
Abstract
Introduction
Pediatric cancer rates have increased slightly in recent decades but have been accompanied by decreased mortality rates as treatment options, including infusion therapy, have expanded and improved (American Cancer Society, 2021). Infusion therapy is a major portion of pediatric hematology and oncology practice because many patients receive chemotherapy as part of their treatment.
Chemotherapy infusions are often administered in infusion centers built specifically to accommodate unique infusion therapy needs. These centers may include a combination of hospital beds and infusion chairs, nursing stations, medication storage, access to pharmacy resources, and access to emergency response services. Infusion centers are located in outpatient settings that may or may not be based in a hospital.
Many publications have addressed the clinical efficacy of treatment (Ganesan et al., 2019; Hutsell et al., 2017; Mueller et al., 2018) and the costs of pediatric infusion therapy (Yang et al., 2020). However, there is a paucity of research on whether the setting (i.e., inpatient, hospital-based outpatient, or outpatient) affects outcomes, patient safety, or patient satisfaction (Kelly et al., 2014). The literature discusses the need for further research and inquiry (Bolsover, 2018; Fesler & Toms, 2020; Yusef et al., 2017).
At our large, tertiary academic medical center, the hospital-based outpatient Pediatric Infusion Therapy Center (PITC) is located on an inpatient campus that is about 1.7 km (1 mile) from the center's outpatient buildings. The PITC contains three treatment rooms: one room has an infusion chair, one has a hospital bed, and one has two chairs and a hospital bed.
The PITC averages 2,600 to 3,000 patient appointments per year and offers a wide range of infusion therapies, including chemotherapeutic agents and nonchemotherapeutic agents. The outpatient pediatric hematology and oncology practice include 15 physician full-time equivalents (FTEs) who see an average of 500 new patients and 5,000 outpatients each year.
The COVID-19 pandemic has greatly affected how care is provided to children, especially in the PITC. Patient capacity was immediately decreased by 40% because physical distancing is not possible in the treatment room with two chairs and a hospital bed. The pandemic also exacerbated some additional constraints facing the PITC and increased the number of pediatric infusions administered in environments that were not ideal, such as the general pediatric inpatient unit and the adult infusion therapy center.
In response to these challenges, a multidisciplinary team was formed to investigate the use of outpatient clinic examination rooms for pediatric infusions. Our aim was to improve patient and family satisfaction and reduce the amount of time in an appointment itinerary without negatively impacting patient safety.
Description of Process or Innovation
Our team selected therapies most appropriate for administration in an outpatient setting. The new workflow was then designed and tested with a two-phase pilot. Each member of the multidisciplinary team had unique responsibilities that contributed to the success of the project.
Therapy Selection
The multidisciplinary team first reviewed all the infusion therapies offered in the PITC. The team stratified those therapies into groups according to the number of medications included in therapy, the time required to infuse the medication(s), and the potential for adverse reactions.
Workflow Design
The team worked to redesign the infusion administration workflow into a process that would fit the new infusion location. Figure 1 shows a comparison of a standard patient itinerary before and after the workflow redesign. Before this project, patients were required to see their physician or advanced practice provider in an outpatient clinic and then travel to the hospital-based PITC for their infusion. The new process eliminated the travel because the infusion was administered in the same outpatient clinic examination room where the appointment with the physician or advanced practice provider occurred.
