
Abstract
Although many migrant and refugee women in Australia experience healthy pregnancies, inequities in perinatal outcomes persist. Perinatal education supports health literacy and informed decision making about pregnancy, birth and early parenting, yet little is known about how migrant and refugee women become aware of and experience these services. This study explores the experiences of migrant and refugee women in Western Sydney in navigating the Australian health system and accessing perinatal education. We adoted a mixed-methods phenomenological research approach, comprising semi-structured interviews in Arabic, Mandarin, Dari and Hindi alongside a quantitative survey. Purposive sampling was used to recruit women from culturally and linguistically diverse backgrounds through antenatal clinics and community health centres, with participants representing varying levels of engagement in perinatal education. Qualitative data was analysed using thematic analysis and quantitative data were analysed descriptively. A total of 22 participants completed interviews, and 246 participants completed the survey. Nearly all survey participants (92.3%) spoke a language other than English, representing more than 18 languages and 34 countries of birth. Quantitative findings demonstrated low uptake of perinatal education, with 86.2% (n = 212) reporting no engagement with formal programs. Qualitative analysis identified four key themes: (1) Pregnancy as a pivotal introduction to health care; (2) Mirrored barriers to engagement with care and education; (3) Care through connection - social and cultural bridges, and (4) Scrolling for solutions: the digital classroom. Across both qualitative and quantitative data, women described intersecting barriers including language, cost, cultural expectations, and limited awareness of available services alongside facilitators such as bilingual providers, community networks and digital platforms. These findings highlight the need for equity-oriented approaches to perinatal education, including community based and culturally responsive awareness and delivery methods.
Keywords
Background
Pregnancy and childbirth are major life events that place complex demands on women’s physical and psychological wellbeing. In Australia, more than half (56%) of women who gave birth in 2022 were born overseas. 1 This includes women from migrant backgrounds (i.e. people who have migrated to Australia voluntarily for reasons such as work, study or family reunification purposes), as well as women from refugee and asylum-seeking backgrounds (i.e. people who have been forcibly displaced due to persecution, conflict or humanitarian crisis, including those with refugee status, humanitarian visas or who are seeking asylum).2,3
Although many migrant and refugee women experience healthy pregnancies, challenges associated with resettlement, including language barriers, unfamiliarity with health systems, and social isolation contribute to poorer perinatal outcomes compared to Australian-born women.4–6 These disparities include increased risks of gestational diabetes, preterm birth, lower birth weight infants, postpartum mental health conditions, and reduced engagement with perinatal care services.5,7,8 While migrant and refugee populations are distinct, they may share some resettlement-related challenges and are often considered together in literature focused on equity and access in maternity care2,9
Levesque et al.’s 10 conceptual framework of access to health care highlights access as a dynamic interaction between individuals and the health system. It identifies five dimensions of service accessibility (1) approachability; (2) acceptability; (3) availability and accommodation; (4) affordability; and (5) appropriateness which together shape how services are organised and delivered. It also recognises that access is not determined by service characteristics alone. 11 It is generated through the interaction between these dimensions and five corresponding abilities of individuals: to perceive, seek, reach, pay for and engage with care. 10
In the maternal health context, Billett et al.’s 12 qualitative evidence synthesis comprising 27 studies representing women in Australia from 42 countries similarly underscores that migrant and refugee women often face substantial barriers that impact on access to health care across the maternity care continuum. This includes limited access to interpreters, discrimination, and challenges navigating the health system. Positive experiences, by contrast, are strongly linked to culturally sensitive care, respectful communication, and the accommodation of traditional health practices.13,14 In Australia, access is also shaped by visa status, insurance eligibility and local service availability. For migrant and refugee populations, these factors can significantly limit navigation, uptake, and meaningful engagement with care. 15 Together, this work points to the need for maternity care models that move beyond service provision alone and actively address systemic barriers and promote culturally responsive, accessible, and equitable maternity care.
Against this backdrop, perinatal education represents a key opportunity to strengthen understanding, navigation, and engagement with care. It serves as an essential intervention to enhance health literacy, support informed decision-making, and foster confidence, particularly among first-time parents. 16 In Australia, perinatal education classes are generally provided free of charge through the public health system to those who are Medicare-eligible. Community-based programs vary in cost and are not covered by Medicare. 17 In this way, access to perinatal education for migrant and refugee women may be constrained by structural, cultural, and practical barriers, including language gaps, limited system navigation, financial hardship, and the absence of familiar support networks.18,19
Aim
This study explores the experiences of migrant and refugee women in Western Sydney, Australia, in navigating the Australian health system and accessing perinatal education, focusing on the identified barriers and facilitators within this context. 20
Method
Research methodology and design
This study used a mixed-methods phenomenological research design with concurrent quantitative and qualitative data collection. 21 Specifically, we adopted what Mayoh & Onwuegbuzie 22 describe as a “PHEN → quan” model, in which the a primary phenomenological qualitative phase captures participants’ lived experiences in depth, followed by a secondary quantitative phase to add breadth to complement the qualitative findings in a single study.This design enabled an in depth exploration of migrant and refugee women’s experiences of navigating the Australian health system and perinatal education while capturing descriptive information on service use, language and support needs across a broader sample. This model fits with both the discovery-oriented nature of the phenomenological research traditions focused on “the way that a person experiences or understands their world as real or meaningful” recognising that meaning is embedded in human existence, 23 and the traditionally explanatory nature of postpositivist approaches. 22
Ethics and reporting
Ethical approval for this study was obtained from the Western Sydney Local Health District Human Research Ethics Committee (2022/PID00543 and 2022/ETH00479). Reporting of qualitative findings follows the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist. 24 Reporting of the quantitative findings aligns with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.25,26
Setting
Western Sydney, home to 1 million residents, is one of the most culturally and diverse regions in Australia. Nearly half (49.9%) of the population was born overseas—substantially higher than the New South Wales (NSW) average of 31.0% - and over half (54.3%) speak a language other than English at home, compared to 28.2% state-wide. 27 There are approximately 200 self-reported languages, with eight principal languages accounting for about 50% of all non-English linguistic expressions in the area. The region therefore presents a mosaic of global cultures making Western Sydney a key setting for examining access to perinatal care and education among migrant and refugee communities.
