
Abstract
Keywords
Introduction
Cancer remains a leading cause of disease-related death in children and adolescents/young adults (AYAs). Treatment advances and improved supportive care for adverse effects of cancer therapy, however, have led to an estimated 80% survival rate (Howlader et al., 2021). These survival rates have spurred research of childhood cancer survivors (CCSs), and the recognition of their healthcare needs throughout the childhood cancer-survivorship continuum. Research on the long-term effects of childhood cancer and its treatment led to the development of guidelines for long-term survivorship care in 2003, and the ongoing evidence-based revisions to these and related health education resources (Bhatia, et al., 2015). Addressing long-term care needs is one important aspect of survivorship. Another critical time point in the childhood cancer survivorship continuum is the transition period at the successful completion of cancer therapy, or end of treatment (EOT). In the limited body of evidence exploring EOT experiences, it has been found that this is a particularly vulnerable time for CCSs and their families, deserving of attention and intervention (Wilford et al., 2019). Considered a milestone marking the completion of the often arduous cancer treatment, the EOT transition period is often a time of uncertainty and anxiety. Many CCSs and their parents report feeling unprepared for navigating the physical, emotional, and psychosocial challenges inherent in recovering from treatment and reintegrating into school, work, and family life (Bjork et al., 2011; Inhestern et al., 2020; Mckenzie & Curle, 2011; Muffly et al., 2016; Wilkins et al., 2014). Indeed, distress and worry about current and future challenges, fear of relapse, loss of support from the health care team, and unmet educational and psychosocial needs are hallmarks of the EOT experience for CCSs and their parents (Al Ghriwati et al., 2021; Conway Keller, King, et al., 2020).
To improve the transition to survivorship and prepare to meet posttreatment challenges, there have been calls to provide CCSs and their parents comprehensive health information, assistance with adaptation and coping, and support to address their physical, medical, and social-emotional concerns (Jones et al., 2020; Mitchell et al., 2016; Muskat et al. 2017; Walker et al. 2019; Weiner et al., 2015). Despite this, there are currently no established guidelines for the care of CCSs during the EOT transition period, which results in the inconsistent provision of services and puts children and families at risk for suboptimal medical and psychosocial outcomes (Conway Keller, King, et al., 2020; Jones et al., 2020; Karst et al., 2018; Shea et al., 2019). A few studies have described intervention strategies related to CCSs and their families at the EOT, with reports of feasibility but limited information regarding the impact on health outcomes (Salem et al., 2021; Shea et al., 2019; Wakefield et al., 2021). Fewer still have included health care professional's (HCP's) impressions of families’ needs, reports of services they routinely provide, or compared their perspectives to those of CCSs and families for whom they care.
In response to the limited research regarding EOT transitions, this article describes a study of CCSs, their parents/primary caregivers, and pediatric oncology HCPs, capturing current EOT practices and CCSs’ and families’ experiences at EOT. The purpose of this study was to compare patient/family EOT perceived needs to actual services provided, to inform the future development of meaningful services and support during the EOT transition period.
The primary research question explored was: what is the current state of EOT care, as described by HCPs, CCSs, and parents, and are there differences between what is provided and what is received? Secondly, does the current care provided by HCPs during the EOT transition period meet the needs of CCSs and their parents, as determined by levels of satisfaction with the EOT process and perceived preparedness for the transition following the completion of cancer therapy?
Method
Study Design
The EOT transition study employed a mixed methods design. The Connecticut Children’s institutional review board reviewed and approved the study.
