
Abstract
Introduction
The severity of the psychological impact on parents of children with cancer has been well documented, with one of the most common psychological disturbances being depressive symptoms (Al-Maliki et al., 2016), and mild-to-severe stress (Krisnana et al., 2019). The causes of these psychological disturbances may vary, but in pediatric oncology, they are primarily related to the child's cancer diagnosis, treatment, treatment side effects, lack of social support, missing information about their child's disease (Njuguna et al., 2015), and understanding how to care for their child during treatment (Fisher et al., 2021).
While childhood cancer is rare, the burden of the disease is increasing due to increased success with common childhood infectious diseases (Bhakta et al., 2019). Childhood cancer accounts for an increasing proportion of child mortality in countries at all levels of income (Endalamaw et al., 2021). While high-income countries have had significant success in childhood cancer survivorship, the same is not evident in countries with limited resources (Bhakta et al., 2019). The global estimate of childhood cancer (0–19 years) is approximately 400,000 new cases per year (Steliarova-Foucher et al., 2017), and the 5-year survival rate is less than 30% for the approximately 384,000 children living in lower- to middle-income countries (Lam et al., 2019). Lack of a specialized pediatric oncology workforce, poor access to care, inaccurate diagnosis, and limited treatment options (including the expensive cost of drugs and diagnostic investigations) results in decreased survival rates in middle- to low-income countries (Stefan, 2014). Efforts to increase the number of qualified professionals and cancer units has led to the development of three pediatric cancer units in Ethiopia, staffed by appropriately trained medical professionals (Hailu et al., 2019).
The incidence of pediatric cancer in Ethiopia is estimated to be approximately 6,000 new cancer cases per year among children less than 18 years of age (Yifru & Muluye, 2015). The most prevalent childhood cancers in Ethiopia are leukemia, lymphoma, retinoblastoma, Wilms tumor, and bone and soft tissue sarcomas (Shad et al., 2013).
Jimma, Ethiopia
Ethiopia has the second largest population in Africa, 119 million, and Jimma Town's population is estimated at 128,306 (Worldometers, 2022). In 2019, Ethiopia's Human Development Index (HDI) was 0.485 (low), reflecting a status of 173rd of 189 countries (United Nations Development Program [UNDP], 2020). The HDI is calculated with consideration to health and life expectancy, access to knowledge/education, and standard of living measures (Roser, 2014).
Jimma Town is a rural setting with a large, eponymous public university with 42,000 students, a College of Public Health and Medical Sciences including a School of Nursing. Most parents/caregivers of children with cancer who are treated at the Jimma University Medical Center (JUMC) are poor and come from agricultural areas (Abebe et al., 2021). Twenty-two million people in the Jimma Zone (including Jimma Town, see Figure 1) live below the national poverty line (Asesefa Kisi et al., 2018).
Map of Jimma Town, Jimma Zone, Oromia regional state, in Ethiopia.
Food insecurity in the region is of concern. Asesefa Kisi and colleagues (2018) found that from 339 Jimma Town households selected at random, 66 (16.5%) of the respondents were food secure while 17 (4.3%) and 257 (64.4%) of respondents experienced mild and severe food insecurity, respectively. Most rural families are subsistence farmers, and their crops depend on rainfall (Adamseged et al., 2019). Therefore, long hospitalization times for a child with cancer are deleterious to the family's economy, food source, finances, and social support from community members. Understanding parents’ psychological burdens can help the pediatric oncology team understand how to identify and support the most at-risk and vulnerable and provide educational support, through a link with mental health professionals/psychologists for counselling and further treatment.
This article reports on a subset of data from a larger study conducted at JUMC (Mezgebu et al., 2020). The purpose of this study was to evaluate predictors of depressive symptoms among parents of children with cancer at JUMC. Objectives included documenting the prevalence of depressive symptoms and identifying factors associated with depressive symptoms.
Methods
Study Design
A quantitative, single-institution, cross-sectional study design was employed. Nonprobability sampling methods were used—purposive and convenience sampling. Purposive sampling ensured that only parents with children in the pediatric hematology and oncology unit were approached to participate, and convenience sampling meant all volunteering participants were chosen for their availability and willingness to participate.
