
Abstract
The Healthy Living Practices (HLPs) outline nine essential guidelines for maintaining health in remote Aboriginal communities, yet high costs and poor availability make them financially out of reach for many families. We assessed the cost and availability of essential goods required to support the HLPs in eight remote Kimberley community stores, recording prices during three visits in 2022 as part of the SToP (See, Treat, Prevent) Skin Sores and Scabies Trial, and retrospectively comparing these (inflation-adjusted) with Perth and Broome prices in 2024. Owing to limited stock, data were analysed at a Cluster level (geographically proximal communities) using paired-sample t-tests in SPSS. Across 23 store visits, a standardised ‘shopping basket’ was significantly cheaper in Perth ($20.29) and Broome ($21.76) than in remote communities ($39.19–$47.87; p < 0.001); whitegoods (refrigerators, washing machines) were also significantly more expensive remotely (p < 0.01). Availability was inconsistent—the full basket was available in remote stores in only 56.5% of visits, with essential healthcare items frequently unavailable. These findings indicate that affordability and access to goods required to support the HLPs are substantially compromised in remote Kimberley communities, emphasising the need for targeted policy interventions to ensure equitable health outcomes.
Key messages
• In remote Kimberley communities of WA, the goods needed to uphold the Healthy Living Practices cost roughly twice as much as in Perth and Broome (around $39–$48 vs ∼$20–$22 respectively), placing basic food items and hygiene beyond the budgets of many households. • Availability is unreliable, as a complete set of essential items was found on the shelf in only 57% of remote store visits, with first-aid and hygiene basics the most frequently missing. • Major appliances that are critical for healthy skin and home environments, such as refrigerators and washing machines, were typically priced about 45% higher in remote community stores than in metropolitan comparators. • Taken together, these price and supply conditions make achieving the Healthy Living Practices unrealistic without targeted policy measures, including price relief on essentials, freight support, and enforceable minimum-stock standards.
Introduction
Remote Aboriginal communities in the Kimberley region of Western Australia (WA) are located on land with deep, ongoing, and unceded traditional connections to custodians, allowing for the maintenance of cultural strength and identity—referred to as ‘Country’ or traditional estates. 1 However, these communities face significant barriers to achieving health and wellbeing, shaped by the social determinants of health, including inadequate housing, limited access to services, and economic disadvantage. 2 While the regional town of Broome serves as a hub for some services, people living in more remote areas experience delays in household maintenance and repairs due to the limited availability of qualified tradespeople. Accessing secondary and tertiary healthcare often requires travel to Broome or the state capital, Perth, meaning individuals must leave Country for acute or chronic care. 2 The Kimberley also experiences a wet season from November to March, during which heavy rainfall and flooding can further limit access to essential services, disrupt supply chains, and worsen housing conditions. 3 Aboriginal health and wellbeing indicators continue to lag behind those of non-Indigenous Australians,4,5 with diseases such as rheumatic heart disease (RHD) and trachoma persisting at endemic rates despite elimination across the rest of the nation.6,7 These disparities are compounded by systemic inequities, resulting in a disproportionate health burden on remote-living Aboriginal populations.
The Healthy Living Practices (HLPs) provide a framework for sustaining health within the home, consisting of nine key guidelines: (1) washing people, (2) washing clothes and bedding, (3) removing wastewater safely, (4) improving nutrition through the ability to store, prepare and cook food, (5) reducing the impact of crowding, (6) reducing the impact of animals, insects, and vermin, (7) reducing dust, (8) controlling temperature, and (9) reducing hazards that cause trauma. 8 Sustaining these practices relies on access to essential ‘health hardware’—including functioning showers, taps, and whitegoods such as washing machines and refrigerators—as well as the ongoing maintenance of these items. 9 Additional items, often referred to as ‘health software,’ are also essential, including washing powder for cleaning clothes and bedding, soap for personal hygiene, and towels for drying. 8
Given the chronic underinvestment in housing and infrastructure in remote regions, 10 communities require substantial support to establish and maintain healthy living environments. 9 In WA, the Aboriginal Environmental Health (AEH) Program—funded by the State Department of Health—partners with Aboriginal Community Controlled Organisations (ACCOs) to deliver culturally appropriate environmental health services in remote Aboriginal communities. 9 The program prioritises the implementation of the HLPs through a range of services, including urgent plumbing repairs, pest control, health promotion, and safe bathroom assessments. 9 As part of a broader Trial focused on skin health, 11 we analysed the cost of goods needed to support the Healthy Living Practices (HLPs) across eight remote Aboriginal community stores, with a particular focus on the affordability and accessibility of essential health-related products, bringing a novel focus to skin health.