Sample and Setting
The study took place in the outpatient setting of a pediatric oncology program at a 182-bed Magnet® designated children's hospital in the northeastern United States. The onsite hematology-oncology outpatient unit sees 50–75 patients per day and treats 80–110 newly diagnosed children and AYAs with cancer, from birth to age 35 years, per year. Convenience sampling included eligible participants from the following populations: CCSs between the ages of eight and 21 years who were within 1–6 months of the end of cancer treatment; parents/primary caregivers of CCSs between the ages of zero and 21 years who were within 1–6 months of the end of cancer treatment; and HCPs working with pediatric oncology patients at the institution. Eligible HCPs were pediatric oncologists, advanced practitioners (APP), nurses, social workers, child life specialists, and rehabilitation therapists. All participants spoke and read English. Of the CCS and parent sample, all were in remission from first cancer, and none had relapsed prior to or during the course of the study.
Procedures
Study enrollment occurred between March 2017 and September 2018. At the beginning of a scheduled follow-up appointment 1 to 6 months postcancer treatment completion, a member of the study team approached eligible CCSs and their parents/primary caregivers about study participation. A member of the study team explained the purpose of the study, risks, benefits, and voluntary nature of the study. A study staff member was available to clarify any questions about the survey items or to read the items to the participant if this was preferred. Recruitment occurred in a private space and trained members of the team obtained informed consent/assent. After consent, the CCSs and parents/caregivers completed the appropriate version of the End of Treatment Questionnaire (EOTQ) via paper and pencil before or immediately after the follow-up appointment. All CCS and parent participants received a $10 gift card as a thank you for completing the survey.
Potential HCP participants were introduced to the study at a staff meeting in March 2017. Subsequently, a study recruitment email was sent to all eligible HCPs. Informed consent and a study description were included in the email, as well as a SurveyMonkey© link to the EOTQ for HCP (EOTQ-HCP). Completion of the questionnaire implied consent. The study staff sent follow-up recruitment emails to HCPs every 4 weeks for 3 months to maximize participation. Data collection occurred between April and July 2017.
Measures
The EOTQ, the primary measure in this study, was an instrument adapted, with permission, to be administered within the first months of completing treatment for childhood cancer (Conway Keller, Ruiz, et al., 2020; Nagel et al., 2002). The survey was designed to assess the specific psychoeducational needs of respondents, as well as the preferred timing and modes of delivery of EOT interventions. The study team adapted and further refined the EOTQ with respect to developmental level and/or role to include the EOTQ-Child for children 8–14.99 years, the EOTQ-AYA for AYAs 15–21.99 years, the EOTQ-Parent for parents/primary caregivers of CCSs, and the EOTQ-HCP for pediatric oncology HCPs. Each version of the EOTQ contains 37–38 items. Close-ended items in each version include demographic and medical history questions, as well as multiple choice and rating questions. One open-ended question is included in each instrument (with two questions in the EOTQ-HCP) to obtain more in-depth information in the respondents’ own words. Multiple-choice questions in the EOTQ-child, EOTQ-AYA, and EOTQ-parent elicited information on the psychoeducational services received by CCS/AYA and their parents/primary caregivers, while the satisfaction with the services received, and preparedness for posttreatment issues following EOT were rated by respondents using a 3-point Likert scale. The EOTQ-HCP uses multiple choice questions to collect data on psychoeducational services HCPs provide and 3-point Likert scales to rate perception of patient/family satisfaction and preparedness for posttreatment issues (Conway Keller, Ruiz, et al., 2020).
Content validity was established for the EOTQs, each having a content validity index of 100%. Additional information on the development and psychometric testing of the respective EOTQ instruments is published elsewhere (Conway Keller, Ruiz, et al., 2020). Participants completed the child (EOTQ-child), AYA (EOTQ-AYA), parent/primary caregiver (EOTQ-parent), or HCP (EOTQ-HCP), as appropriate.
Data Analysis
Quantitative Analysis
Descriptive analyses, including frequencies, means, standard deviations, and count/percent of demographic data and medical history were conducted using IBM SPSS Statistics (Version 27) predictive analytics software. Kruskal–Wallis and Fischer's exact tests explored responses by CCSs, parents/primary caregivers, and HCPs. The chi-square test and Fisher's exact tests compared the frequency of CCSs’ and parents/caregivers’ satisfaction with the EOT meeting and preparedness for the EOT transition period. The chi-square test was also used to compare the responses of CCSs and parents to HCP responses. Odds ratios were obtained via cross-tabs in SPSS. The alpha level was .05 for all statistical tests.
