
Abstract
Introduction
Children with cancer experience frequent pain and fear related to the disease and its treatment, most notably from needle procedures such as port-a-cath access (Ljungman et al., 1996, 2000). A port-a-cath is a plastic or metal device embedded under the skin in the patient's upper chest area. It is intended to administer medication and chemotherapy to the patient directly to the larger blood vessel (Implanted Venous Access Port, n.d.). Despite the use of pharmacological and topical treatments (e.g., eutectic mixture of local anesthetics lidocaine/prilocaine), port-a-cath access is reported to be painful, frightening, and distressing for young children (Lüllmann et al., 2010). Thus, it is critical to identify nonpharmacological interventions that can also be used during port-a-cath needle procedures as part of a multimodal pain management approach.
In addition to pharmacological and topical treatments, psychological support, such as distraction, deep breathing, and other cognitive-behavioral techniques, is recommended as the standard of care for all youth with cancer undergoing port-a-cath access (Birnie, Noel, et al., 2018; Flowers & Birnie, 2015; Implanted Venous Access Port (Mediport Placement), n.d.; Sander Wint et al., 2002). Distraction is efficacious for reducing needle-related pain and fear in pediatric populations (Uman et al., 2013), as well as managing procedure pain among children and adolescents with cancer (Bukola & Paula, 2017; Jibb et al., 2015). Virtual reality (VR) is thought to be a particularly effective distractor for pain, given its inherent immersive and interactive properties (Eijlers et al., 2019; Ford et al., 2018; Griffin et al., 2020; Mallari et al., 2019; Malloy & Milling, 2010; Won et al., 2017), with effects on both attention and affect identified (Gold et al., 2007; Gupta et al., 2018).
VR games create an immersive environment and are more distracting than other forms of distraction. For instance, studies comparing the impact of VR interventions to other interventions for pain in burn victims found that immersive VR games were more effective than traditional video games (Hoffman et al., 2000) and cognitive-behavioral techniques (Geisser et al., 1995; Tan & Leucht, 1997). VR intervention has been utilized with adults and children to manage needle procedures, dressing changes, and chronic and postsurgical pain (Gold et al., 2007, 2009; Jibb et al., 2015; Kenney & Milling, 2016; Won et al., 2017). However, to date, little is known about the use of VR interventions with childhood cancer patients during port-a-cath needle procedures. Most previous studies using VR distraction for children with cancer examined VR use with other cancer-related procedures (e.g., lumbar puncture, venipuncture). These studies found reduced procedure-related pain, fear, anxiety, distress, and physiological reactivity, as well as shorter procedure times (Gershon et al., 2003, 2004; Sander et al., 2002; Schneider & Workman, 2000; Windich-Biermeier et al., 2007; Wolitzky et al., 2005). However, not all studies show positive effects for children with cancer (Nilsson et al., 2009).
Effective VR distraction interventions are those that capture attention, are immersive, fun, interactive, novel, and goal-orientated (Birnie et al., 2017; Gershon et al., 2004; Jibb et al., 2015; Triberti et al., 2014). These qualities of VR intervention may differ based on age, gender, and individual preferences. In addition, the initial high cost of VR headsets and immersive VR games has been reported as a barrier to the adoption of VR intervention in clinical care (Lauwens et al., 2020). To increase the likelihood of VR intervention use in standard clinical practice, it is important to evaluate and ensure the effectiveness, acceptability, and usability of cost-effective, commercially available VR interventions. The current study is the first to examine the use of commercially available and free VR interventions for pain and fear during port-a-cath access in children with cancer. The current study aimed to evaluate the preliminary effectiveness of the commercially available Oculus Go VR system (https://www.oculus.com/go/), with freely available VR games, for reducing pain and fear levels during port-a-cath access procedures in children with cancer aged 4–17 years. In addition, we assessed acceptability and usability among children, parents, and nurses.
