
Abstract
Modern diabetes care faces increasing clinical and technological complexity. While generalist-led models are widely promoted for continuity and accessibility, they may fall short in addressing the nuanced needs of patients with diabetes, particularly in complex or rapidly evolving clinical contexts. The aim of the article is to critically evaluate whether general practitioner (GP)-led models of diabetes care adequately meet patient needs and to explore the role of specialist access within contemporary health systems. A narrative and conceptual analysis of current literature was applied, focusing on patient-centered care, equity, and the organization of diabetes services. Patient-centeredness and equity should underpin diabetes care, including individualized goal setting and shared decision-making. However, overreliance on generalist-led care may contribute to delays, suboptimal care, and reduced clinical precision in complex cases. Open access to specialist care may enhance patient autonomy and enable more timely, comprehensive, and personalized management. At the same time, general practitioners remain essential for holistic care, coordination, and long-term patient engagement. Integrating specialists within primary care through hybrid or collaborative models may combine the strengths of generalists and specialists and improve outcomes, while maintaining equity. Strategic policy initiatives, workforce planning, and technological innovation are necessary to sustainably expand access.
Keywords
Introduction: Recognizing the dilemma
The generalist model is a system in which primary care physicians act as principal providers and gatekeepers, managing most aspects of chronic disease and controlling access to specialist input. 1 The expansion of general practitioner (GP)-led health care delivery has been widely adopted in an effort to increase efficiency, streamline access, and reduce pressure on ambulatory care.2,3 Nurses have also assumed growing responsibility in managing chronic illnesses, often guided by predefined protocols. 4 In gatekeeping models of care, access to specialists must first be authorized by a primary care provider. In theory, gatekeepers promote equity by judiciously matching health services, including specialty referrals, with patients’ needs. At the same time, they encourage initial contact with primary care clinicians, thereby reducing the need for self-referrals. 5 Though frequently described as “patient-centered”, this scheme often functions as a “Trojan Horse”. It is presented as a gift of improved care and empowerment, yet it ultimately serves as a vehicle for cost containment. The potential underlying drivers, including economic limitations, specialist workforce shortages, and systemic strain, may suggest that generalist-led care is often an unavoidable compromise rather than a principled clinical evolution.
Primary care constitutes the basic level of health services, providing first-contact, accessible, and sustained services for a wide range of medical needs. It is predominantly administered by GPs, who are trained to manage uncomplicated conditions, offer holistic treatment, and coordinate referrals across the health system. Within its intended scope, general practice excels at providing comprehensive, relationship-based care, particularly in the early recognition and routine management of stable or self-limiting cases. Despite the crucial role of GPs in ensuring continuity and availability of services, many patients may eventually receive suboptimal care if they remain limited to this level of services. 6 This is due to a lack of multidisciplinary support, limited promotion of self-management, inadequate adherence to evidence-based guidelines, and ineffective clinical audit. 7 Patients are usually less satisfied with gatekeeping than with direct-access systems. 8
Meanwhile, the increasing complexity and specialization of modern medicine have raised the importance of concentrated expertise in achieving optimal outcomes. Specialization not only enables targeted interventions but can also be cost-effective. 9 As patients become more informed and proactive in their health decisions, the demand for specialized, high-quality care is likely to grow. 10 This dynamic shifts expectations toward more individualized management, especially for chronic and multifaceted diseases such as diabetes mellitus, where nuanced adjustments can significantly impact the clinical course. These realities pose a fundamental dilemma for contemporary health systems: should priority be given to the cost-efficiency of generalist-led models or to the clinical advantages of specialist expertise? This is a crucial question, particularly in diseases like diabetes mellitus, where complexity is the rule rather than the exception. This article aims to critically examine whether the GP-led model of diabetes care genuinely meets patients’ needs or represents a financially driven structural compromise. It also proposes hybrid frameworks for more equitable, specialist-integrated care. The present review adopted a narrative approach to synthesize existing knowledge and ideas. The relevant literature was identified through a targeted review of publications that could serve the construction of a cohesive overview of diabetes care models, the highlighting of ongoing debates about generalist and specialist involvement, and the establishment of foundations for future practices and policies. While the discussion draws on international evidence, it is particularly relevant to countries with gatekeeping systems, where general practitioners play a central role in diabetes management.