Methods
The SToP (See, Treat, Prevent) Skin Sores and Scabies Trial was launched in 2019 across nine remote Kimberley communities, aiming to reduce skin infections in Aboriginal children aged 5–9 years by 50% through improved identification, treatment, and prevention strategies. Designed as a stepped-wedge cluster randomised trial, it prioritised equitable access to study activities while addressing environmental and social determinants of health, integrating enhanced training, evidence-based treatments, and environmental health initiatives. 12 A core principle of the SToP Trial was Community Participatory Action Research (CPAR), ensuring that communities were actively involved as equal partners in shaping the research, guiding Trial activities, and ensuring locally relevant outcomes. 13 Since most SToP Trial team members—including authors Stephanie L. Enkel, Hannah M. M. Thomas, and Asha C. Bowen—identified as non-Indigenous Australians, cultural mentoring was essential in shaping all aspects of the research, from the delivery of Trial activities to the dissemination of results. The team participated in cultural training and maintained ongoing mentorship with Aboriginal colleagues, including author Rachel Burgess, to ensure the study and subsequent interpretation of data was guided by local perspectives, priorities, and ways of knowing.14,15
The nine participating communities were grouped into four ‘Clusters’ of similar population size. Two Clusters each comprised a single larger community, while the remaining two consisted of three and four smaller communities, respectively. These latter Clusters included geographically proximate communities with frequent movement of people, services, and goods between them, including shared access to local stores (Figure 1). The SToP trial clusters.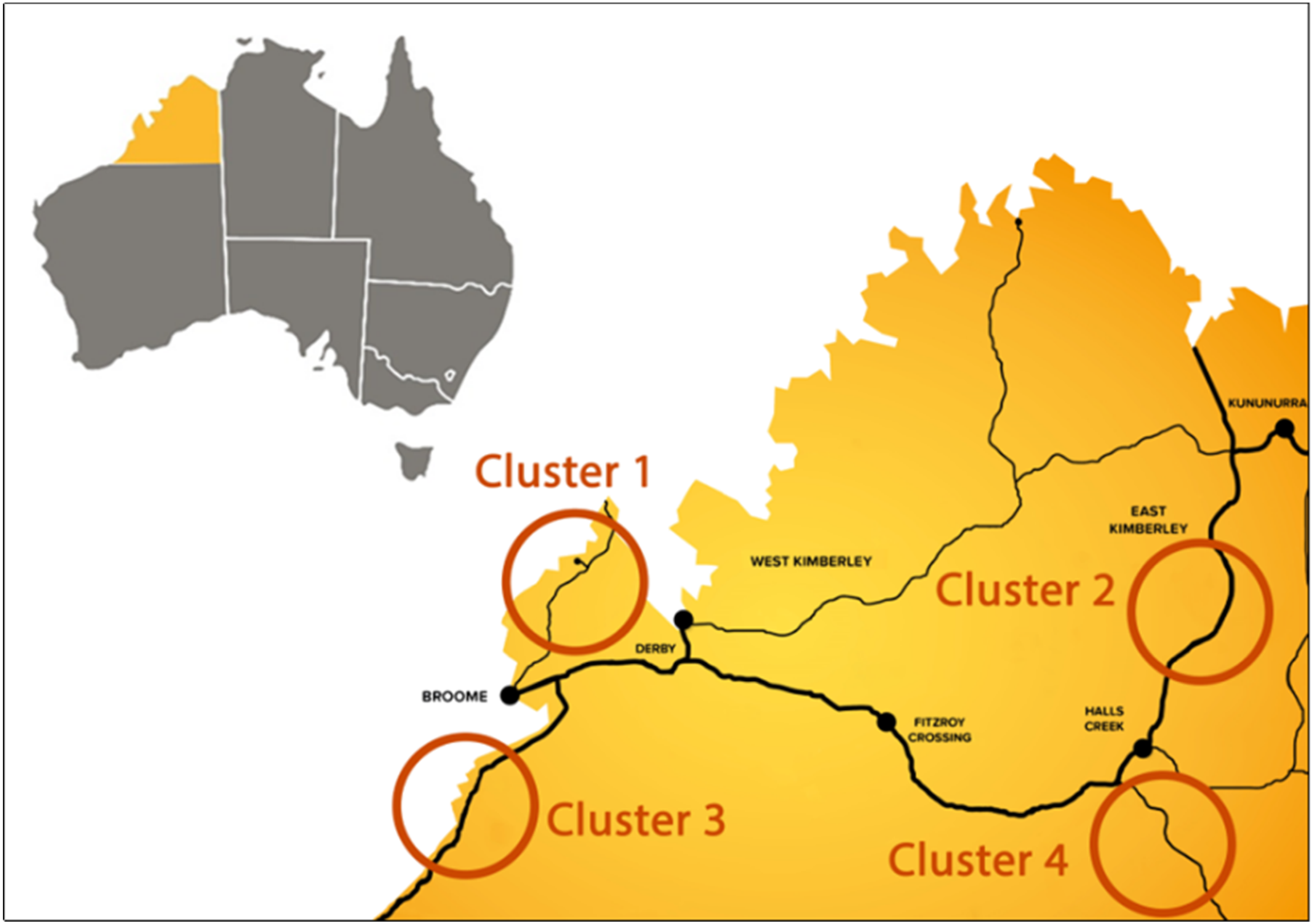