Participants and eligibility
Participants were eligible for this study (including both qualitative and quantitative components) if they were women aged 18 years or above and were currently pregnant or had given birth within 2 years from Arabic, Mandarin, Hindi (Subcontinent) and Dari speaking communities. These community groups were selected using local demographic and health service utilisation data to ensure representation of key migrant and refugee populations contributing to childbirths in Western Sydney. Specifically, local demographic data from the Australian Bureau of Statistics (ABS) and perinatal health utilisation data from the New South Wales Perinatal Data Collection were used to identify the largest maternal birth cohorts in the region between 2017 and 2021; Arabic, Mandarin, Hindi (Subcontinent) and Dari speaking communities correspond to the highest birth cohorts recorded in Western Sydney and the state of NSW between 2017 and 2021.
Recruitment
A mix of purposive and convenience sampling was used for this study, designed to target women across three levels of engagement with perinatal education (no engagement, engagement in structured programs, and engagement in unstructured or one-on-one perinatal education) in order to build a comprehensive understanding of the barriers and facilitators influencing perinatal education uptake. Pregnant women accessing antenatal services were recruited through women’s health clinics across the three major public hospitals in Western Sydney Local Health District (Westmead, Blacktown, and Auburn hospitals). Participants were approached by maternity liaison officers, midwives and multicultural health staff at the Women’s and Newborn Health waiting rooms. Women enrolled or attending perinatal education/classes at WSLHD hospitals were also invited to participate by maternity liaison officers and midwives during their perinatal education/classes. Women who had given birth in the past 2 years and had previously attended perinatal education classes were recruited through community health and migrant health organisations, including migrant resource centres that support vulnerable women from diverse socioeconomic and ethnic backgrounds. Information flyers in English and translated flyers in Arabic, Mandarin, Hindi and Dari were also developed to support passive recruitment. Flyers were posted in women’s health clinics and circulated through community networks.
Voluntary participation was emphasised throughout the recruitment process; staff informed women that their decision to participate or not participate would not affect their care and members of the research team obtained informed consent. Participants were advised that they could decline any questions or withdraw at any time without consequences and bilingual staff explained the study in participant’s preferred language. Interviewed participants were provided with a $30 gift card as payment for their time involved in line with Australian guidelines for the reimbursement of research participants.
Data collection
Qualitative data collection
We developed a purpose-designed, semi-structured interview guide, informed by a review of previous literature on factors influencing migrant and refugee access to health care services and education. Specifically, interview guides were developed to explore women’s experiences and perspectives accessing perinatal education and navigating perinatal care in Australia, including a series of open-ended questions as well as prompts to elicit more specific or detailed information. In line with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist, the guides were pilot tested with maternity liaison officers, clinicians and multicultural health staff to ensure clarity and cultural appropriateness.
Interviews were conducted over the phone by bilingual interviewers who were trained in qualitative methods, in the language preferred by the participant (English, Arabic, Mandarin, Hindi or Dari). Debriefing sessions with bilingual interviewers were conducted after each interview to discuss key findings, identify emerging patterns, refine the lines of inquiry, and assess the adequacy and completness of the data collected. All interviews were audio-recorded and transcribed verbatim, and in-language interviews were translated into English using meaning-based translation by bilingual interviewers. The time taken to complete the interviews varied between 45 min and 60 min.
Demographic information including age and country of birth were collected at the end of each interview. Health literacy was assessed using a single-item screener, which asks participants, “How confident are you filling out medical forms by yourself?” a question shown to be a reliable for identifying individuals with limited health literacy. 28
Quantitative data collection
To further support the qualitative insights, a quantitative survey was administered to participants from the same four linguistic communities: Arabic, Dari, Hindi (subcontinent) and Mandarin. Initially, an online survey was made available; however, due to low uptake, hard copy questionnaires were provided in-clinic to those who consented.
Demographic characteristics of survey participants (n = 246).