Qualitative Analysis
Responses to open-ended questions were analyzed using an inductive approach to qualitative content analysis (Erlingsson & Brysiewicz, 2017; Graneheim et al., 2017; Graneheim & Lundman, 2004). Each response was condensed into a meaning unit, codes were developed to describe the meaning units, and these codes were then appraised to develop general categories and themes. Four authors (AN, KE, KF, and MCK) independently reviewed the responses and created codes. Consensus on codes was reached and themes were developed. To increase the dependability of the analysis, the same four authors independently assigned the themes to each response. The initial percent agreement of raters was 82%. Themes were refined through discussion and discrepancies were resolved through consensus.
Results of the quantitative and qualitative analysis were then compared using a convergent mixed methods design (Creswell & Clark, 2018). The intent of this process was to more fully examine potentially unmet needs and to gain a more complete understanding of the EOT experiences of all participants.
Results
Eighty-four CCSs and their parents/caregivers were considered for study participation. Upon further review, seven potential participants did not meet the inclusion criteria. Additionally, two CCSs and their parents/caregivers declined participation. Therefore, a total of 75 (89.3%) CCS and parent/caregiver participants enrolled and completed the study (Table 1). Of the 75 participants, 46 were parents/caregivers, 16 were AYAs, and 13 were children. Nearly two-thirds of all participants (64%) identified themselves as White. The children of parent/caregiver respondents were evenly divided among those younger than 8 years (34.1%), those between 8 and 14 years (31.8%), and those between 15 and 21 years (34.1%). The majority of children (31; 68%) were male. CCS respondents ranged in age from 8 to 21 years, with a median of 14.4 years. They had a variety of cancer diagnoses. Treatment duration ranged from less than 6 months to 4 years, and averaged 13 months. Most CCSs (23; 79.3%), however, received 12 months or less of total treatment time.