Materials and Methods
Study Setting and Design
A mixed-method, pre-posttest, approach was used to examine the VR intervention usability (ease of use, acceptability) and impact on nurses workflow and on patients experience for children aged 4–17 years undergoing port-a-cath access. The study was performed by a team of psychology research assistants and nurses at an outpatient pediatric cancer clinic in the southeastern United States. Potential participants were identified and initially approached by a member of their clinical care team. If the child and caregiver expressed interest, a research assistant obtained informed consent and assent. Child–caregiver dyads volunteered for this study and did not receive compensation.
Participants
Patients were eligible if they were (a) between the age of 4 and 17 years, (b) had a diagnosis of any type of cancer, (c) were receiving port-a-cath access, and (d) were able to speak and verbally understand English. This age range is similar to other pediatric studies evaluating VR (Eijlers et al., 2019; Won et al., 2017) and was chosen to be as inclusive as possible for evaluating the VR intervention in a real clinical setting. In addition, the patient's caregiver had to be: (a) 21years or older, and (b) able to speak, read, and write in English. Patients were excluded if they (a) had visual, auditory, or cognitive impairments that precluded them from using the VR intervention independently, (b) were unable to understand and/or answer questionnaires, (c) were sedated (e.g., drowsy due to Ativan), (d) were end-of-life (due to the high burden of treatment and care these patients and families experience), or (e) had methicillin-resistant Staphylococcus aureus infection or symptoms of respiratory or gastrointestinal infection (to avoid contaminating the VR equipment).
Intervention
Children were given a 5 min demonstration of the Oculus Go VR hardware and game software. Children were allowed to choose an age-appropriate game from select games downloaded onto the Oculus Go device. Children were required to be seated during the VR intervention practice and port-a-cath access procedure. Children were allowed to remove the VR headset at any time during the port-a-cath procedure.
Assessments
Caregivers were asked to complete a demographic questionnaire and then rated the child's dizziness, nausea, pain, and fear prior to VR intervention. Children rated pain and fear prior to VR intervention and were monitored for dizziness and increased nausea while using the VR headset. Immediately following the port-a-cath procedure children and caregivers rated pain and fear a second time.
Demographic Information
Caregivers completed a demographic questionnaire that collected information including patient and caregiver age, gender, and ethnicity. Additional patient health information, including cancer diagnosis, date of cancer diagnosis, date of treatment, treatment(s) received, and date of birth, were obtained from the electronic health record.
Distress
The Fear Thermometer is a commonly used, single item, visual analog scale for self-reported anxiety or fear in children. The scale rates fear from 0 = not scared to 10 = extremely scared (Katz et al., 1980). Children and their caregivers were asked “How nervous are you [is your child] before your port-access?” before and “How nervous were you [was your child] during your port-access/” immediately after the port-a-cath procedure.
Pain
The Faces Pain Scale-Revised is a visual analog scale for pain. It demonstrates appropriate use and reliability for the assessment of children's acute pain intensity for ages 4 years and up (Hicks et al., 2001). The scale rates pain from 0 = no pain to 10 = very much pain. The child and caregiver were presented with six faces showing no pain up to very much pain and asked to point to the face that indicated their pain level at previous port-a-cath access procedures (pre intervention) and during their current procedure (post intervention).
Dizziness and Nausea
The Physical Symptoms Questionnaire was used to assess symptoms of nausea and dizziness before and after the VR intervention. Caregivers were asked to rate “What is your child's current nausea?” and “What is your child's current dizziness?” pre intervention on a scale from 0 = none to 4 = very severe. These questions were adapted from the Memorial Symptom Assessment Scale (Portenoy et al., 1994).
Semistructured Interview
A qualitative semistructured interview (Birnie, Nguyen, et al., 2018) was used to assess ease of use (e.g., “What was hard/easy with using the game?”), acceptability (e.g., “What did you like/like the least about the game?”), and adverse events of VR intervention (e.g., “Did you feel queasy or dizzy?”) during the port-a-cath procedure. Interview items also asked what participants would change about the VR intervention and whether they would be interested in using it during future needle procedures. Finally, the nurse completing the port-a-cath access was asked about the patients’ benefit (e.g., “Was it beneficial for the patient to use the VR system to this process?”) of the VR intervention and workflow interference (e.g., “Did it impact your workflow in any way?”).