Evolving diabetes care: A challenge to the generalist model
The trajectory of modern medicine is undeniably toward specialization and technological sophistication. Across disciplines, and especially in diabetes management, society is witnessing rapid scientific and technological advances that promise to transform the delivery of care. Current technologies, such as mobile health platforms, 11 hybrid closed-loop systems, 12 and artificial intelligence, 13 are increasingly incorporated into routine care. Furthermore, therapies targeted at the cellular level, 14 artificial pancreas systems, 15 and gene editing, 16 are novel interventions that aim to reshape future clinical practice. These innovations envision a prospect of greater self-control, improved outcomes, and increasingly personalized treatments for patients with diabetes. In light of these advances, clinging to traditional models centered on general practice alone may limit some patients’ ability to fully benefit from the next generation of diabetes care.
The increasing complexity further highlights the limitations of a model that confines diabetes management to generalist settings. 17 Effective use of advanced technologies and therapies depends not only on patient engagement but also on a clinical environment that is equipped to individualize care, adjust regimens dynamically, and anticipate complications proactively. Yet, patients often remain managed entirely within the boundaries of general practice, even when their condition progresses beyond the scope of protocolized strategies. Specialist input, if obtained at all, may be indirect, delayed, or reduced to written advice based on second-hand data. Limited knowledge can pose the risk of therapeutic inertia18,19 and clinical imprecision20,21 at a time when personalized, real-time medicine is becoming the new standard.
Advocates of GP-led care often cite improved continuity, accessibility, and budgeting. These benefits are not trivial. Leaning on general practice can offer reliable and efficient solutions, especially in low-resource contexts, conditions of increased demand for medical services, and underserved populations and geographical areas. However, efficiency should not eclipse clinical depth, nor should broad access be mistaken for adequacy. General practice can effectively manage straightforward and non-fluctuating cases, but it may not fully substitute for the diagnostic refinement, interpretive reasoning, or therapeutic judgment that specialist training provides. Therefore, task-shifting, in which generalists or nurses undertake roles of specialists, must be examined critically. While such strategies may be necessary in resource-limited contexts, they should not be established as a normality. Doing so may institutionalize a lower standard of care for the public while reserving precision, specialist-led medicine for selected cases.
Patient-centeredness and equity in care: The missing core
The principle of patient-centeredness has long been heralded as a defining feature of modern health care. This concept extends beyond timely access or continuity of contact with a clinician. True patient-centered care entails shared decision-making, individualized goal setting, and responsiveness to the patient’s values, preferences, and beliefs. 22 It acknowledges that each person’s experience of illness is shaped not only by physiological variables but also by psychological, social, and economic realities. Integrative biopsychosocial approaches can better address the complex needs of patients. 23 A modern patient-centered framework prioritizes timely access to specialist care, seamless communication and coordination between patients and clinicians, and the reduction of unnecessary or duplicative tests. It also emphasizes continuous monitoring of quality, safety, and performance. While evidence supporting this model remains limited and the overall costs and benefits for clinical practices are not yet fully established, it shows significant potential for advancing value-based care. 24
Equity in care implies that health systems can provide clinical services of sufficient quality without imposing excessive inconvenience or costs on patients. 25 Within this concept, fairness is defined not by uniform restrictions but by proportionate opportunities. Equity represents a parallel and inseparable dimension of patient-centered care. A system cannot genuinely claim to be patient-centered if access to expertise varies according to income or institutional affiliation. Nevertheless, even in health systems organized around a gatekeeping model, patients may still use private means to obtain specialist referrals more readily than those who rely solely on standard coverage.26,27 Such disparities constitute a direct violation of the principle of equity in care. In contrast, open access to specialist care may reasonably be regarded as a step toward greater equity within health systems.