Participants
The study was conducted at JUMC, which has more than 800 beds, and a dedicated pediatric oncology unit with 22 beds (Hailu et al., 2019). The pediatric oncology unit is headed by one pediatric oncologist and 12 nurses trained in pediatric oncology, supported by four pediatric oncology pharmacists. Radiotherapy is not available, and two pediatric surgeons conduct surgeries. All parents (biological mother or father only) caring for a child ≤ 18 years old, with a confirmed cancer diagnosis, were offered the opportunity to participate in the study. If both parents accompanied the child (this is quite rare at JUMC), then one parent was selected at random. Parents of critically ill patients or those that did not speak one of the local languages, Oromiffaa or Amharic, were excluded from the study.
Ethics Considerations
The Ethics Review Board of the Addis Ababa University College of Health Science, School of Nursing and Midwifery, granted ethics clearance (protocol No. 034/20/SNM). The JUMC pediatric hematology and oncology unit also granted permission for data to be collected in their unit. All potential participants were informed about the purpose of the study, their right to refuse, and assured confidentiality. All participants provided informed verbal consent before the questionnaire was administered orally by the data collectors. To maintain participant privacy, the questionnaire was administered in a room on hospital premises, but not in the pediatric oncology unit.
A study team member emphasized that participation was voluntary and explained to all participants that they had the right to withdraw if they so wished. Participants were assured that declining to participate did not risk or jeopardize their, or their child's, access to health services. Personal data, including names, that could identify participants were not recorded. All digital data were kept confidential through nonidentifying labels on a device only accessible by the researcher.
Data Collection Tool
Parental sociodemographic characteristics and child health-related factors were collected through a questionnaire developed by the research team. Clinical data were collected from the child's medical record. The study measure used was the depression subset of the Depression, Anxiety and Stress Scale 21 (DASS21; Lovibond & Lovibond, 1995). This subscale has seven items scored on a 4-point Likert-type scale (0 = never, 1 = sometimes, 2 = often, and 3 = almost always). A total score can range from 0 to 21 for the depression subscale. For the purpose of this project, scores of ≥ 10 were regarded as indicative of high levels of depressive symptoms.
The English version of the DASS21 was translated into two local languages: Oromiffaa and Amharic, and back-translated into English to verify accuracy. These are the most widely spoken languages in Jimma. The questionnaire was pretested at Addis Ababa's Black Lion Hospital with 5% of parents of children with cancer, and necessary modifications were made based on the gaps identified. At times, the “accurate” translation of words may obscure understanding. For example, the question, “What is the duration of the illness for your child with cancer?” may have parents respond with the child's lifetime illness history, including information not concerning cancer. In those cases, the research assistant explained that the duration meant the time since the child was diagnosed with cancer.
Study Procedure
Four experienced data collectors with a BSc in nursing were recruited from health centers in Jimma Zone. They were supervised by an experienced nurse researcher from JUMC. They trained over 2 days on the study objective, the data collection tool, and conducting the oral administration of the questionnaire to every participant (for consistency, and because many participants cannot read or write). The questionnaire took approximately 15–20 min to complete. Data collectors were both male and female and not matched to the participant's gender as the questions were not considered culturally gender sensitive in an Ethiopian setting. Participants were not remunerated for their participation.
Data Processing and Analysis
The data were captured, cleaned, and coded on Epi-Data v4.6.2. Analyses were conducted using SPSS v26. Descriptive figures were calculated (Table 1). A multivariate regression model was used to identify factors predicting depressive symptoms. First, variables were correlated with the depressive symptoms measure: variables that were not significant were not added to the regression model. The variance inflation factor was within the range 1.112 ≤ VIF < 1.419. To check for multicollinearity, tolerance values were in the range of 70.5% to 89.9%, a good indicator for the absence of multicollinearity. The Durbin–Watson value was 1.442, acceptable as evidence for normally distributed residuals. The Cronbach's alpha for the translated versions of the depression subset of the instrument was .860.
