
Abstract
Background
School-based iron supplementation is a key national intervention to reduce anaemia among adolescent girls, however evaluation regarding processes is lacking. This study evaluated adherence to iron supplementation and its determinant factors among schoolgirls in Indonesian settings.
Methods
A cross-sectional study was conducted at selected schools in priority areas of East Java (n = 3) and Bali (n = 4) from April-September 2023. A questionnaire administered to approximately 100 girls at each school collected data on the individual factors and adherence. School databases and interviews with 7 health unit staff was used to understand the environmental factors, and content analysis elicited the themes. Binary logistic regression summarised associations of individual and environmental factors contributing to adherence.
Results
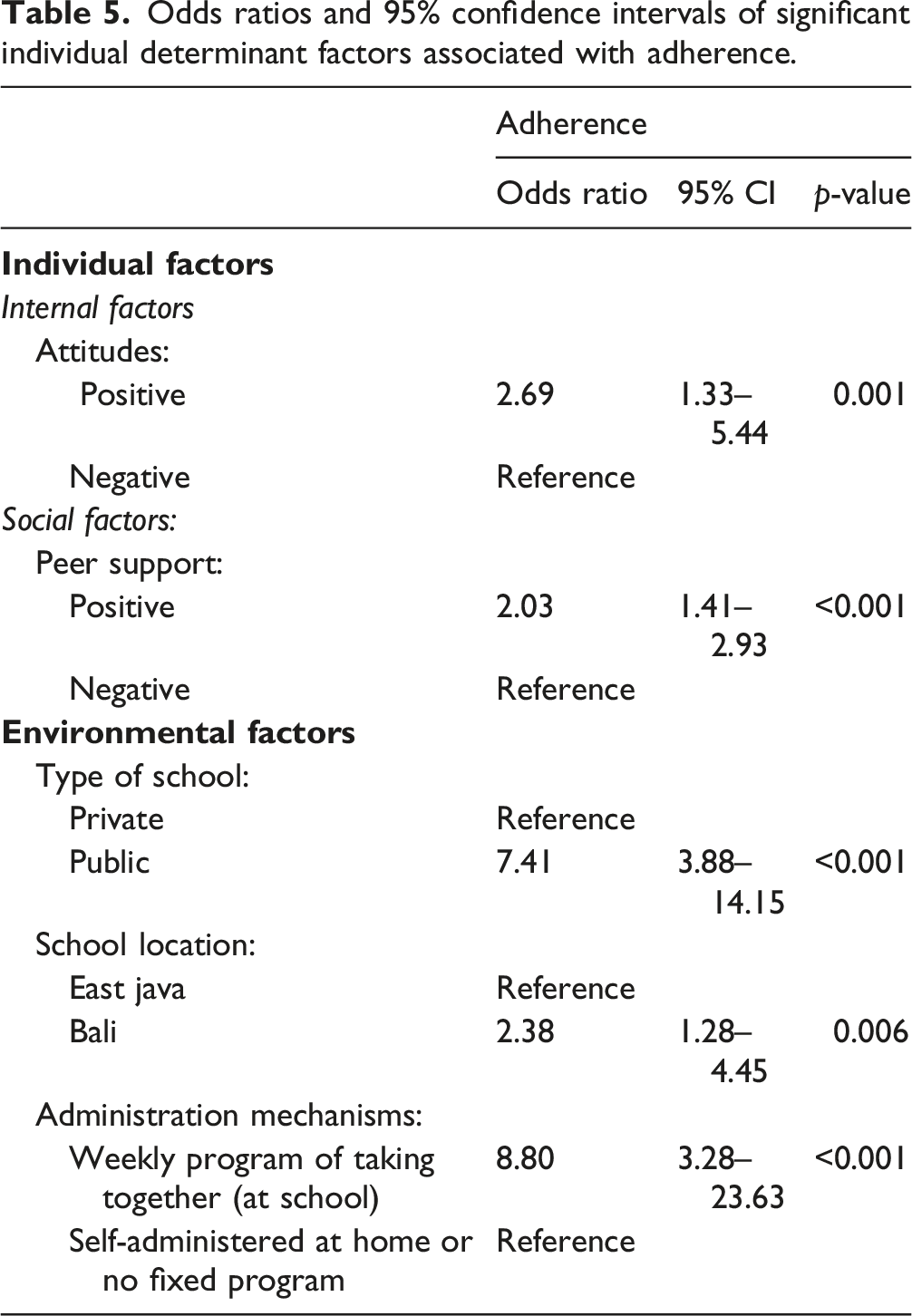
A total of 694 girl respondents reported a mean adherence of 40%. Environmental themes included location (East Java/Bali), type and level of schools (private/public and Junior/Senior High School), iron tablet distribution and administration mechanisms (1-week supply/1-month supply/varied and weekly program at school/self-administered at home/no fixed program). Binary logistic regression confirmed that individual associations (i.e., attitude, Odds Ratio (OR) 2.69; peer support, OR 2.03), and environmental factors (i.e., type of school, OR 7.41; location, OR 2.38; administration mechanisms, OR 8.80) were independently associated with adherence.