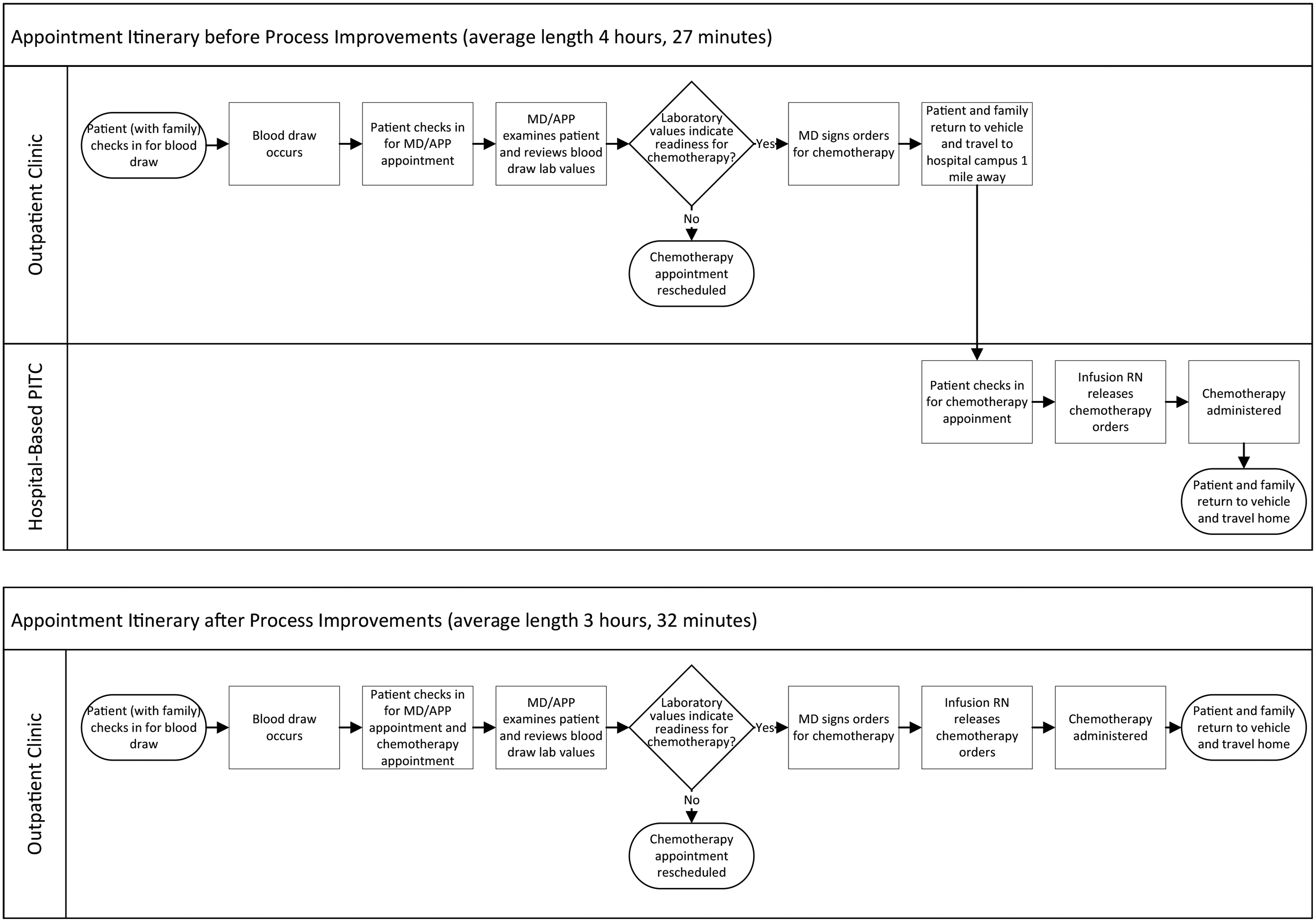
Flowcharts showing appointment itineraries. (Upper) Before process improvements, the average time for the appointment itinerary was 4 hr and 27 min. The distance from the outpatient clinic to the hospital-based Pediatric Infusion Therapy Center (PITC) is about 1.7 km (1 mile). (Lower) After process improvements, the average time for the appointment itinerary was 3 hr and 32 min.
Two-Phase Pilot
Our team used a two-phase approach that allowed us to start small and learn from the first trial. This helped inform how to design the next phase and the final future state.
Phase 1
Five unique medications and six total therapies were selected for phase 1 of the pilot (Table 1). These were selected because they carried a low risk of adverse reactions and they required only a short infusion time for administration. The duration of this phase was 3.5 months, during which 25 unique patients received a total of 52 infusions. The project team met regularly throughout phase 1 to address any immediate concerns and to discuss any practice or workflow changes that were needed.
Infusion Therapy Offerings During Phase 1 of the Pilot
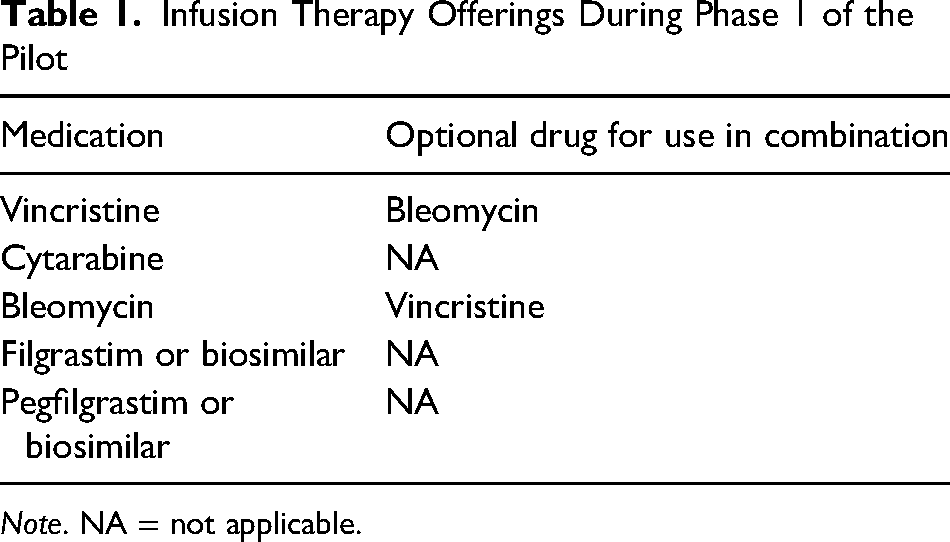
Note. NA = not applicable.
