
Abstract
Introduction
Children and adolescents treated for cancer, and those receiving a hematopoietic stem cell transplant (HSCT), face significant disruption in their physical, social, and emotional development. Beyond the limitations imposed by hospitalization and the physical discomfort associated with treatment, some have proposed that undergoing cancer treatment in childhood reduces the capacity for normal physical activity and interrupts the natural development of leisure activities (Götte et al., 2014; Viña et al., 2013). This reduction in leisure activity directly limits opportunities for social interaction, which are recommended for all patients as a Psychosocial Standard of Care in Pediatric Oncology (Christiansen et al., 2015; Wiener et al., 2020). These standards emphasize the need for activity and socialization both in and out of the hospital setting.
In addition to the negative social implications of inactivity and isolation, the side effects of treatment paired with a sedentary lifestyle can lead to further chronic disease and cancer recurrence in survivorship (Ward et al., 2014). The differences in physical activity between children with cancer and healthy siblings and peers is not just a problem of survivorship; rather it begins during treatment and is maintained for decades after treatment is completed (Ness et al., 2009; Stössel et al., 2020). As a result, the American Cancer Society and the American College of Sports Medicine have encouraged exercise as safe and important throughout cancer treatment (Campbell et al., 2019; Rock et al., 2012). Still, evidence-based recommendations about the quantity and variety of physical activity children need while hospitalized remain lacking.
The vast majority of children and adolescents diagnosed with cancer will be hospitalized at least once in their first year of treatment (de Oliveira et al., 2017). While there is variability, the average length of stay for a child with cancer is 12 days (Anhang Price et al., 2012). For a child receiving a HSCT, hospital stays often exceed one month (Broder et al., 2017). Time in the hospital removes children from their social environment and interferes with their ability to participate in previously enjoyed activities, leading to increases in social isolation, boredom, and low mood (DeJong & Fombonne, 2006; González-Gil et al., 2008; Kazak & Noll, 2015; Rourke et al., 2015). Previous studies have identified links between worsening mood and both frequency and length of hospitalizations (Doupnik et al., 2016; Esmaeeli et al., 2014), and pediatric patients themselves have indicated a need for activity and a desire for new experiences when in the hospital (Oksala & Merenmies, 1989; Runeson et al., 2002). When provided with additional opportunities to be active, children have demonstrated improved health-related quality of life (HRQoL) and increased satisfaction with their care (San Juan et al., 2008; Speyer et al., 2010).
Prioritizing the socioemotional health of a child and helping them to meet developmental milestones while hospitalized is a challenge for patients and providers alike. Fortunately, physical activity programs performed with children with cancer have been demonstrated to be safe and efficacious (Baumann, Bloch, & Beulertz, 2013; Braam et al., 2016). One specific approach to increasing activity in cancer and HSCT patients during treatment is therapeutic recreation (TR). Certified TR specialists (CTRSs) use a variety of modalities (e.g., games, dance, music, art) to help individuals restore or rehabilitate their level of function, maximize independence in life activities, promote health and wellness, reduce or eliminate activity limitations caused by illness, and enhance their quality of life (Carter & Van Andel, 2020). While there is some overlap between CTRS and certified child life specialists (CCLS) in the pediatric setting, there are important differences. A CTRS uses a child's leisure activities to address specific goals, whereas a CCLS will use activities to increase coping and diversion. For example, a CTRS working in a pediatric oncology setting may use pinball to build standing tolerance after an extended PICU stay or may work on adaptive strategies to help a child suffering from neuropathy hold playing cards. TR has been studied in a variety of adult populations and has demonstrated improvements in well-being, social skills, mood, and quality of life (Bauer et al., 2010; Buettner et al., 1996; García-Villamisar et al., 2017). However, it remains an understudied intervention, particularly with youth in the hospital setting.
The current study was designed to evaluate the impact of a TR program on an inpatient oncology and HSCT floor. Specifically, we hypothesize that children and adolescents provided with structured opportunities for TR will improve in the domains of physical activity, mood, social connectedness, and HRQoL compared with patients with limited opportunities. We also describe the experience with TR programming from the perspective of patients and parents.
Methods
Study Design and Setting
This was a single-site, interventional study with historical controls used to evaluate the impact of TR programming provided on an inpatient medical floor. A convenience sample of participants were recruited from the oncology and HSCT services at a large tertiary children's hospital in Wisconsin. Historical control data was collected between November 2016 and May 2017, prior to the initiation of a TR program. Once the TR program was well-established and became an expected part of care, data collection resumed (February 2019). Enrollment was discontinued in March 2020 due to the detrimental impact the coronavirus disease 2019 (COVID-19) pandemic had on our ability to offer TR programming.