Conclusion
Low adherence levels among schoolgirls reported in this study warrants attention. Identified contributing factors provide a basis for the development of strategies to improve adherence to school-based iron supplementation programs in Indonesian settings, particularly at priority areas.
Introduction
Anaemia is a global public health concern and indicates reduced red blood cells and therefore lower than normal haemoglobin concentrations. 1 In 2019, anaemia affected 29.9% in women of reproductive age (15–49 years of age), in which menstruating adolescent girls were among the most vulnerable groups. 1 Anaemia in adolescent girls has negative consequences on school performance, productivity, and current and future reproductive health; they have a higher risk of becoming anaemic women of childbearing age. Infants born to anaemic mothers are associated with increased risks of stunting and perinatal mortality.2,3 Efforts has been made to meet the World Health Assembly’s target of a 50% reduction in anemia in women of reproductive age (aged 15–49 years) by 2025. 4 A key action recommended by the World Health Organization (WHO) is increasing consumption of certain micronutrients, including but not limited to iron and folic acid. 5 Intermittent iron and folic acid supplementation (administered at least once weekly for 3 months, twice yearly, or after the school semester) is recommended in settings where anaemia prevalence in women of reproductive age indicates a public health concern (anaemia >20%). 6
Indonesia is among the top-10 highest prevalence countries for anaemia in South East Asia, 1 and the latest Indonesian Health Survey in 2023 reported that 15.5% of adolescents were anaemic.7,8 In accordance with the WHO recommendation, the Indonesian Government has introduced iron supplementation (which consists of 60 mg elemental iron and 0.4 mg folic acid) for adolescent girls as a national nutritional intervention since 2014. 9 Further, arrangements specified in the Ministry of Health circulatory letter recommends once weekly supplementation for the whole school year. The program is targeted at girls 12–18 years of age, and is distributed via the School Health Unit [Unit Kesehatan Sekolah/Madrasah (UKS/M)] at junior/senior high school levels, and provided free of charge. It was suggested to assign ‘1 day of taking iron supplementation together’ each week based on an agreement with local stakeholders. 10
One key indicator established by the Indonesian Government to evaluate the effectiveness of the school-based iron supplementation program was adherence, particularly since haemoglobin tests have not always been possible due to limited local budgets. Previous Indonesian studies have reported that adherence rates vary significantly across areas, such as East Kalimantan (1.4%), Jakarta, West Java (45.6%) and Yogyakarta, Central Java (62.1%).11–13 Adherence is acknowledged as a multifactorial phenomenon which can be influenced by many factors. 14 A recent systematic review, which included 20 international studies (i.e., India, Indonesia, Iran, Ghana, Ethiopia and Burkina Faso), has classified determinants of adherence to iron supplementation among adolescent girls into four general categories: 1) personal; 2) social; 3) environmental; and 4) regimen/drug factors. 15 However, this review included only one Indonesian study which indicated issues with regimen [i.e., unpleasant taste and smell (p < 0.01), experiencing side effects (nausea) (p = 0.02)], personal factors [i.e., forgetfulness (p = 0.04)], and social factors [i.e., lack of peer support (p = 0.03)]. 15 Further exploration is required to understand the issues of adherence among schoolgirls, particularly in variious priority settings with high prevalence levels of anaemia and/or stunted children.
This study aims to evaluate adherence to iron supplementation and its determinant factors among adolescent schoolgirls in priority areas in East Java and Bali Provinces, Indonesia. Findings of this study should provide evidence-based information for stakeholders to design strategies for sub-national and national scale-up programs of iron supplementation, as well as information on the school-base modality of iron supplementation, particularly in priority settings with high prevalence of anaemia and/or stunted children.
Method
A cross-sectional study in priority areas in Indonesia was conducted. The data collection instrument and methodology used in this study were approved by the Ethics Committee of University of Surabaya (Number 154/KE/VI/2023), and this study granted official permission from the local health offices and related schools as the research settings.
Study settings
This study was conducted in East Java and Bali Provinces. East Java Province has the second largest economy in Indonesia which is dominated by industrial operations, and most of the population is Muslim. 16 While Bali Province has been dominated by tourism with >80% of the population Hindu. 17 No complete data-set of anaemia prevalence of adolescents across areas in East Java and Bali was available, hence two areas in East Java (i.e., PA and BU) and one area in Bali (i.e., DP) were selected by the provincial health offices' staff since those areas were considered stunting priority areas, and therefore iron supplementation priority areas. Further, the same staff selected three schools in East Java [i.e., one private and one public JHS (in PA area), and one public JHS (in BU area)], and four schools in Bali [i.e., one private and one public junior high school (JHS), and one public and one private senior high school (SHS) in DP area] as the research settings. The selection was based on the available data on schools provided with iron supplementation supply within the last 6 months and had high anaemic cases (>50%) based on the random haemoglobin tests or physical checks (e.g., pallor) in the first trimester of 2023 – it should be noted that these data were not available for all schools in those areas.