Phase 2
After a preplanned interim analysis, the results of phase 1 were shared with departmental and organizational leadership, and 12 additional therapies, including six additional unique medications, were approved for phase 2 of the pilot. In total, 11 unique medications and 18 therapies were offered in the outpatient examination area (Table 2). Phase 2 lasted for 5 months, during which an additional 132 infusions were administered to an additional 24 unique patients.
Infusion Therapy Offerings During Phase 2 of the Pilot
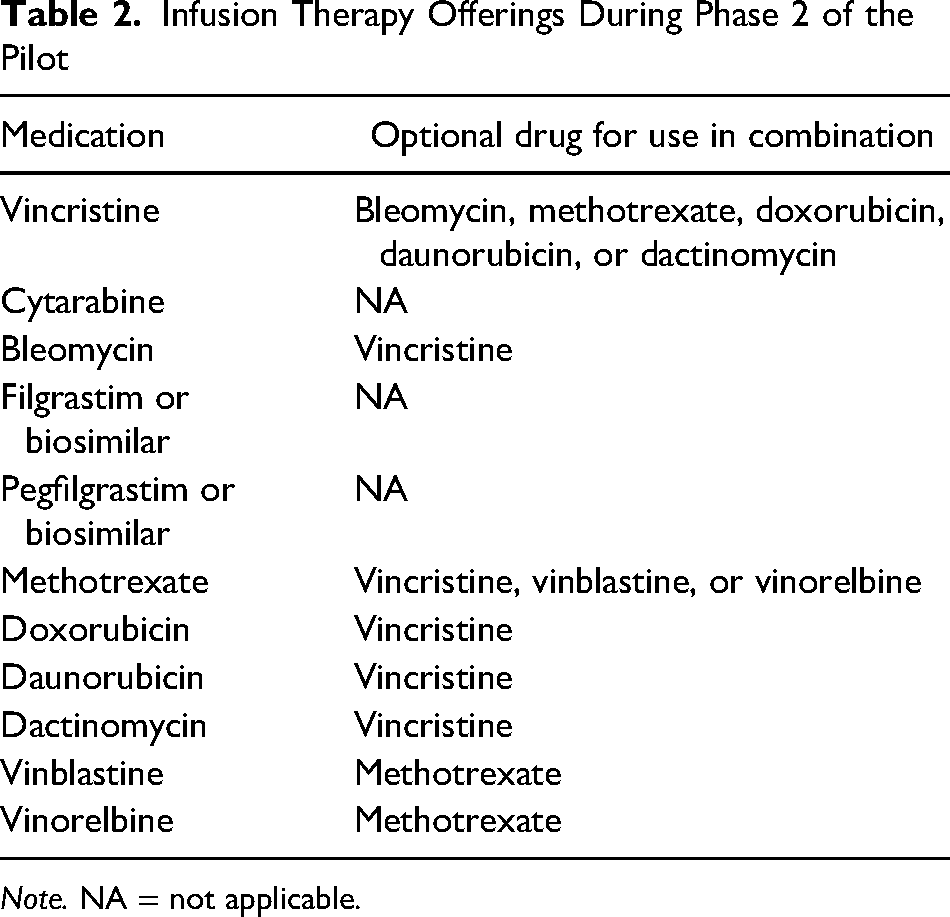
Note. NA = not applicable.
Multidisciplinary Project Team
The project team consisted of representatives from inpatient nursing, outpatient nursing, infusion therapy nursing, pediatric and adult pharmacy, infusion therapy physician leadership, pediatric hematology and oncology (physicians), operations management, and health systems engineering. Each team member filled a unique and valuable role in helping this project progress.
