
Abstract
Introduction
Successfully adhering to the complex outpatient medication regimen after pediatric hematopoietic stem cell transplant (HCT) is important for mitigating morbidity and mortality risk (Pai et al., 2018; Skeens et al., 2019). However, children and families struggle to take outpatient medications as prescribed (i.e., medication adherence), such that only 73% of doses were taken, on average, within the first 6 months after discharge from the initial HCT hospitalization (McGrady et al., 2014). Improving medication adherence represents a potentially modifiable and minimally invasive behavioral target to improve health outcomes in this population.
The heterogeneity of diagnoses associated with pediatric HCT results in caregivers entering treatment with a wide range of medication management experience (minimal to extensive). During the HCT hospitalization, the post-HCT regimen is managed by the child's medical team with minimal required caregiver involvement. However, upon hospital discharge, caregivers assume full responsibility for their child's critical and extensive medication regimen, often too quickly for them to adequately prepare due to the unpredictable and multifactorial clinical courses of pediatric HCT.
While caregivers often view hospital discharge positively, they also describe concurrently feeling overwhelmed and intimidated by the prospect of taking over their child's medical care (Kaziunas et al., 2016). During this process, they are learning how to effectively manage a complex and highly demanding medication regimen while also balancing other treatment demands (e.g., tube feeds, clinic appointments, and infection control procedures), their own emotional needs (e.g., feeling overwhelmed or uncertain), and competing responsibilities associated with their daily life (e.g., caring for other children, returning to work; Chardon et al., 2022; Hoegy et al., 2019; Kaziunas et al., 2016; Morrison et al., 2018). The degree to which these demands and responsibilities are salient and serve as barriers to medication adherence varies widely between caregivers (Chardon et al., 2022; Hoegy et al., 2019; Morrison et al., 2018). Consequently, a one-size-fits-all intervention to improve outpatient medication adherence is unlikely to be effective. Intervention development efforts that include caregiver perspectives have been shown to be more relevant, meaningful, and better aligned with the interests and needs of specific populations (Lambert et al., 2019). Research is needed to systematically explore caregiver perspectives of and recommendations for outpatient medication adherence support post-HCT.
This study aimed to (a) characterize caregivers’ perspectives on what type(s) of supports provided by the medical team were most helpful for managing their child's outpatient medication regimen and (b) present the practical recommendations caregivers provided for enhancing supports provided by the medical team to improve medication management for future families undergoing HCT. Results will inform the development of future interventions to promote outpatient medication adherence post-HCT. There were no a priori hypotheses as this was an exploratory study.
Methods
Participants
Participants were primary caregivers of children (≤12-year-old) who received an HCT in the last two years. Eligible caregivers were fluent in English, did not have cognitive impairments that precluded participation, and had a child prescribed oral HCT medication at the time of recruitment or would be after hospital discharge. Sample characteristics were chosen because a large portion of pediatric HCTs occur in ≤12-year-old children when caregivers are primarily responsible for medication management. To provide insight into caregiver perceptions of medication adherence supports leading up to and after hospital discharge, purposeful selective sampling was used to recruit caregivers of children who were post-HCT and either still in the hospital but approaching discharge or who had already been discharged.
Of the 35 caregivers approached, 30 consented to participate. One caregiver withdrew prior to completing study procedures resulting in a total sample of 29 caregivers who completed the semi-structured interviews (9 inpatients; 20 outpatients) and provided demographic information. Caregivers (Mage = 36.2 years; SD = 8.6) were predominantly female (86%), White (83%), and non-Hispanic (97%). Most children (Mage = 5.8 years; SD = 3.6) were male (62%), White (83%), and non-Hispanic (93%) and had received an allogeneic HCT (86%). The most common HCT-related diagnosis category was bone marrow failure (e.g., Kostmann syndrome, myelodysplastic syndrome, and Shwachman-Diamond syndrome; 45%). Mean days since HCT was 219 days (SD = 210). Detailed sample characteristics are included in Table 1.
Participant and Child Demographics.