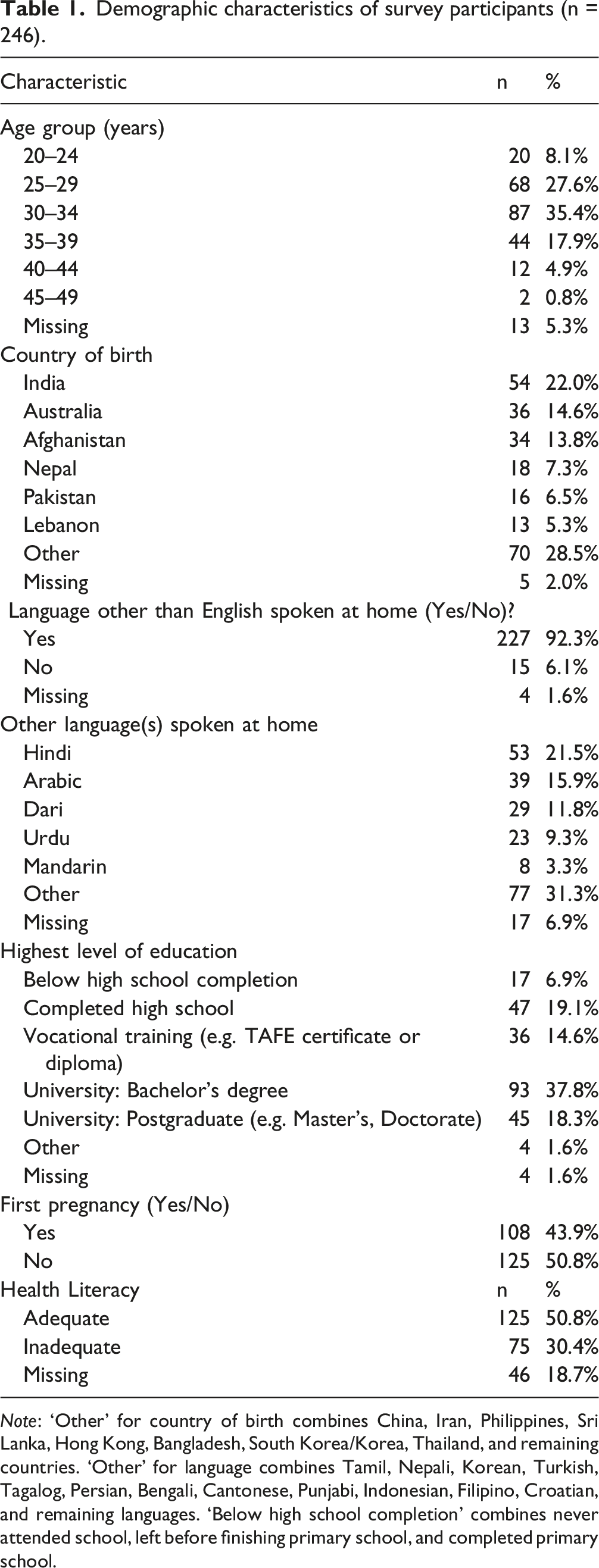
Note: ‘Other’ for country of birth combines China, Iran, Philippines, Sri Lanka, Hong Kong, Bangladesh, South Korea/Korea, Thailand, and remaining countries. ‘Other’ for language combines Tamil, Nepali, Korean, Turkish, Tagalog, Persian, Bengali, Cantonese, Punjabi, Indonesian, Filipino, Croatian, and remaining languages. ‘Below high school completion’ combines never attended school, left before finishing primary school, and completed primary school.
Analysis
The interview data were analysed using reflexive thematic analysis,29,30 with data managed primarily in Word processing software. Analysis was iterative and interpretive, involving repeated engagement with the data to generate patterns of meaning across the dataset. Transcripts were initially read and re-read by DZ and DMM to support data familiarisation and reflexive noting. Initial coding was conducted inductively, with codes developed from the data rather than from a pre-existing framework. These codes were then progressively refined through an ongoing, iterative process of analysis. DZ and DMM met reguarly to discuss developing codes and candidate themes, exploring relationships within and across codes and considering multiple possible interpretations. Themes were generated through an active process of researcher interpratation, rather than identified or agreed through coding consensus, consistent with a reflexive epistomological stance. Themes were then reviewed against the full dataset to ensure they captured meaningful patterns of shared meaning while retaining coherence and distinction. This involved further refinement, re-working and reorganising of themes as analysis progressed. The final themes represent interpretive outputs constructed through engagement between the researchers and the data rather than ixed categories derived from a pre-existing framework.
Quantitative data were analysed using Microsoft Excel, with descriptive statistics used to summarise participant characteristics and key study variables, including means and standard deviations for continuous variables, and frequencies and percentages for categorical variables. These descriptive findings were used to contextualise and complement the qualitative themes.
Reflexivity
Qualitative research is subjective, and the process of reflexivity enhances our understanding of this subjectivity. 31 By engaging in a process of reflexivity, we acknowledge that our qualitative analysis is naturally informed by our understanding and experiences and that the complete elimination of bias is not something that can be achieved in qualitative research and more importantly should not be an aim. Our team brought a range of personal and professional backgrounds to this research. Several members have lived experience of migration and of finding their way through unfamiliar health systems; experiences that informed how we listened to and interpreted participants’ accounts. At the same time, as health service providers and researchers, we were also “insiders” to the very system that participants described as difficult to navigate. We were mindful of this tension throughout the analytic process. Interviews were conducted by both trained Bilingual Community Educators and members of the research team, whose professional roles and personal experiences of health care access may have shaped data collection and interpretation. Their linguistic and cultural proximity to participants strengthened rapport and enabled richer data collection, while also introducing the possibility that shared experience shaped what was elicited and how it was interpreted. For this study, we held regular team meetings to discuss findings and critically reflect on our positionality and representation of research findings. In reporting the results, the study also aimed to centre participants’ words in a descriptive manner keeping their accounts central to preserve their intention and experiences. 32
Results
Participant characteristics
Demographic characteristics of interview participants (n = 22).