Nursing
Ambulatory pediatric hematology and oncology registered nurse care coordinators (RNCCs) were key stakeholders in the design, implementation, and success of the pilot. The RNCCs all had prior experience administering chemotherapy infusions in the PITC. They attended meetings as active participants, shadowed colleagues in the adult and pediatric infusion therapy centers, and attended chemotherapy education and a skills-assessment laboratory to ensure competency in best practice. The tiered system acquisition model was used for orientation, and a chemotherapy-trained preceptor observed and provided just-in-time feedback to the RNCCs as chemotherapy was administered and documented (Joswiak, 2018).
Further, in collaboration with nursing leadership, the RNCCs reviewed protocols and guidelines for chemotherapy administration, identified equipment needs and personal protective equipment required for administration, and worked with environmental services personnel to learn disposal processes for hazardous medications. Two examination rooms were selected for chemotherapy infusions, and supplies, equipment, personal protective equipment, and a chemotherapy spill kit were made readily available. After the implementation of the pilot, infusion therapy leadership audited the RNCCs’ documentation and billing for accuracy.
An infusion therapy calendar was created with available appointments for RNCCs who had completed chemotherapy competency assessments. During the pilot, four additional nurses completed their chemotherapy education and competency assessment and were added to the pool of those available to administer chemotherapy. Over time, the additional RNCC staff and the efficiencies gained through experience allowed for additional infusion therapy appointments and increased availability of chemotherapy agents, further meeting the needs of patients and their families.
Pharmacy
Pediatric-trained pharmacists provided direction on potential drug reactions and equipment needed to offer infusions in the new location. They also ensured competence of adult-trained pharmacists and pharmacy technicians because medications used for pediatric infusion therapy in the outpatient clinic would need to be processed, prepared, and dispensed by adult chemotherapy infusion center pharmacy staff. Pharmacy staff were informed of the coming changes in advance so that questions about competence or confidence related to the change could be addressed. Additionally, a clinic-based pediatric hematology and oncology pharmacist was available for support and facilitation of timely ordering of the infusion therapies.