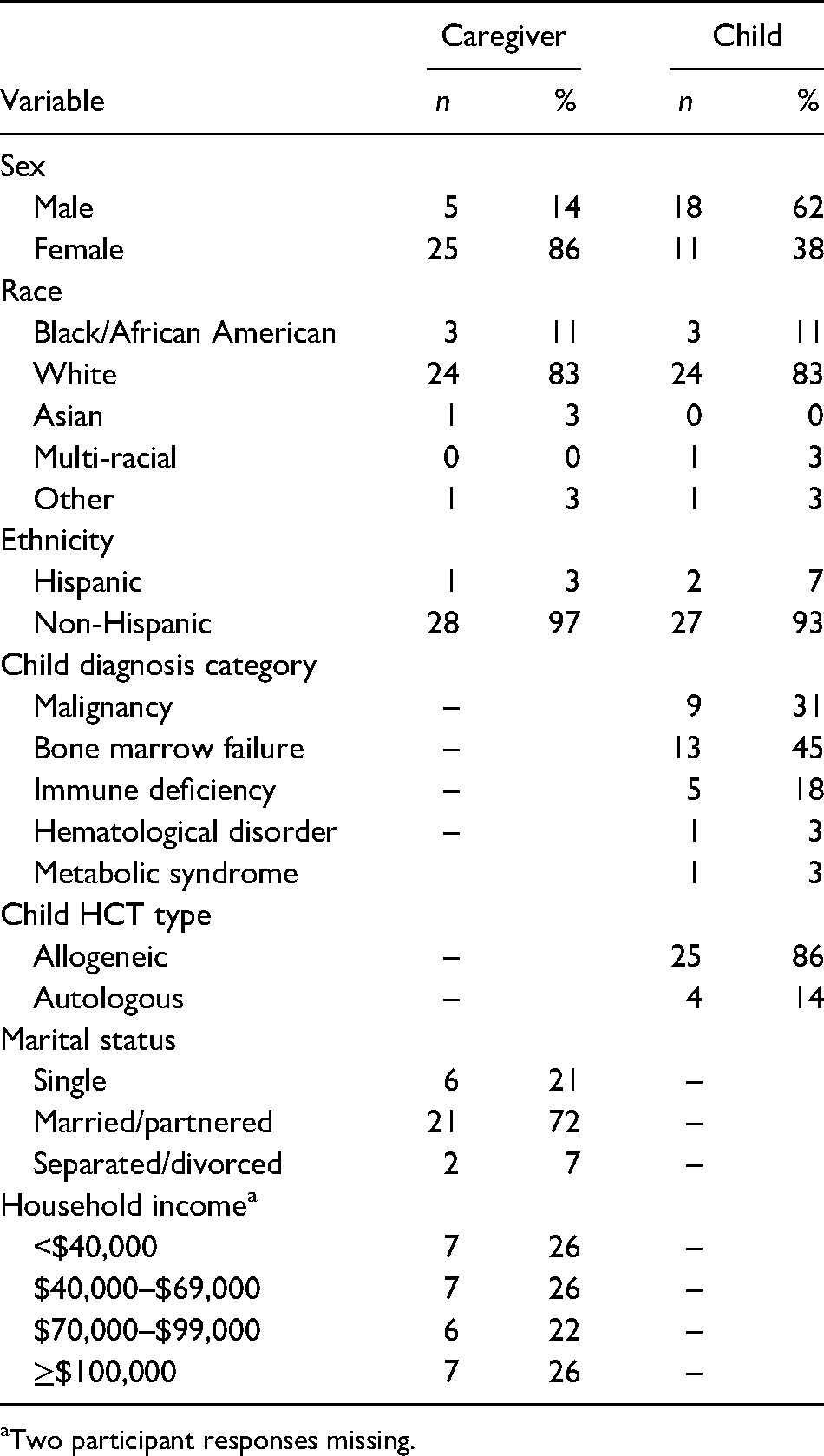
Two participant responses missing.
Study Procedures
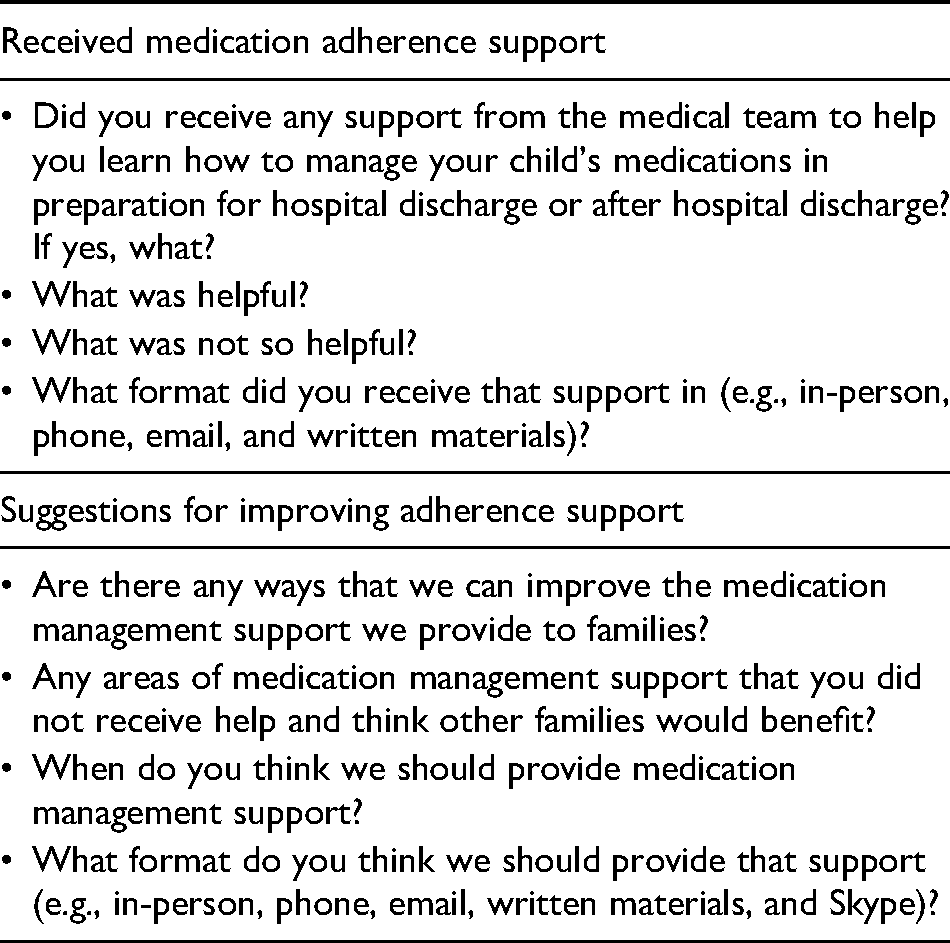
Study procedures were approved by the Institutional Review Board at the pediatric hospital where data were collected. Caregivers were identified via medical record reviews and recruited between April 2020 and July 2020. After providing informed consent, caregivers completed individual semi-structured interviews (29–84 min) over the telephone. To guide interviews, a topic guide was developed in consultation with two experts in pediatric HCT adherence and based on the current literature in this area (Hoegy et al., 2019; Konstantinou et al., 2020; Morrison et al., 2018). It included open-ended questions to elicit caregivers’ perception of medication adherence support provided by the medical team and their suggestions for improving such support (see Table 2). Interviews were audio-recorded and transcribed verbatim by a HIPPA-compliant transcription service.