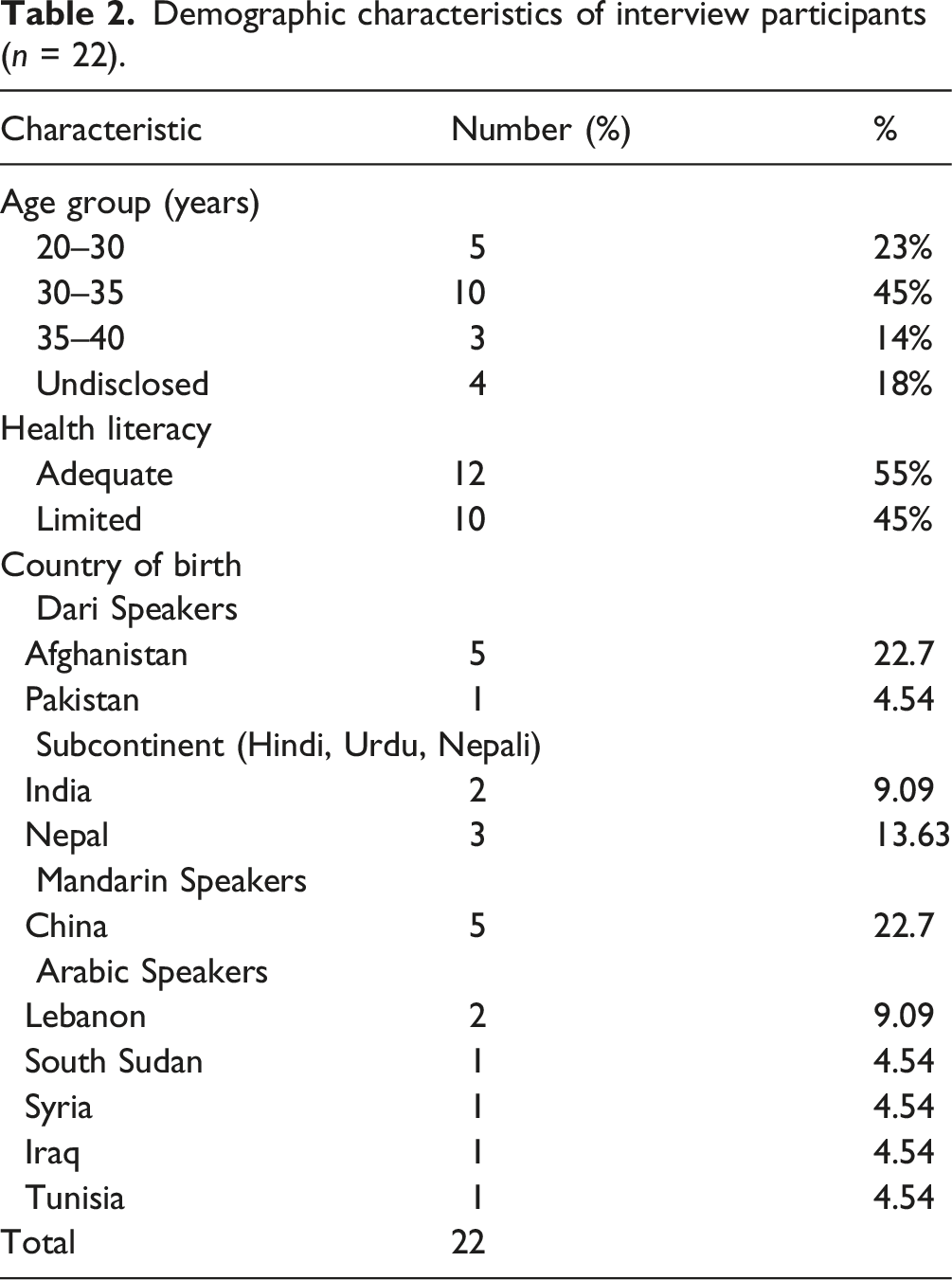
Table 1 summarises the demographic profile of the participants in this study who completed the quantitative survey (n = 246). Two thirds of responses (161; 65.4%) were from the community groups (Arabic, Dari, Mandarin, and Hindi/subcontinent) purposively targeted for the qualitative interviews. Most respondents were aged 25–34 years (63.0%). Participants represented diverse backgrounds across 15 countries, with the largest group from India (22%). Nearly all participants (92.3%) spoke a language other than English at home, encompassing more than 18 languages. The most frequently spoken languages were Hindi (21.5%), Arabic (15.9%), and Dari (11.8%). The majority had completed high school and over half held a university qualification. Just under half reported that this was their first pregnancy (43.9%).
Qualitative results
Through our qualitative analysis, we identified four major themes, illuminating the complexities and multifaceted nature of the challenges and supports encountered by these migrant and refugee mothers in the perinatal context: (1) Pregnancy as a pivotal introduction to with health care, (2) Mirrored barriers to engagement with care and education, (3) Care through connection - social and cultural bridges, and (4) Scrolling for solutions - the digital classroom.
Theme 1: Pregnancy as a pivotal introduction health care
For many migrant and refugee women, pregnancy represents a pivotal introduction to Australia’s health system. Participants often described how their pregnancy was the first time they had engaged extensively with the health system, with some articulating a dichotomy of feelings and emotions that marked their pregnancy journey in a new country. “My pregnancy is the first time I have interacted with the health system here in Australia” (Hindi 4) “I was so happy to find out I was pregnant, but also afraid of having a baby here alone for the first time, away from my family. Giving birth was an unknown area, and I wasn’t sure how things would go.” (Arabic 4)
For some participants, their perinatal journey was perceived positively, with care described as being “pretty good” and women feeling that “our needs are well addressed”, Participants shared stories through which markers of care and quality were seen in both visible actions (e.g. staff taking the time to teach new mothers how to care for their babies; regular calls for appointments) as well as less visible, patient-centred values (e.g. respect, understanding, “genuine care”). “I stayed in hospital for 3 days after giving birth. During that time the nurses showed me how to bathe the baby, helped me have my first shower, taught me how to feed the baby, and even massaged my shoulders sometimes. They were very nice and supportive.” (Arabic 5) “I liked it when they called me regularly for appointments and visits.” (Hindi 1) “I’m very happy my three kids were born in Australia…The places are clean. They treat me calmly, with respect, and they understand me.” (Arabic 2)
Participants’ narratives reflected that their early experiences were foundational in determining their overall confidence and willingness to engage with health services in the future, demonstrating pregnancy as a key opportunity for establishing trusting, meaningful relationships between migrant and refugee families and the Australian health system. Positive encounters during pregnancy often led to greater trust and satisfaction, encouraging continued engagement with health services: “I’m encouraged to become pregnant again and have more kids because it's such a fantastic system.” (Arabic 5)
Theme 2: Mirrored barriers to engagement with care and education
While many participants reported positive experiences and markers of care, the intersection of structural, social, financial, linguistic and cultural factors played a defining role in shaping migrant and refugee women’s experiences with the Australian health system. Participants highlighted barriers such as communication and language difficulties, financial constraints and limited access to Medicare as significant obstacles to engaging with care during the perinatal period. These challenges created anxiety and uncertainty, reinforcing structural inequities.
Through our analysis, we identified that the barriers to health care broadly mirrored those discussed in relation to perinatal education. Participants’ accounts of perinatal education were embedded within, and shaped by, their wider experiences of care.