Data collection
Individual factors and adherence
A questionnaire was developed to collect data on individual factors and adherence among schoolgirls based on current literature.18–24 The questionnaire was face-validated with an expert panel with one pharmacy practice expert, one public health expert, and 1 health policy expert to ensure the questions addressed the study objectives. Most of the questions were closed-ended questions with binary formats as limited time was available to complete the questionnaire during class (approximately 20 min); literature suggested that binary formats were easier to understand and involved less time and costs.
25
The final questionnaire consisted of three sections (Sections A-C) as Supplementary Material available only on-line. (1) Section A: “Participant characteristics”, including age. (2) Section B: “Individual Factors” included: • Internal factors, including: - Knowledge (20 True/False questions): for each question, one point was given for the correct answer, and 0 point was given for the wrong answer. The total score of the correct answers from each participant was calculated, and converted to a percentage [i.e., total score/20 (maximum score) x 100%].21–23 - Attitude (16 Agree/Disagree statements): the positive statements were scored 0 point for ‘Disagree’, and one point for ‘Agree’, while reversed scores were applied for negative statements. The total score from all questions was calculated for each participant, and converted to a percentage [i.e., total score/16 (maximum score) x 100%].21–23 - Other (an open-ended question). • Drug factors, including: side effects (6 Yes/No questions of common side effects, such as nausea, vomiting, abdominal pain); organoleptic issues (3 Yes/No questions for issues with taste, odour, and/or colour; and other (an open-ended question) • Social factors, i.e., social support experienced by adolescents to improve compliance of iron supplementation, including: family support (13 Yes/No statements), peer support (10 Yes/No statements), and school representative support (5 Yes/No statements). For each statement, one point was given for ‘Yes’, and 0 was given for ‘No’. The sum of points was calculated for all statements, and converted to a percentage [i.e., total score/maximum score x 100%]. (3) Section C: “Adherence” was assessed using a Yes/No question: “Have you regularly taken iron tablets (i.e., one tablet per week) over the last 3 months?”
The questionnaire was piloted with 30 adolescent girls in a school other than the research settings. Cronbach’s alpha values for internal consistency for knowledge (α = 0.836), attitudes (α = 0.842), family support (α = 0.770), school representative support (α = 0.724), and peer support (α = 0.730); all of which were considered acceptable (>0.7). 26
Population sampling frames of adolescent girls at the research setting schools.

Abbreviations: JHS, junior high school; SHS, senior high school.
The girls were invited at a face-to-face session arranged by the school, and their parents/guardians were informed about the nature of the study via a school announcement by the researchers (NL,CH, LPS). Parental/guardian consents were obtained from all adolescent girls under 18 years of age. Those who provided consent were asked to complete the questionnaire; this process was assisted by two data collectors who read the questions and asked the students to write down their individual responses to the questionnaire sheets. The data collectors attended a briefing session and simulations until they could perform the data collection functions without errors.
Environmental factors
Environmental factors of the schools included location, type/level of schools, and iron tablet distribution and administration mechanisms. School databases were used to confirm information on the location (i.e., East Java/Bali Provinces), and type and level of the school (i.e., private/public and JHS/SHS); while face-to-face interviews with seven school health unit staff (i.e., one staff per school) – as the person in charge of iron supplementation programs – were used to inform the distribution and administration mechanisms. Whilst the government has provided a general guideline for iron tablet supplementation at schools, no specific guideline was available at these schools; hence, distribution and administration of iron tablets was arranged by the health unit staff based on the resources available at each school. The interviews used a semi-structured interview guide to explore two key topics, i.e., the distribution and administration of iron tablets. It should be noted that the seven schools included in this study had received iron supplementation supply within the last 6 months, so issues of environmental factors related to the availability/supply were not relevant.
The interviews were performed by the researchers (NL, CH, LPS) who were Bachelor/Master of Pharmacy students and trained to conduct the interviews. Prior to the interview, the staff were informed about the study, and asked to complete a written informed consent if they agreed to participate. The interviews were conducted in the school health unit over 15–20 min, and were audio-recorded. The data collection occurred from April to September 2023.