Participants
Children were eligible if they were between the ages of 8-17 years, had an oncology diagnosis or were receiving a HSCT, and were expected to be hospitalized for at least three days. Participants were excluded if they were non-English speaking, unable to leave their hospital room due to isolation precautions, too sick to participate in recreational programming (as determined by the medical provider), or had significant developmental delays that would have prevented them from completing required study questionnaires. There were 106 children screened for eligibility. Of these, 50 (47.2%) were excluded. Thirty participants were enrolled in the historical control arm, which occurred prior to the development of the TR program; 29 were included in the analysis. An additional 26 age- and treatment intensity-matched participants were enrolled in the intervention arm; 20 were included in the analysis. See Figure 1 for additional information about enrollment and participation.
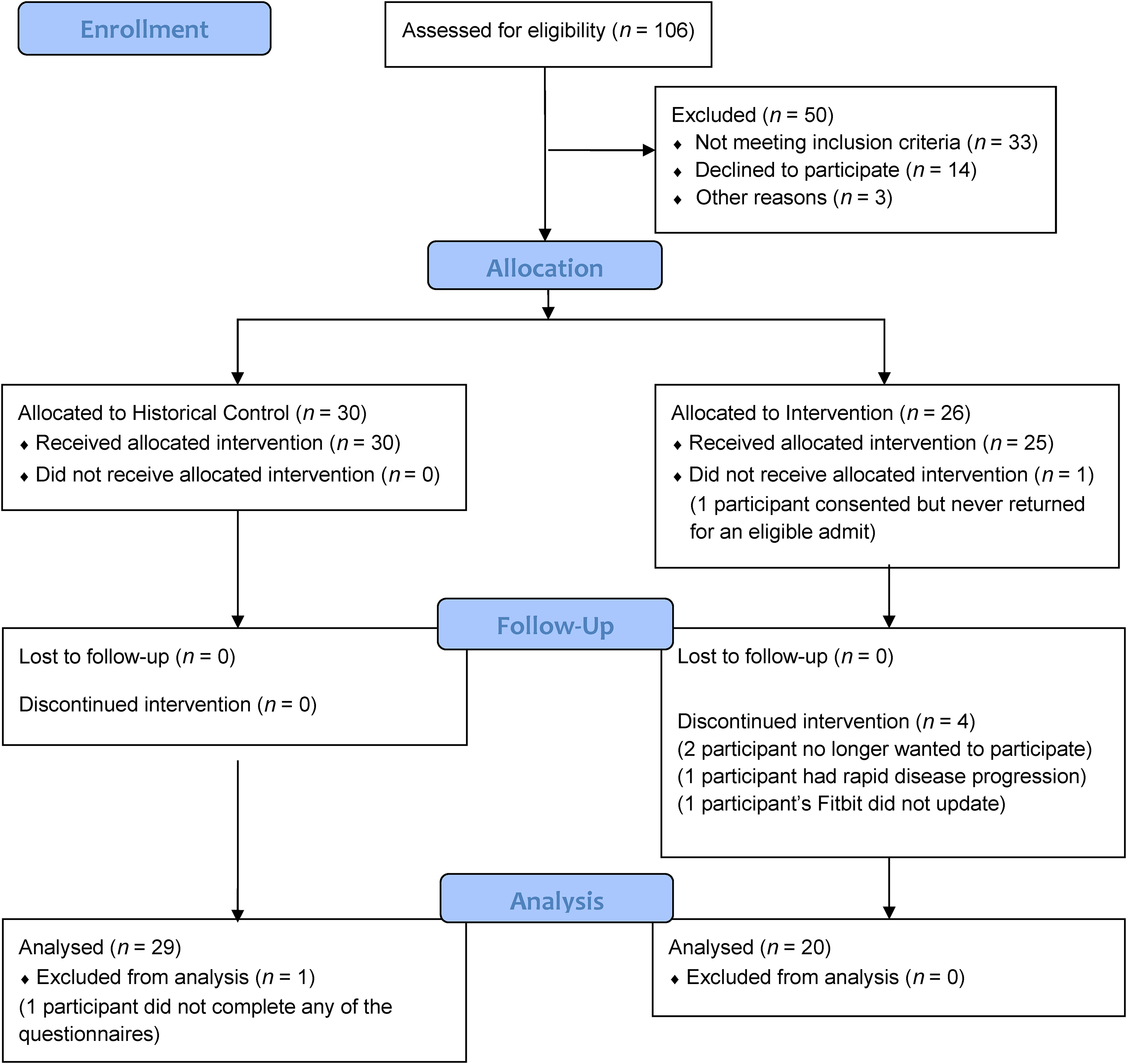
Enrollment diagram.