Communication and language
Communication was reported as one of the most significant barriers to engaging with health care services, particularly during critical health moments. Perceived inabilities to effectively communicate health information, as well as reports of missed or lacking communication on the part of health care providers, created stress, fear, and uncertainty. “I am not good at English. I was afraid that I couldn’t communicate well when in the hospital, which might affect the baby.” (Chinese 5) “During the antenatal appointment, the staff was very nice and provided much-needed information. However, communication was lacking when I needed to meet the early pregnancy team… I needed to know why I was bleeding—what was happening? They had no answers for me.” (Arabic 6) “Sometimes they forgot to tell me about my ultrasound reports—they didn't explain properly. I didn’t know the status of my baby or what was going on.” (Hindi 4)
As it pertained to education, women often reported a lack of communication – and subsequent lack of awareness – about perinatal education opportunities. While many expressed that they “would have attended if I knew about the classes” (Arabic 5), common sentiments that “nobody told me about the classes” (Arabic (2) pervaded conversations. “I was not informed of any additional services …I didn’t know about these classes” (Arabic 3) “No one told us where to go” (Chinese 4).
Participants also specifically described significant language barriers across their perinatal care journey, including the absence of interpreters during labour and limited access to translated materials. Some relied on family members for language interpretation, raising concerns about privacy and incomplete understanding “The biggest obstacle was language. I didn’t have an interpreter when I was giving birth. Everyone was speaking English… There wasn’t an interpreter or Chinese information, so I couldn’t understand those special terms and meanings.” (Chinese 1) “From pain levels to telehealth usage… For people who cannot read or write even in their own language, it’s challenging to enter all the details in English to see a doctor.” (Arabic 3 and Dari 4) “I had to rely on my husband to translate everything for me, and sometimes I felt like I wasn’t getting the full picture from the doctor.” (Arabic 3)
Where available, the quality and availability of interpretation services were described as variable. Women faced challenges in this respect, particularly when interpreters did not fully understand their dialect or cultural nuances. However, in one-on-one settings, some participants were able to adopt strategies to navigate communication even in sub-optimal conditions. “I needed an interpreter for all my appointments. I found the Sudanese interpreter didn’t always understand my Syrian dialect. The Lebanese interpreter was easier to talk with.” (Arabic 5) “On the phone or in person, they usually ask if I need an interpreter. I can understand Lebanese and Egyptian dialects, but if it were an Iraqi dialect, I would ask them to speak slowly.” (Arabic 3)
Participants described similar experiences highlighting the importance of language alignment and bilingual support in perinatal classes. Many reflected on the benefits of engaging in in-language programs but noted that these educational offerings were not always available; most of the public health system’s perinatal classes were delivered in English only. “They’re most of the classes… the other classes that are from hospital… it’s all in English.” (Hindi 5)
Women’s shared experiences highlighted the essential role that bilingual educators play in communicating links to – and engagement with – perinatal education. “I attended online Zoom antenatal classes which was recommended by the doctor. It was run by the hospital. The doctor was speaking in Chinese. (Chinese 1) “I got a message from the bilingual health worker about the time and place of the antenatal class. It was a face-to-face class” (Dari 5)
Costs and practical constraints
Cost was a recurring theme among participants, with both direct and indirect health care expenses preventing full engagement with perinatal services. Women on temporary visas or those without private health insurance reported facing significant financial strain, including substantial out-of-pocket costs for maternity care. Participants highlighted uncertainties about their eligibility for services, as well as difficulties navigating complex administrative requirements for health care access. “For my first baby, I was on a visitor visa, so it cost me ten thousand dollars out of pocket.” (Arabic 3) “As I am on a student visa, I need to wait for a certain period to access midwives—otherwise, it is out of pocket.” (Hindi 5)
The quote below highlights the financial uncertainty and emotional burden experienced by some migrant women navigating perinatal care in a new health system. Concerns about Medicare eligibility and the cost of care added layers of stress during pregnancy, impacting their sense of security and wellbeing. “I was constantly worried about how I would afford my medical care and whether I was eligible for Medicare. It was exhausting and stressful.” (Hindi 5)
The same financial barriers were evident with respect to accessing perinatal education, with participants reporting that they “did not attend due to cost…lack of funds” (Arabic 3). Here, participants spoke of the significant financial barriers to engaging with education programs only offered at a cost, reflecting the broader systemic issues and disparities within the health system. “Private insurance also did not cover… every class was costing between $200-$300” (Hindi 1). “The first class was free, but the next four cost $60. Now it’s around $150. (Chinese 1) “I did not take any help from any organisations as you would only get benefits or support if you are a permanent resident. Otherwise, you do not get any support.” (Hindi 1)
Hospital fees, transportation costs, childcare responsibilities and financial dependency on partners or family members further constrained women’s ability to attend appointments, classes, and follow-up care. Logistical challenges, including transportation, childcare, and financial constraints, frequently impeded attendance at both perinatal care appointments and education classes: “I went for my check-up visits on my own using the bus or Uber—sometimes my husband, but he had to wait for me for two hours until I finished my appointment.” (Arabic 1) “Mostly with the transport issues, you know, most of the time their husband is at work, and they don’t have anyone. I had those difficulties—those issues. I had to ask someone else nearly every time to drop me at the hospital for my appointments.” (Arabic 3) “Transport could be a reason to stop women from attending the classes” (Arabic 2).
Cultural norms and expectations
Cultural expectations and norms also influenced how comfortable women felt engaging with health care services and education. For example, in clinical settings some women expressed discomfort receiving care from male health care providers given that they “come from a very conservative family background” (Hindi 3). Cultural sensitivities were similarly reported to affect participation in perinatal education with many women preferring gender-specific or individual sessions. Here, the desire was not only for health care services to “provide information in own language” (Arabic 2) but also to “respect the culture”. “…would prefer…a ladies-only group” (Arabic 6). “Men and women were placed together in one class. I was with my husband. It was very uncomfortable for me. I didn’t want to attend with all those images and pictures with other men in the room.” (Dari 3)
Theme 3: Care through connection - Social and cultural bridges
Bilingual family and community members as well as health care providers and community workers significantly shaped migrant and refugee women’s perinatal care experiences, playing a key role in bridging communication gaps and facilitating effective health care and educational engagement.
