
Abstract
The purpose of this article is to further develop the concept of family-centered care (FCC) in childhood cancer using Rodgers’ evolutionary method of concept analysis. A search of the existing literature related to the overarching concept of FCC revealed several concept analyses specific to hospitalized children and children with chronic illness; however, none of these were specific to children with cancer. Five defining attributes of FCC in childhood cancer were identified through this concept analysis: ripple effect, customized care, family functioning, collaboration, and communication. A definition of FCC in childhood cancer is offered based on identified characteristics of the concept. Findings of this concept analysis provide a starting point for on-going development of the concept of FCC in childhood cancer and may facilitate more rigorous nursing studies involving FCC in childhood cancer.
The experience of receiving a childhood cancer diagnosis is life-changing for the family unit (Barrera et al., 2016; Popp et al., 2015; Salvador et al., 2019, 2020). With current family structures ranging from traditional nuclear, blended units, multigenerational, and beyond, the ripple effects of a cancer diagnosis in childhood are far-reaching and unanticipated (Crespo et al., 2016; Mooney-Doyle et al., 2020). Families undoubtedly experience a wide range of feelings when faced with a childhood cancer diagnosis. For pediatric oncology nurse researchers and clinicians, caring for the psychosocial needs of children and their families is as important as dealing with the biomedical needs of the patient (Barrera et al., 2016). To meet the myriad of needs that families of children diagnosed with cancer have, nurses may take on a family-centered approach (Mooney-Doyle et al., 2020). Family-centered care (FCC) is a widely adopted perspective in nursing (Mikkelsen & Frederiksen, 2010) and other health disciplines as this approach acknowledge the multifaceted biopsychosocial needs of children and their families in pediatric oncology (Mooney-Doyle et al., 2020).
While FCC has been widely incorporated into the care of pediatric oncology patients internationally, the concept of FCC in childhood cancer is poorly defined and implemented (Crespo et al., 2016). Variation exists in the delivery of FCC in childhood cancer across disciplines as well (Foster, 2015; Mikkelsen & Frederiksen, 2010; O’Connor et al., 2019). Mooney-Doyle et al. (2020) confirm that despite the ongoing study of FCC in childhood cancer over the last several decades, the concept remains ill-defined and inconsistently implemented in health care. Clinicians’ and researchers’ definitions of FCC in childhood cancer are varied and include FCC as an approach to patient care, as a philosophy, and as a conceptual model (Mooney-Doyle et al., 2020). According to Mooney-Doyle et al. (2020), “Family-centered care (FCC) is a philosophy and an approach to care that provides a pathway to engage with children and their families during their experience with cancer.” (p. 7) In pediatric oncology nursing research and practice, there is an incongruence between conceptualization and operationalization of the concept of FCC in childhood cancer (Barrera et al., 2016). Recently, nursing scholars have developed an FCC in pediatric oncology conceptual framework to help guide clinicians as they interact with and care for families of children with cancer (Mooney-Doyle et al., 2020). Pediatric nurses can use a family-centered approach to patient care to better assist children and their families as they attempt to navigate the difficult childhood cancer journey.
The purpose of this article is to further develop the concept of FCC in childhood cancer using Rodgers’ evolutionary method of concept analysis. In a search of the existing literature related to the overarching concept of FCC, several concept analyses specific to hospitalized children and children with chronic illness (Mikkelsen & Frederiksen, 2010; O’Connor et al., 2019; Smith, 2018) were located, however, none of which were specific to children with cancer. Given the unique attributes and needs of this population (Davis et al., 2017) along with the lack of conceptual clarity in research and practice (Barrera et al., 2016), the development of the concept of FCC in childhood cancer is needed.
Definition of Concept
Prior to undertaking an analysis of a concept, it is important to establish a working definition for the term concept. Rodgers (2000) defines a concept as “a cluster of attributes.” (p. 83) Concepts are best considered as mental representations or abstractions of a phenomenon. According to Rodgers, concepts are dynamic and are influenced by social, cultural, and contextual factors over time. Additionally, they emphasize that individuals use words to express or represent concepts; however, the words themselves are not the concepts (2000).