Example Questions for Suggestions of Support.
After semi-structured interviews, caregivers completed questionnaires via RedCap or in paper-and-pencil format. Caregiver and child demographic information was collected from caregiver report on a demographic form and on select items within the Psychosocial Assessment Tool-HCT (Pai et al., 2019). Medical treatment information was collected from children's electronic medical records.
A card sort task questionnaire was developed after the first four semi-structured interviews to help identify which medication adherence supports caregivers received and recommended for future families. Information used to develop this questionnaire consisted of caregiver interviews (n = 4), literature review, and consultation with an expert in pediatric HCT medication adherence. This resulted in 16 areas of medication management support (see Tables 4–6). For each area, caregivers were asked (1) if they received that support (yes/no) and (2) if they believed another family would benefit from support in that area (yes/no). If caregivers endorsed question 2, they were asked a series of follow-up questions to determine the timing of such support(s), how support(s) should be provided, and who from the medical team should provide such support(s). They were also asked about their preference for six specific adherence tools. Given the branching logic, this questionnaire was only administered electronically via RedCap. Thus, the two caregivers who opted to complete questionnaires via paper-and-pencil did not complete this measure. One caregiver also failed to complete questionnaires, resulting in 22 caregivers who completed the card sort task questionnaire.
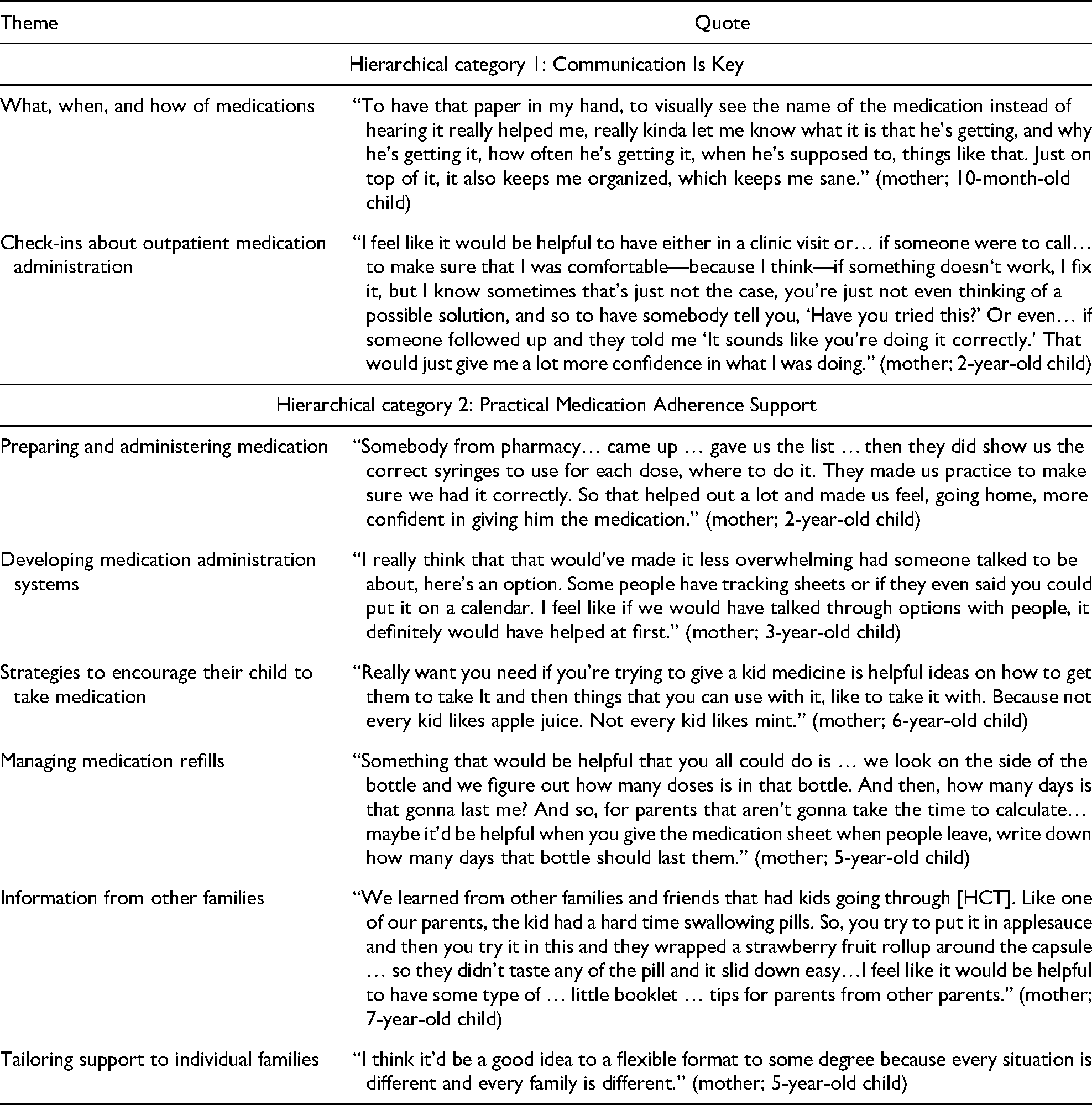
Example Quotes for Qualitative Themes.