Data analysis
Individual factors and adherence
IBM SPSS Statistics version 25.0 (IBM Corp, Armonk, NY, USA) was used for data analysis. Responses from the questionnaires administered to the schoolgirls were summarised using descriptive analysis; the detailed analysis were as follows: (1) Section A: “Participant characteristics” related to the age was presented as mean ± standard deviation. (2) Section B: “Individual Factors” • Internal factors − Knowledge (20 True/False questions): The total score which was converted into percentage was categorised into “low” (≤55%), “moderate” (>55-≤75%), or “good” (75-100%).21–23 Then, the absolute and relative (%) frequencies of participants in each category were presented. − Attitude (16 statements of Agree/Disagree statements): The total score which was converted into percentage was categorised into “negative” (percentage of agreement ≤50%) or “positive” (percentage of agreement >50%).21–23 The absolute and relative (%) frequencies of participants in each category were presented. − The open-ended question was analysed using content analysis.26,27 The responses were coded by the researchers (NL, CH, LPS). If there was a disagreement, a discussion with the research team was carried out to reach a consensus about the code. The frequencies and percentages of the codes were then calculated. • Drug factors − The absolute and relative (%) frequencies of participants who provided responses ‘Yes’ or ‘No’ related to side effects and organoleptic issues were presented. − The open question was analysed using content analysis.
28
• Social factors, including: − A total score of family support (13 Yes/No statements), peer support (5 Yes/No statements) and school support (3 Yes/No statements) were calculated and converted into percentages; this was then categorised into “low support” (≤50% agreement) and “high support” (>50% agreement). The absolute and relative (%) frequencies of participants in each category were presented. (3) Section C: “Adherence” (a Yes/No question) was analysed using the absolute number and relative (%) frequencies of participants provided responses ‘Yes’ (adherence) or ‘No’ (non-adherence). All calculations were done for each student, and their cohort in each setting as well as for the total.
Environmental factors
School databases were used to confirm themes of the locations and type/level of the schools. Data from the interviews with school health unit staff were analysed using content analysis to inform iron tablet distribution and administration mechanisms. The analysis initially involved verbatim transcription of the interviews and data familiarization; significant statements were then identified and coded. 28 The process of coding was conducted manually by cutting and pasting between transcript documents. The initial coding was performed by NL, CH, LPS, and the emerging themes related to iron tablet distribution and administration mechanisms were discussed with the research team to reach a consensus. Finally, examples of responses were selected to illustrate each theme. Data analysis was conducted using the Indonesian language ‘Bahasa’ (as the language used during the interviews); the illustrative verbatim quotes and themes were then translated into English by an academic with competent English language skills. Member-checking was used to enhance trustworthiness. 28
Factors contributing to adherence