Preanalysis Definition of FCC in Childhood Cancer
The Institute for Patient- and Family-Centered Care (IPCC) defines patient- and family-centered care (PFCC) as “an approach to the planning, delivery, and evaluation of health care that is grounded in mutually beneficial partnerships among health care providers, patients, and families” (Institute for Patient- and Family-Centered Care [IPCC], n.d., para. 1). IPCC designates the core concepts of PFCC as dignity and respect, information sharing, participation, and collaboration (IPCC, n.d.). While this definition clarifies the overarching concept of PFCC, it does not take into consideration-specific contexts such as childhood cancer. The nature of PFCC may change based on specific contexts such as setting and time.
Guiding Principles
Rodgers’ model of concept analysis is unique among other frameworks as it is cyclical and iterative in nature. In addition, the evolutionary method holds that concepts develop in relation to specific contexts and through time. The significance, use, and application of a given concept may evolve according to disciplinary, social, cultural, and theoretical contexts across a period of time (Rodgers, 2000). While not necessarily linear in implementation, activities included in Rodgers’ evolutionary method include identification and naming of the concept of interest; identification of surrogate terms and related concepts; selection of an appropriate realm for data collection; collection and analysis of data relevant to the identification of attributes, antecedents, consequences, and contexts; identification of an exemplar or model case of the concept as appropriate; and identification of implications for additional development of the concept (Rodgers, 2000). Examination of each of these activities as they relate to the concept of FCC in childhood cancer will be described throughout this article.
Data Sources
According to Rodgers (2000), the first step in the process of concept analysis is identification of the concept. The concept of FCC in childhood cancer was identified during the initial exploration of existing literature specific to pediatric oncology nursing. Following identification of the concept to be developed, the setting of electronically indexed databases was chosen. In accordance with Rodgers’ recommendation, a well-defined search strategy was implemented (2000).
A preliminary search of the literature using electronic databases revealed that FCC in childhood cancer is a relevant concept in medicine, nursing, psychology, social sciences, and genetics. As Rodgers’ method prescribes that the researcher consider how the concept is defined across disciplines (2000), databases that include publications within these areas were identified and utilized to identify the sample. A search of PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Scopus, and Web of Science was conducted in November 2021 using a combination of the key search terms, “family-centered care,” “cancer,” “child,” “pediatric,” and “oncology.” The initial search of the databases using these terms yielded 4,389 results. To arrive at a manageable sample (Rodgers, 2000), searches were limited to those that were English language publications, peer-reviewed, available in full-text, and dated from November 2011 to November 2021. This timeframe was chosen in acknowledgment of the evolution of what society at large defines as “family” over the last decade (Mooney-Doyle et al., 2020; Toruner & Altay, 2018) and interest in how the concept has evolved in recent years. Redefinition of the concept of family impacts FCC in childhood cancer in practice as well as research involving it. Applying limits to the search resulted in 180 articles of which the titles and abstracts were reviewed to determine the role of FCC in childhood cancer within the article. Abstracts wherein FCC in childhood cancer was not a prominent aspect were discarded (Rodgers, 2000), resulting in 30 articles remaining. Upon full-text reading of the remaining articles, three additional articles were discarded as FCC in childhood cancer was not central to the article. A total of 27 articles were included in the final sample, 10 of which were specific to the field of nursing (Branowicki et al., 2016; Davis et al., 2017; Gil et al., 2016; Jestico & Finlay, 2017; Long et al., 2015; Lyu et al., 2019; Popp et al., 2015; Pyke-Grimm et al., 2019; Ringnér et al., 2013; Toruner & Altay, 2018).
As noted in guiding principles, Rodgers’ method of concept analysis was further implemented to identify surrogate terms, related concepts, attributes, antecedents, and consequences of FCC in childhood cancer. To avoid premature closure and influence of researcher bias, formal analysis was delayed until near the end of the process. This delay allowed for characteristics of the concept to emerge naturally from the dataset without influence of researcher bias (Rodgers, 2000). The findings of the analysis were synthesized to develop a refined definition of the FCC in childhood cancer.