Sociodemographic Characteristics of Participants
Results
Sociodemographic Characteristics of Participants
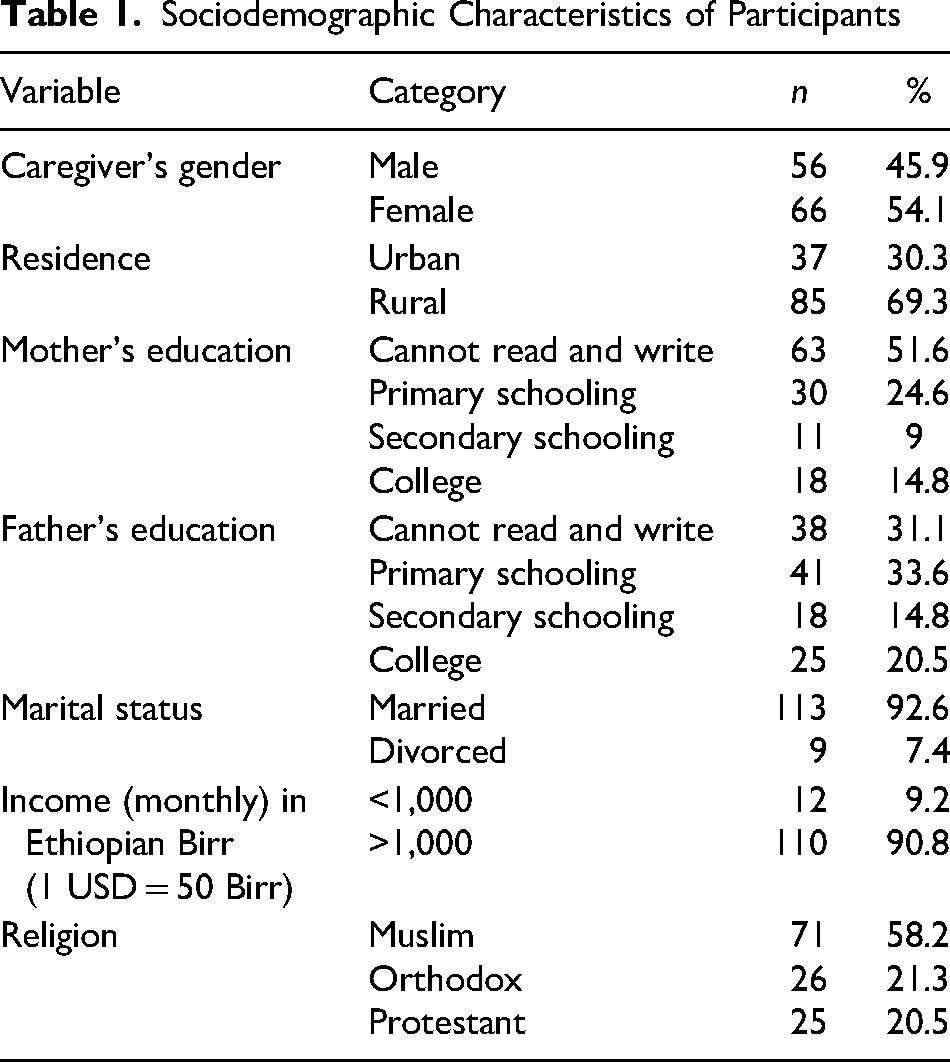
Of 126 participants who were enrolled, four returned incomplete questionnaires which were excluded, leaving a final sample of 122 participants. Sociodemographic characteristics are presented in Table 1. Most participants were Muslims (n = 71; 58.2%) and lived in rural areas (n = 85; 69.3%). Almost all were married (n = 113; 92.6%). Most mothers (n = 35; 51.6%) and fathers (n = 39; 69.7%) were employed. Most participants (n = 102; 83.6%) lived outside of Jimma Town.