Demographics of Children, Adolescent/Young Adults and Parent/Caregivers
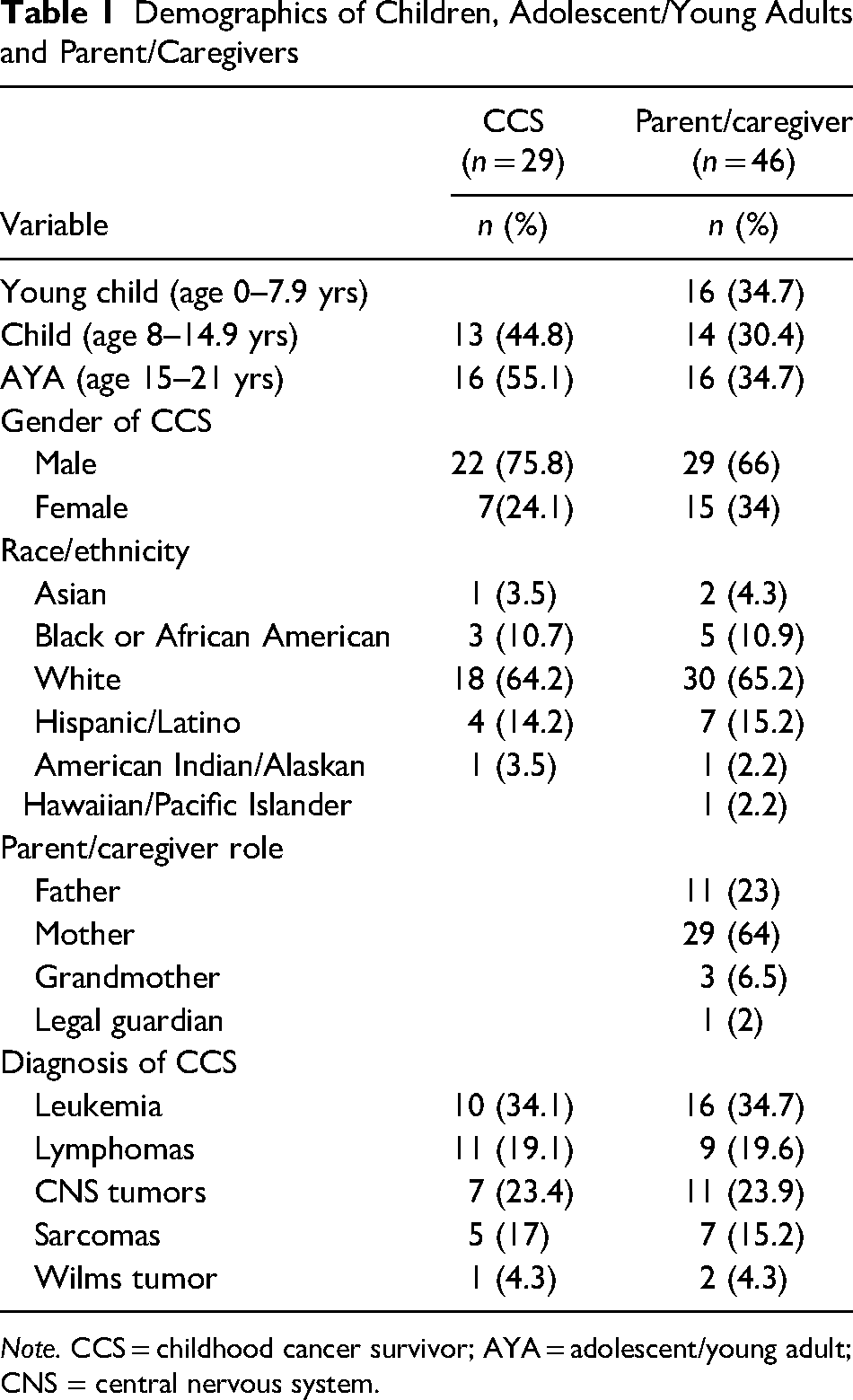
Note. CCS = childhood cancer survivor; AYA = adolescent/young adult; CNS = central nervous system.
Twenty-one of 29 potential pediatric oncology HCPs completed the online survey with a 72.4% participation rate. This included five attending physicians, five rehabilitation therapists, four nurses, three APPs, two child life specialists, and two social workers. Fifteen of 21 HCPs (71%) had been practicing in their stated profession for 16 years or longer. Of note, an additional six pediatric oncology HCPs who practice in this outpatient setting–three nurses, two APs, and one child life specialist—did not participate as HCP respondents because they were study team members and coauthors of this research.
End of Cancer Treatment Services Received
Childhood cancer survivors and parents/caregivers described their experiences at EOT, including the services they received. Overall, 36/46 (78%) parents/caregivers and 15/16 (94%) of AYAs recalled having an EOT “meeting” or “talk.” In contrast, only 4/13 (31%) children, and none under the age of 11 years, recalled having an EOT talk.
Information regarding program content was elicited from participants who recalled having an EOT meeting/talk, Many participants stated they received written information about EOT, including 20/46 (42.6%) parents/caregivers, 9/16 (56.3%) AYAs, and 3/13 (23%) children. An even greater number from each group would have liked to receive information in writing: 40/46 (85.1%) parents/caregivers, 12/16 (75%) AYAs, and 7/13 (53.8%) children. Approximately one-third of children and half of parents/caregivers and AYAs stated they received supportive services, such as a follow-up phone call, from their oncology team after EOT.