Findings
Surrogate Terms
During the initial stages of data collection several surrogate terms, defined by Rodgers (2000) as other words or phrases that are often used to describe the concept, were identified. The phrases family-based care (Toruner & Altay, 2018) and family-oriented care (Ringnér et al., 2013) were used interchangeably with the term family-centered care. Additionally, the phrases pediatric oncology (Davis et al., 2017; Garcia et al., 2017; Gerhardt et al., 2015; Gil et al., 2016; Pyke-Grimm et al., 2019; Ringnér et al., 2013; Salvador et al., 2020; Sisk et al., 2021) and pediatric cancer (Barrera et al., 2016; Branowicki et al., 2016; Crespo et al., 2016; Salvador et al., 2019, 2020) were used frequently as substitute terms for childhood cancer.
Related Concepts
According to Rodgers (2000), related concepts “bear some relationship to the concept of interest but do not seem to share the same set of attributes” (p. 92). During the initial search of existing literature to identify the concept of interest, several analyses of the concept of family-centered care were identified (Mikkelsen & Frederiksen, 2010; O’Connor et al., 2019; Smith, 2018). However, these FCC analyses were conducted using a broad sample of hospitalized children and young adults while the current concept analysis is specific to children with cancer. As will be described in this article, attributes and consequences of FCC within this specific context are comprised of characteristics similar to but different from FCC as a general concept (Davis et al., 2017). Davis et al. (2017), Siembida et al. (2018), and Pyke-Grimm et al. (2019) also describe the related concept of patient-centered care in their recent works as associated with yet not directly the same as FCC. Identification of these related concepts underscores the philosophical assumption that all concepts exist in a network, from which significance and context of each concept can be derived (Rodgers, 2000).
Attributes
Rodgers’s evolutionary method involves the researcher's unbiased review of the sample for statements relevant to characteristics of the concept (2000). According to Rodgers (2000), “identification of the attributes of the concept represents the primary accomplishment of the concept analysis” (p. 91). Several common features of FCC in childhood cancer emerged from the sample during full-text analysis. These themes were coded according to similar characteristics and grouped into attributes and sub-themes upon subsequent full-text readings of the articles. Five defining attributes of FCC in childhood cancer were identified from the data: ripple effect, customized care, family functioning, collaboration, and communication.
Ripple Effect
Healthcare providers’ recognition of the ripple effect a diagnosis of childhood cancer has on the family was distinct in most of the articles reviewed in the current concept analysis (Barrera et al., 2016; Crespo et al., 2016; Garcia et al., 2017; Gerhardt et al., 2015; Jestico & Finlay, 2017; Livingston et al., 2020; Long et al., 2015; Popp et al., 2015; Ringnér et al., 2013; Salvador et al., 2019, 2020; Toruner & Altay, 2018; van Bindsbergen et al., 2021; Wakefield et al., 2012; White et al., 2017). The ripple effect was garnered by families’ experiences of uncertainty (Branowicki et al., 2016; Crespo et al., 2016; Salvador et al., 2020; Wakefield et al., 2012) related to their child receiving a life-threatening medical diagnosis, patient outcomes, and impact on family functioning. For example, Salvador et al. (2020) describe emotional reactions and confusing medical information compounded with uncertainty about the child's future as part of the complexity of pediatric cancer.