Univariate analysis with chi-square was used to test the association of each environmental factor or individual factor as the dependent variable with adherence as the independent variable (i.e., a Yes/No binary variable). For the analysis, environmental factors were quantified by calculating numbers of schoolgirls from schools having the same theme (e.g., schools implementing a 1-week supply distribution mechanism). Statistically significant factors were entered into the model binary logistic regression. Odds ratio (OR) together with 95% confidence intervals (CI) more than one and p-value less than 0.05 indicated a statistically significant association.
Results
Environmental factors
Location and type/level of schools
Themes on the environmental factors of the schools.
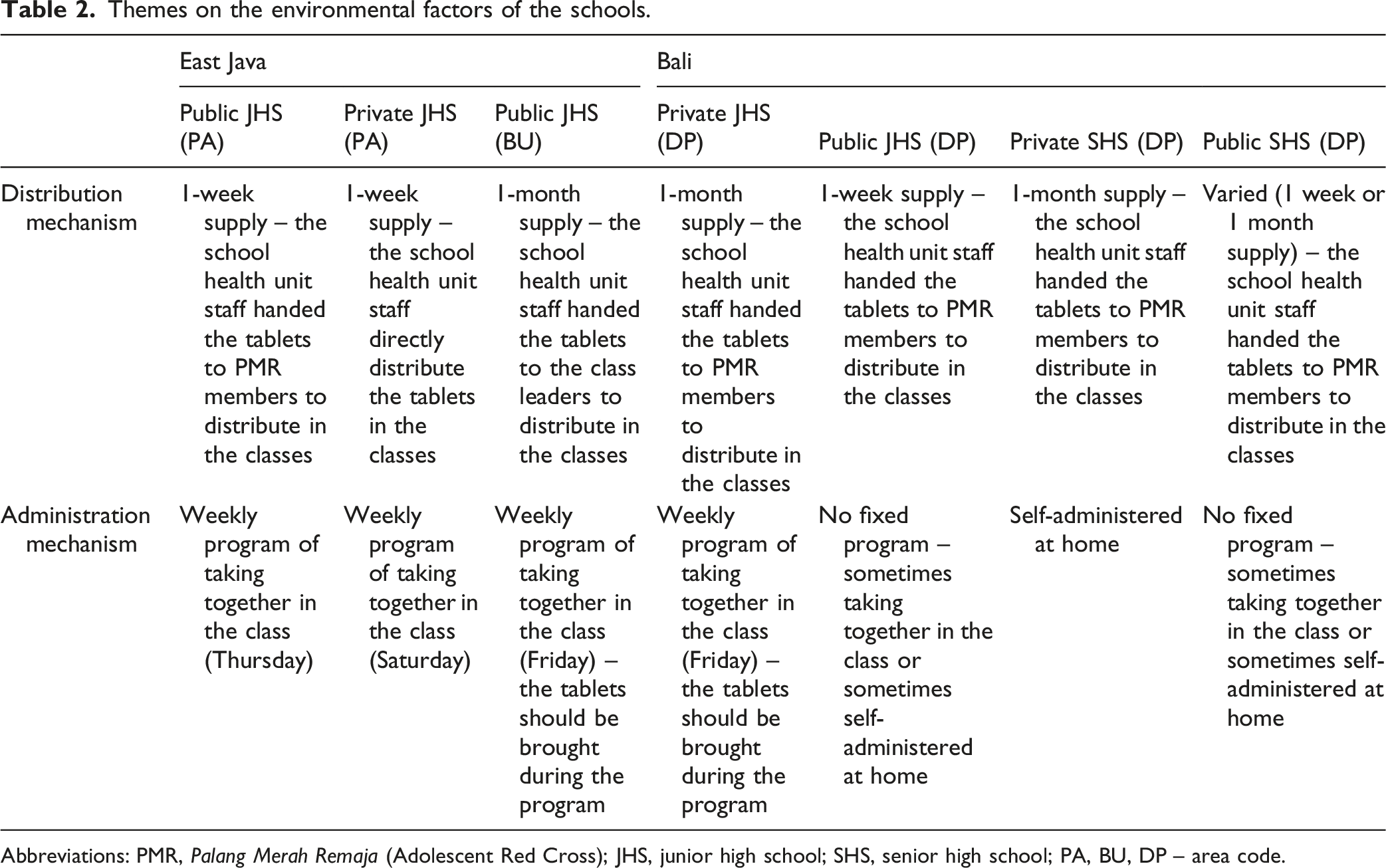
Abbreviations: PMR, Palang Merah Remaja (Adolescent Red Cross); JHS, junior high school; SHS, senior high school; PA, BU, DP – area code.
Distribution mechanisms
Themes emerging for the iron tablet distribution and administration mechanisms were summarised in Table 2; the data achieved saturation. It was reported that all seven schools had their iron tablets supplied from Puskesmas (i.e., a public primary health facility in the district level). The quantity of iron tablets supplied was based on the number of girls in the school; the supply period provided varied between 6 months to 1 year. The iron tablets were delivered to the school health unit staff-member employed as the person in charge of the iron supplementation program.
Whilst the government has provided a general guideline for iron tablet supplementation at schools, no specific guideline was available at these schools. Distribution was arranged by the health unit staff based on the resources available at each school. The staff had either distributed the tablets himself/herself (n = 1 school), or supervised the distribution via a member of Adolescent Red Cross (Palang Merah Remaja, PMR – i.e., a forum for adolescent activities at school which is under the Indonesian Red Cross) (n = 5 schools) or the class leader (i.e., a student appointed as the class representative) (n = 1 school). The tablets were distributed either as 1-week supply (n = 3 schools), or 1-month supply (n = 3 schools) or varied (1-week or 1-month supply, n = 1 school) (Table 2).
Administration mechanisms
Two schools with a 1-week supply followed with a weekly administration process in the class (Table 2). However, ensuring all the girls were present and taking the tablets was identified as a problem; as stated by the staff at the Public JHS (PA area): “Then (the supply was) followed with a program of taking together every Thursday. Though, it is hard to know whether everyone really takes it.” The third school with 1-week supply and the school with varied supply reported no fixed program for iron tablet administration, as reported by the staff at the Public SHS (DP area):“We actually arrange to have a program of taking together every Friday, but sometimes the tablets were taken home, as there is no fixed program yet.”
From 3 schools with 1-month supply, two schools adopted weekly administration. Thus, the tablets should be brought every week during the administration program, which increased the risk of forgetting, as reported by the staff at Private JHS (DP area): “(We have) a program of taking together every Friday… for students who forget to bring their tablets, they would be asked to self-administer at home, thus no assistance provided.” While the third school with 1-month supply asked the students to self-administer the tablet at home due to the time constraints, as stated by the staff at the Private SHS (DP area): “It is not possible to arrange a taking together program due to the busy schedules of the girls, so they were asked to self-administer the tablet at home.
Individual factors
Individual factors and adherence to iron supplementation among schoolgirls.