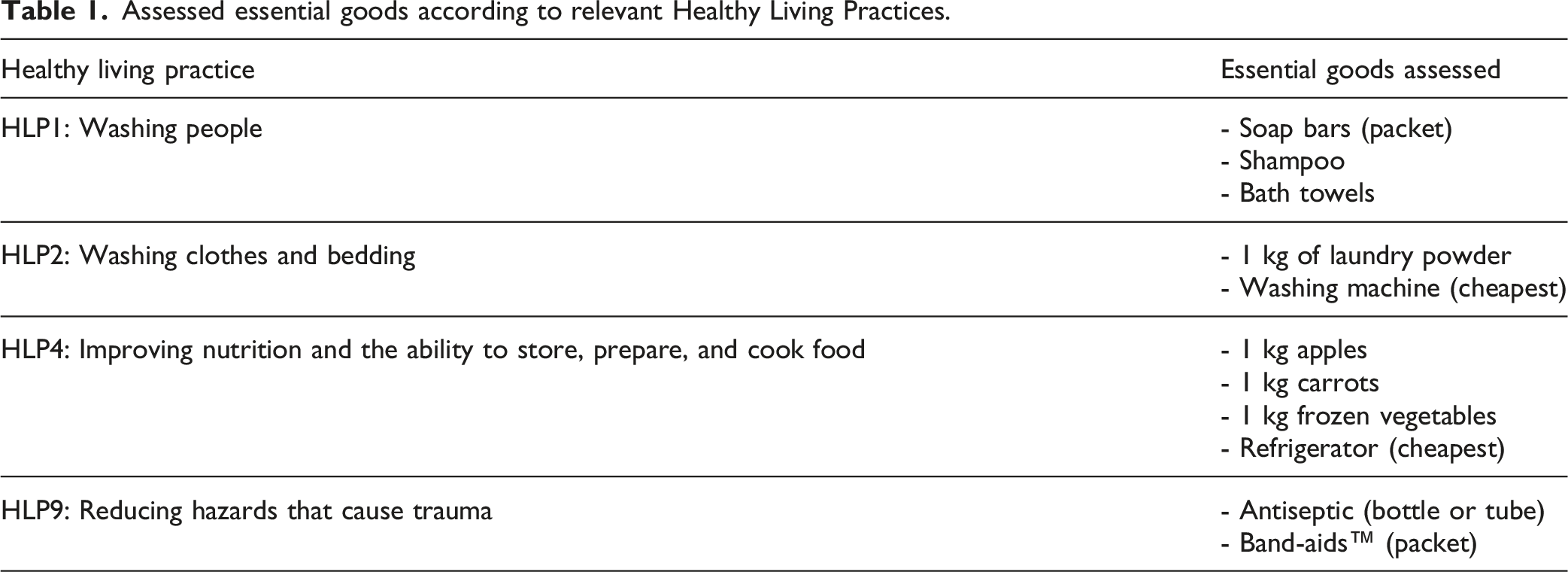
Assessed essential goods according to relevant Healthy Living Practices.
The data collection process was piloted between 2019 and 2021 and refined accordingly, with rigorous quantitative data collected during all three visits in the final year of the SToP Trial in 2022. Photos of household items and their prices were taken to support data entry and cleaning. Full prices were recorded rather than weekly specials to capture the standard listed shelf price rather than temporary promotional pricing, which can vary by store and week and may not be consistently available to households. This approach was used to support comparability across sites. Data were collected using REDCap. 16 In 2024, the cost of household goods sold in remote Aboriginal communities was retrospectively compared with prices in Perth and Broome, where data were collected from Coles and Woolworths—the only two major supermarket chains operating in both of these locations. For these comparator sites, standard listed shelf prices were also recorded rather than weekly specials. To account for inflation, 10.1% was deducted from 2024 prices to ensure parity with 2022 prices, as determined by the Reserve Bank of Australia inflation calculator (June 2022–June 2024). 17 Where whitegoods brands were available, prices were sourced and adjusted for comparison with 2022 pricing.
Data were analysed in IBM® SPSS® Statistics (Armonk). 