Card Sort Task Questionnaire Results: Counts of Caregiver Endorsement of Received Support and Recommendations for Adherence Support Content/Timing.
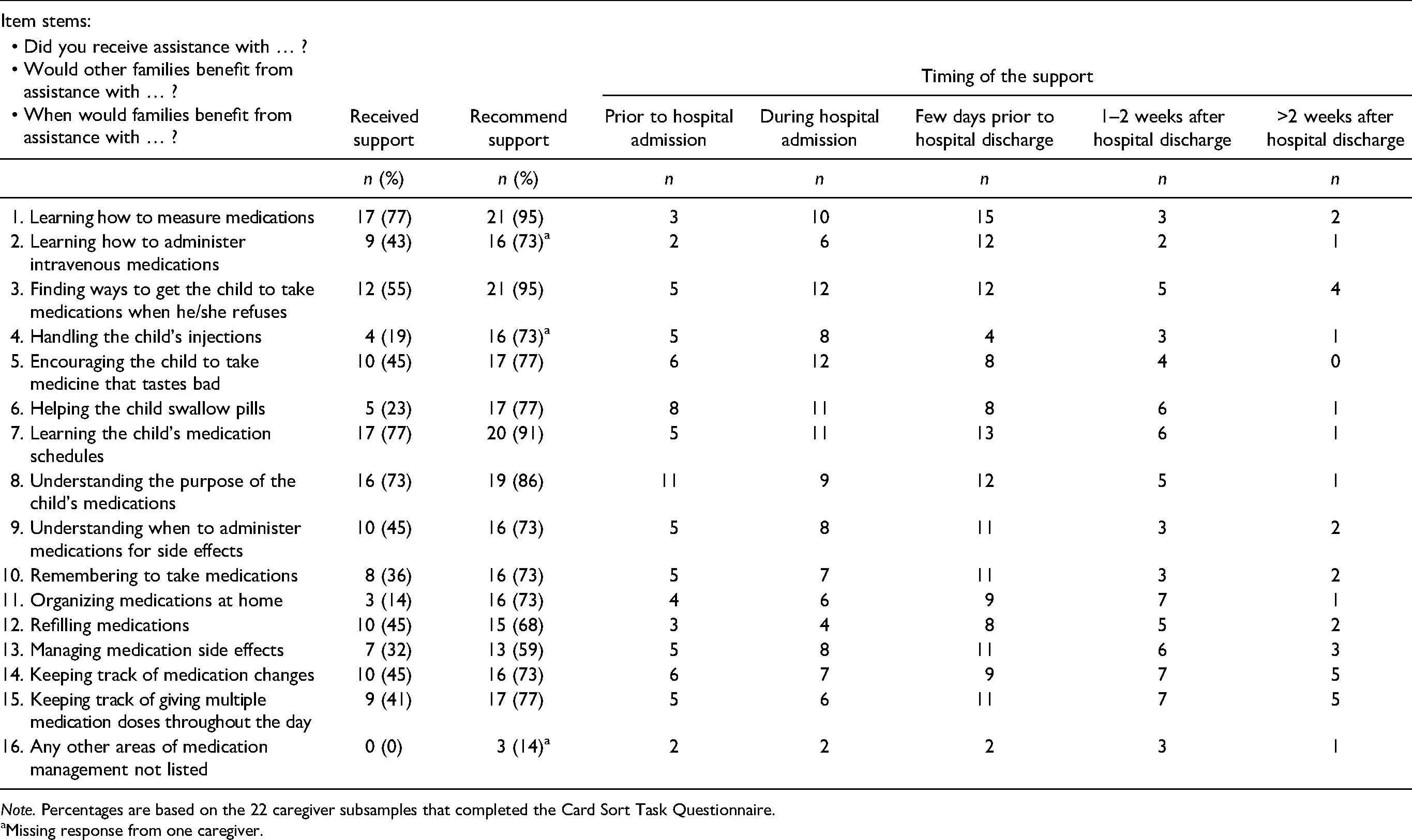
Note. Percentages are based on the 22 caregiver subsamples that completed the Card Sort Task Questionnaire.
Missing response from one caregiver.