Physicians
Physicians on the team included the PITC medical director and the chair of the pediatric hematology and oncology practice. These physicians offered their expertise on clinical issues such as therapy offerings and potential future demand for therapies. In addition, the PITC medical director was instrumental in presenting the case for these changes to operational and clinical leadership.
Operations Management
Operational leaders helped resolve problems related to space needs for outpatient infusions and scheduling complexity.
Health Systems Engineering
A health systems engineer assisted with workflow design, data analysis, and project management.
Results
Throughout both phases of the pilot our team tracked multiple metrics related to patient safety, efficiency, and patient satisfaction. These data were compared with baseline data captured from the 3.5 months immediately preceding the pilot. All metrics showed improvement. No harm came to any patient who received an infusion, and patient appointment itineraries were shortened, allowing sick patients to return home sooner. Satisfaction survey responses indicated a clear preference for the new process.
Patient Volumes
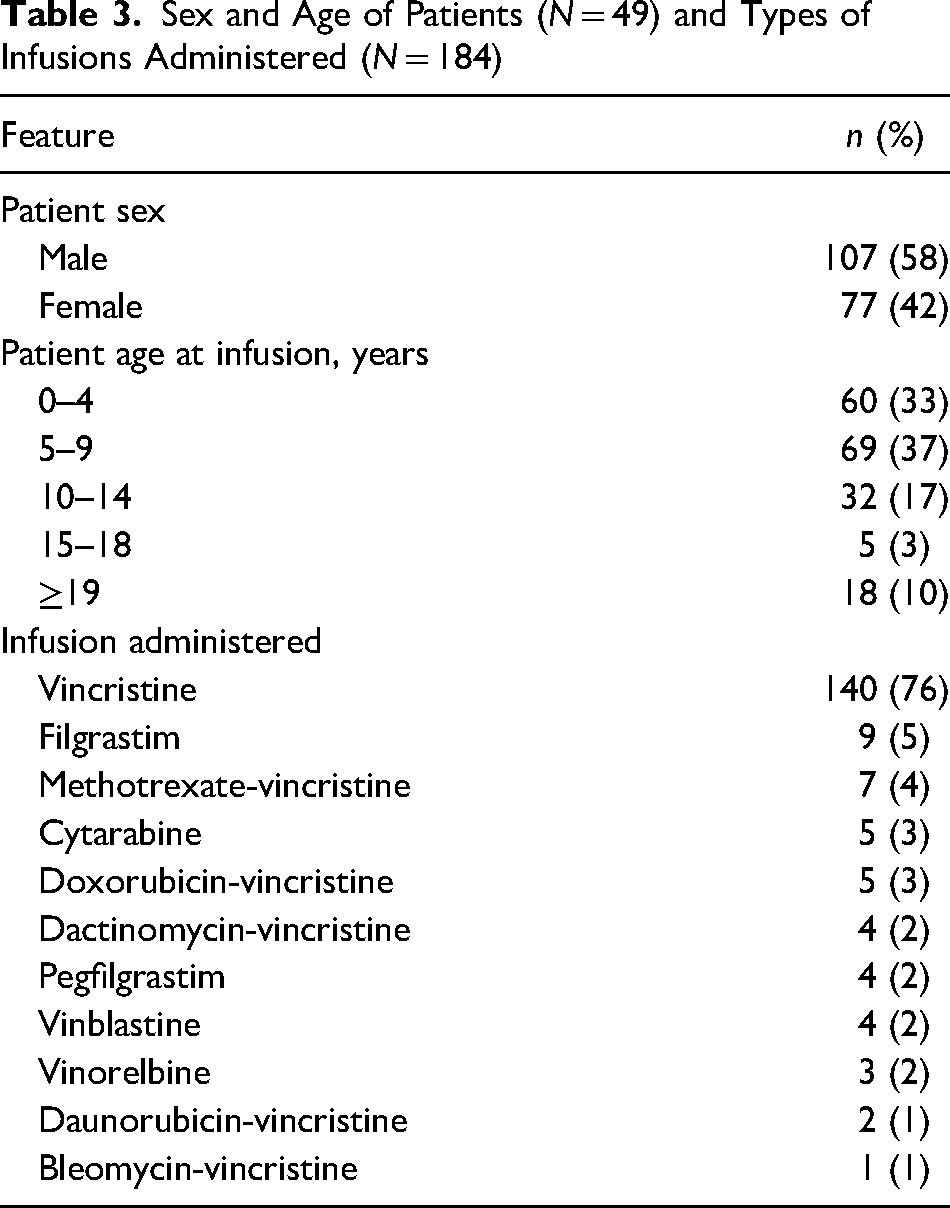
Throughout the 8.5-month pilot, a total of 184 infusions were administered to 49 unique patients (Table 3).
Sex and Age of Patients (N = 49) and Types of Infusions Administered (N = 184)
Patient Safety
The safety culture at our organization encourages diligent safety practices and prompt incident reporting whenever a patient safety incident occurs. During the pilot, no safety events related to infusions administered in the outpatient examination rooms were reported to the organization's incident-tracking system. This matched the incident report rate for the PITC in the 3 months preceding the pilot, so patient safety was not negatively affected by the new workflow.
Efficiency
Appointment Itinerary Duration