Data Management
Data collected from this study was stored for child–caregiver dyads using a unique identifying number. All electronic data were stored in a password-protected secure REDCap database. Paper materials were deidentified upon data entry, marked with the participant's unique identifying number, and kept in a locked file cabinet.
Data Analysis
SPSS 23.0 (IBM, Chicago, IL, USA) was used for all statistical analyses. Parent fear and pain, pre- and post report was not obtained for one participant. Bayesian modeling was used to handle the missing data. Descriptive statistics were used to calculate patient and caregiver demographic information. A multivariate analysis of variance (MANOVA) was conducted to examine differences in patient versus caregiver-reported pain and fear scores. A paired-sample t-test was conducted to compare pain and fear levels prior to and after the VR intervention for both child report and caregiver report. Lastly, the usability, acceptability, adverse events, and workflow interference of the VR intervention were examined with descriptive statistics.
Ethical Considerations
Upon recruitment, child patients and their caregivers were given oral and written information about the study. Caregivers provided informed consent and child patients provided assent. Participants were allowed to withdraw from the study and child patients were allowed to discontinue VR headset use at any time. The study was reviewed and approved by the Institutional Review Board at the University of Mississippi Medical Center in Jackson, MS (04/27/2020, 2018-0169).
Results
Descriptive Statistics
A total of 24 patients were approached regarding this study and 19 patient–caregiver dyads were enrolled. Two patients declined to participate, one was excluded due to cognitive impairment, and two were excluded due to not needing port-a-cath access because of low white blood cell counts. Three participants withdrew from the study after enrollment due to medical distress (one patient was allergic to topical anesthetics) and frustration (one patient became frustrated with the gaming system during the demonstration and one patient wanted to lay down during port-a-cath access, and the chosen VR game did not work while lying down). Thus, a total of 16 patient–caregiver dyads completed the study. Patients who withdrew from the study had a higher mean age (10.67 years [SD = 3.14 years] for non-completers vs. 9.13 years [SD = 3.54 years] for completers). More males (n = 4 [66.7%]) than females (n = 2 [33.3%]) withdrew from or were ineligible to participate in the study.