Children's Health-Related Characteristics, and Service-Related Factors
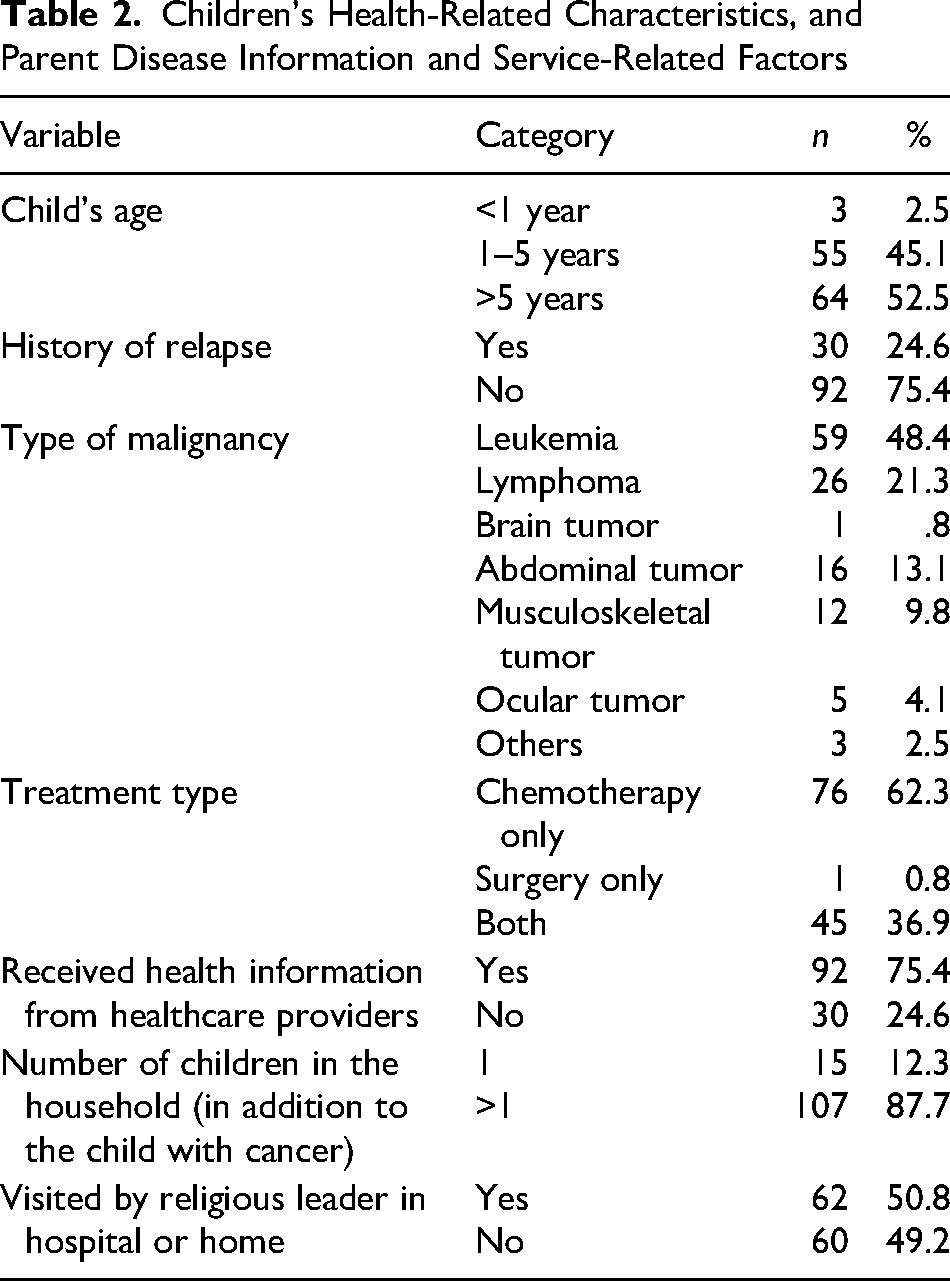
The characteristics of the children with cancer, parental experience of being informed about their child's disease, and support from religious leaders are presented in Table 2. More than half of the children were >5 years (n = 64; 52.5%) and nearly a quarter (n = 30) had a history of cancer relapse. Almost half of the children (n = 59) had leukemia. All children had received chemotherapy, and 46 (37.7%) had received surgery. Most parents (n = 92; 75.4%) reported receiving health information about their child's cancer. Most parents (n = 62; 50.8%) had been visited by religious leaders in the hospital or at home.
Children's Health-Related Characteristics, and Parent Disease Information and Service-Related Factors
Prevalence of Depressive Symptoms Among Parents of Children With Cancer
Of the 122 parents with complete data, just over half of fathers (n = 29) and over two-thirds of mothers (n = 45) had DAS-Depression scores of 10 or greater, indicating severe levels of depressive symptoms. Table 3 compares the characteristics of mothers and fathers based on DAS-Depression scores.
