curation
Bailey Brewer: Review and Editing, Writing - Accepted Manuscript
Britany Mandeville: Review and Editing, Writing - Original Draft
Caroline Welch: Data Curation, Writing - Review and Editing
Madeline Noh: Data Curation, Project Administration, Writing - Review and Editing
Angela R. Bazzi: Conceptualization, Writing - Review and Editing
Katie Biello: Conceptualization, Writing - Review and Editing
Madina Agénor: Conceptualization, Data Curation, Writing - Review and Editing, Supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Catalyst Research Grant from Brown University School of Public Health (awarded to M Agénor and K Biello) and a National Institutes of Health (NIH) grant R01DA051849 awarded to K Biello and A Bazzi. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Considerations
All research activities were approved by the Human Research Protection Program (HRPP) at Brown University (IRB# 00000556).
Consent to Participate
All participants provided verbal consent during their interview after a comprehensive discussion of the informed consent forms.