Crespo et al. (2016), Salvador et al. (2019), Popp et al. (2015), Salvador et al. (2020), and Ringnér et al. (2013) spoke to the immense challenges parents specifically face when their child receives a cancer diagnosis. Specifically, parents question their self-efficacy (Salvador et al., 2019), experience caregiver burden (Crespo et al., 2016), and struggle with decision-making regarding their child's care (Salvador et al., 2020). Additionally, Long et al. (2015), White et al. (2017), and Gerhardt et al. (2015) provided insight into the significant stresses experienced by siblings of children diagnosed with cancer. Generally, siblings felt excluded (White et al., 2017) and experienced anxiety, depression, and lower quality of life (Gerhardt et al., 2015; Long et al., 2015). The breadth and depth of the ripple effect were also influenced by cultural (Garcia et al., 2017; Lyu et al., 2019; Toruner & Altay, 2018), linguistic (Garcia et al., 2017), and spiritual (Livingston et al., 2020) contexts.
Customized Care
Customized care was a common theme throughout existing literature on the concept of FCC in childhood cancer (Crespo et al., 2016; Garcia et al., 2017; Gerhardt et al., 2015; Gil et al., 2016; Lyu et al., 2019; Mooney-Doyle et al., 2020; Popp et al., 2015; Salvador et al., 2020; White et al., 2017). Gerhardt et al. (2015) recommended flexibility in care-planning that is considerate of each family's unique environment, lifestyle, and circumstances. Findings by Salvador et al. (2020) reaffirm the necessity of pediatric oncology clinicians to provide customized care and reject the one-size-fits-all approach when caring for families who have a child diagnosed with cancer. Families’ varied psychosocial and emotional (Barrera et al., 2016; Crespo et al., 2016; Long et al., 2015; Popp et al., 2015; White et al., 2017), cultural (Garcia et al., 2017; Lyu et al., 2019; Toruner & Altay, 2018), spiritual (Livingston et al., 2020), and linguistic (Garcia et al., 2017; Gil et al., 2016) needs support the imperative for health care providers to adopt a tailored approach to care in pediatric cancer.
Family Functioning
Family functioning, including the interactions, relationships, conflicts, and adaptations of families and individual family members was central to many of the articles under review (Barrera et al., 2016; Branowicki et al., 2016; Crespo et al., 2016; Garcia et al., 2017; Gerhardt et al., 2015; Long et al., 2015; Lyu et al., 2019, 2020; Pyke-Grimm et al., 2019; Rensen et al., 2019; Siembida et al., 2018; van Bindsbergen et al., 2021; White et al., 2017). When considering family functionality, several authors emphasized the importance of acknowledging the family as a system as well as individual members (Barrera et al., 2016; Garcia et al., 2017; Gerhardt et al., 2015; Long et al., 2015; Pyke-Grimm et al., 2019; Siembida et al., 2018). According to Long et al. (2015), “A child's cancer diagnosis can be a devastating event that leads to emotional strain and substantial changes in the day-to-day functioning of the family … which can chronically disrupt the family system” (p. 21). Clinicians should bear this information in mind when engaging with families of children diagnosed with cancer.
Many authors integrated health care providers’ knowledge and understanding of families’ psychosocial and emotional needs as integral to helping families maintain functioning (Barrera et al., 2016; Long et al., 2015; Lyu et al., 2019; McCarthy et al., 2018; Ringnér et al., 2013; White et al., 2017; Yu et al., 2014). Yu and colleagues reported that a family-centered nursing care model that included psychological and social interventions to have improved the quality of life of children with brain tumors (2014). In addition, Livingston et al. (2020) recommended that psychosocial care be provided for not only children with cancer but also their families, to improve quality of life.
Coping and adaptation (Long et al., 2015; Lyu et al., 2019, 2020) also emerged as sub-themes of the attribute family functioning. Lyu et al. (2020) found that how well a family adapts to a stressful life event is largely dependent upon how well the family copes with the event. In an earlier study, Lyu et al. found that coping strategies used by families are often determined by the parents of the family (2019). Additionally, Long et al. (2015) describe siblings’ experiences of coping with and adapting to life after their brother or sister received a diagnosis of cancer as tenuous.
By recognizing the family as a unit as well as individual members and acknowledging the psychosocial, emotional, and coping needs of families of children diagnosed with cancer, health care providers may be better equipped to effectively deliver FCC in childhood cancer.