Characteristics of Mothers and Fathers Based on DAS-D Score
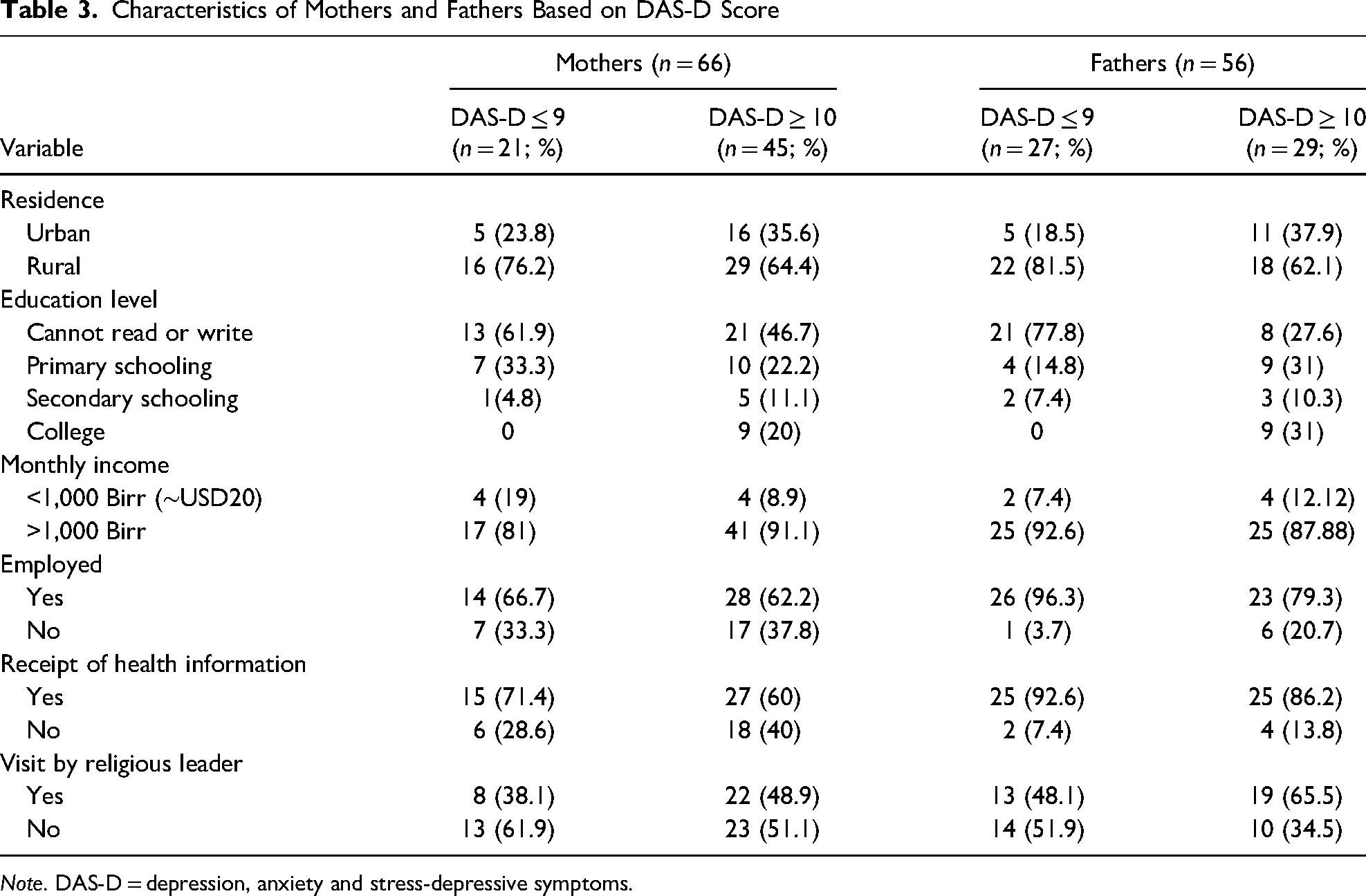
Note. DAS-D = depression, anxiety and stress-depressive symptoms.