Patient-centeredness and equity are interconnected pillars of diabetes care. Appropriate services must adapt to the biological and psychosocial diversity of people living with diabetes and ensure that access to therapies, technologies, and expertise is proportionate to each patient’s needs. Although empirical evidence is still limited, open access to specialist diabetes care may represent an important step toward this vision by reducing avoidable delays, mitigating therapeutic inertia, and aligning care more closely with the principles of justice and patient autonomy. Whether these potential benefits materialize in practice remains to be demonstrated, as outcomes are likely to depend on implementation, workforce distribution, service availability, and utilization patterns. In any case, they warrant serious consideration in the evolution of equitable and patient-centered diabetes care.
The patient’s interests: A sidelined parameter
Clinical outcomes remain a key benchmark in assessing care quality. Evidence suggests that specialist involvement yields measurable benefits for patients with diabetes. Studies indicate that specialist-led care is associated with lower HbA1c values, improved blood pressure control, better lipid profiles, and more consistent weight management.28–30 Patients under specialist care are also more likely to receive comprehensive monitoring, including regular assessments of renal function, lipid levels, and foot and eye health. 31 While the individual gains in each area may appear modest, together they reflect a more attentive and potentially more effective approach to managing the multidimensional nature of diabetes. Nonetheless, other observations indicate that the magnitude of difference in clinical outcomes between specialist-led care and general practice may be inconsequential. However, this should not be interpreted as evidence of complete equivalence. Rather, it likely reflects broader systemic deficiencies in the quality of care 32 or derives from poorly investigated evidence. 33 In general, different settings in health care and variations in research methodology may partly explain the heterogeneity of findings.
One might argue that GPs could undergo additional training to better adapt to the evolving challenges of diabetes management. While this is a reasonable proposition, it effectively amounts to suggesting that generalists should acquire the depth of expertise traditionally associated with specialists. 34 This notion, if extended logically, would imply that GPs should pursue specialized competencies across a wide range of chronic and complex conditions. However, this expectation is both impractical and misaligned with the fundamental purpose of general practice. 35 The scope, and indeed the strength, of general medicine lies in its ability to deliver broad care across the spectrum of patients’ needs, not in mastering the nuanced management of every demanding disease.
The gap between clinical needs and system structures becomes most noticeable in chronic diseases. Conditions such as diabetes exemplify this tension. Although common, this disorder is pathophysiologically diverse, with evolving classifications, numerous comorbidities, and an expanding arsenal of medications. Nevertheless, many systems manage patients primarily in general practice, even when their condition deteriorates or becomes increasingly complex. In some instances, specialists offer advice by letter without having examined or even met the patient, relying solely on reports from primary care clinicians. While this approach is efficient in terms of expenses, access, and workforce utilization, it might lead to fragmented care and lower clinical precision, especially when detailed assessments and sophisticated interventions are necessary.
Justice and autonomy: Ethics beyond the illusion of empowerment
The ethical implications of a GP- or nurse-led model in diabetes care are profound. A system that purports to empower patients while restricting their access to specialist expertise could erode the foundational principles of medical ethics. Justice is challenged when access to specialist care is strictly rationed. Patients with complex or atypical forms of diabetes may not receive timely recognition or appropriate therapy if managed solely in non-specialist settings. Furthermore, structural inequity becomes a looming danger when generalist-led care is the default and often the only realistically accessible option. This may foster a two-speed pathway: a protocol-driven, constrained model for the majority, and a flexible, specialist-guided approach for a privileged minority. Individuals with limited means must settle for generalist-led care, while more affluent patients can access specialist services through private routes. 36
Autonomy requires meaningful choice. While the rhetoric of patient empowerment is common in the field of health management, it rings hollow when the range of available options is narrowed by intentional systemic design. 37 A protocolized, gatekeeping model may offer accessibility to health services in the most basic sense, but it certainly does not equate to optimal care. For patients with diabetes, making thoughtful decisions about adjunctive pharmacotherapies, insulin regimens, continuous self-care, and lifestyle strategies requires access to specialized knowledge, not merely access to care. When such expertise is obstructed and open access is limited to general practice, patients may appear to be autonomous, but genuine empowerment remains a utopia.