To measure the impact of this project on the duration of patient appointment itineraries, we searched for patients who received the same therapy at both the PITC and the new outpatient location in the period before the pilot and during the pilot. Figure 2 shows a comparison of appointment itinerary durations between the infusion locations for itineraries that did include lumbar puncture and itineraries that did not. Appointment itinerary durations were decreased by nearly an hour for both groups of patients. This allowed patients and families to return to their daily lives sooner.
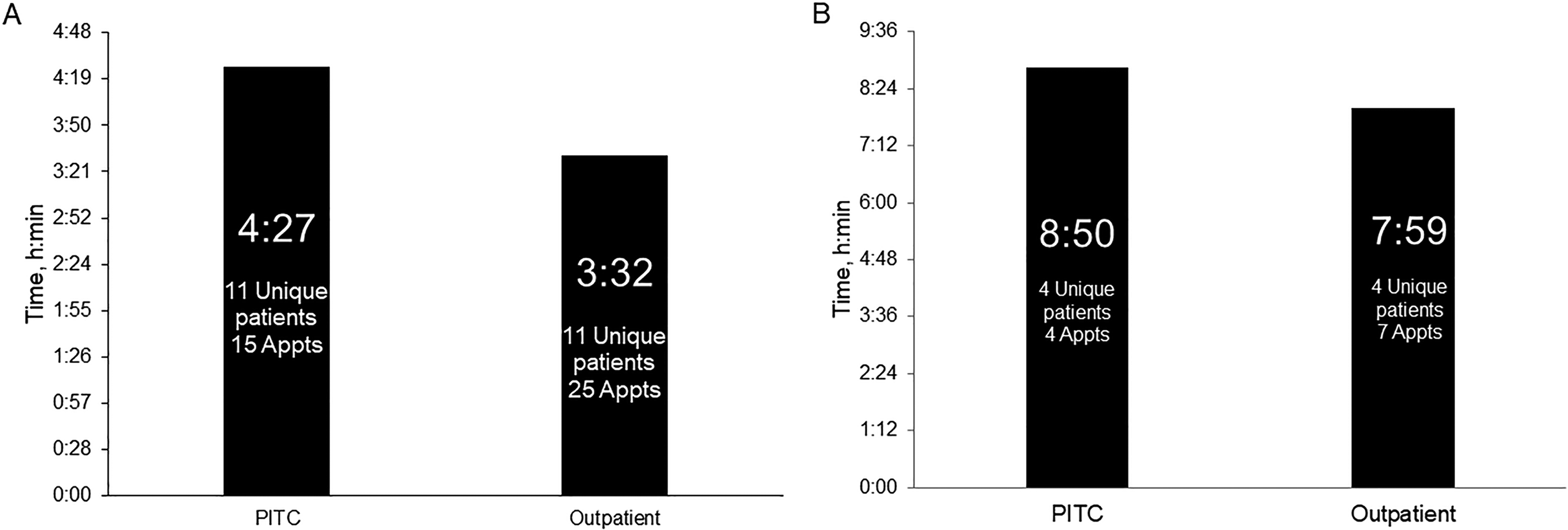
Average duration of patient appointment itinerary. (A) Patients who did not undergo lumbar puncture. (B) Patients who did undergo lumbar puncture. Time is shown for patients according to whether they received chemotherapy infusions during appointments (Appts) in the Pediatric Infusion Therapy Center (PITC) before and during the pilot or in an outpatient examination room (Outpatient).
Appointment Location
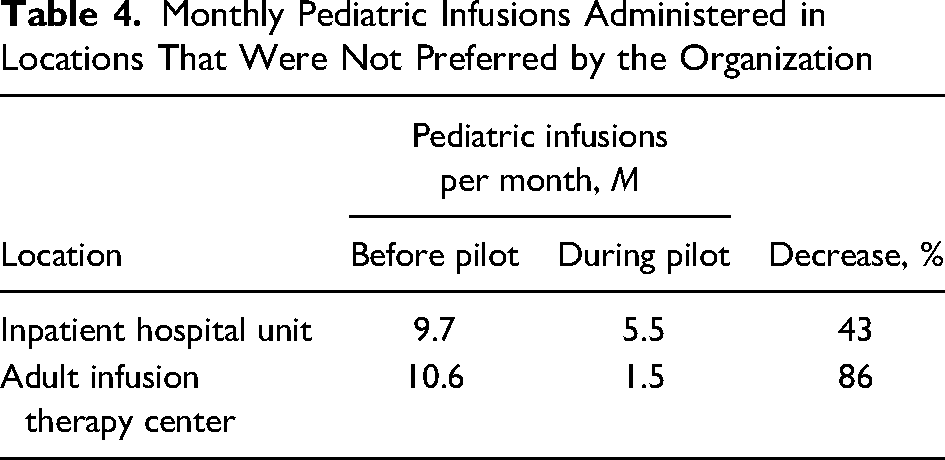
Table 4 shows the percentage decrease in the number of pediatric infusions per month (before and during the pilot) that took place in settings not preferred by our organization for pediatric infusions. The data show that the pilot helped ensure that more pediatric patients received their infusions from pediatric-trained caregivers in an outpatient setting. This kept inpatient beds available for acute care needs and decreased the number of children who received care in space intended for adults.
Monthly Pediatric Infusions Administered in Locations That Were Not Preferred by the Organization
Patient and Family Satisfaction
To ensure that the changes were improving the experiences of the patients and families, the team created a satisfaction survey that parents and caregivers completed as they left their child's infusion appointment in the outpatient examination room. The survey included questions about satisfaction with the date and time of the appointment, the duration of the appointment, the outpatient examination room facilities, patient safety throughout the appointment, and willingness to recommend the outpatient location for infusions to others. Responses to these questions were based on a 5-point Likert scale (from strongly agree to strongly disagree). A total of 30 respondents (parents and caregivers involved with 184 injections; 16% response rate) provided responses to the optional satisfaction survey (Figure 3).