Collaboration
Collaboration among members of families and members of the health care team was a major theme within the existing literature on FCC in childhood cancer (Barrera et al., 2016; Crespo et al., 2016; Davis et al., 2017; Garcia et al., 2017; Gil et al., 2016; Popp et al., 2015; Pyke-Grimm et al., 2019; Salvador et al., 2020; Siembida et al., 2018; Sisk et al., 2020, 2021; Toruner & Altay, 2018). Davis et al. (2017) reported that one of the best predictors of family satisfaction with care provided was staff working together. Additionally, the collaborative approach that emphasizes the family perspective often results in parents feeling validated and comforted during difficult times (Popp et al., 2015). Parents felt empowered in their decision-making when working in collaboration with the healthcare team (Pyke-Grimm et al., 2019; Sisk et al., 2021; Toruner & Altay, 2018). Garcia et al. (2017) and Gil et al. (2016) implemented interdisciplinary, collaborative, family-centered interventions in pediatric oncology that resulted in the establishment of supportive relationships among families and the health care team.
Other authors described collaboration from the perspective of partnership (Pyke-Grimm et al., 2019; Salvador et al., 2019, 2020). Salvador et al. (2020) describe FCC in pediatric oncology as a collaborative partnership in which families receive support and respect and that encourages families’ involvement in their child's care. Sisk et al. (2021) confirm Salvador et al.'s claims that respect is fostered by a collaborative approach. Additionally, Toruner and Altay (2018), Sisk et al. (2020), and Gil et al. (2016) identified trust as a by-product of collaboration in pediatric oncology. The sub-themes of support, respect, and involvement are congruent with basic tenets of PFCC in general (IPCC, n.d.).
Communication
Communication was identified as a defining attribute of FCC in childhood cancer among several articles in this concept analysis (Gerhardt et al., 2015; Jestico & Finlay, 2017; Livingston et al., 2020; Pyke-Grimm et al., 2019; Siembida et al., 2018; Sisk et al. 2020, 2021; White et al., 2017). Sisk et al. (2020) identify prognostic communication as “an essential component of family-centered care in pediatric oncology.” (p. 1) In a follow-up article, Sisk et al. (2021, p. 4957) claim that high-quality communication provides parents of children with cancer peace of mind, trust in physicians, and feelings of acknowledgment and comfort. Parents also felt more confident and empowered in their decision-making when they believed communication was effective and that they were included as part of the healthcare team (Pyke-Grimm et al., 2019; Salvador et al., 2020). The sub-theme of trust emerged in relation to both communication and collaboration (Gil et al., 2016; Sisk et al., 2020; Toruner & Altay, 2018).
Family information needs to be served as a catalyst for communication in many articles (Crespo et al., 2016; McCarthy et al., 2018; Ringnér et al., 2013; Salvador et al., 2019, 2020; Toruner & Altay, 2018; Wakefield et al., 2012; White et al., 2017). McCarthy and colleagues found that adolescent cancer patients and their parents had high levels of need for information and that unmet information need was associated with symptoms of post-traumatic stress (2018). Siblings also reported feeling that they lacked the information needed about their brother's or sister's cancer diagnosis (White et al., 2017). Crespo et al. (2016) suggested that parents are avid information seekers because of their new caregiver role as well as the uncertainty surrounding their child's cancer diagnosis.
Antecedents
Conditions or events that precede FCC in childhood cancer were identified through this concept analysis. The first antecedent that emerged from the data was a child being diagnosed with cancer. Without this antecedent, FCC in childhood cancer would not exist as a concept. All of the articles in the sample were predicated on a child having cancer. Additional antecedents of FCC in childhood cancer were existence of a family and a health care team. These conditions lay the foundation for the development of family–provider partnerships described by several authors (Pyke-Grimm et al., 2019; Salvador et al., 2019, 2020). Additionally, FCC as an approach to patient care appropriate to childhood cancer underscores the philosophical assumption that the family plays an integral role in the child's life (Salvador et al., 2019). Each of these constitutes essential prerequisites to FCC in childhood cancer.