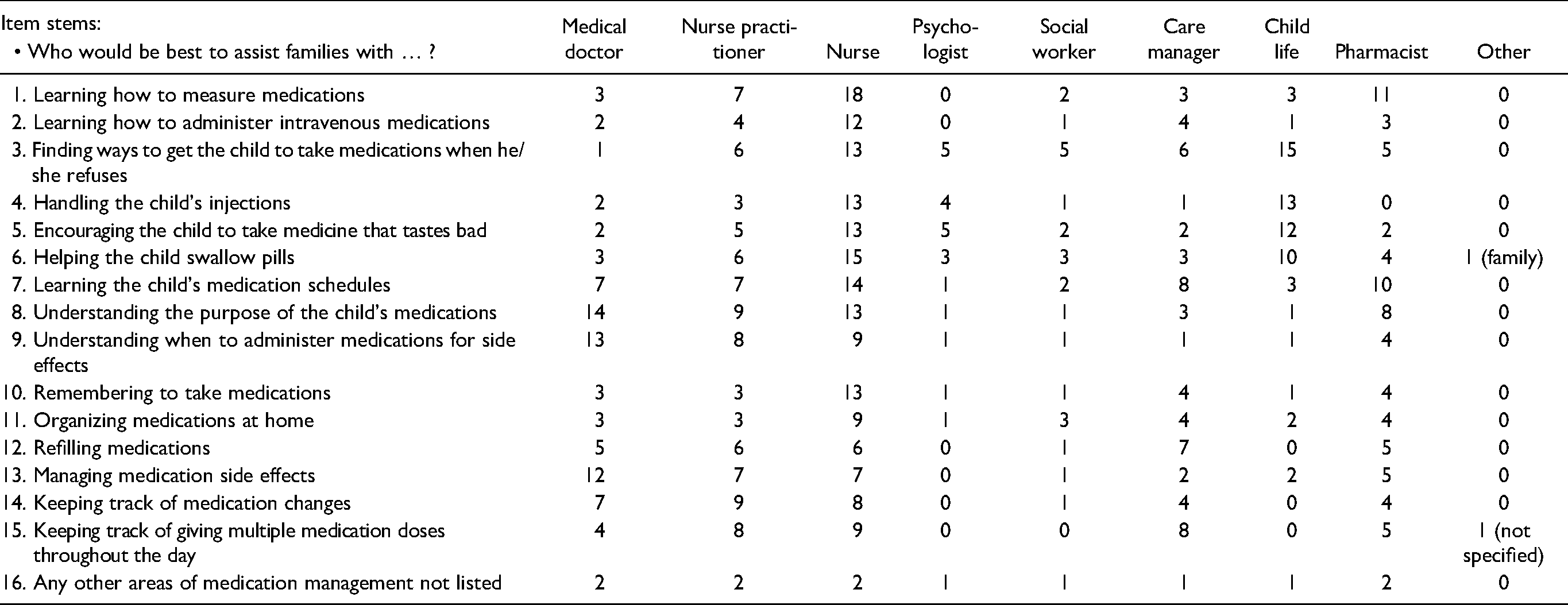
Card Sort Task Questionnaire Results: Counts of Caregiver Endorsement for Personnel to Provide Adherence Support.
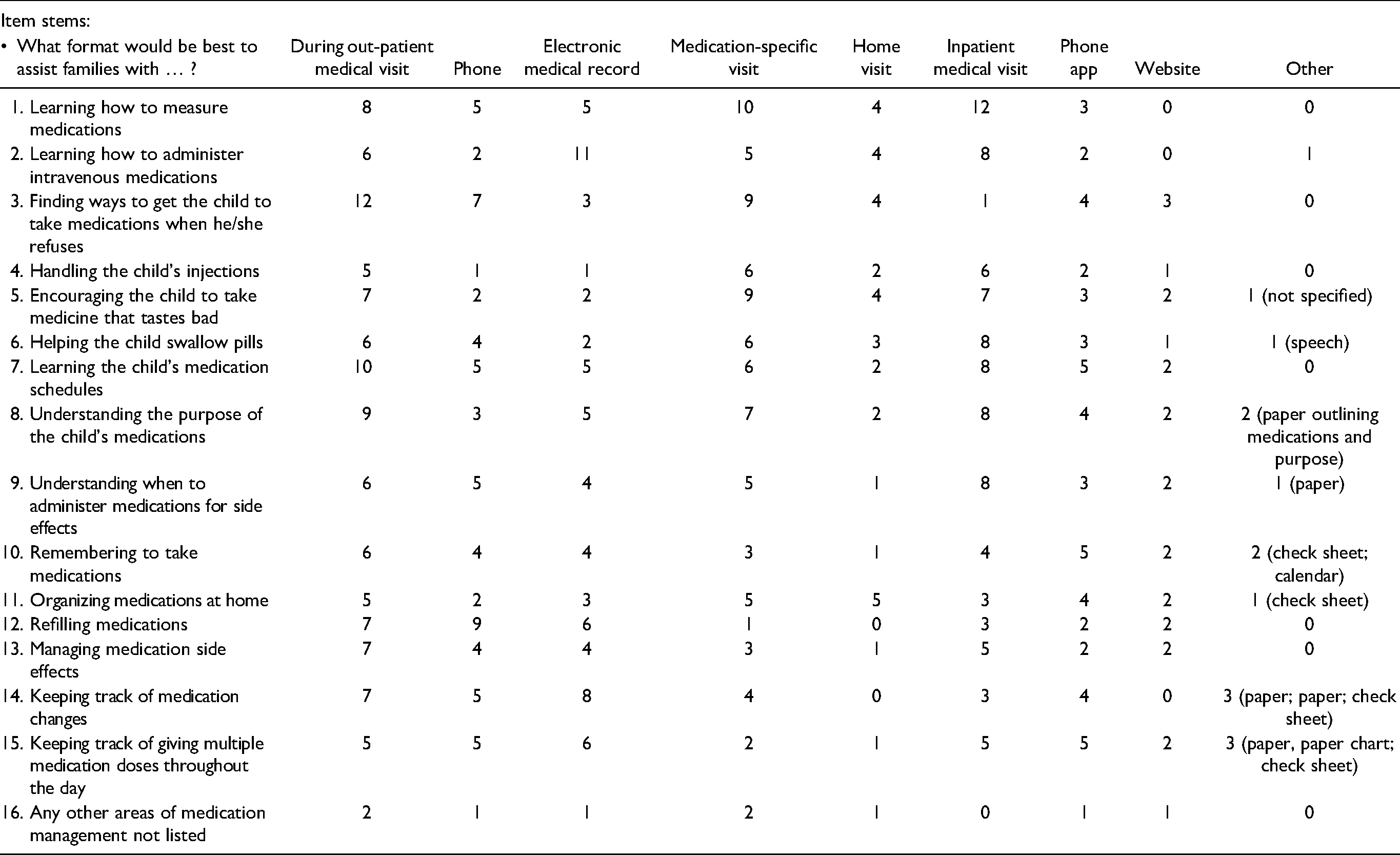
Card Sort Task Questionnaire Results: Counts of Caregiver Endorsement for the Format to Provide Adherence Support.