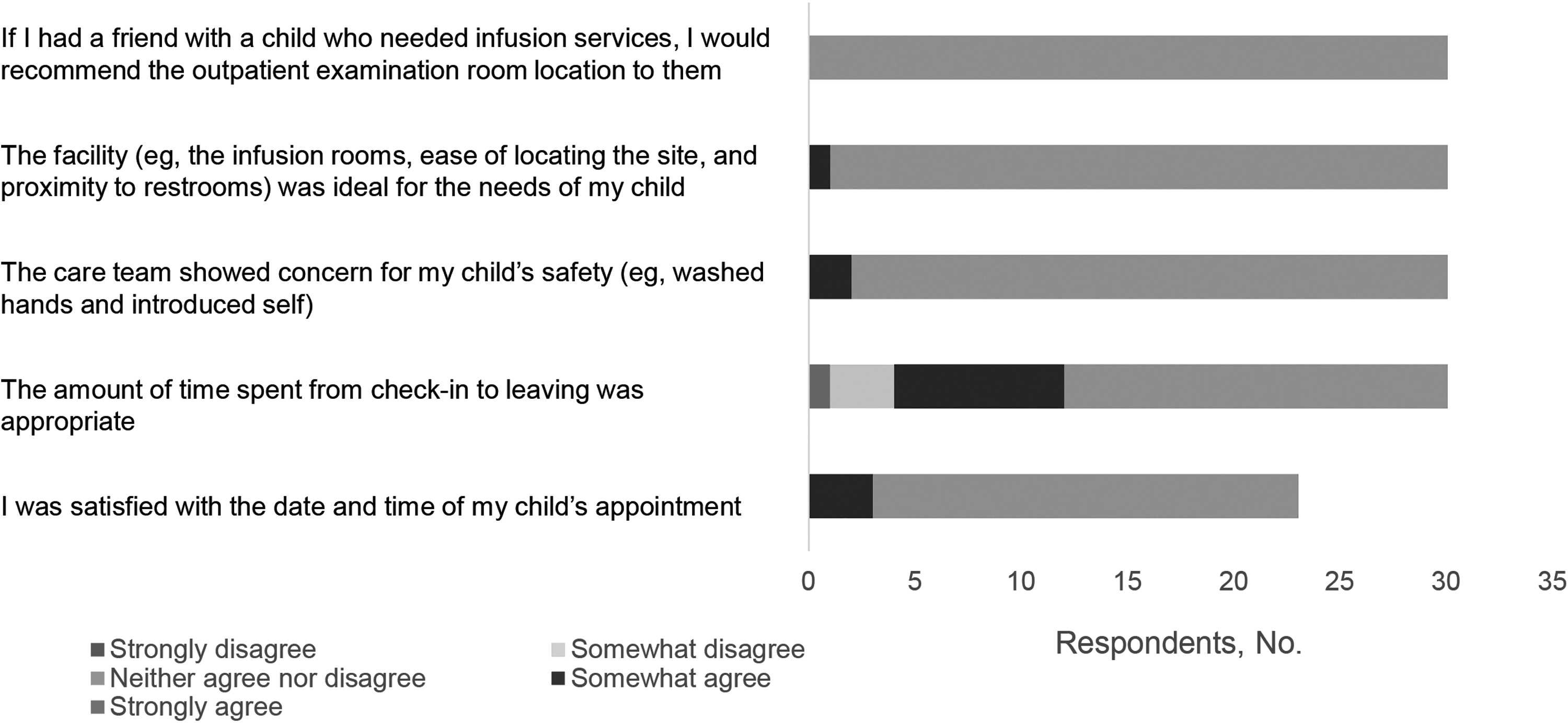
Patient and family satisfaction survey results.
The survey also asked respondents whether they preferred to receive an infusion in an outpatient examination room or in the PITC. The survey provided space for respondents to write free-text responses about why they preferred the chosen location and what impressed and disappointed them about their infusion appointment. Of the 30 respondents, 28 (93%) preferred an outpatient clinic examination room, and none of the respondents preferred the PITC (2 [7%] had no preference). Some of the free-text comments explained the reasons for this preference (Box 1).
Selected Free-Text Comments From Survey
My child is … comfortable having to stay in the same room.
It was incredibly convenient to not leave our room … from port access, provider visit, and infusion. Most importantly, it is what is safest for the child and helps to prevent fatigue and burnout of child and caregiver (parking, walking, checking in, and waiting).
Sometimes there is a pharmacy delay, but even with that I would rather stay put in one place.
The days are long and exhausting enough for our child/family—this helps as we do not have to shuffle from building to building and there is less anxiety in our child with this.
Upon completion of phase 2, metric results were presented to departmental and institutional leadership. The pilot was approved for transition to an operational state with the assumption that the infusions offered in phase 2 would be offered for administration in the outpatient examination rooms indefinitely.