Consequences
The potential consequences of effectively implemented FCC in childhood cancer are immense. However, the consensus among findings from the literature in this sample is that while theoretically FCC in childhood cancer should result in the biopsychosocial needs of individual family members met and family unit functionality being met (Crespo et al., 2016; Lyu et al., 2019; Popp et al., 2015; Salvador et al., 2019, 2020; van Bindsbergen et al., 2021), there is little empirical evidence of the effectiveness of CC in childhood cancer (Crespo et al., 2016; Salvador et al., 2019, 2020). According to Salvador et al. (2019), “Despite the growing body of empirical evidence on FCC and its correlates, there is a lack of research specifically addressing the potential benefits of this approach for parents of children with cancer.” (p. 1927) In a related study on FCC in childhood cancer, Crespo et al. (2016) asserted, “Although FCC is broadly advocated, empirical examination of its benefits for patients and families is surprisingly scarce.” (p. 32) Mooney-Doyle et al. (2020) confirm that limited data exists about the implementation of FCC in pediatric oncology and add that “little intervention research exists to support a core function of FCC: promotion, maintenance, and restoration of the parental role in care of the hospitalized child.” (p. 10)
Garcia et al. (2017) implemented a targeted intervention to address an identified gap in FCC in childhood cancer. According to the authors, cultural and linguistic considerations are a weakness of FCC in childhood cancer in its current state. By integrating a patient consultant-advocate into the collaborative team, Garcia et al. (2017) were able to strengthen FCC in childhood cancer, resulting in improved outcomes for their study population.
Toruner and Altay (2018) provided an encouraging report that there is currently an increasing emphasis on evaluating the benefits of FCC in childhood cancer. This uptick in interest was also noted during data collection for this concept analysis. There was at least a two-fold increase in the number of articles published on the concept in the second half of the data collection timeframe across all four electronic databases. Toruner and Altay also presented inconsistency in quality of care and mechanical interactions of staff as potential negative consequences of FCC in childhood cancer (2018).
Exemplar Case
Unique to Rodgers’s evolutionary method is the identification, not construction, of an exemplar (Rodgers, 2000). Additionally, the exemplar should “illustrate the characteristics of the concept in relevant contexts and, as a result, enhance the clarity and effective application of the concept of interest” (Rodgers, 2000, p. 96). As has been described in the discussion of attributes, FCC in childhood cancer is highly contextual and must be customized to fit each family and its associated members. These circumstances made it difficult to identify a generic and universal exemplar among the sample. An additional field search to identify an exemplar was conducted unsuccessfully. In these situations, Rodgers cautions against presenting an exemplar to avoid premature closure as to not express more conceptual clarity or usefulness of the concept than is appropriate in its current state (2000). An explanation of the limited effective application of FCC in childhood cancer may be due to poorly operationalized definitions of the concept. The incongruence between theoretical and operational conceptual definitions of FCC in childhood cancer warrants further investigation.
Justification of Findings
To the best of my knowledge, there have been no other concept analyses of FCC in childhood cancer. The objective of this novel concept analysis was to develop the concept of FCC in childhood cancer, with the intent to better understand its defining characteristics. While the concept is widely employed in practice, there has been little attention given to its conceptual development. The lack of consistency in application of the concept and limited evidence of its efficacy could be because it has not been fully developed conceptually.
Based on what has been presented in this article, I believe the argument can be made that FCC in childhood cancer holds significance as the literature in this sample displayed that it is used often (Rodgers, 2000). The current concept analysis has provided clarity with regard to the surrogate terms, related concepts, attributes, antecedents, and consequences of FCC in childhood cancer. Identification of these defining characteristics of the concept sets a foundation for future development of the concept and serves as a springboard for future inquiry related to FCC in childhood cancer. Additional study is needed to provide refinement of the concept as it evolves over time and within contexts (Rodgers, 2000). Further concept development may also provide for an exemplar to be identified.