Procedure
Eligible participants were approached by study personnel and provided with information about the study. Caregivers signed consent forms for their child's participation and all children provided written assent. Participants were given a Fitbit at the time of enrollment and asked to wear it continuously during study participation. The Fitbit was set to block participants from viewing their steps taken to ensure that motivation to reach step counts did not present a confounding variable. Caregivers and/or children completed a set of questionnaires at the end of three days or just prior to hospital discharge, whichever came earlier.
Participants enrolled in the historical control arm of the study had access to a team of psychosocial providers, including a certified child life specialist (CCLS). The CCLS offered one-on-one bedside interventions as needed, primarily aimed at providing anticipatory guidance and support during procedures, but occasionally also involving therapeutic play. Participants enrolled in the intervention arm of the study were provided with the same team of psychosocial providers, with the addition of structured TR programming performed by a single certified TR specialist (CTRS). TR programming was not a standardized intervention in that daily individual and group programming was offered but participation was not mandatory. Sessions ranged from 30 to 90 min and were tailored to fit the abilities and leisure interests of the participants.
Measures and Materials
Relevant demographic data was gathered from the electronic health record. Specific data obtained included date of birth, ethnicity, gender, date of diagnosis, length of treatment, treatment intensity (utilizing the Intensity of Treatment Rating Scale; Kazak et al., 2012), length of hospitalization, and reason for hospitalization. All dates were removed once calculations were made (e.g., age at diagnosis).
A Fitbit Charge HR activity tracker worn on the dominant wrist was used to track daily number of steps. Prior work assessing physical activity has found Fitbit devices to be an adequate estimate of physical activity requiring less interfering and less expensive equipment than actigraphy (Evenson et al., 2015). Participants were instructed to wear the Fitbit continuously during the three days of study participation, aside from bathing. We used heart rate data from the Fitbit to determine if participants were wearing it as instructed. A day was considered valid if the participant wore the Fitbit for 80% of the 24-h period. A research coordinator checked in with study participants and uploaded data from the Fitbit daily.
The Behavioral, Affective, and Somatic Experiences Scale-Revised (BASES-R) is a 22-item measure of HRQoL in patients undergoing active and intensive therapy (Phipps et al., 1999). It includes four domains: somatic distress (5 items), mood disturbance (7 items), quality of interactions (3 items), and adherence (5 items). Scores on each item range from 1–5 with lower scores indicating better quality of life. Additionally, there is one question about physical activity and sleep each. The BASES-R has demonstrated adequate reliability and validity in children aged 5 to 17 years.
The Pediatric Peer Relationships – Short Form 8a is an 8-item self-report measure of friendship from the Patient-Reported Outcomes Measurement Information System (PROMIS) Pediatric Item Bank v2.0 used to evaluate the availability of perceived companions during study participation. It was modified to instruct participants to recall their peer interactions over the past three days. This measure has demonstrated strong psychometric properties when used in children between ages 8–17 years (DeWalt et al., 2013). All scores are reported as T-scores with a mean of 50 and a standard deviation of 10. Higher scores indicate better social relationships.
Positive Affect is a 4-item self-report measure from the PROMIS Pediatric Item Bank v2.0 used to evaluate happiness and joy experienced during study participation. It was modified to instruct participants to recall their mood over the past three days. This measure has demonstrated strong psychometric properties when used in children between ages 8–17 years (Forrest et al., 2018). All scores are reported as T-scores with a mean of 50 and a standard deviation of 10. Higher scores indicate better mood.
Participants were asked to complete a brief survey assessing their perception of the content and availability of recreation programming, their satisfaction with each aspect of programming, and to offer suggestions for improving future programming.
Data Analysis
Study groups were compared using Chi-square or Fisher's exact test for categorical variables and Student's t-test or Mann-Whitney test for continuous and ordinal variables. Study groups were compared with the normative sample using the one-sample t-test. Statistical software used included SAS 9.4 and SPSS 26. Unadjusted p-values <0.05 were considered statistically significant.