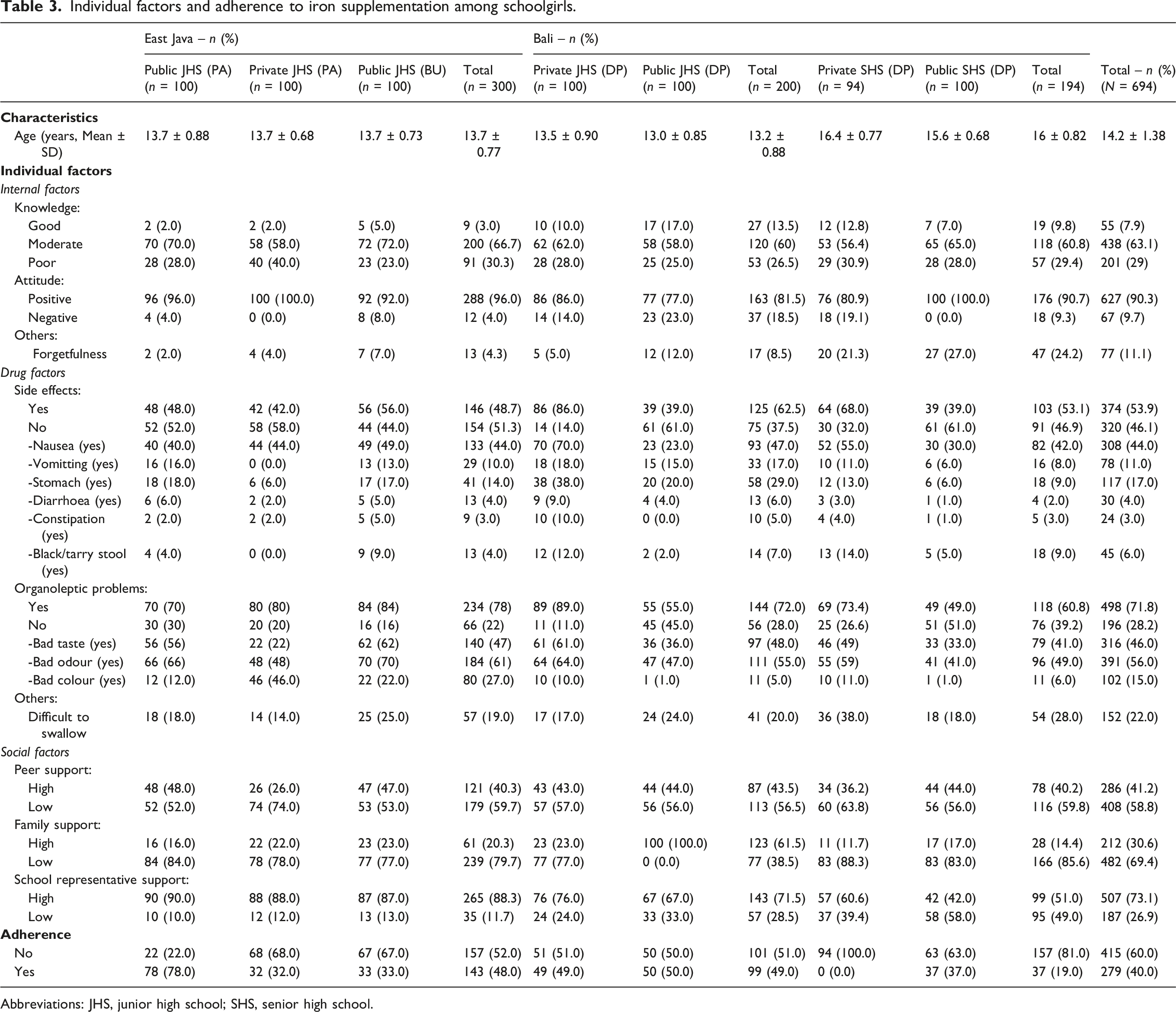
Abbreviations: JHS, junior high school; SHS, senior high school.
Internal factors – less than 10% of adolescent girls had good knowledge regarding iron supplementation, those from public and private JHS (BU area, East Java) had the lowest percentages (2% and 2%, respectively). On the contrary, approximately 90% of the girls across schools had positive attitudes toward the school-based iron supplementation program.
Drug factors – approximately half of the participating girls across schools reported an experience with adverse effects, particularly nausea. Moreover, more than 70% of the girls also indicated issues with organoleptic properties of the iron tablet, particularly in relation with its taste and odour. In addition, approximately 20% of the girls reported other problems, especially difficulty in swallowing the tablet.
Social factors – The majority of girls reported positive support from school representatives, particularly those from JHS (>65%). On the contrary, only approximately 40% of girls across schools have had positive support from their peers; and even less support was indicated from their families (<30%), except those from public JHS in Bali (100%).
Adherence and the determinant factors
The level of adherence among adolescent girls to iron supplementation in the last 3 months varied across schools where girls from SHS in Bali generally had lower adherence (19%). A better adherence of approximately 50% was reported across JHS in Bali as well as East Java.
Univariate analysis between each determinant factor versus adherence (N = 694).