18 Descriptive statistics were calculated for average prices and item availability. Due to gaps in the dataset—resulting from unavailable items and missing pricing—the average price of each good in each community Cluster was used to construct an overall ‘shopping basket’ (all items noted in Table 1 excluding whitegoods). Items were standardised by volume to allow for comparable calculations: shampoo (500 ml), soap (4-pack), and Band-aids™ (20-pack). Antiseptic could not be standardised due to varying packaging sizes (30 ml tube or bottle). Towels were excluded from Cluster-level analysis due to frequent unavailability. Paired-sample t-tests were used to compare Cluster prices with those in Broome and Perth, as well as differences in the cost of whitegoods. All data are presented de-identified, with brand names excluded.
This work was completed according to The Aboriginal and Torres Strait Islander Quality Appraisal Tool 19 (Supplemental Material 1) and Strengthening the reporting of observational studies in epidemiology Tool 20 (STROBE, Supplemental Material 2).
Ethics
The SToP Trial Partnership Steering Group—comprising representatives from all four partner organisations: The Kids Research Institute Australia (formerly Telethon Kids Institute), Kimberley Aboriginal Medical Service, WA Country Health Service, and Nirrumbuk Environmental Health and Services—granted approval for the study and provided Aboriginal governance, ensuring guidance on data sovereignty throughout the Trial, including all associated sub-studies. With support from the Kimberley Aboriginal Health Planning Forum Research Subcommittee (2017–018), ethical approval was granted by the Child and Adolescent Health Service (RGS0000000584), WA Aboriginal Health Ethics Committee (Ref 819), University of WA (RA/4/20/4123), Catholic Education WA (RP2017/57), WA Department of Education (D18/0281633), University of Notre Dame (2021–128F), and Murdoch University (2022/196) for student projects.