HCP Participation and Family Satisfaction
Participants indicated which HCPs were involved in the provision of EOT services. Those most frequently identified by parents/caregivers and AYAs as involved in the EOT process were, respectively, oncologists (78.7% and 81.3%), nurses (74.5% and 81.3%), and APPs (59.6% and 75%). The HCPs most frequently identified by child respondents were nurses (61%), oncologists (53.8%), and APPs (46.2%). Social workers and child life specialists were identified by between 25% and 33% of all respondents as being involved in EOT meetings/talks. When these responses were compared with family members’ satisfaction with the EOT meeting, there was no clear indication that HCPs from a particular profession who participated in EOT meetings affected family satisfaction. A positive trend was noted, however, between the number of HCPs identified as included in the EOT process and resultant AYA satisfaction (p = .07).
EOT Discussion Topics and the Association With Satisfaction and Preparedness
Participants identified the number and content of topics discussed in the EOT meeting: 13 for parents/caregivers and AYAs, and 12 topics for children (Table 2). The most commonly discussed topic recalled by parents and CCSs alike was “the plan for follow-up” (70/75; 93.3%). Similarly, all three groups stated that information regarding medical topics, including “a review of the cancer treatment” (57/75; 76%) and “a review of side effects” (54/75; 71%), were among the topics most frequently identified as discussed. Differences did exist in the various groups’ recollection of discussion topics. Most notably, the majority of parents recalled discussing the “ongoing role of the primary care provider” (34/47; 72.3%), whereas AYAs recalled discussing “individual or family stress” (15/16; 93.8%), and children recalled discussing “healthy lifestyle” (8/13; 61.5%) with HCPs at EOT.
Participant Responses to Topics Covered During End of Treatment Conversation
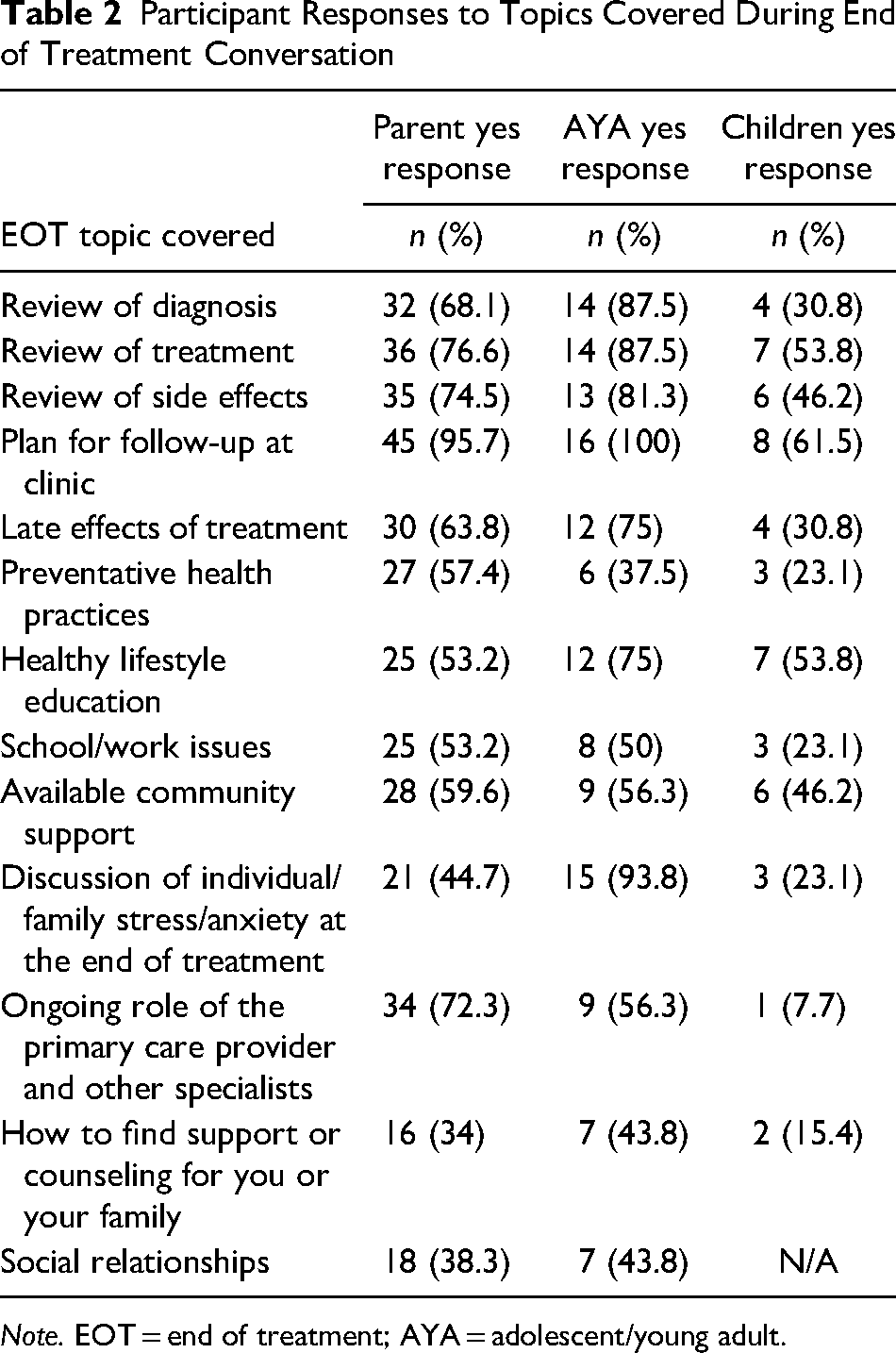
Note. EOT = end of treatment; AYA = adolescent/young adult.