Results
Demographics
Participant demographics are presented in Table 1. There were 29 historical control and 20 intervention participants included in the analyses. There were no differences between groups by participant age, gender, race, diagnosis, treatment intensity, time in hospital prior to study participation, or reason for hospitalization. Five of the 20 (25%) intervention participants declined to participate in TR programming. They were no differences between these participants and the other participants in the intervention group. We reassigned the five TR nonparticipants from the intervention to the historical control group and reran our analyses. All significant results remained the same; there was one finding related to program satisfaction that went from nonsignificant to significant with the reassignment. This result is reported below in the “Programming Satisfaction” section. However, to remain true to our intervention (i.e., TR programming available but not mandatory), all other results are based on analyses that include the five TR nonparticipants in the intervention group.
Participant Demographics.
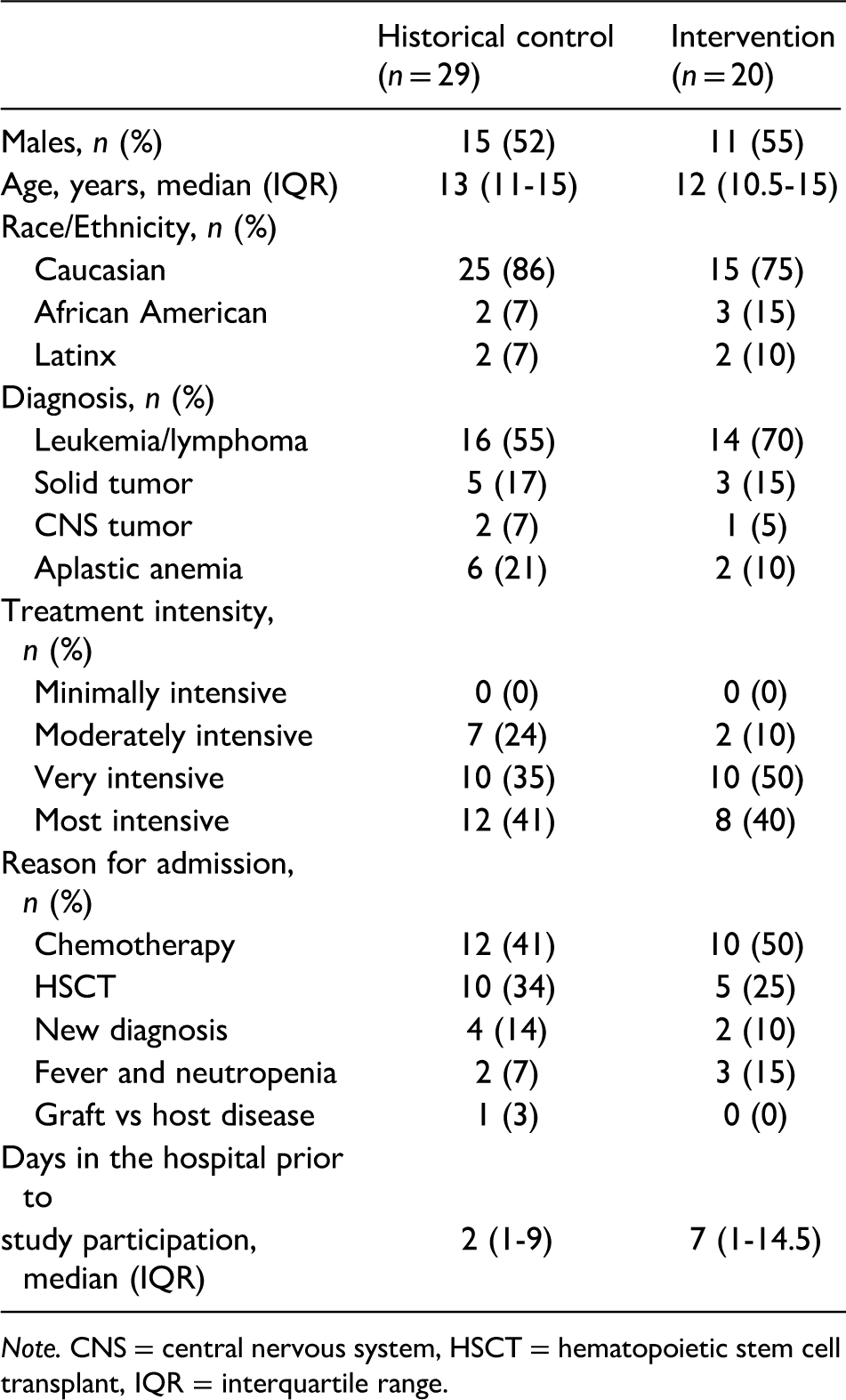
Note. CNS = central nervous system, HSCT = hematopoietic stem cell transplant, IQR = interquartile range.