These are not abstract concerns. They determine who receives advanced therapies, who attains diagnostic clarity, and ultimately, who avoids preventable harm. If health systems are to remain ethically coherent and scientifically progressive, they must resist conflating what is pragmatic with what is ideal. As Hippocrates cautioned, the duty of medicine is to “benefit or at least do no harm” (“ὠφελέειν ἢ μὴ βλάπτειν”). A system that delays or limits specialized care in the name of efficiency must reckon with whether it is truly centered on the patient or simply functioning within the boundaries of compromise.
General practice in a specialized era: An indispensable role
As diabetes care becomes more stratified, the role of GPs must be understood not as a barrier to advanced care but as a valuable asset within it. More than gatekeepers, GPs can act as navigators, guiding patients through an increasingly departmentalized health system. Embedded within communities, they are uniquely positioned to advocate for patients’ best interests, safeguarding against neglect, inequity, or procedural oversight. They can also manage straightforward cases, thereby contributing to positive clinical outcomes and ensuring that care remains responsive to individual patient needs. In fact, the use of a primary care institution as the main source of care can be associated with lower outpatient and inpatient costs and a reduced risk of hospitalization among patients with relatively well-controlled diabetes. 38
The distinctive training of GPs equips them to approach care holistically. This is an especially critical attribute in the management of diabetes, where a series of comorbidities can often co-exist. In such cases, GPs do not assume the role of specialists but operate most effectively as collaborators. They can coordinate timely access to various specialties, monitor disease progression, and translate complex clinical information into comprehensible input for patients. Within a well-interconnected system, their presence enhances both the responsiveness and personalization of care.39,40
As is well known, behavioral guidance is a key element in diabetes control. This is an area in which GPs hold a structurally advantageous position. Indeed, they can reinforce long-term lifestyle strategies, tailored to individual needs and evolving circumstances. Furthermore, they play a pivotal role in supporting adherence to treatment through ongoing dialogue, motivational engagement, and sustained follow-up. In addition, GPs often serve as a vital link to broader social support systems, connecting patients to community resources, financial assistance, or psychosocial services. 41
Bridging the divide: Hybrid models of diabetes care
The funding model of a health system markedly influences access to specialist care. In private health care, availability is governed by free market principles, allowing individuals to seek specialist input directly, either out of pocket or through private insurance coverage. In contrast, public and social security-based systems must carefully balance equity, efficiency, and sustainability. Within these frameworks, it is essential to expand the presence of specialists in community settings and reconsider the mandatory referral requirement from general practitioners. Should these changes lead to increased costs, though not necessarily significant, they could be reasonably offset through modest co-payments or optional supplementary insurance contributions. 42 This would help preserve system integrity while offering patients greater choice. Crucially, such interventions must be assessed using robust analyses that link cost to health outcomes, ensuring that reforms remain widely available, economically viable, and clinically justified. 43
Hybrid generalist–specialist models offer a strategic response to the growing demand for specialized care. These approaches can be implemented by establishing multidisciplinary teams within shared clinical settings. Such integrated models are capable of managing complex chronic conditions, such as diabetes and its complications, at a single point of care.
44
By consolidating services that would otherwise be fragmented across multiple providers and institutions, integrated care models enhance continuity, strengthen coordination, and reduce unnecessary duplication.
45
They are also likely to reduce expenses and improve health outcomes.