To determine variables for inclusion in the multivariate regression, a chi-square test of independence was performed to examine the relation between the variables gender, religious contact, and health information, with the dependent variable of depressive symptoms converted to a dichotomous variable of “not depressed” = ≤ 9 and “depressed” = ≥ 10. The proportion of respondents who reported being depressed did not differ by caregiver's gender (χ2 = 3.41; p = .09) or receipt of health information (χ2 = 2.68; p = .13). Receipt of religious contact did, however, differ among those who had less depressive symptoms compared with those who had more severe depressive symptoms (χ2 = 4.31; p = .04). A Spearman rho correlation identified a positive correlation between DAS-D scores and maternal educations (rho = .39; p < .01).
A multiple linear regression analysis was statistically significant (F5 = 6.579, p < 0.001) and indicated that parent gender, maternal educational level, and receipt of health information predicted 18.7% of the variance in depressive symptoms. Being a mother (p = .033) and greater maternal educational attainment (p < .001) were predictive of greater depressive symptoms. Receipt of health information was predictive of lower depressive symptoms (p = .031). Religious contact and monthly income were not significant predictors (Table 4).
Multivariate Regression Coefficients for Predicting Depressive Symptoms
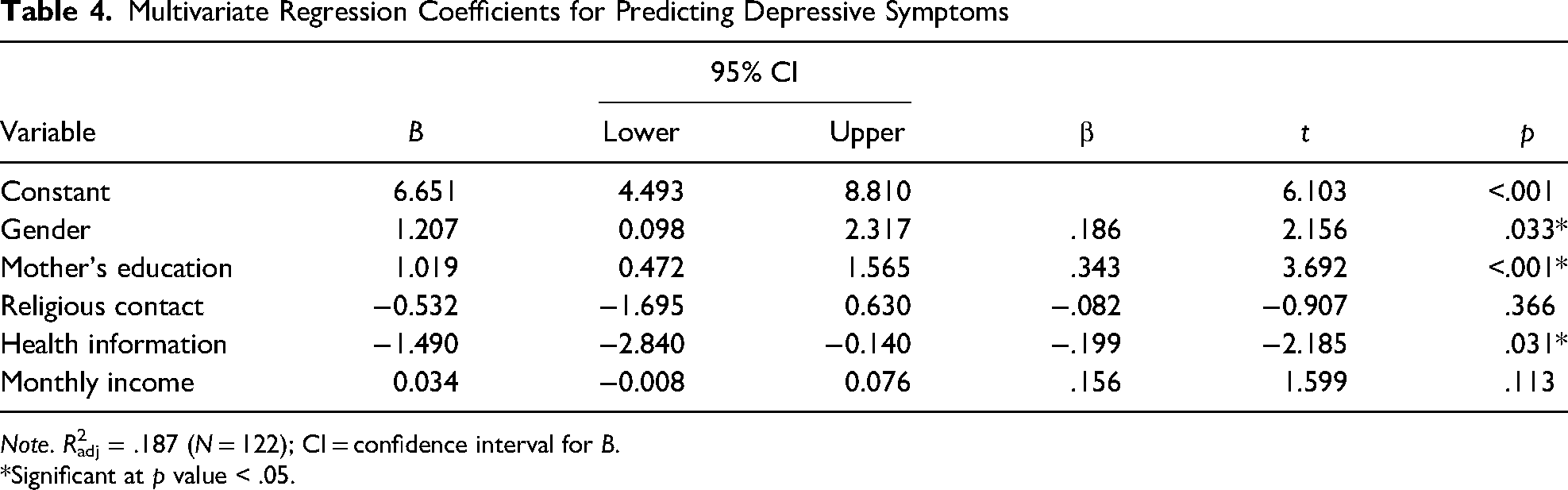
Note. R2adj = .187 (N = 122); CI = confidence interval for B.
*Significant at p value < .05.
Discussion
This study investigated the prevalence of depressive symptoms among parents of children with cancer receiving initial and/or on follow-up to treatment at JUMC. Being a mother was predictive of greater depressive symptoms as was higher maternal educational attainment. Receipt of health information on the child's treatment was associated with decreased depressive symptoms. These indicators suggest that parental roles and responsibilities might have features that prime depressive symptoms in mothers and that receiving information about the child's diagnosis and treatment lessened depressive symptoms.