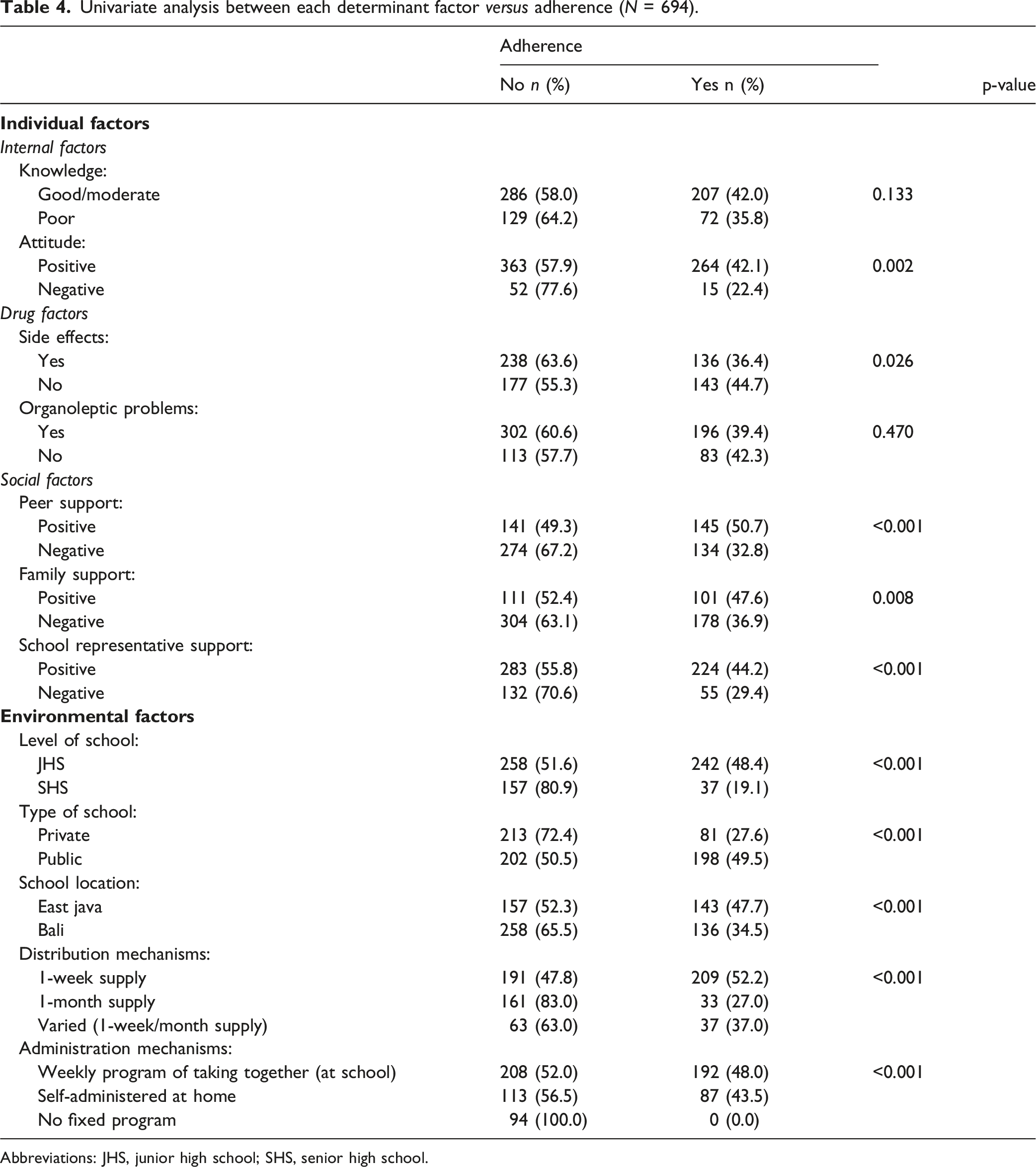
Abbreviations: JHS, junior high school; SHS, senior high school.
Odds ratios and 95% confidence intervals of significant individual determinant factors associated with adherence.
Discussion
This study has provided insights regarding important aspects of school-based iron supplementation programs at selected schools in Indonesia, specifically located in the known stunted priority areas in East Java and Bali Provinces. The levels of adherence to iron administration – as one key indicator of the program – varied across schools, but was overall suboptimal with an average of 40%. Suboptimal levels of adherence were also reported in previous Indonesian studies (1.4% - 62.1%);11–13 while international studies in certain African and Indian regions reported varied levels of adherence (14.5% - 92.3%). 15 Low levels of adherence among schoolgirls warrants attention since adherence to iron supplementation is suggested to be positively associated with serum haemoglobin concentration and negatively associated with anaemia. 29 Systematic reviews conducted in 2016 and in 2017 reported that iron supplementation significantly reduced anaemia by 33% and 27% among adolescents (mostly girls), respectively.30,31 Hence, this study highlighted the importance to optimise processes of school-based iron supplementation to improve adherence, particularly in priority settings.