46
As health systems worldwide grapple with multimorbidity, demographic ageing, rapid technological advancement, and rising expectations, hybrid care models may provide a pragmatic and flexible complement to primary care reform efforts. Figure 1 is a conceptual illustration of the patient’s pathways in gatekeeping and open-access hybrid systems. Nonetheless, hybrid care models may be challenged by workforce shortages, funding constraints, interoperability limitations, and the need for sustained coordination between professionals and institutions. Gatekeeping and open-access systems offer different pathways to specialist care for patients with diabetes.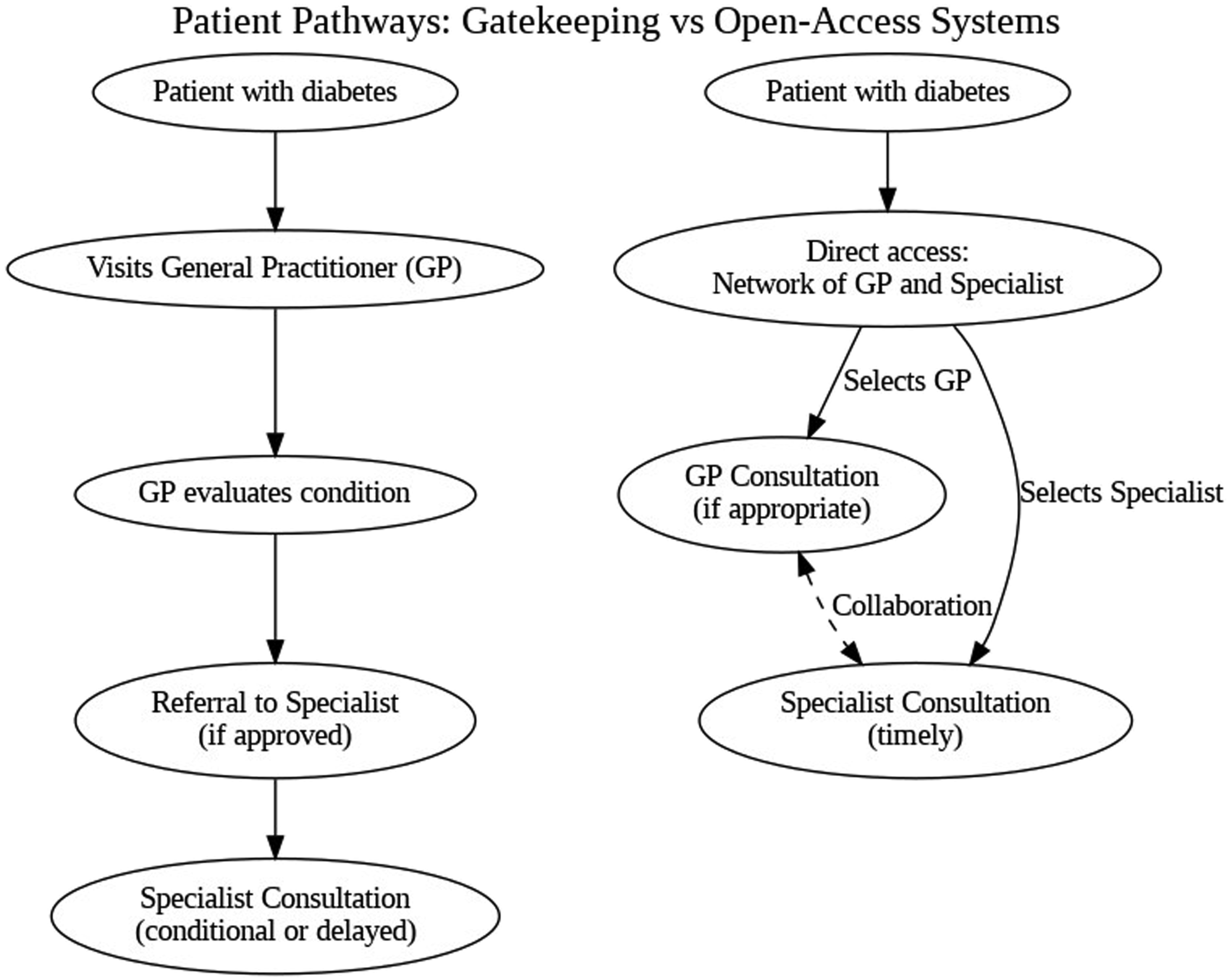
Effective collaboration between generalists and specialists relies on continuous communication and mutual understanding. General practitioners often serve as holistic care coordinators by managing a wide range of patient needs. Specialists contribute vital expertise and support for complex, condition-specific issues. Yet, collaboration is frequently hindered by differing expectations, ambiguous role boundaries, and inconsistent information exchange.
