
Abstract
Introduction
Malignant brain tumors are the second most common malignancy diagnosed in children, with a prevalence rate of 22.31/100,000 (Zhang et al., 2017). Physical symptoms related to having a brain tumor include headache, nausea, blurred vision, seizures, and fatigue (Packer et al., 2003), some of which may be exacerbated by treatment. In addition to surgical resection and chemotherapy, craniospinal irradiation (CSI) is an effective therapy for reducing the recurrence of particularly aggressive tumors and preventing dissemination within the cerebrospinal fluid (CSF). Therefore, CSI is typically used in the treatment of medulloblastoma, primitive neuroectodermal tumor (PNET), germ cell tumors, and other tumors that show evidence of CSF dissemination. However, CSI is associated with numerous acute toxicities, including fatigue (Suneja et al., 2013), which may significantly impact the quality of life for children undergoing treatment (Kuhlthau et al., 2012). In fact, cancer treatment is associated with highly distressing fatigue in 70% to 100% of patients (Mock et al., 2007). While it is well established that cancer patients experience fatigue, our study is among the first to characterize on-therapy fatigue in pediatric brain tumor survivors by using the longitudinal assessments of fatigue.
Fatigue, which is a subjective experience that manifests as physical, emotional, or cognitive exhaustion, adversely affects an individual's daily functioning and may negatively impact treatment efficacy (Berger et al., 2015; Efficace et al., 2015; Groenvold et al., 2007; Stauder et al., 2013; Suzuki et al., 2018). Previous studies have reported that survivors of pediatric brain tumor experience elevated levels of fatigue in the years following therapy completion (e.g., > 2 years off therapy; Armstrong et al., 2010; de Ruiter et al., 2016; Meeske et al., 2004, 2007; Mulrooney et al., 2008; Pelletier et al., 2002; Puhr et al., 2018), but less is known about fatigue prior to or during radiotherapy among pediatric patients with brain tumors. It is important to investigate fatigue not only following radiotherapy but also prior to and during radiotherapy to understand the pathophysiology of fatigue in this vulnerable population. Moreover, recent advancements in radiotherapy, including proton beam radiotherapy, may result in less sequelae by more precisely delivering radiation doses to the tumor. However, no studies have systematically compared severity of fatigue prior to and during therapy among pediatric patients with brain tumor treated with proton beam radiation (PBRT) or photon radiation (XRT). Therefore, the primary objective of this study was to evaluate the longitudinal course of fatigue in newly diagnosed pediatric patients with brain tumors undergoing CSI. We also describe preliminary analyses examining fatigue as a function of radiotherapy modality (XRT vs. PBRT).
Methods
This study was developed to systematically and prospectively evaluate patient-reported symptoms, including fatigue, and neurocognitive performance in pediatric patients with brain tumors across the state of Texas. Briefly, patients with central nervous system (CNS) tumors diagnosed between 2014 and 2016 were recruited from five participating sites across the state of Texas: Texas Children's Cancer Center (Houston, TX), MD Anderson Cancer Center (Houston, TX), UT Southwestern Medical Center (Dallas, TX), UT Health Science Center at San Antonio (San Antonio, TX), and Austin Cancer Center (Austin, TX). Eligible patients were between the ages of 3 and 18 years at diagnosis, underwent cranial radiotherapy, received CSI, and had Spanish- or English-speaking caregivers. Patient clinical, treatment, and demographic data were abstracted from electronic medical records. The study was approved by Institutional Review Boards at each participating institution.
Symptoms of fatigue were evaluated prior to radiotherapy and weekly through the end of radiotherapy using the caregiver-completed Parent Fatigue Scale (PFS), a validated instrument designed for use in pediatric cancer populations (Hockenberry et al., 2003). The instrument was provided in-person to the caregiver during their appointment. The PFS is a 17-item questionnaire designed to assess fatigue severity based on Likert scale ratings ranging from 0 to 4 (“Not at all”–“Always”), with higher scores representing greater fatigue. All questions reflected the child's behaviors and feeling during the previous 72 hours. Based on published thresholds (Hockenberry et al., 2003) and unpublished recommendations from one of the developers of the instrument (Dr. Marilyn Hockenberry, Texas Children's Hospital), a fatigue score ≥ 41 was used to define severe fatigue, while scores between 23 and 40 were classified as moderate fatigue and scores ≤ 22 were classified as none–mild. Given that validated self-reported fatigue instruments were not available for the majority of the patients in our sample (i.e., children younger than 8 years old; n = 17) and the increased instances of missing data among the self-reported outcomes, only parent-proxy reports were included in the analysis.