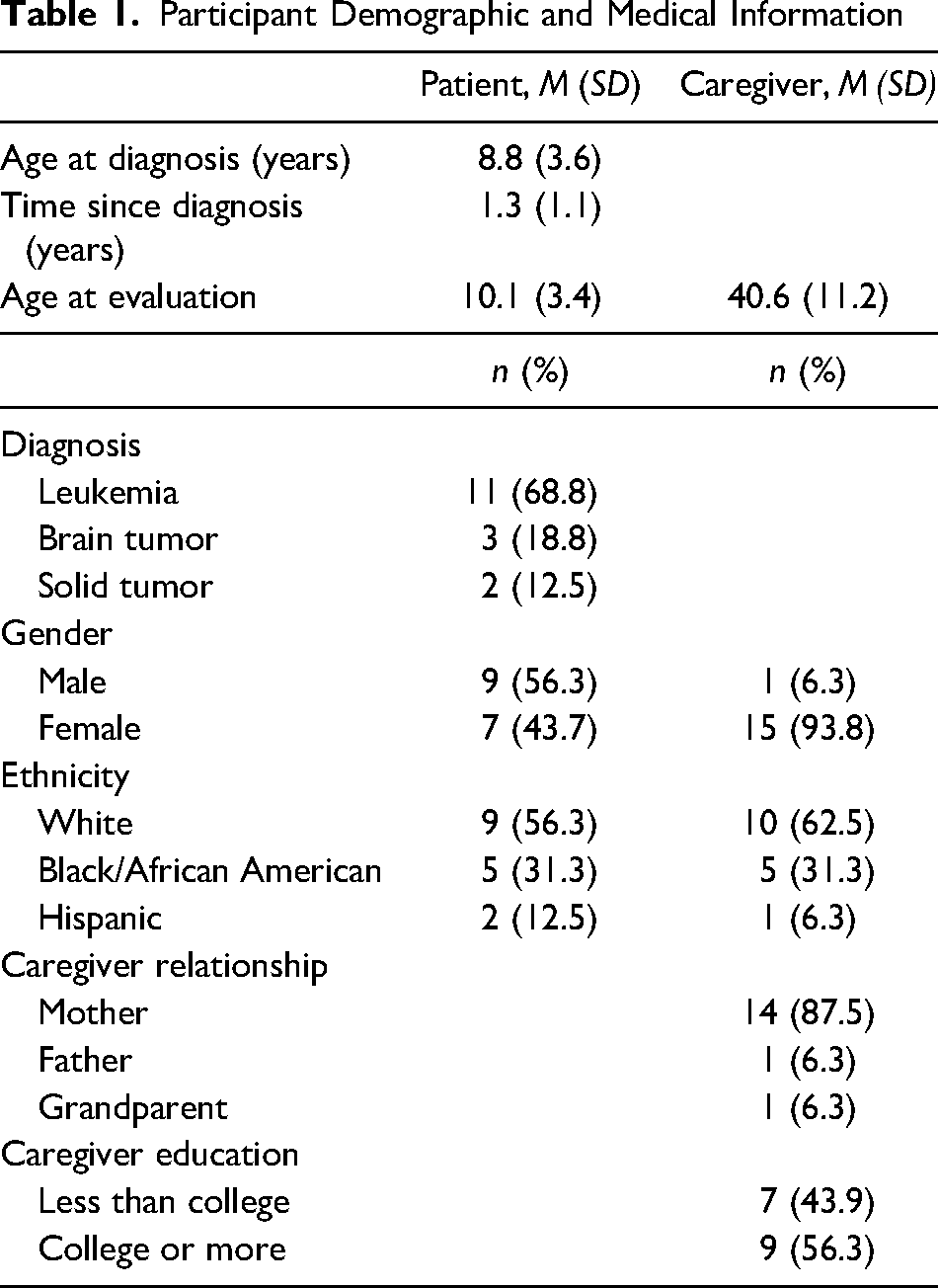
The final sample included 16 child–caregiver dyads. Patients included nine males and seven females, with a mean age at diagnosis of 8.79 years old (SD = 3.64) and mean time since diagnosis of 1.31 years (SD = 1.08). A little over half of the patients were White (56.3%) and the majority of patients were diagnosed with leukemia (68.8%). All participants had completed at least one port-a-cath needle procedure prior to participating in the study. Further information on demographics and medical data for patients is shown in Table 1.
Participant Demographic and Medical Information
Effects of VR Intervention
Pain
A significant decrease in pain was reported by younger children, F(2, 11) = 4.16, p < .05, from pre- to post-Cath-A-Port access. No other significant change or differences in pain scores were reported.
Fear
A significant decrease in fear scores was reported for child report (pre-Mfear = 4.63, SD = 2.75 vs. post-Mfear = 2.00, SD = 2.71; t-test = 3.35, p < .05) and caregiver report (pre-Mfear = 5.60, SD = 3.81, post-Mfear = 2.67, SD = 3.31; t-test = 3.42, p < .05).
Usability (Ease of Use, Acceptability)
Most patients (87%) used the VR headset during their port-a-cath procedure, while the rest used it just before the procedure but took it off during the procedure (n = 2). In terms of ease of use, most participants (81.3%) using the VR headset during their procedure indicated that the game was easy to use. Some of the issues reported by participants were not being able to visually see the controller and high difficulty levels on games. In regard to the acceptability of the VR games, the majority of patients (87.5%) wished to use the VR headset again and 12.5% said they might be interested in using the VR headset again. When asked “What was the best part of the VR games?,” 50% of participants reported distractibility and helpfulness (e.g., “Getting stuck in the game,” “Forgetting the chemotherapy port,” “It distracted me,” “That it helped”). And 42.86% reported individual games features (e.g., “seeing all the robots,” “the games,” “driving the rollercoaster”) as the best part of the game. One participant (7.14%) said they were unsure what they liked the most. When asked, “What did you like the least?,” 28.57% reported game-specific features or missing games (The “Moana video,” “I wanted to play Star Wars,” “Not as many games of the headset”); 57.14% reported “nothing” or did not report what they liked the least. Two participants (14.29%) reported “not knowing what was going on” when asked what they liked the least about the VR headset.