Modified Definition
According to Rodgers (2000), the process of concept development is continuous and involves definition and refinement of the concept over time. While the essence of FCC in childhood cancer may be dynamic within this view, the current analysis has provided a basis for defining the concept. Using my pre-analysis understanding of FCC in childhood cancer along with findings from the current analysis, I offer a modified definition of FCC in childhood cancer for further concept development and foundation for inquiry: FCC in childhood cancer is a contextual, customized approach to the care of families who have a child diagnosed with cancer that involves interdisciplinary as well as family collaboration, communication that addresses family information needs and fosters trust, and that acknowledges the ripple effect of the diagnosis on functioning of the family as a system as well as individual members (Figure 1).
Implications
It is important to note the interdisciplinary nature of FCC in childhood cancer, with two of its attributes being communication and collaboration. Sisk et al. (2021) noted “past studies have shown that some physicians do not feel comfortable addressing emotional needs, whereas nurses and psychosocial professionals view this role as integral to their professional identity.” (p. 4966) The authors go on to describe how nurses and nurse practitioners may find it difficult to deliver troublesome news to families, whereas physicians feel these activities are essential to their role. Sisk et al. (2021) assert that communication with families of children with cancer should be a team endeavor, leveraging the strengths and skills of individual clinicians. I provide this example as an illustration of how FCC in childhood cancer is often viewed as an interdisciplinary, in contrast to disciplinary, concept.
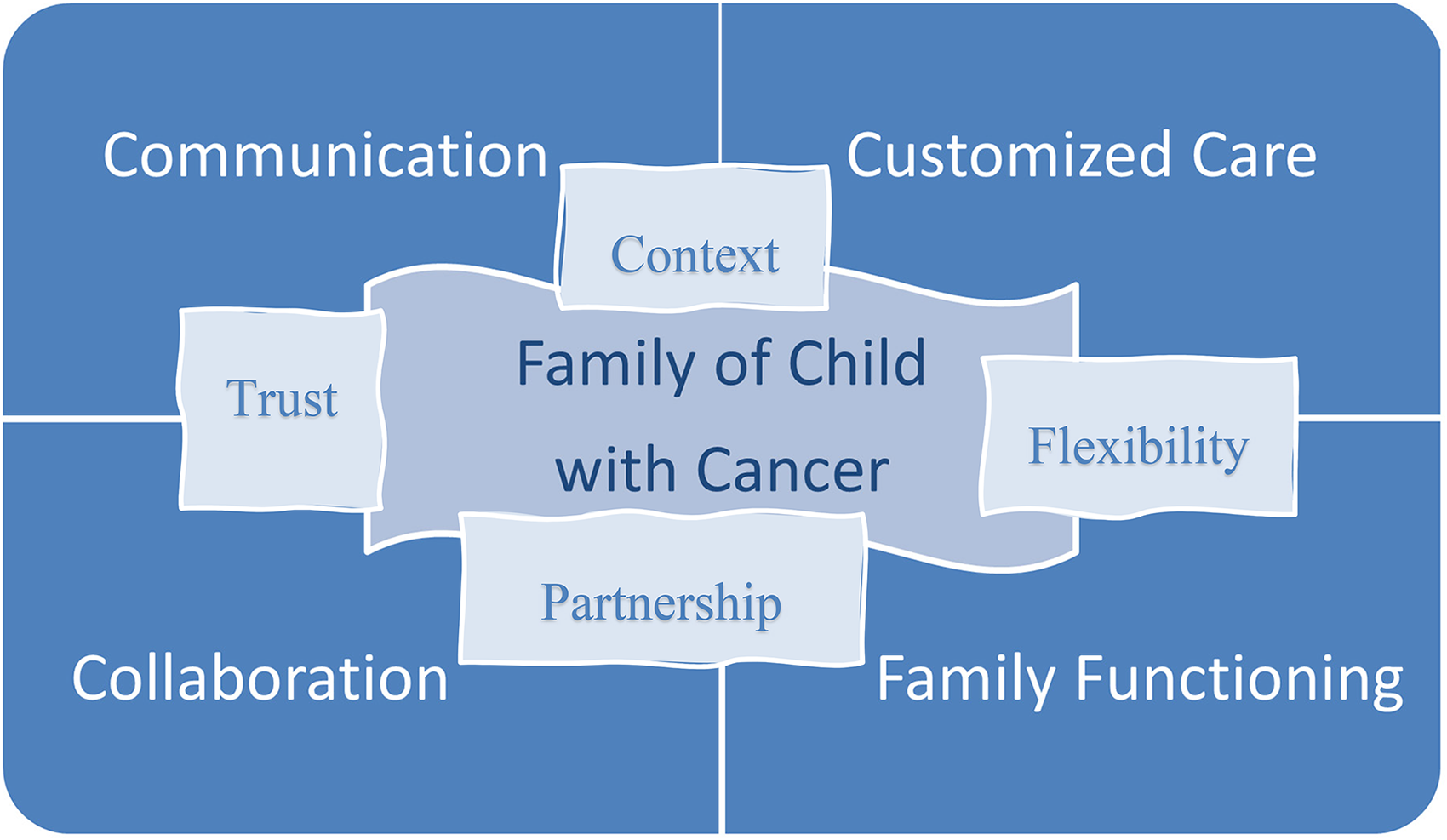
Relational matrix of FCC in childhood cancer.
However, certain aspects of FCC in childhood cancer, namely the ripple effect, customized care, and family functioning, lend themselves well to the discipline of nursing. Based on its influence on other attributes of FCC in childhood cancer, the ripple effect should be viewed as an interwoven attribute that necessitates the family-centered approach in pediatric oncology. The ripple effect is an enmeshed attribute that differentiates FCC in childhood cancer from FCC as a general concept. As is well noted in the literature (Long et al., 2015; Ringnér et al., 2013; Toruner & Altay, 2018) and can be derived from the earlier quote by Sisk et al. (2021), nurses are well-known for their focus on the psychosocial and emotional