Descriptive statistics, including counts and percent of the total for categorical variables, and means and standard deviations (SDs) for continuous variables were estimated for the entire cohort, as well as PBRT and XRT subgroups. The mean PFS fatigue rating and corresponding 95% confidence interval (CI) were calculated for each time point. Univariate linear regression, as well as t-tests, fisher's exact test, and chi square tests were conducted to evaluate the association between fatigue at each of the seven assessments (pre-radiation and weekly for 6 weeks) and relevant clinical and demographic factors, including radiation modality, age at diagnosis, age at radiation, preconditions, type of brain tumor, CSI administration dose, prior chemotherapy, prior surgery, or the presence of hydrocephalus at diagnosis. Factors associated with fatigue (p < .20) at one or more time points in univariate models were simultaneously evaluated using a backward stepwise approach in separate multivariable linear regression models for each time point until only variables associated with fatigue (p < .20) at one or more time points in multivariable models remained. All statistical analyses were conducted in Stata version 15 (Stata Corp, College Station, TX).
Results
Overall, 37 eligible children with pediatric brain tumors and their primary caregivers were enrolled. Four individuals were lost to follow-up and did not complete fatigue measures, resulting in 33 eligible and evaluable children with caregivers that completed the PFS (Table 1) prior to radiotherapy and at least once during active therapy. Caregivers were English (n = 29) or Spanish-speaking (n = 4) and provided proxy reports of fatigue for pediatric patients treated with PBRT (n = 26) or XRT (n = 7) who were diagnosed with medulloblastoma (n = 23), PNET (n = 2), ependymoma (n = 2), germ cell tumor (n = 1), pineoblastoma (n = 1), atypical teratoid rhabdoid tumor (n = 1), or other unspecified tumors (n = 3). The median age at diagnosis of participants was 8.14 years (range: 2.43–16.37) with a median age at start of radiation therapy of 8.26 years (range: 3.05–16.41). The median number of days from surgery to radiation was 35 days, with a range of 23–511 days. Three patients (9%) required two surgeries prior to radiation therapy, with all remaining patients requiring a single surgery. The median CSI administration dose for the combined cohort was 36.0 Gy, with similar doses between PBRT and XRT groups (p = .410). Patients were mostly male (57.6%), non-Hispanic White (45.5%), had not received chemotherapy prior to radiotherapy (83.3%), underwent total/near total resection surgery prior to radiotherapy (69.7%), and displayed hydrocephalus at diagnosis (65.5%).