Data Analysis
Descriptive statistics and frequencies for the card sort task questionnaire were computed in SPSS Version 25. Transcripts were coded using thematic analytic methods in QSR NVivo (Version 13; Attride-Stirling, 2001). Qualitative methods (grounded theory and thematic analysis) were used as they are ideal for studies examining novel areas of research since they allow for data to be gathered inductively and directly from participant experiences, which limits researcher bias (Attride-Stirling, 2001; Wu et al., 2016). Coding occurred in four stages to ensure that themes were inductively built (Charmaz et al., 2018). In the first stage, first and fourth authors independently completed line-by-line coding of one inpatient and two outpatient transcripts to inductively build themes. In stage two, the first and fourth authors then created an initial coding dictionary to guide further analysis by comparing their independently generated line-by-line coding using axial and dimensional coding. In the third stage, the first author, the master coder, trained the second author on all procedures. Once 80% agreement was achieved across authors 1 and 2, the first author coded the remaining 20 transcripts independently while also meeting periodically with the second author to review coded transcripts and discuss any amendments to the coding dictionary. The fourth author was consulted to resolve discrepancies between coders and reviewed any coding dictionary amendments. Recruitment and qualitative methodology used in this study have been previously published by Chardon et al. (2022).
Results
Eight themes emerged from qualitative interviews, which were organized into two hierarchical categories: Communication Is Key and Practical Medication Adherence Support. Example quotes for themes are presented in Table 3.
Hierarchical Category 1: Communication Is key
Caregivers uniformly identified frequent, clear, and open communication between themselves and the medical team as key to helping them optimally manage their child's medication regimen. Provider communication was perceived as imperative for caregivers to be knowledgeable and well-informed about their child's medication regimen, which they described as the foundation for mediation adherence. They also noted the importance of being empowered to work collaboratively with the medical team to coordinate their child's care and treatment needs. “Communication is key … keep the lines of communication open…. That is monumental because that's the only way to get your child through this. So, everybody will be on the same page” (mother; 5-year-old child). Specifics about the communication content caregivers found helpful and recommend for future HCT families fell into the two themes discussed below.
Discussing the What, When, and Why of Medications
Caregivers described it as important to receive education from the medical team about what medications their child was prescribed (e.g., medication names), when to administer medications (e.g., dosing/weaning schedules), and why the medications were prescribed (e.g., purpose of the medication). The medical team reportedly communicated the what and why of medications consistently during the inpatient admission (e.g., during hospital rounds and discussions with nurses), hospital-to-home transition (e.g., pre-discharge meeting with the pharmacist), and post-discharge (e.g., during clinic visits). Caregivers struggled to retain medication information early in their child's HCT admission, largely due to their lack of familiarity with medications and the vast amount of information to learn during that period. Consequently, caregivers benefited from frequent discussions with medical providers about the what and why of medications, as well as being able to ask questions throughout the inpatient period. Ongoing communication during their child's hospitalization helped them assume responsibility for the outpatient medication regimen as they were already familiar with many of the medications. Caregivers preferred when the medical team avoided jargon and recommended prioritizing using layman's terms when communicating about medications (e.g., “medications that lower your child's ability to fight infections” vs. “immunosuppressants”).
Discussions about the when of medications (e.g., dosing schedules) typically began several days prior to hospital discharge when caregivers met with the pharmacist to review their child's planned outpatient medication regimen. Following discharge, dosing schedules were discussed primarily during clinic visits. Information about the ideal administration schedule was communicated clearly; however, information about flexibility in medication administration timing (e.g., medication can be given in an hour window) was not. Caregivers thought that clear, direct information about medication administration timing would be helpful for future caregivers.
Finally, caregivers appreciated being provided written materials to support communication about medications (i.e., medication lists, checklists, calendars, electronic medical records, and emails). These materials helped them retain medication information and coordinate daily administrations, especially when juggling many medications with complex dosing schedules. Preference for paper versus electronic formats of these materials differed between caregivers. One caregiver noted that the MyMedSchedule Plus app (MyMedSchedule Plus, 2021) was useful as it allowed the medical team to update any changes to their child's medication regimen in real time rather than waiting to provide them with a new written medication list at their next clinic visit. Caregivers suggested adding information about medication purposes and side effects to these materials. They also thought families may benefit from a list of questions to ask the medical team about managing their child's medications, as caregivers described frequently feeling unsure about what to ask. Communication materials were primarily given near hospital discharge and during outpatient clinic visits. Several caregivers noted that it would be helpful to receive these tools earlier in the hospital admission to help them learn medication information.