Discussion
Many pediatric health care organizations offer infusion therapy in an outpatient infusion therapy center; however, we did not find reported examples of organizations that offer infusions in the same outpatient examination rooms that are used for appointments with physicians and advanced practice providers. There are also few articles that address safety and other care outcomes for pediatric infusions in an inpatient setting compared with an outpatient setting. Some research has focused on adult patients, and those studies did not find a difference in safety and other care outcomes by setting (Corsi et al., 2020; Jones et al., 2019).
Our project showed that the use of outpatient clinic examination rooms is a viable way to provide timely and safe administration of short infusion therapies for pediatric patients in hematology and oncology practices. All measured metrics showed favorable outcomes. The use of an alternative infusion therapy location minimized the number of pediatric patients who needed to be moved to a less desirable location, such as an inpatient hospital unit or an adult chemotherapy infusion center. In addition, the use of outpatient examination rooms was favorably received by patients and families.
This novel solution merits consideration by any health care organization that provides pediatric infusions. Health care organizations that may benefit the most are those like ours—facilities with a growing patient base but a small number of infusion treatment rooms and no physical space for expansion. Infusions for consideration do not need to be limited to oncologic therapies, and we encourage further investigation into other therapy options.
The limitations of this study include the relatively small number of patients who received infusions. Owing to capacity constraints and the limited availability of nurses and pharmacists, only short, low-risk infusion treatments were piloted in the outpatient examination rooms. Further study of the feasibility of offering longer and potentially higher-risk treatments is warranted.
Implications for Pediatric Hematology and Oncology Nursing
Implementing a process where infusions are provided to pediatric patients in outpatient clinic examination rooms has implications for an organization's nurses in three main areas: work integration, task distribution, and nurse accreditation. We hope that what we have learned will help other organizations that are considering the use of outpatient clinic examination rooms for infusion therapy.
Work Integration
Our organization asked RNCCs in our outpatient clinic to provide infusion therapy in this setting instead of moving nurses from the PITC. The incorporation of this incremental work into a busy pediatric hematology and oncology outpatient clinic was a complicating factor and resulted in some RNCCs working more than their allocated FTE at times. This is a focus for improvement and refinement as the project transitions from the pilot to operational practice.
Task Distribution
The RNCCs and nurse leaders continue to have ongoing dialog with patients, physicians, and pharmacy and operations personnel because the primary focus is to optimize workflow efficiencies to enhance the patient experience. When appropriate, tasks such as retrieving infusions from the pharmacy, administering nonchemotherapeutic medications, cleaning equipment, and preparing rooms have been delegated to licensed practical nurses and desk operations specialists.
Accreditation
Many of the RNCCs had experience providing infusion therapy in the past, but because they had not worked in the PITC for more than a year, they were required to attend chemotherapy classes and skills assessments to maintain competency. This also ensured that our organization continued to meet the accreditation requirements of the American College of Surgeons Commission on Cancer (American College of Surgeons, 2021). The limited frequency and availability of these classes and assessments delayed our project timeline and limited the infusion appointments that could be offered.
Implications for Patients
Some of the most important patient benefits realized through this project were improved patient and parent satisfaction with no negative impact on safety. Through satisfaction surveys, we learned that families overwhelmingly preferred that the infusion be given in an outpatient examination room instead of the hospital-based PITC.
Many patients receiving chemotherapy are immunocompromised, making them susceptible to infection. While we found no evidence that patients who receive treatment in the PITC have an increased risk for hospital-acquired infections or other patient harm, we believe that decreasing the duration of appointment itineraries and decreasing the number of patients receiving infusions in the inpatient setting can only have a positive impact. In fact, other research has shown that outpatient treatment was as safe as inpatient treatment and provided other benefits for pediatric and adult oncology patients (Getz et al., 2021; Mielke et al., 2020; Orme et al., 2014).
Further research and investigations are warranted to determine whether patient safety is comparable when pediatric patients receive their infusions in an outpatient setting, including outpatient examination rooms such as those used in our pilot.
Conclusion
The aim of this project was to test the feasibility of a new approach for administering pediatric chemotherapy infusions. We piloted the administration of infusion therapy in outpatient clinic examination rooms with the goals of improving patient and family satisfaction and shortening the duration of appointment itineraries. These goals were accomplished without a negative effect on patient safety. This novel approach may be especially helpful for health care organizations confronting external influences such as lack of physical space, increased patient volumes, and pandemics.
Footnotes
Acknowledgments
Randall J. Fritz, DVM, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading and administrative and clerical support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.