Demographic and Clinical Variables for Pediatric Patients Brain Tumors.
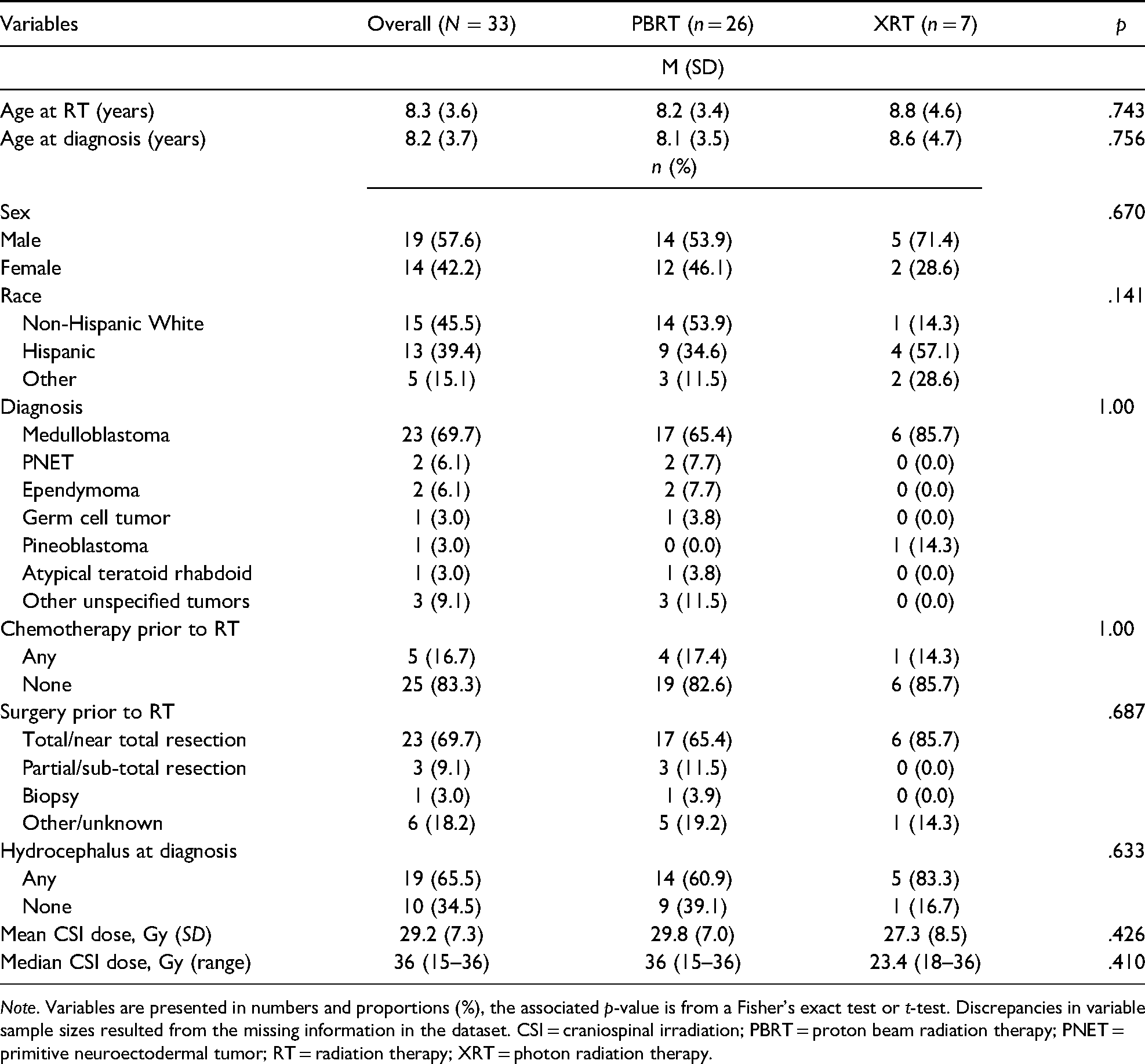
Note. Variables are presented in numbers and proportions (%), the associated p-value is from a Fisher's exact test or t-test. Discrepancies in variable sample sizes resulted from the missing information in the dataset. CSI = craniospinal irradiation; PBRT = proton beam radiation therapy; PNET = primitive neuroectodermal tumor; RT = radiation therapy; XRT = photon radiation therapy.
Fatigue surveys, via caregiver proxy report, were completed a median of 6.5 days (range: 0–20 days) prior to radiation therapy, and weekly following the initiation of radiation therapy. Of the eligible participants who completed pre-radiation fatigue assessment (N = 33), surveys were obtained on 54.4% (n = 18) one week into radiotherapy, 72.7% (n = 24) at two weeks, 84.4% (n = 28) at three weeks, 84.4% (n = 28) at four weeks, 87.9% (n = 29) at five weeks, and 87.9% (n = 29) post-radiotherapy. Of the 33 evaluable participants, 29 provided parent-reported fatigue measures during radiation therapy. Overall, 33.3% (n = 11) completed all seven of the assessments, 30.0% (n = 10) completed six of seven assessments, 21.2% (n = 7) completed five of seven assessments, 9.1% (n = 3) completed four of seven assessments, 3.0% (n = 1) completed three of seven assessments (n = 1), and 3.0% (n = 1) completed two of seven assessments. All statistical models were adjusted to account for missing data. Symptoms of fatigue were prevalent prior to, during, and at end of radiotherapy. Overall, 66.7% of the patient caregivers reported severe fatigue (22/33) prior to radiotherapy, with an additional 27.3% (9/33) reporting moderate fatigue. Severe fatigue was reported by most participants via caregiver proxy report: 66.7% (22/33) prior to radiotherapy, 72.2% (13/18) during week 1, 58.3% (14/24) during week 2, 60.7% (17/28) during week 3, 67.9% (19/28) during week 4, 65.5% (19/29) during week 5, and 62.1% (18/29) at the end of radiotherapy. Overall, 87.9% (29/33) of the caregivers reported severe fatigue at some point during radiotherapy. Only a single caregiver reported mild symptoms of fatigue during radiotherapy, which occurred during week 4 of treatment. No significant differences in fatigue were detected between PBRT and XRT groups.