Check-ins About Outpatient Medication Administration
Check-ins about medication administration during outpatient clinic appointments were described as helpful as they prompted discussion about medication administration challenges the caregiver may not have thought to express. Additionally, seven caregivers reported feeling empowered and reassured by their child's medical team. This promoted engagement in shared decision making and increased their confidence, both of which facilitated outpatient medication adherence.
Caregivers indicated that it would be helpful for the medical team to initiate check-ins about outpatient medications. They explained that they often felt overwhelmed during the discharge process and thought they needed to problem-solve medication administration concerns independently. Thus, they recommended that the medical team prioritizes frequent in-person or phone check-ins during the first few weeks post-discharge as caregivers are becoming familiar with their child's outpatient medication regimen and establishing routines that could then be spaced out based on family preference. It was also noted that being provided with clear instructions about who to contact when medication administration problems arise between clinic appointments would be helpful.
Hierarchical Category 2: Practical Medication Adherence Support
Caregivers noted the importance of being provided with support about how to organize, prepare, measure, and administer their child's outpatient medications. This category included six themes described below.
Preparing and Administering Medication
In a 48-hr practice period before discharge, caregivers were fully responsible for medication administration under the supervision of the medical team. Caregivers appreciated this hands-on training as it increased their confidence about administrating their child's medications independently and recommended it for future families. A few caregivers also suggested that it would be helpful to encourage future caregivers to take on a more hands-on role in their child's medication administration earlier in the hospital admission. A few caregivers who had significant medication administration experience prior to their child's HCT admission expressed a desire to be able to demonstrate mastery in a less burdensome fashion.
Developing Medication Administration Systems
Some caregivers received medication organization suggestions from their home care nurse before leaving the hospital or during a home visit after discharge. All caregivers who received this support described it as helping them establish their own outpatient medication administration system. Six caregivers reported receiving physical tools at hospital discharge that aided in the development of their medication organization and administration systems (e.g., pillbox, extra syringes, and medication bag/container). All indicated that they were able to establish an effective organization system and routine; however, they noted that this took time and thought it would be helpful for the medical team to initiate conversations about (and provide suggestions for) such systems/routines before discharge. They also expressed an interest in a centralized resource (e.g., booklet, handout, and website) that includes organizational tips from other families of children who received an HCT. They believed such a resource would help future caregivers trial different options independently to identify what works best for their family.
Strategies to Encourage Children to Take Medication
Caregivers reported that the most difficult aspect of managing outpatient medications was getting their child to consume medication. Medication administration was hindered by refusal (e.g., spitting out medication), poor taste, pill swallowing difficulties, and aversive side effects (e.g., nausea). The medical team was described as making efforts to help caregivers address these difficulties; however, some of the suggestions provided were perceived as more helpful than others. Caregivers particularly appreciated suggestions for improving medication taste and addressing modality issues (e.g., providing options to switch bad-tasting liquid medications to nasogastric administration or pill form). Behavior management suggestions, such as establishing behavior plans, using reinforcement, and increasing child autonomy (e.g., allowing the child to choose who administers the medication), were also appreciated; however, some caregivers opted to address behavioral challenges independently as they reported knowing their child best. Caregivers expressed interest in receiving behavioral management resources to learn strategies that they can then try on their own. They also suggested for a resource to include behavioral management strategies used by caregivers of children who previously underwent HCT.
Managing Medication Refills
Five caregivers noted that future families could benefit from assistance with organizing outpatient medication refills. Specific suggestions included reminders to request refills and help with advocating for insurance companies to refill medications prior to them running out and assistance with establishing mail-delivery of medications. Two caregivers indicated that it would be helpful to add information about when their child's medication should be due for a refill on the medication list they are given at hospital discharge.
Information From Other Families
When caregivers encountered issues with medication administration (e.g., child disliking the taste or struggling with pill swallowing), several found it helpful to seek out suggestions from other caregivers. Five thought it would be helpful, when preparing for discharge, to be provided a resource of complied tips from caregivers who had previously navigated pediatric HCT. They explained that this resource would help caregivers engage in trial and error to identify the most useful medication strategies for their child. Suggestions of topics included improving medication taste (e.g., mixing medicines with beverages), managing child medication refusal (e.g., rewards), medication organization strategies (e.g., central location), medication administration strategies (e.g., asking for extra syringes when leaving the hospital), and managing unexpected administration barriers develop (e.g., child vomits shortly after medication administration). Suggested formats for this resource included written material (e.g., handout or booklet) or website. Caregivers expressed a desire for this resource to be vetted by their child's medical team and be specific to the institution's pediatric HCT practices.
Tailoring Support to Individual Families
Fourteen caregivers noted the importance of tailoring medication adherence supports to each family's specific needs. For instance, families who experience specific medication administration barriers may benefit from tailored supports to address those identified concerns.