Mothers acting as primary caregivers for children who are ill is common across countries and cultures. In Canada, for example, it is not uncommon for mothers/women to be the primary caregiver of an ill child (Molinaro & Fletcher, 2018). In Iran, this is true, especially in the hospital setting due to religious regulations concerning gender separation (Khanali Mojen et al., 2022). In a Japanese study, authors found that mothers may feel that they only trust themselves to be the main caregiver, and this new responsibility adds to the pressures of maintaining family life, especially if they have more than one child, and becoming the child's protector in hospital, from distress or other perceived dangers (Saiki-Craighill, 2012). This can feed into perceived assumptions about female/maternal instincts and role expectations of being physically present with the child (Young et al., 2002). With the mother as the main caregiver to the child with cancer, responsibilities are often restructured among family members. Because many cultures regard childrearing as the “mother's realm,” mothers can sometimes experience feelings of guilt about their child's illness, accompanied by the assumption of full responsibility for care, through singular dedication to care and sacrifice of personal desires (Lee & Lee, 2020).
Mothers may experience feelings of paralysis at the news of the diagnosis, fear of the disease and or death, and anticipate challenges in the treatment experience (Shattnawi et al., 2021). Yeh (2002) found that while Taiwanese mothers experienced higher levels of distress, both parents experienced high levels of distress and marital dissatisfaction if their child's diagnosis was recent. Norwegian mothers and female caregivers reported higher levels of fatigue, sleep disturbances, anxiety, stress, and more strain on social relationships than fathers and male caregivers (Johansen et al., 2018). Mothers would like to take a break without feeling anxious, taking time to chat with friends, spend time with their family, and to potentially further their careers in Korea (Kim et al., 2017). All of these converging emotions can contribute to feelings of guilt for personal needs and desires while their child is ill.
Collectively, these factors can potentially impact an individual greatly should roles and responsibilities pull them away from their ill child. In this study, all parents from households in which mothers had received tertiary education (n = 18) had high depressive symptoms. Of these households, 15 reported that the mother was employed. It is possible that these mothers are in professional occupations or demanding jobs, and they may be less able to freely structure their time to fulfill all desired responsibilities. Svavarsdottir (2005) found that mothers experienced emotional support and personal care for their ill child, emotional labor in the family, and providing emotional support for their other children as time-consuming and difficult. One could imagine that for mothers working in occupations heavily demanding of time and effort, fulfilling these needs over and above other roles would be difficult at best, or not possible at worst.
Receiving health information related to the child's diagnosis and treatment was associated with lower DAS-D scores. The foundation of this is health literacy, which involves the ability to read, write, communicate, and find information; an understanding of the structure of health systems and how to obtain access; and participating through following treatment courses, and changing behaviors to facilitate health (Lambert & Keogh, 2014). Being provided with the appropriate information empowers patients and parents to perform these tasks, to ask questions and find answers, and to know what to anticipate in this very difficult period. The accessibility of this information is particularly vital, as 51.6% of mothers and 31.1% of fathers in this sample were illiterate. Meeting the needs of caregivers from their level of understanding is imperative.
Limitations of the Study
This study has several limitations. It was conducted in a single center and completion of the questionnaire involved direct interaction with a data collector. Though there was the capacity for anonymity, the effect of social desirability cannot be disregarded. Previous research has suggested that some traditional African cultures and communities believe mental illness arises from a weak constitution or negative impact of personal choices (Shah et al., 2017), or a failure to uphold cultural standards and values of character, and behavior that society expects (Monteiro & Balogun, 2013). Responses given to the data collector could be interpreted as possibly incurring negative judgments from the facilitator. Research needs to consider the vulnerability of the persons being surveyed, especially regarding sensitive topics.
This study did not qualitatively investigate participants’ opinions. As the scale used closed responses, it would be helpful to examine what people understood by caregiving, literacy, and support from religious figures and the community. Cultural norms and expectations about parenting (and mothering) can help to construct a map of responsibilities, desires, and needs of parents caring for children with cancer. The inclusion of income status (Mekonnen et al., 2020) and spending can add perspectives on the socioeconomic effects of caring for a child with cancer, especially in a country where poverty is widespread. An elaboration on literacy can provide perspectives on how medical information can be shared. The impact of preexisting mental health conditions on the current psychological state can highlight situations that strengthen or deteriorate psychological burdens (Al Qadire et al., 2018; Walubita et al., 2018).