In multivariable models accounting for age, CSI dose, and hydrocephalus at diagnosis, differences in the mean level of fatigue were similar between PBRT and XRT groups (p > .05) with the PBRT group reporting slightly higher levels, particularly during week 3 of therapy (p = .09). The univariate analysis revealed no statistically significant associations (p > .05) between fatigue severity and demographic and clinical characteristics. Multiple linear regression analyses revealed that CSI administration dose was the only significant predictor of fatigue, but these findings were restricted to the first week of therapy (p = .037) and were no longer present by therapy completion (Table 2). In a separate analysis, time from surgery to radiation was included in the pre-radiation regression model and was not found to be a predictor of fatigue (p = .495, data not shown).
Association Between Clinical Factors of Fatigue Reported During Cranial Radiation Treatment.

Note. Models adjusted for other variables are presented in Table 1. Sample size ranged from 18–33 participants depending on the number of surveys completed at each assessment period. CI = confidence interval; CSI = craniospinal irradiation; Gy = gray; PBRT = proton beam radiation therapy; RT = radiation therapy; XRT = photon radiation therapy.
Discussion
This pilot study is among the first prospective evaluations of fatigue during radiotherapy in a cohort of pediatric patients with brain tumors treated with CSI. Despite fatigue being a well-established complication of radiation among pediatric brain tumor survivors (Meeske et al., 2004), a few studies have investigated the natural history of fatigue during therapy. The results of this study provide unique insight into the severity and prevalence of fatigue prior to and during radiotherapy and highlight the following: (a) moderate-to-severe fatigue is common in pediatric brain tumor survivors prior to radiotherapy and (b) symptoms of fatigue persist throughout radiotherapy.
Two-thirds of our sample reported severe fatigue prior to radiation therapy. The high levels of fatigue observed in our participants may be related to surgical resection given that the median interval between surgery and radiation therapy was just over one-month. It is important to note, however, that time since surgery was not predictive of pre-radiation fatigue. Although fatigue is believed to progressively increase and peak during post-radiation therapy, fatigue appeared to peak during the third week of treatment in our sample, particularly for children treated with PBRT. This is consistent with a prior study examining acute neurotoxicities in children treated with PBRT recorded by clinic nurses, which reported a peak during in fatigue during the middle of treatment with improvement thereafter (Suneja et al., 2013). The pathophysiology of fatigue among pediatric patients with brain tumors is likely multifactorial, with the contribution of each factor dependent on timing within the course of treatment. Prior to radiation, levels of fatigue may be due to the tumor itself, surgical resection, and complications from surgery. During radiation therapy, levels of fatigue may be influenced by recovery from surgery as well as disruption to homeostatic, circadian, psychological, and physical processes involved in sleep-wake regulation (Rosen et al., 2008). While the mechanisms underlying fatigue have yet to be established, studies have implicated the role of inflammatory cytokines (Brown et al., 2005), hypothalamic–pituitary–adrenal (HPA) axis dysfunction (Peters et al., 2014), deficits in monoamine neurotransmission (Hinds et al., 2000), and psychological influence (Pelletier et al., 2002) in the onset and progression of cancer-induced fatigue.
The effective management of fatigue requires a better understanding of the factors and mechanisms that contribute to symptom severity in at risk populations. In the current study, the majority of participants reported severe fatigue prior to treatment initiation and fatigue remained high throughout treatment, suggesting that patients may benefit from early intervention to mitigate fatigue, particularly those receiving CSI. CSI radiation dose was the only clinical factor associated with a statistically significant difference in on-therapy fatigue, especially during the early phases of treatment. Previous studies have reported favorable physical and psychosocial outcomes for patients treated with PBRT (Warren et al., 2018; Yock et al., 2014); however, results of this preliminary investigation appear to be consistent with a recent cross-sectional study of symptoms reported by pediatric brain tumor survivors that did not identify a significant difference in fatigue severity in patients receiving XRT and PBRT (Lai et al., 2019).