TR Programming
Of the intervention participants, 40% engaged in TR every day of study enrollment; 20% engaged in TR 2 of 3 days; 15% engaged in TR 1 of 3 days; and 25% declined to participate in TR. Thirty-nine percent of sessions were 30–45 min in length; 25% were 60 min; and 36% were 75−90 min. Most of the participants (67%) engaged in individual TR sessions only; 20% engaged in group TR sessions only; and 13% engaged in both individual and group programming. TR activities fell into five main categories: physical activity (41%), board or card games (36%), video games (9%), arts and crafts (9%), and therapeutic conversation (4%).
Physical Activity
There were no significant differences in daily number of steps measured by the Fitbit between the historical control (Mdn = 1314, IQR: 883−2044) and intervention groups (Mdn = 1579, IQR: 881−2883). Participants in both groups rated their level of activity similarly as somewhere between “a little active; sitting up in bed” and “fairly active, out of bed.”
HRQoL
There were no significant differences between the groups in ratings of somatic distress, level of cooperation with cares, or quality of interactions with parents and medical staff. There was a difference between the groups with respect to ratings of sleep quality, with the intervention group rating their sleep as significantly better than the historical control group (p = 0.003). Median BASES scores for sleep were 3 (IQR 2–3) for the historical control group and 2 (IQR 1–2.5) for the intervention group on a 1–5 score scale with lower scores representing better sleep.
Peer Relationships
There was no significant difference between the groups’ scores on the quality of their peer relationships. Both the historical control (mean [M] = 39.76, standard deviation [SD] = 13.40) and intervention (M = 39.64, SD = 17.54) group scores were a full standard deviation below the normative value (p < 0.001 and p = .03, respectively), indicating a poorer perception of the availability and support of peer companions.
Mood
Compared with the historical control group, participants in the intervention group had significantly higher scores on a measure of positive affect and significantly lower scores on a measure of mood disturbance, p = 0.03 and p = 0.03 for both variables. The intervention group had similar levels of positive affect as the normative sample (M = 47.82, SD = 10.16), while the historical control group neared one standard deviation lower than the normative sample (M = 41.89, SD = 10.60, p < 0.001).
Programming Satisfaction
There were significant differences between groups on the TR satisfaction survey. Compared with the historical control group, the intervention group: Agreed more strongly that there were age-appropriate and interesting activities offered (p = 0.04); identified that there were enough opportunities for recreation while hospitalized (p = 0.002); and were more highly satisfied with the recreational programming (p = 0.01). When we included the five TR nonparticipants in intervention group, there was no difference between the groups in frequency of participation, with both groups identifying that they participate in recreational activities somewhere between 2–3 times per week and once a day. When we shifted the five TR nonparticipants to the historical control group, the remaining participants in the intervention group identified more frequent engagement in recreational activities than the historical control group (p = 0.04).
Discussion
Children and adolescents with cancer and those receiving a HSCT spend significant time in the hospital (Anhang et al., 2012; Broder et al., 2017), which interferes with their ability to participate in previously enjoyed activities and spend time with friends, leading to low mood, impaired HRQoL, and severe reductions in physical activity (González-Gil et al., 2008; Kazak & Noll, 2015; Rourke et al., 2015; Stössel et al., 2020). This study was designed to address these challenges by comparing the standard psychosocial care offered in the hospital to the addition of structured TR programming.
While there is a dearth of literature specific to TR, our findings support previous research that has identified a link between mood and increased leisure activities (Gillard, 2019; Pressman et al., 2009). We found that, compared with the historical control group, children receiving TR reported increased positive affect and decreased mood disturbance. This finding aligns well with stress and coping literature, which has demonstrated that deliberate engagement in pleasant and distracting activities can attenuate depressive episodes (Broderick, 2005; Lazarus et al., 1980; Nolen-Hoeksema et al., 1993).