This present study has indicated that environmental factors (related to the contexts of the schools) have demonstrated significant associations with adherence to iron supplementation, including locations (i.e., East Java), type of schools (i.e., public schools) and administration mechanisms (i.e., weekly program of taking together). The effectiveness of a weekly program of taking together (at the school classroom) was also evidenced in a prior Indonesian study in Jakarta, West Java. 11 While this present study indicated that not all schools have implemented a weekly program of taking iron tablets together, broadening the uptake of that program warrants consideration; particular attention should be given to private schools. Unlike public schools, private schools are funded/operated by private sectors and enjoy significant autonomy, 32 thus strengthening the implementation of the government’s iron supplementation program, would be essential in these settings.
In general, this study reported lower associations to adherence for individual factors (i.e., social factors, internal, and drug factors) compared to the environmental factors. Social factors related to peer support and was found as a significant predictor. In parallel, prior research in Gujarat, India reported that involving peer educators (under a voluntary organisation) in community-based weekly iron supplementation programs showed promising results in improving adolescent adherence. 33 Peer educator activities also were reported to be able to improve adolescents’ attitudes, normative beliefs, subjective norms, and perceptions of behavioral control in factors relating to prevention of illicit substance abuse. 34 However, the influence of social factors seems to be different across settings; a systematic review included studies reported a range of social support can influence adherence to iron supplementation, either from teachers,35–37 parents,37,38 family, 13 or peers.13,37,38 While this study reported no significant association of family and school representative support to adolescent adherence, further exploration would be required to determine whether support or training are required to enhance their roles in the iron supplementation program.
With regards to the internal factors among adolescent schoolgirls, this present study reported that attitudes have significant associations with adherence; however, no significant association was reported between knowledge and adherence. In contrast, prior international studies have reported knowledge (related anaemia, posistive effects/benefits of iron tablets, iron deficiency issues) can influence adherence.35,36,39,40 Whilst it is generally acknowleged that better knowledge will lead to improved attitudes and practice;41,42 in this study, only a small percentage of the girls had good knowledge, but most of them reported positive attitudes. This might be due to the girls’ familiarity with the iron supplementation program (as part of the national program which has been implemented via their schools), however a lack of information or insufficient attention to the relevant knowledge may be factors for further exploration.
This study has some limitations. This study specifically evaluated profiles of adherence among adolescent girls at selected schools in East Java and Bali; thus, some caution should be exercised in generalising these results. However, this study included a range of schools’ characteristics which can provide insights to the broader Indonesian school context. In addition, it should be noted that some self-reported data could be biased when participants could not accurately recall the information asked (recall bias). However, the questionnaire in this study was designed to include information regarding participants’ behaviour in taking iron supplementation over a short period of time, i.e., in the last 3 months, hence issues with recall bias might be minimal. The use of binary formats in this questionnaire forced respondents with an opinion in the middle to transform to an extreme answer, resulting in a higher tendency to agree. However, the use of predictive wording (i.e., refer to what one should do, what is right or wrong, or good or bad) in this questionnaire might help the accuracy of the binary format in providing directions of answers. 25
Conclusion
School-based iron supplementation programs in some priority areas in East Java and Bali were sub-optimal, thus requiring additional attention, especially by school health unit staff. Strategies related to environment aspects of the school, in particular implementing a weekly program of taking the iron tablet (directly after being distributed at the school), paying more attention to the private schools, as well as improving peer support, might be considered for a successful implementation of school-based iron supplementation program in priority areas in the low-resource countries. The impacts of the program on the health outcomes beyond adherence, such as in reducing the prevalence of anaemia and child stunting, warrants further long-term exploration.
Supplemental Material
Supplemental material - Evaluation of school-based iron supplementation adherence and determinant factors among adolescent girls in Indonesian settings
Supplemental material for Evaluation of school-based iron supplementation adherence and determinant factors among adolescent girls in Indonesian settings by Adji Prayitno Setiadi, I Gusti Agung Ari Kusuma Yana, Gusti Ayu Putu Laksmi Puspa Sari, Catherina Hutahaean, Ni Nyoman Laila Nordewi Yani, Susilo Ari Wardhani, Bruce Sunderland and Yosi Irawati Wibowo in Community Health Equity Research & Policy
Footnotes
Acknowledgments
We would like to thank the East Java Provincial Health Office, and the participating schools which hosted the survey as well as their staff and students who supported in the data collection.
ORCID iDs
Ethical considerations
The data collection instrument and methodology used in this study were approved by the Ethics Committee of University of Surabaya, Indonesia (Number 154/KE/VI/2023), and this study granted official permissions from the local health offices and related schools as the research settings. Parents/guardians were informed about the nature of the study via school announcement and were given opportunity to provide written informed consents for their adolescent girls to participate.
Authors’ contributions
APS: methodology, formal analysis, conceptualitation, writing-original draft preparation. YIW: methodology, writing – reviewing and editing. AKY, LPS, CH, LNY: investigation, formal analysis, data curation. SAW: methodology, validation. BS: conceptualisation, writing- reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, YIW, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.