Results
Eight remote Aboriginal Kimberley community stores (with two SToP Trial communities being serviced by the same store) were included in this analysis across 23 separate visits. Only one store visit (4% of total visits) could not be completed due to store closure.
The cost of a shopping basket in Perth and Broome was $20.29 and $21.76 respectively. Comparatively, the shopping baskets in Clusters ranged from $39.19 to $47.87, representing a 1.93–2.36-fold increase over Perth prices and a 1.80–2.20-fold increase over those in Broome. Figure 2 presents a visual summary of the statistics per Cluster, Broome and Perth. Further details are provided in Supplemental Table 1 inclusive of unstandardised amounts. The cost of individual goods and the combined ‘shopping basket’ in the Clusters, Broome and Perth ($AUD).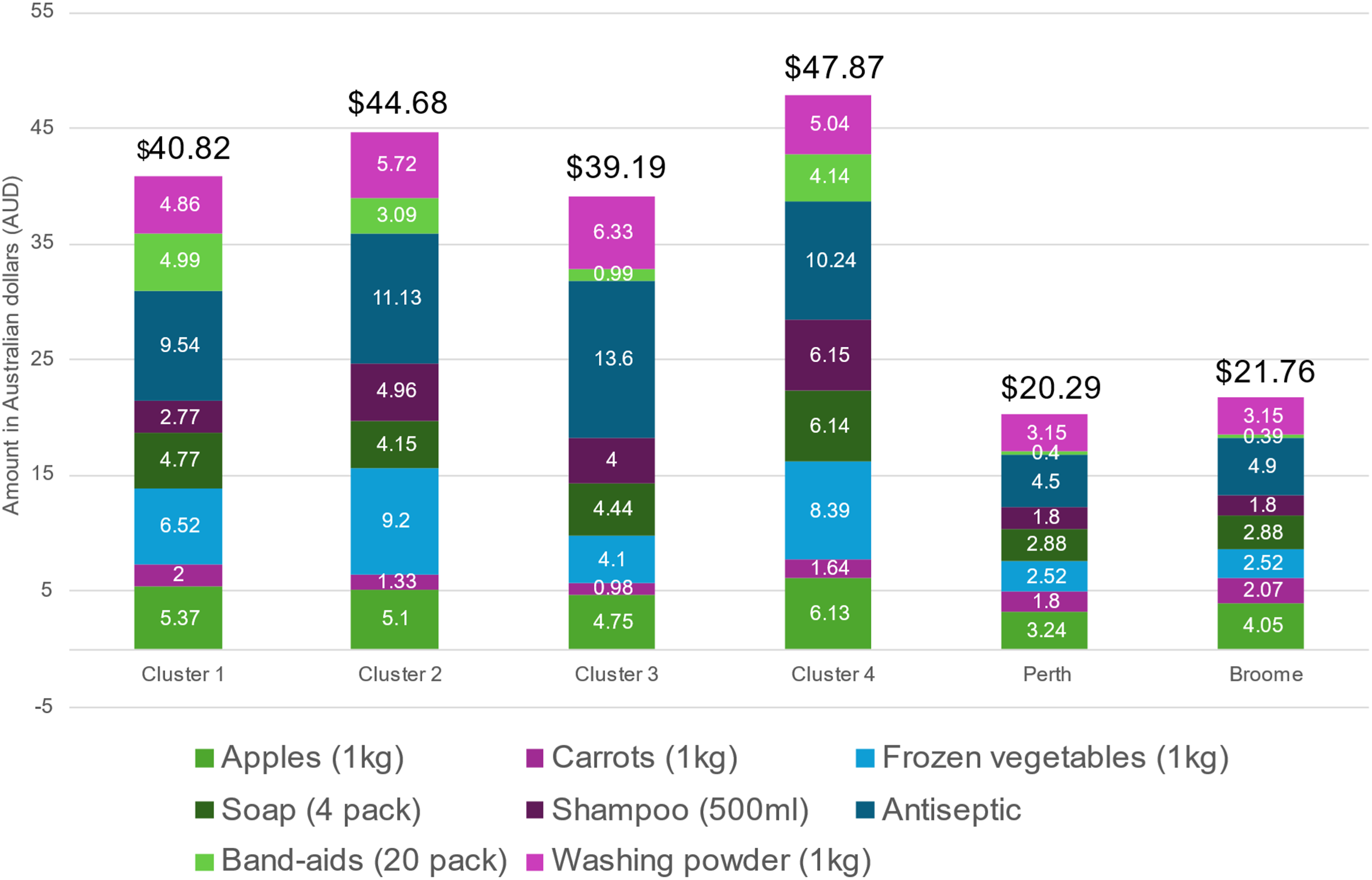
Paired-sample t-test results comparing Cluster ‘shopping baskets’ against Perth and Broome.