TR was not a successful mechanism to increase peer support in the hospital with both the historical control and intervention groups rating the availability of peers as low. The TR program was designed to offer bedside and group activities. We did not mandate participation and found that group activity participation was low, with many days when no one participated. Anecdotal findings revealed several challenges, including wide-ranging developmental differences amongst children on the floor at a given time and difficulties finding common times to participate due to medical cares, fatigue, or not feeling well. It is relevant to note that this study was implemented pre-COVID so participation was not restricted by policies related to communicable disease.
Previous reviews of clinical exercise interventions have found that increasing activity during cancer treatment is feasible and safe, and results in benefits to cardiorespiratory fitness, muscle strength, and endurance (Baumann et al., 2013; Braam et al., 2016). While our TR program was not a structured exercise intervention, it offered increased opportunities to be more physically active while hospitalized. Contrary to our expectations, however, physical activity did not increase in the TR group. According to the Physical Activity Guidelines for Americans, 2nd Edition, school-aged children should participate in 60 min of moderate (e.g., brisk walking)-to-vigorous (e.g., running) intensity physical activity daily (U.S. Department of Health & Human Services, 2018). This is equivalent to somewhere between 11,000–15,000 steps per day for younger children and 10,000–11,700 steps per day for adolescents (Tudor-Locke et al., 2011). At under 2,000 steps per day, our study participants demonstrated a very low level of activity compared with recommendations for healthy children. This finding is consistent with previous research, which has identified that children undergoing cancer treatment are severely deconditioned compared with healthy children, even when they are ambulatory and appear well (Hooke et al., 2013).
Pediatric patients have identified a number of barriers to increasing activity during cancer treatment, such as side effects of chemotherapy, low energy, poor motivation, and lack of space in the hospital (Götte et al., 2014). Our CTRS offered individualized activities and a willingness to be flexible with intervention timing to better coordinate with periods of feeling well. Nevertheless, the lack of established guidelines for physical activity during pediatric cancer treatment have contributed to a culture of inactivity in the hospital. Additionally, despite our efforts to provide more engaging activities to motivate children to get out of bed, the limitations of our physical space mean that many activities are not possible.
Limitations and Future Research
This is one of the only studies examining the role of TR in a cohort of hospitalized pediatric patients. Although this study has several strengths, limitations must be noted. First, due to the nature of leisure interests and the population under study, the TR intervention could not be standardized, making it difficult to draw conclusions about which of our findings were due to the intervention and which were due to the increased attention our intervention participants received. Furthermore, we did not mandate participation in TR activities, which presents challenges to the rigor of the study, although offers perhaps a more realistic view of the effectiveness of TR programming in the hospital setting.
The small sample size and disproportionately low numbers in our intervention group presents a second limitation. Our original intent was to recruit 30 matched participants into each arm of the study. Unfortunately, the COVID pandemic caused an untimely closure to the study. We additionally learned that a small but significant number of participants in the intervention group declined all TR programming. These challenges reduce the likelihood that our study is powered to detect a true effect. Future research should include a larger sample, offer more structured individual and group programming, and build in better controls for variable attendance.
A third limitation is related to the physical activity tracker selected. The Fitbit Charge HR had two band sizes available to accommodate differently sized wrists; however, the small band was still too large on some younger participants and made for uncomfortable wear and potentially less accurate measurement. There is also some recent data to suggest that the Fitbit Charge is less accurate than other trackers at slower gait speeds (<8 km/h) and may undercount steps (Chow et al., 2017; Toth et al., 2018). Additionally, while the Fitbit Charge monitors heart rate, it lacked sensitivity to identify the differences between sleeping and awake but sedentary or heart rate increases related to physical activity and those related to fever. In the years since this study was designed, the landscape of wearable fitness tracking options has skyrocketed. Future research would benefit from a physical activity tracker that is better suited for pediatric use, is more accurate for slow speeds, and is able to consider the variability in heart rate that is seen in this population.
Conclusions
Children and adolescents undergoing HSCT and other cancer treatments should be encouraged to get out of bed and engage in leisure activities during hospitalization. Given the risks of sedentary behavior during hospitalization, TR programs offer one avenue to increase physical activity and improve mood and sleep. With their frequent interactions with patients, nurses are a primary source of support and guidance about activity in the hospital. This provides nurses a unique opportunity to promote programs, such as TR, and, more broadly, the engagement in leisure activities while hospitalized.
Footnotes
Acknowledgments
We would like to thank Northwestern Mutual Foundation for their philanthropic support of our therapeutic recreation program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a grant from the Midwest Athletes Against Childhood Cancer (MACC) Fund.