Bridging care through bilingual health care providers
Women frequently described bilingual General Practitioners, Maternity Liaison Officers, and community health workers as vital resources who improved their ability to navigate perinatal care services, sharing how receiving care from providers with common language and cultural backgrounds enhanced their feelings of familiarity, and levels of understanding and comfort. “My Arabic-speaking family doctor was very supportive. I prefer contacting and seeing my family doctor or the hospital because they know my situation.” (Arabic 4) “My GP from my hometown state Gujarat—I was familiar with him as I knew him before.” (Hindi 1) “I also visited Chinese medicine practitioners three times throughout my pregnancy. The effect was good.” (Chinese 1)
Accessibility to formal perinatal education was similarly well-received when delivered by Bilingual Community Educators in culturally familiar contexts. Overall, bilingual health care providers were discussed as being key enablers, greatly facilitating meaningful engagement and improving perinatal experiences for migrant and refugee women. “The class was in the Dari language …… information provided was very important especially for first-time mothers who are very anxious and have no family support.” (Dari 6) “It was a huge help- an Afghan bilingual community worker supported me a lot. I had sessions with her on breastfeeding, diet, and exercise during pregnancy.” (Dari 1)
Those who did not have access to in-language or culturally concordant perinatal education reflected that access to such offerings would increase their willingness to engage and enhance learning. “Having antenatal educator from the same cultural background will be better and easy learning.” (Hindi 5)
Family networks as sources of strength and knowledge
Strong social and familial networks further reinforced these formal supports, percieved to offer practical advice, emotional reassurance, and culturally relevant guidance throughout pregnancy and early motherhood. Family members, particularly mothers, sisters, and in-laws were seen to have provided essential advice and assistance throughout the perinatal journey: “I called my mum and my friends in Lebanon seeking advice about my pregnancy… My sister in Lebanon is a nurse, and she supported me greatly over the phone.” (Arabic 1) “My mother-in-law was here helping to take care of me. I moved to her house in the last one to two weeks before my delivery.” (Chinese 3) “My husband's brother is here. They already have a baby ‐ we are getting ideas from them.” (Hindi 5)
Peer networks, including friendships and community groups, served as additional sources of reassurance and information, particularly from those who had recently experienced pregnancy and childbirth. These informal relationships were described as allowing women to exchange practical knowledge, resources, and emotional support, enhancing their preparedness and confidence in navigating perinatal care. As one participant shared, “I have two WeChat mother groups, one group of mothers who delivered the baby in April and May…. very helpful to me…. they’ve shared a lot of experience with me” (Chinese 4). “Special thanks to my friends who have already given birth. They taught me many details—preparation, what to be aware of, precautions.” (Chinese 2) “Because of my first pregnancy's experience I had many friends who supported me when I became pregnant again.” (Arabic 3)
Theme 4: Scrolling for solutions: The digital classroom
Many participants described how social media, search engines, and online communities were their primary sources of information, often in response to barriers in the formal health system. For many women, digital tools provided a readily accessible and familiar way to seek information, with participants recognising that “we could get any information from Google”.
When health services felt unfamiliar, hard to reach, or not quite aligned with their cultural needs, many women turned to the digital world for support. Platforms like YouTube, Google, and social media became their go-to guides to accessible, relatable, and often available in their own language For many migrant and refugee mothers, pregnancy was a journey navigated not just through clinics and classes, but through phones and shared screens. In these online spaces, health knowledge wasn’t something handed down; rather, it was something discovered, shared, and made sense of together. “I go to YouTube or search Google to answer my concerns about the right food suitable with pregnancy, the right position to sleep.” (Arabic 1) “I am good at gathering information from the internet. I often find most of it and continue looking” (Arabic 3) “On the internet, I watch symptoms, trimesters, and YouTube videos.” (Hindi 5) “Sometimes I use Google to find out whether the chilli I consume may harm my unborn child.” (Arabic 2)
Participants spoke about the internet as a way of reducing reliance on a health system that wasn’t always responsive to their cultural or linguistic needs and preferences. Here, digital educations’ appeal lay in its cultural familiarity and linguistic appropriateness; participants described being able to source “information and support” immediately in-language via online resources and accounts. “I have relied on myself, getting the information and support I needed through searching Google in Arabic language.” (Arabic 1) “I also used social media. I followed a TikTok account of a doctor from my country who gives information about pregnancy. I also searched for information in my own language.” (Hindi 2)
For some, online information supplemented the communication they received within the health system and helped to bridge gaps left in their understanding. “YouTube helped me understand better.” (Chinese 1) “Later I watched YouTube of Indian doctors in Hindi, especially for Hindi translations of English medical terms to understand them better.” (Hindi 2)
Direct comparisons were made between traditional perinatal education and online information. Many women preferred digital resources over traditional classes, citing convenience, accessibility, and affordability. Even where direct comparisons were not made, participants emphasised characteristics of online education which stood in contrast to currently available perinatal education (e.g. free of cost). “These days, lots of information is available on social media, so they prefer to search on the internet rather than spending time, effort, and money to go to these classes.” (Hindi 3) “I didn’t attend the antenatal class in the hospital. I attended one online. I found it from ‘Little Red Book’ App.” (Chinese 1) “I got such information from the WeChat group. I have a friend who works in an Obstetrics and Gynaecology Hospital. She sent me the link. I happened to be free. It was in Chinese.” (Chinese 2)
Social media platforms provided more than just information, they fostered a sense of community and shared learning. Participants described engaging with WhatsApp, WeChat, and Facebook groups to connect with other expectant mothers, seek advice, and discuss their experiences. “We chatted more via WeChat, sharing parenting experiences. There were also face-to-face meetings but only occasionally due to the pandemic. There were about ten of us who gave birth to babies at a similar time.” (Chinese 2)
Despite the benefits, participants also highlighted challenges in navigating digital health information including credibility concerns, noting that not all online information was accurate or reliable.