Adverse Events
Most patients reported no dizziness or nausea prior to the intervention (75%). Three patients reported feeling slightly dizzy and nauseous (18.8%) and one patient reported very severe dizziness and nausea prior to the intervention; however, this patient reported no dizziness after the procedure. One of the two participants who decided to remove the VR headset during the access of their port-a-cath reported a headache due to not being able to use his glasses with the VR headset. No medical intervention was needed for the child once the VR headset was removed.
Interferences With Nurse Workflow
Based on the semistructured interview, 84.6% of the nurses reported no issues using the VR headset during the port-a-cath procedure and 92.3% reported no interference with their workflow. Reported difficulties with VR headset use included: Patients preferred to watch the port-a-cath access procedure. One nurse indicated that her workflow “slows down a little” when the VR headset is used. No other procedural changes, changes to medical workflow, or changes in aseptic were needed. All nurses reported the intervention to be beneficial to the patient.
Cost Analysis
The required hardware for this project included two Oculus GO VR headsets ($200 each headset). Individual packaged, alcohol prep pads ($4.39 for 100 packs) were used to clean the headset before and after each participant had utilized the headsets. The Oculus GO VR games were free of charge. The total cost of this project was $404.39.
Discussion
Children and adolescents with cancer experience frequent pain and distress related to the treatment of their disease, most notably from needle procedures (Ljungman et al., 1996, 2000). Port-a-cath needle access has been shown to be especially painful, frightening, and distressing for children, even when pharmacological treatments, such as topic anesthetics, are used.3 The current pilot study adds to the literature and provides evidence that commercially available VR games may be effective in reducing children's pain and fear during port-a-cath access procedures, particularly in younger children. Preliminary evidence of usability is further indicated with caregivers and children reporting ease of use (81.3%) and no negative side effects (i.e., dizziness, increased nausea) during the VR intervention. Regarding nurse workflow, nurses indicated that the use of the VR headset had minimal impact on nurse workflow for the port-a-cath procedures. Finally, high acceptability was reported by both patients and nurses. Overall, the current pilot study demonstrates preliminary efficacy that commercially available VR intervention may offer an effective and cost-effective behavioral intervention to reduce fear and pain in children undergoing port-a-cath access.
Strengths
The current pilot study’s strengths were a mixed-method approach, assessment of usability (ease of use, acceptability), and assessment of adverse side effects from the patient, caregiver, and nurse perspectives. In addition, as the cost of VR interventions has been pointed to as an important barrier to implementation in clinical settings, the current study provides evidence that a commercially available VR system and freely available games may be effective in reducing children's pain and fear during port-a-cath access procedures.
Limitations
Limitations of the current study include the small sample size and lack of a control group. Of note is that some children chose to remove the VR headset during the port-a-cath access procedure due to the child's preference of watching the procedure. In addition, some children may prefer to lie down for their port-a-cath procedure, and although the procedure can be completed both seated and laying down, some VR games may not allow for the person to be in a horizontal position. Thus, some VR games may not be feasible in all situations. This highlights individual differences in coping strategies during painful medical procedures and encourages providers to let children lead their individual pain management plans. The use of mostly semiquantitative prevalence measures is also noted as an important limitation of this study. Both the use of rating scales and observational field notes may be criticized for its susceptibility to bias and thus more robust quantitative measures should be included in future studies. In addition, future studies should also aim at exploring how different types of pain management may benefit patients interchangeably, as well as evaluate the combination of VR with other evidence-based modalities such as relaxation and coaching by professionals (e.g., child life, psychology).
Conclusions
In conclusion, the findings of this pilot study suggest that the use of commercially available VR intervention may reduce children's fear and pain levels during the port-a-cath procedure, especially for younger children. Parents and nurses may also benefit from children utilizing VR interventions as it may reduce caretaker burden on parents and nurses. More research is needed to fully understand the benefits and limitations of the use of VR intervention in this setting.
Footnotes
Acknowledgments
We would like to thank the children and caregivers who volunteered to participate in this pilot study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article