Across 23 visits to community stores in 2022, a complete ‘shopping basket’ could only be assembled in 13 visits (56.5%). The most frequently unavailable items were Band-aids™ (26% of visits) and carrots (13% of visits). While not formally recorded or quantified, there was often only a single option available for certain items—such as a single brand and size of shampoo—limiting consumers’ ability to achieve economies of scale and save money.
In 2024, the cheapest bath towel in both Perth and Broome could be purchased from a popular department store for $2.50. In contrast, bath towels in remote Aboriginal community stores averaged $21.58, with prices ranging from $9.85 to $36.99. It was also observed that towels sold in community stores were often the same brand as those available in Perth and Broome, but at significantly higher prices. On one occasion, the same towel that retailed for $6.00 in Perth was sold for $12.50 in a community store. Bath towels were unavailable on five occasions (21.7% of visits).
Fridge/freezers and washing machines were available for purchase in community stores on 18 of 23 visits (78.2%) and 16 of 23 visits (69.5%), respectively. For reasons unknown to the SToP Trial team, these items were frequently stored outside their boxes, increasing the risk of damage during transport to purchasers’ homes. Results indicate that the price of whitegoods in community stores (mean = $945.25, Standard Deviation [SD] = $259.71) was significantly higher than prices elsewhere (mean = $650.65, SD = $172.18); t(19) = 5.73, p < 0.01, representing a 1.45-fold increase (Supplemental Table 2).
Discussion
Remote-living Aboriginal people are paying a high price for their rightful connection to Country, reflected in the ongoing health inequities experienced in remote communities. Compounding this issue, the cost of goods remains disproportionately high, adding further strain to already stretched household budgets. The vastness of WA and Australia more broadly means that goods and services must be transported over long distances, often on unsealed roads, increasing prices to offset additional costs. 21 However, the reality that a ‘shopping basket’ in a remote community can cost almost double that of Perth is deeply concerning, particularly given that incomes in these locations are significantly lower than in metropolitan centres. While these findings demonstrate substantial price differentials, this study did not examine the underlying drivers of pricing, which are likely to be complex and may include freight, supply logistics, scale, and other structural factors worth further consideration.
Prior research has analysed the cost of goods in rural and remote regions of Australia,21–23 however, to our knowledge this is the first occasion where skin health has been the primary focus of the overall study. The inclusion of items such as Band-aids™, antiseptic, soap, shampoo and towels differs from prior investigations in this area. It was encouraging that these items were generally available to consumers, but they were often available at a markedly higher cost, particularly towels. Avoiding towel sharing is a key preventive strategy against the transmission of infectious diseases such as skin sores and trachoma. However, in overcrowded homes, the limited availability of towels in local stores creates both financial and logistical challenges. 24 Additionally, the lack of size and colour options makes it even more difficult for individuals to identify their own towel, further hindering efforts to prevent sharing.