Quantitative results
Survey questions and responses related to access to health services and antenatal education during pregnancy.
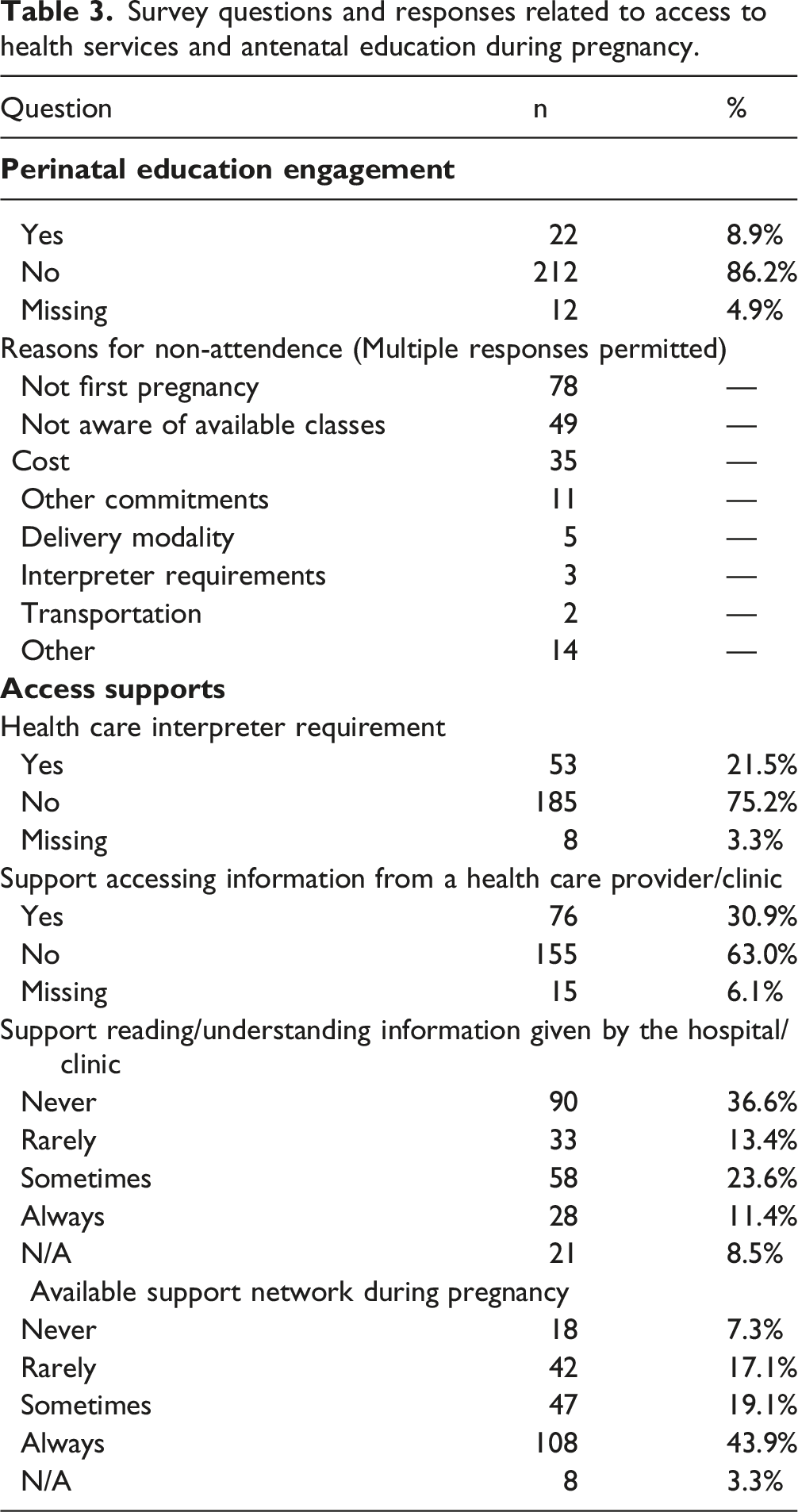
While just over one-fifth of respondents reporting needed a health care interpreter (21.5%), almost one third (30.9%) indicated they needed someone (such as a family member, friend, hospital staff or caregiver) to help them access information from providers and around one third “ sometimes” or “ always needed help to read or understand information given by hospitals or clinics. 63% of respondents reported that they “sometimes” or “always” had a network of people to support them during pregnancy.
Discussion
Drawing on an in-depth exploration of the experiences of 22 migrant and refugee women from Arabic, Mandarin, Dari and Hindi speaking backgrounds, alongside insights from 246 quantitative surveys, this study highlights how access to perinatal education is shaped by a complex interplay of individual, social, and systemic factors. For many participants, pregnancy represented their first meaningful interaction with Australia’s health system, often characterised by uncertainty and unfamiliarity. Structural and informational barriers including language, cost, limited awareness of available services, and cultural expectations intersected to constrain engagement with both perinatal care and education. Within this context, bilingual educators, providers and culturally familiar support emerged as key enablers of trust and understanding. Extending this, participant accounts highlighted the significant influence of informal learning environments such as social media, peer networks, and community-led initiatives which remain underrepresented in existing literature. 33
Levesque’s et al.’s 10 framework offers the theoretical foundation for interpreting how barriers and enablers to perinatal care and education operate across dimensions of approachability, acceptability, availability, affordability, and appropriateness. The alignment of quantitative and qualitative data in the current study highlight low perinatal education uptake (8.9%) as well as key reasons for non-attendance (e.g. lack of awareness, cost, and language barriers). These reflect Levesque et al's framework and reinforce the significant structural and informational barriers that exist for migrant and refugee women in perinatal contexts. Barriers were evident across all dimensions: limited awareness constrained approachability, cultural norms shaped acceptability, transport and language barriers affected availability, affordability was reflected in participant's discussion of financial cost and appropriateness improved when care was delivered in language and in culturally responsive ways; however, this was not always the case. Our findings are also consistent with broader research on migrant and refugee navigation of health systems beyond the perinatal period. Migration-informed health care research highlights how language barriers, cultural discordance, insecure visa or insurance status, and unfamiliar administrative processes create cumulative barriers across care pathways throughout the life course. 34 The challenges described by participants in understanding referral pathways, eligibility, and associated costs mirror wider difficulties in navigating appointments, entitlements, and insurance structures.