47
Enhancing professional relationships through joint continuous medical education and regular interactions can help overcome these challenges by fostering trust and improving teamwork. This dynamic and relational approach is essential for achieving more integrated, patient-centered care. Figure 2 depicts how a hybrid model of care could theoretically use the complementary strengths of both generalist and specialist-led approaches to provide optimal diabetes management. A hybrid model combines the strengths of generalist and specialist care, delivering a more comprehensive and patient-centered approach to diabetes management.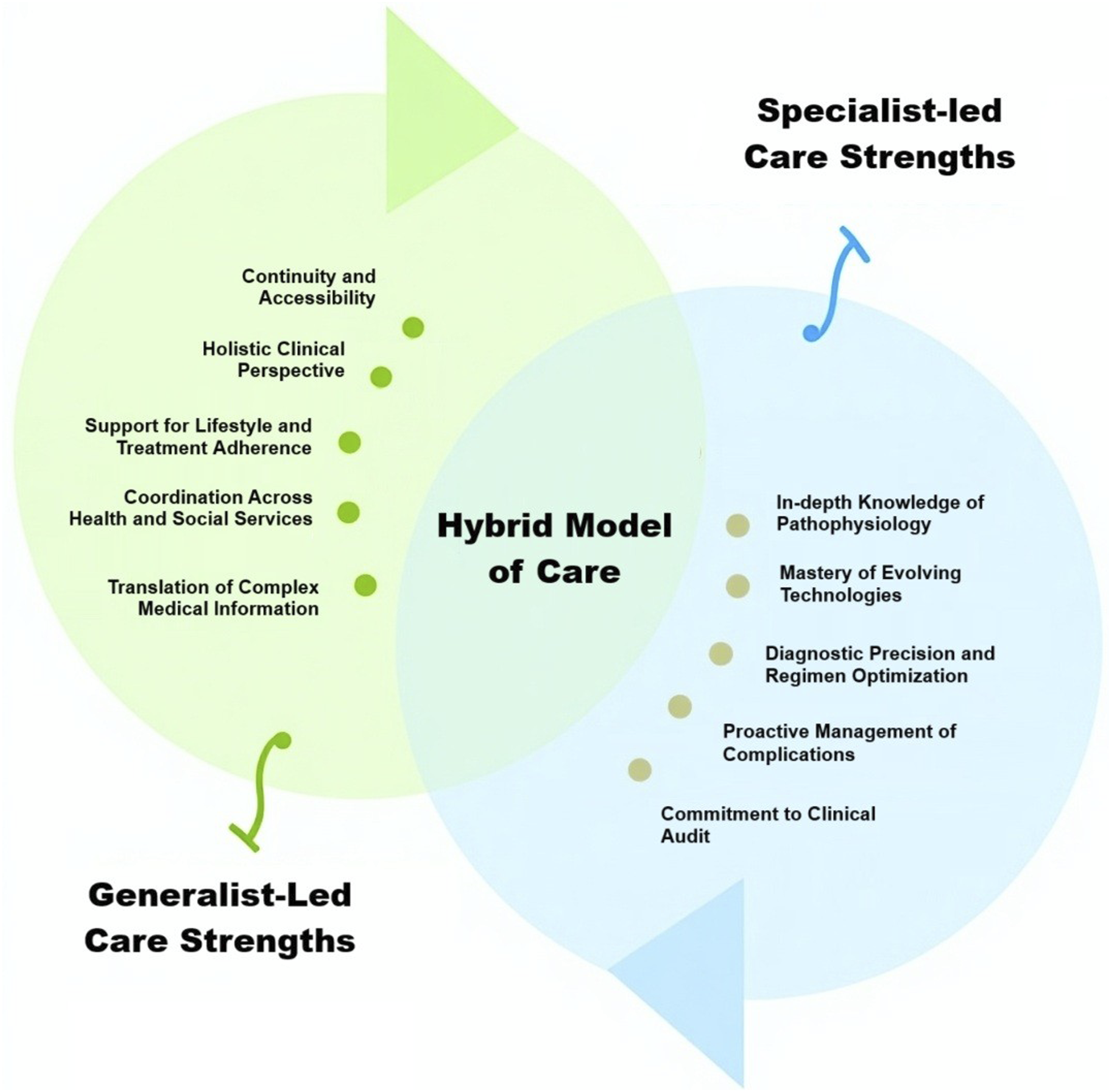
Policy and workforce implications: Aligning intent with capacity
Shifting away from gatekeeping policies to open access to specialist care is indeed a bold and radical deviation from established convention. However, it represents an alignment with the reality of modern scientific and social progress. The intricate landscape of chronic diseases, especially of diabetes, demands a model that prioritizes timely expertise over rigid hierarchies. While once justified in the name of resource allocation, practices that control, and usually limit, access to specialized knowledge are no longer defensible in health systems seeking to expand patient-centered and equitable access to expertise.