The tool in this study, the DASS21, is a short version of the DASS. As a screening tool, the DASS21 is not intended to address the greater symptomatology of depression: changes in cognitive function, low energy, insomnia, changes in weight and appetite, and suicidal ideation and behavior (Kendler, 2016).
Implications for Clinical Practice
Asking parents to make decisions about their child's treatment presupposes that parents are equipped with the knowledge and experience to access, process, and understand potentially complex medical information. Information can be presented in an accessible manner to accommodate those with low literacy (Ryan et al., 2014). Glewwe (1999) described the relationship between literacy and health knowledge as indirect—through numeracy and literacy one gains skills in health knowledge, health information is not explicitly taught. If there are differing levels of literacy among parents of children with cancer, it becomes important to communicate medical information clearly and effectively, and to uphold spaces for parents to ask questions. This issue needs to be clearly evaluated, with appropriate interventions implemented.
Concern for parents’ mental and physical health is crucial when their child is diagnosed with cancer. Appropriate support and interventions are necessary, particularly for mothers, who we have shown are more likely to experience psychological distress than fathers. Incorporating a mental health professional, like a psychologist, to the multidisciplinary team is a significant way to address children’s and parents’ distress not typically feasible through routine support measures (e.g., social workers, parent groups, and housing and transportation assistance). Further research using adapted and tested screening tools, specifically for this population, is essential. It would benefit practice if nurses were trained to identify signs of psychological distress, but this requires careful consideration of nurses’ responsibilities to the patient, and their existing workload. Developing a better understanding of risk factors for emotional distress in an Ethiopian context of childhood cancer care will allow local medical professionals to unpack and address issues contributing to Ethiopian parental depressive symptoms.
Preexisting parental psychological issues could be shared with the treatment team so that nurses can intervene and link parents to local aid. Nurses have a key role as advocates for parents during multidisciplinary team rounds or meetings. Further research is needed on parental experiences in pediatric settings and across cultures while practicing an evidence-based approach to supportive care.
In settings with no dedicated psychologist specifically allocated for pediatric oncology, as in JUMC, dedicated social workers may collaborate with the multidisciplinary team to address psychosocial issues affecting the child and their parents. However, Ethiopian pediatric oncology nurses are not specifically trained on how to manage parental psychological issues.
Incorporating a psychologist in the team and training nurses to note signs of psychological distress is paramount and how psychosocial issues can be addressed with other team members. Nurses are closest in proximity to patients and parents, both physically and mentally. They can easily understand parents’ issues and play a key role as caregiver, counselor, and advocate with appropriate training. Nurses’ proximity also gives them the opportunity to learn details about patients and their families.
Nurses are also at risk of psychological distress due to the nature of their work. Childhood cancer treatment creates a strong bond between child, family, and nurses. Thus, it is important to address the psychological health of nurses as well. Nurses are often recipients of parents’ questions about diagnosis and treatment and thus serve to clarify information and address misconceptions about childhood cancer. Establishing trust and involving parents in the decision-making process can improve the relationship between parents and medical professionals.
Nurses want to develop a space where their patients, and their parents, can communicate openly and seek help when they need to. Paying attention to possible psychological distress will improve interactions and relationships, caring for those involved in the cancer treatment journey.
Conclusion
Mothers of children hospitalized for cancer treatment are at risk for depressive symptoms. This is in line with existing literature from other settings. Nurses have an important role in identifying depressive symptoms in parents but require training to do so. In Jimma Town, this training is not yet available. Nursing training for identifying vulnerable parents in psychological distress is needed to prevent severe consequences and to ensure that children with cancer have continual healthy parental support throughout their treatment.
Footnotes
Acknowledgments
The authors would like to thank the parents of the children with cancer who so graciously gave their time to participate in this research. The authors also wish to acknowledge Opoku Agyemang Dominic for his contributions to the statistical analyses.
Disclosures
We have no known conflicts of interest to disclose. Dorcas Malahlela was remunerated for her contributions to this article in the form of statistical analysis and knowledge of psychology. Opoku Agyemang Dominic was remunerated for his contributions to the statistical analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.