Strengths of the current study include the prospective, longitudinal, and systematic evaluation of fatigue during radiotherapy in an ethnically diverse, contemporary population of pediatric patients with brain tumors. Longitudinal investigations are particularly effective for assessing the trajectory of fatigue, which can inform interventions for patients during both active and post-therapy. The limitations of this study include a small sample size composed of heterogenous diagnosis groups, although all patients were treated with surgery and CSI. In addition, there was a relatively high rate of missing responses for fatigue assessments that were collected during active therapy (12%–45% missing). As a result, this pilot study was underpowered to adequately evaluate the diverse set of clinical and treatment factors used in the treatment of pediatric patients with brain tumors. Moreover, this study enrolled the convenience sample of research participants. Therefore, these findings may not be generalizable to all pediatric CNS tumor populations. Another limitation is the use of the parent-report fatigue questionnaire, which has previously only been validated for children seven years and older. However, this questionnaire has been used in individuals less than seven years of age with hematologic malignancies and has been found to be a reliable measure of fatigue (Hockenberry et al., 2003, 2017). Furthermore, in a secondary analysis restricted to individuals at least seven years of age, we see similar overall associations between clinical and demographic outcomes and fatigue (Table 3). These findings suggest that the inclusion of children less than seven years of age did not significantly influence our results. Future studies are warranted to replicate the preliminary results of this study in larger, independent populations and better characterize the trajectory of fatigue.
Association Between Clinical Factors of Fatigue Reported During Cranial Radiation Treatment (> 7 Years).

Note. Models adjusted for other variables are presented in Table 1. Results restricted to participants aged 7 years and older. Sample size ranged from 9–18 participants depending on the number of surveys completed at each assessment period. CI = confidence interval; CSI = craniospinal irradiation; Gy = gray; PBRT = proton beam radiation therapy; RT = radiation therapy; XRT = photon radiation therapy.
Conclusion
Routine psychosocial assessments are recommended for pediatric patients with brain tumors and their families (Kazak et al., 2015). However, information is limited on acute symptoms experienced by pediatric patients with brain tumors during active therapy. This study provides important information on the frequency and severity of fatigue experienced by pediatric patients during an understudied period of the cancer continuum. The impact of acute fatigue on other outcomes among pediatric patients treated for brain tumors is largely unknown. The symptoms of fatigue have been shown to correlate with long-term outcomes including overall survival in various cancer populations (Bower et al., 2014; Howell et al., 2013; Kazak et al., 2015; Peters et al., 2014; Portenoy & Itri, 1999). To identify patients who are most likely to benefit from supportive care, future studies should consider longitudinal evaluations, similar to this study, to assess the potential link between acute on-therapy fatigue and long-term outcomes, including survival, functioning in daily life, and the eventual development of chronic fatigue among pediatric patients with brain tumors. Additionally, interventions to mitigate fatigue which have been successful in other cancer populations, including exercise programs (Collett et al., 2007; Dimeo, 2001) and nursing interventions (Genc & Conk, 2008), should be considered for pediatric patients with brain tumors prior to or while undergoing radiation therapy. Specifically, nursing interventions can involve spending more time with patients and/or their caregivers to educate and inform them of recommendations to reduce fatigue (e.g., taking naps, increasing visitor interaction, and planning fun activities) while monitoring fatigue reports and participation rates in the nurse-provided recommendations (Genc & Conk, 2008). Given the young age at diagnosis, it is essential that caregivers be involved in monitoring on-therapy fatigue and interventions, which mitigate these effects. The serial monitoring of fatigue (prior to, during, and following therapy) is a crucial aspect of understanding the pathophysiology of cancer-related fatigue and should also be implemented into any intervention program.
This pilot study provides novel insight into caregiver ratings of patient fatigue prior to and during CSI and also demonstrates the feasibility of assessing the trajectory of fatigue during active therapy. Similar longitudinal research strategies could be conducted on a larger sample of patients with brain tumors to better understand treatment-related fatigue and how it can impact long-term outcomes. It is possible that fatigue fluctuates during therapy and potential interventions could be implemented at these time periods to mitigate long-term side effects. The current study reported fatigue outcomes for patients with brain tumors being treated with contemporary radiation therapy which are relevant to the current standard of care treatment protocols for pediatric brain tumor populations. Although underpowered for our study, future studies should examine the trajectory of fatigue and make comparisons between radiation modalities to improve patient care.
This study observed a high proportion of pediatric patients with brain tumors who experienced moderate-to-severe fatigue prior to and throughout radiation therapy. As previously mentioned, fatigue needs to be monitored prior to, during, and following therapy to fully understand the pathology of treatment-induced fatigue in pediatric patients with brain tumors. As advancements in brain tumor treatment continue to evolve, it will be essential for health care providers to monitor patient fatigue throughout therapy to improve treatment strategies and potentially reduce chronic fatigue and other associated late effects. The symptoms of fatigue correlate with overall survival and daily functioning in pediatric cancer populations (Hofman et al., 2007); therefore, it is essential for nursing professionals to understand and monitor cancer-related fatigue, so early interventions can be provided to mitigate any long-term side effects.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a Cancer Prevention and Research Institute of Texas grant.