That said, structural reform must address pragmatic concerns. In several countries, access to specialists remains uneven, particularly in rural, remote, or economically strained areas. The maldistribution of the specialist workforce, and in some cases, its overall scarcity, demands an insightful response. The implementation of telemedicine can help bridge these gaps by enabling consultations with patients with diabetes, regardless of their physical location. 48 The use of electronic communication technologies has already demonstrated cost-effective benefits in diabetes care, including improved glycemic control, enhanced self-management, and lower rates of hypoglycemic events. 49 Therefore, sustained investment in digital infrastructure and training is essential.
Understandably, concerns regarding the financial implications of such reforms may exist. No one can ignore the potential costs of expanding access to specialist care. Yet, these costs are not inherently unsustainable. Health insurance plans that provide services through a network of specialists and a shift toward value-based funding models can offer a balanced management of resources. 50 Contrary to expectations, open access may not increase expenses to an uncontrollable extent. On the contrary, greater competition among clinicians for posts can moderate remuneration levels. The same dynamic applies to technology. In diabetes care, broader uptake of digital applications can lead to increased market competition, thereby lowering prices and expanding access. Thus, the cost of reform is not synonymous with waste. It is a redirection of investment, away from procedural bottlenecks and toward a model that values precision, access, and justice.
Conclusions and imperatives: Reclaiming quality in diabetes care
In an era of accelerating technological innovation and rising clinical complexity, the expectation for more personalized, expert-driven care is not only reasonable but also inevitable. Responding to this reality does not mean dismantling the foundations of primary care. Rather, it requires a deliberate strengthening through strategic integration with expertise. Embedding specialists, such as endocrinologists and diabetologists, within primary care structures offers a practical and ethically solid response to the challenges of modern diabetes care. Far from overwhelming hospital services, this model enables earlier diagnosis, timelier interventions, and improved continuity. Therefore, health policies must evolve from vague commitments to efficiency toward deliberate calibration of specialist-to-generalist ratios, tailored to the geographical, demographic, and social realities of each country. Only then can health systems truly serve patients with diabetes in a way that is both effective and fair.
Nowadays, patients are no longer passive recipients of care. In a world rich in health information, many individuals are articulate in their preferences and capable of discerning the kind of care they require. In such cases, the gatekeeping function of general practitioners becomes less a safeguard and more an administrative obstacle, an extra step that consumes resources and delays care. After all, a patient-centered system must be grounded in autonomy, not paternalism. While some patients’ requests for specialist care may occasionally reflect misunderstanding or misplaced concern, these instances are rarely disruptive in practice and are tempered by the natural filters of consultation and system logistics. Overregulating access out of fear of misuse reflects a mistrust in patients and burdens the very services those restrictions claim to protect.
Finally, the assumption that specialist-led care is inherently more expensive lacks a credible rationale, particularly in the context of diabetes. The cost of treatment is driven not by the title of the prescribing physician, but by the therapeutic agents used. A diabetes specialist, equipped with focused training, is more likely to tailor regimens effectively, reduce trial-and-error prescribing, and avoid adverse events that ultimately raise costs. Moreover, incorporating specialists into primary care can harmonize costs by reducing duplicative visits, fragmented monitoring, and late-stage complications. Thus, equating the presence of specialists with higher systemic cost overlooks the true sources of inefficiency and ignores the value that expertise can introduce. As Protagoras reasoned: “Πάντων χρημάτων μέτρον ἐστίν ἄνθρωπος” (“Man is the measure of all things”). If we are to reclaim quality in diabetes care, our systems must be measured not by what is cheapest or most convenient, but by what truly serves the patient. Future research should evaluate clinical effectiveness, cost-efficiency, patient satisfaction, and implementation feasibility of hybrid care models across various health systems.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.