needs of patients and families. Moreover, nurses have been shown to spend more time providing direct care to patients than their physician and critical support staff counterparts (Butler et al., 2018). This extended exposure offers nurses a unique perspective into the impact of the diagnosis on the patient, parents, siblings, grandparents, community, etc. Nurses are able to gather information on how well the family is coping with and adapting to their new normal. This knowledge is invaluable to the collaborative team when providing FCC in childhood cancer as it allows for care to be customized to meet individual families’ needs.
Future Considerations
Rodgers asserts that the goal of concept analysis is to enhance the clarity of the concept in order to continue to cycle of concept development. This concept analysis provides insight into the current state of FCC in childhood cancer and identifies gaps in the existing knowledge base (2000). In addition, Rodgers (2000) indicates that concept analysis provides direction for further inquiry and future research on the concept of interest and should not be viewed as an endpoint in itself. This analysis of FCC in childhood cancer provides a conceptual foundation for future inquiry which will strengthen research reliability (Rodgers, 2000). Congruent with the philosophical assumptions of Rodgers’ method of concept analysis, continued development of this concept will be necessary across contexts and time (Rodgers, 2000). It is likely that future research will reveal advances in technology as influential to the communication attribute of FCC in childhood cancer. Additionally, culture, geographic location, and language should be examined more closely from the perspective of how they impact customized care. Furthermore, ongoing concept development of FCC in childhood cancer specific to the context of nursing will enhance knowledge unique to the discipline.
Conclusion
Families who have a child diagnosed with cancer face a myriad of challenges but FCC in childhood cancer offers nurses and other health care providers an approach to effectively meet their needs. This concept analysis provides characteristics of FCC in childhood cancer as they currently exist in the medical, nursing, psychology, social sciences, and genetics literature. This initial analysis of FCC in childhood cancer should be viewed as a starting point for what should be a continuous cycle of concept development. Further examination of the unique attributes and consequences of FCC in childhood cancer is integral for the generation of new nursing knowledge specific to this concept.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.