During the Australian Competition and Consumer Commission Supermarkets Inquiry 2024–25, public hearings examined supermarket pricing practices and the relationship between wholesale and retail prices. 25 This included a focus on the competitiveness of small and independent retailers in rural and remote regions. An interesting finding emerging from the first weeks of public hearings was the use of cheap carrots and other produce in some stores being used as ‘clickbait’ to attract customers 26 which may explain the anomaly we observed in our data of carrots in Clusters being generally cheaper than in Perth and Broome. In some instances, carrots were as low as 98 cents in Clusters compared to $1.80 in Perth and $2.07 in Broome. We were only able to assess prices at Coles and Woolworths as stores accessible in Broome and Perth; supermarkets that do not run the cost model that smaller or more independent stores may.
Australia is presently amid a ‘cost of living crisis,’ and while community data were collected in 2022, the inflation index applied in this work is indicative of a situation that could only have become more acute for rural and remote communities. The most recent census statistics (2021) showed median weekly household income of those living in remote WA to be $1,709, lower than the median $1865 in the State metropolitan centre.27,28 As of 31 March 2023, 17% of those living in remote regions were receiving unemployment payments with a total basic rate per fortnight of $762.70 (amounts varying depending upon individual circumstances). These individuals qualify for a remote area allowance of $18.20 per fortnight. 29 Remote-living households not only earn less, but are also unsuitably compensated by Government assistance programs, demonstrating the increased financial pressures of achieving the HLPs. This cost-of-living pressure means that, for some households, purchasing the goods needed to support the HLPs may be unrealistic and unsustainable. However, affordability is only one part of a more complex picture. Whether households are able to achieve the HLPs is also shaped by behaviour, culture, knowledge, local availability of goods, housing and hygiene infrastructure, competing household priorities, community context and involvement, and broader social determinants of health. As such, financial supports may be one useful component of a broader response to improve access to the HLPs, but are unlikely to be sufficient on their own to prevent skin infections without parallel action on the wider structural and social conditions that constrain healthy living practices.
Several election commitments were made in the lead up to the Australian Federal election to alleviate the cost of goods in remote communities.30,31 Notably, the Albanese Labor Government committed to reducing the cost of 30 essential everyday items in participating remote community stores from July 2025, so that prices are more comparable with those in urban supermarkets. This includes flour, milk, canned tuna, rice, bread, beef, chicken, eggs, several fruits and vegetables, toilet paper, nappies, toothbrushes, toothpaste, and menstrual products. 31 While this represents an important policy response to remote food and household affordability, ongoing evaluation will be needed to determine whether it improves access to the full range of goods required to support the HLPs, including skin health items, towels, first-aid supplies and whitegoods.
We did not examine how goods were transported to stores (i.e., road, rail, sea, or a combination of both) and it is likely some goods may have come from Darwin in the Northern Territory; geographically closer to the Kimberley than Perth. Further work investigating the cost of transporting goods to communities is warranted, as are attempts to also understand the effects of natural disasters, seasonal flooding, and associated disruption of supplies. Our data were all collected during the dry season months when fewer natural disasters occur, and hence are likely to reflect lower costs and higher availability than achieved during the wet season when food supply disruptions are frequent.
The lack of concurrent Perth and Broome price data was a limitation, however, this has been adequately managed with adjustments for inflation. Given budget stores such as SpudShed and Costco were not included in the comparative metropolitan analysis, it is likely that described price differences could be even higher. Despite the inclusion of eight remote Kimberley Aboriginal community stores, the incompleteness of each dataset required analysis at a Cluster level, meaning a reduced comparative sample size. However, we are confident in the statistical analysis and believe this research contributes to a continued awareness of the challenges faced by Aboriginal people in managing skin health.
This research is a subset of the broader SToP Trial, yet it provides crucial insights into skin health in remote Aboriginal communities. By examining the affordability and accessibility of essential items needed to support the HLPs, it highlights the significant financial barriers households face in maintaining skin health and preventing infection. The layered disadvantage caused by higher living costs makes achieving the HLPs at a household level nearly impossible. While the rising cost of living is a pressing issue for metropolitan families, this challenge has long been entrenched and magnified in remote communities by structural and systemic factors that are not easily resolved. We call for further investigation into these larger contributing issues and sustained advocacy at all levels to improve the affordability of essential goods that support healthy skin and overall wellbeing.