Card Sort Task Results
Results for types of medication adherence support that caregivers received and recommended for future HCT families are presented in Tables 4–6. The frequency of received support varied across support types. The two forms of support caregivers most frequently endorsed receiving were: (a) training on how to measure medications and (b) education about the purpose of their child's prescribed medications. Few caregivers reported receiving support with medication organization, injections, and pill swallowing. Regarding recommended supports for future HCT families, 72% of caregivers believed that all but two assessed domains of medication adherence support may be helpful. Assistance with refilling medications and managing side effects were endorsed at a lower rate, although 50% of caregivers identified these supports as potentially being useful for future families. Caregivers most commonly recommended that adherence support be provided during the inpatient stay (particularly in the days right before discharge) or during outpatient visits. Caregiver preferences regarding the team member to provide support varied across types of support with nurses and nurse practitioners being the most frequently endorsed. Child life was frequently suggested for helping with managing behavioral, emotional, and procedural barriers (i.e., refusal, fear of injections, improving bad taste, and learning pill swallowing). Caregivers also indicated that pharmacists may be helpful in learning the purpose of medications, how to measure them, and when to administer them. Caregiver recommendations for specific medication management tools were: printed medication lists (n = 20), printed calendars (n = 16), resources of tips and tricks from other HCT families (website, n = 12; handout, n = 12; booklet, n = 14), pill boxes (n = 11), and medicine bags (n = 1).
Discussion
Study results show that many of the current medication adherence supports provided by the medical team are perceived as helpful by caregivers after pediatric HCT, with a few areas of potential improvement. Findings reflect caregivers preferring medication adherence support to prioritize frequent, clear, and open communication between them and the medical team. Furthermore, communication materials (e.g., medication lists and calendars) can optimize caregivers’ retention of the large amount of information required for optimal medication adherence. Findings are consistent with previous research showing that caregivers’ medication knowledge and increased collaboration with medical providers are important for facilitating medication adherence (Hoegy et al., 2019; Morrison et al., 2018).
Caregivers expressed two main recommendations to improve communication. First, caregivers felt that communication support tools could be strengthened by including information about the purpose of medications, flexibility in timing of dosing, side effects to monitor, and an action plan for who to contact in the case of an administration challenge. They also thought a list of potential questions to ask medical providers about medications would be helpful. Caregivers differed in their preference of format for such tools, suggesting that tailoring for individual families may be beneficial. Electronic versions may be particularly useful in pediatric HCT as medications are frequently adjusted between outpatient appointments; the electronic format would allow medical providers to update medication lists or tracking tools remotely to reduce any potential communication barriers. Readers are referred to Carmody et al. (2019) as well as Psihogios et al. (2020) for an empirically guided framework for identifying applications that may be useful to trial in the pediatric HCT population.
Second, caregivers reported feeling overwhelmed and uncertain of what to expect when assuming full responsibility for their child's outpatient medications. Consequently, they suggested for members of the medical team to initiate conversations about medication management both prior to and after hospital discharge. This suggestion was reflected in both qualitative interviews and the card sort questionnaire. Caregivers specifically recommended prioritizing frequent check-ins about medication administration challenges during the period prior to and just following discharge when they are developing their own systems, and then gradual spacing out of these check-ins based on caregiver needs. Caregivers indicated that nurses and nurse practitioners may be particularly equipped to have such conversations with them. This suggestion is particularly promising for the specific structure of our HCT program as nurses and nurse practitioners are the members of the medical team with whom families have the most consistent interaction (both inpatient and outpatient) and they possess specialized medication knowledge.
Findings also reflect that practical medication adherence supports should be tailored based on individual family needs. This is consistent with previous HCT research reflecting adherence rates and barriers to differ between and within families (Chardon et al., 2022; McGrady et al., 2014; Morrison et al, 2018). Identification of which supports may benefit each family could be achieved through the ongoing assessment of medication adherence barriers, particularly during the acute phase following hospital discharge. For instance, since analyzing these findings, our institution has begun piloting administering a standardized medication adherence barriers questionnaire every month after families discharge from the hospital in order to identify adherence barriers as they arise. Caregivers in the current study reported often problem-solving medication adherence challenges independently but acknowledged that having a resource to facilitate this process would be helpful. For example, being provided a resource that complied tips for addressing medication adherence barriers from other pediatric HCT caregivers’ lived experience (e.g., tips to improve medication taste, medication refusal, or medication organization). Preference for the format of such a resource (e.g., written handout, booklet, and website) varied between caregivers; therefore, individual institutions may consider involving stakeholders within their given service if interested in developing such a resource.
Limitations of the current study should be acknowledged. Findings may be limited in generalizability as this study included a small sample with limited racial and ethnic diversity from a highly resourced hospital. Additionally, children aged 12 years and younger were included given the prevalence of HCT in this population (Health Resources and Services Administration, 2018); however, medication adherence is also challenging for adolescents and young adults (AYA; McGrady et al., 2014; Morrison et al., 2018). The findings from the current study likely have limited relevance to the AYA population as they are challenged with allocating treatment responsibilities between patient and caregiver and developmentally specific barriers (e.g., striving for autonomy). Additional research is needed to examine the preferences of the AYA population to inform interventions. Future medication adherence promoting intervention development research may also benefit from discussing perspectives about medication adherence support needs from other stakeholders (i.e., patients, medical team members).
Results have important clinical implications for facilitating medication adherence in the pediatric HCT population. Medication adherence promotion efforts should continue to prioritize clear and open communication about medications that are supported by communication tools, which could be strengthened with the content discussed above. Clinic-based medication adherence interventions that include systematic screening of barriers, particularly during the initial months after hospital discharge, would be helpful to facilitate conversations and problem-solving around identified barriers. Additionally, caregivers may particularly appreciate a resource of tips from other caregivers to assist them with problem-solving medication barriers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant number: NICHD T32 HD 68233-7).