At the same time, international research emphasises the central role of relational resources in supporting health care navigation among refugee and migrant populations. Trusted providers, community workers and family networks often function as informal navigation supports within complex systems.35,36 Models embedding culturally concordant staff or cross-cultural workers have been shown to improve continuity of care, comprehension and trust across health settings.37,38 Our findings sit squarely within this body of work. Specifically, our findings highlight the role of familiar community channels, bilingual educators and digital platforms in making perinatal education more accessible and culturally relevant. This supports the potential to expand delivery beyond hospital-based classes into settings that women already engage with and trust. Offering sessions through community hubs and in-language education can improve reach and uptake, particularly among migrant and refugee communities. Evidence from other studies also points to the value of such approaches: for example, a recent review found the use of community-based venues in high income countries can strengthen engagement and uptake of antenatal programs. 39
The importance of culturally appropriate outreach and the role of familiar community channels cannot be overstated. 40 Research consistently demonstrates that migrant and refugee women are more likely to engage with health information and services when these are delivered through trusted community networks and in culturally and linguistically familiar formats.12,13,41 Digital platforms also served as key self-directed learning tools when formal education was unavailable or culturally inaccessible. These tools offered culturally relevant, accessible information, and fostered confidence and connection in navigating pregnancy. Similar findings have been reported internationally, with immigrant women increasingly using digital media to meet their perinatal information needs in ways that reflect cultural, linguistic, and social preferences.42–44
Strengths and limitations
This study has several strengths and limitations. A key strength lies in our targeted recruitment, which focused on migrant and refugee women across four main language groups. Our sampling strategy enabled rich, culturally specific insights while enhancing the study’s relevance to diverse communities. This was supported by the provision of multilingual study materials, which exemplifies our commitment to addressing language barriers and promoting access. We also benefited from the direct engagement of Maternity Liaison Officers, Midwives, and Bilingual Community Educators in participant recruitment and data collection - an approach that likely fostered trust and encouraged inclusive participation. However, we appreciate that this resulted in an overrepresentation of individuals already engaged with formal health services. Interview translations could not be independently cross checked due to resource constraints and our quantitative data was limited based on pragmatic considerations. Specifically, to maximise inclusivity and feasibility we created a concise set of purpose-designed questions that minimised burden for participants with diverse language and literacy needs. While this approach may have limited opportunities for more extensive exploration of certain issues and precluded the use of validated instruments, it facilitated participation from groups frequently excluded from research. Our decisions also aligned with our “PHEN - Quan” approach which privilages qualitative data in addressing the study aims.
Future directions
The findings suggest that while formal engagement with perinatal education is hindered by structural and informational barriers, informal, culturally grounded support networks continue to play a vital role in navigating pregnancy among women from culturally and linguistically diverse backgrounds. By centering these voices, the study offers concrete direction for health care providers and policymakers seeking to improve the availability, accessibility, and cultural responsiveness of perinatal education.
Improving perinatal education access for migrant and refugee women requires a strengths-based, community-informed approach aligned with the key themes identified in this study. Recognising pregnancy as a pivotal entry point into the health system, early culturally responsive engagement is essential to building trust and shaping future care interactions. Addressing the mirrored barriers across both care and education particularly around language, cost, and awareness demands targeted investment in free, in-language perinatal education that reflects community needs. Bilingual health care providers, community workers, and peer educators serve as trusted intermediaries; embedding them more systematically in perinatal education delivery may enhance cultural safety, strengthen uptake, and reinforce continuity of care. Evidence shows that migrant and refugee families report positive experiences when accessing culturally aligned services. 13 Responding to these insights requires health systems to prioritise co-designed, equity-oriented models and the policy levers to support them, including Medicare eligibility, health care interpreter access, and dedicated funding for culturally specific programs to ensure the right support reaches the right families at the right time.
Conclusion
As high-income countries become increasingly culturally and linguistically diverse with large migrant populations, equitable access to perinatal care and education has become a pressing public health priority. This study highlights how, for migrant and refugee women, pregnancy often marks an important first encounter with unfamiliar health systems an encounter that can shape not only immediate maternal and neonatal outcomes but also long-term trust and engagement. While structural barriers such as language, cost, and cultural misalignment persist, this research underscores the powerful role of community-driven enablers bilingual providers, peer networks, and culturally responsive models of care in bridging these gaps.
These findings hold relevance beyond the Australian context. They call on health systems in all high-income countries to invest in tailored, accessible, and in-language perinatal education strategies that are co-designed with migrant communities and delivered through trusted channels. 39 Doing so is not just a matter of inclusion is a strategic imperative for improving health equity, strengthening integration, and ensuring that no woman is left behind in her transition to motherhood, regardless of where she was born.
Footnotes
Acknowledgment
We would like to acknowledge the valuable contributions of Maternity Liaison Officers, Multicultural Health staff and the Bilingual Community Educators who assisted with recruitment, conducted interviews and supported translation – Nelma Galas, Athena Kandaris, Amina Hadi, Fouzia Hamdard, Hanaa Nosir, Tanuja Sharma and Fiona Zhou.
Ethical Considerations
Ethical approval for this study was obtained from the Western Sydney Local Health District Human Research Ethics Committee (2022/PID00543 – 2022/ETH00479).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of generative AI use
CHATGPT was used to improve the readability and language of the manuscript. The authors have reviewed and made changes after using this tool and take full responsibility for the final manuscript.