Supplemental Material
Suppplemental material - Cost constraints in supporting the healthy living practices in remote Aboriginal communities: A Western Australian perspective
Suppplemental material for Cost constraints in supporting the healthy living practices in remote Aboriginal communities: A Western Australian perspective by Stephanie L. Enkel, Hannah M. M. Thomas, Rachel Burgess, Asha C. Bowen in Community Health Equity Research & Policy
Footnotes
Author note
Throughout this paper Aboriginal and Torres Strait Islander peoples are respectfully referred to as Aboriginal as this is the common terminology in Western Australia where this work was conducted. We recognise and acknowledge the diversity between Aboriginal and Torres Strait Islander cultures, and do not intend to diminish any identity. We respectfully acknowledge Aboriginal ownership of the land, waters and sky of Australia in continuity for more than 60,000 years.
Acknowledgements
We acknowledge the diverse Aboriginal Traditional Owners of the Kimberley, their enduring connection to Country for over 60,000 years, and the continued vitality of their languages through Elders and families, including Gija, Walmajarri, Jaru, Kukatja, Karrajarri, Bardi, and Nyul Nyul. We honour the wisdom and contributions of the hundreds of participants, families, community members, schools, and clinics committed to healthy skin in the Kimberley, with insights extending across Australia and the world. We recognise the partner organisations—WA Country Health Service – Kimberley, Kimberley Aboriginal Medical Service, and Nirrumbuk Environmental Health and Services—and their staff for supporting the SToP Trial and its governance. We also acknowledge Catholic Education Western Australia, the WA Department of Education, and all Investigators, staff, students, and volunteers involved in the trial. Finally, we appreciate The Kids Research Institute Australia and the Kulunga Aboriginal Unit for their invaluable support in funding, governance, logistics, and operational planning.
Ethical considerations
The SToP Trial Partnership Steering Group—comprising representatives from all four partner organisations: The Kids Research Institute Australia (formerly Telethon Kids Institute), Kimberley Aboriginal Medical Service, WA Country Health Service, and Nirrumbuk Environmental Health and Services—granted approval for the study and provided Aboriginal governance, ensuring guidance on data sovereignty throughout the Trial, including all associated sub-studies. With support from the Kimberley Aboriginal Health Planning Forum Research Subcommittee (2017–018), ethical approval was granted by the Child and Adolescent Health Service (RGS0000000584), WA Aboriginal Health Ethics Committee (Ref 819), University of WA (RA/4/20/4123), Catholic Education WA (RP2017/57), WA Department of Education (D18/0281633), University of Notre Dame (2021–128F), and Murdoch University (2022/196) for student projects.
Author contributors
SLE: Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review and editing. HMMT: Data curation; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Writing – review and editing. RB: Supervision; Validation; Writing – review and editing. ACB: Conceptualization; Data curation; Funding acquisition; Investigation; Methodology; Supervision; Validation; Visualization; Writing – review and editing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by Australian Centre for Control and Elimination of Neglected Tropical Diseases (APP1153727), Western Australian Department of Health (FHWAYR3-2015/16/KHS), Australian National Health and Medical Research Council (GNT1128950) and Healthway (33088). SLE is supported by a Research Training Program Award, a Wesfarmers Centre of Vaccines and Infectious Diseases top-up scholarship and the Stan and Jean Perron Foundation. HMMT is supported through the Western Australian Early-Career Child Health Researcher Fellowships Program, which is a co-funded partnership program of the Future Health Research and Innovation Fund and BrightSpark Foundation. ACB is supported by National Health and Medical Research Council.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to ethical, governance and Aboriginal Data Sovereignty considerations. Requests may be directed to the corresponding author and will be considered in line with relevant ethics and governance approvals.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.