Positive associations were noted between discussion topics and parents’ and CCSs’ satisfaction with the EOT process, as well as preparedness for EOT concerns. Parents/ caregivers stating they were “very satisfied” with the EOT meeting increased significantly relative to the number of topics addressed, from 50% being very satisfied when one to five topics were discussed, to 53% when six to 10 topics were discussed, and to 100% when 11–13 topics were addressed. For every additional topic addressed, the odds of a parent/caregiver being “very satisfied” were increased by a factor of 1.4 (p = .005). The number of AYAs stating they were “very satisfied” also increased significantly relative to the number of topics addressed (p = .02). When 1 to 5, 6 to 10, or 11 to 13 topics were addressed, AYAs reporting being “very satisfied” with the EOT meeting were 0%, 50%, and 100%, respectively. For child participants, the percentage stating they were “very happy” was 100% regardless of the number of topics.
In contrast, the omission of certain EOT discussion topics is negatively associated with satisfaction. The number of parents/caregivers who were “very satisfied” with the EOT meeting was significantly lower when topics related to “late effects of treatment” (p = .01), “finding support” (p = .001), “community support” (p = .04), “social relationships” (p = .007), or “other worries/concerns” (p = .007) were not addressed. The percentage of AYAs who were “very satisfied” was significantly lower when “late effects of treatment” (p = .04), “finding support” (p = .007), or “community support” (p = .01) were not included.
Satisfaction and Preparedness for EOT
Of the respondents who recalled participating in an EOT meeting, 26/36 (72%) parents/caregivers, 9/15 (60%) AYAs, and 4/4 (100%) children were “very satisfied” or “very happy” with the EOT meeting/talk. Overall, 20/46 (43%) parents/caregivers, 9/16 (56%) AYAs, and 3/13 (23%) children reported that they were “very prepared” for the posttreatment period. In each group, participants who recalled having an EOT meeting/talk were more likely to feel “very prepared,” while those who did not recall having an EOT meeting/talk were more likely to feel “somewhat prepared” for any posttreatment worries or concerns. The association, however, was not statistically significant (parents/caregivers: p = .17; AYA: p = .44; children: p = .76). No significant association was found between being very satisfied and being very prepared.
Unexpected Problems or Worries
Despite the majority of participants being satisfied with EOT services, many indicated that they experienced unexpected worries or problems following EOT, potentially indicating a lack of preparedness. This included 24/46 (52.1%) parents/caregivers, 8/16 (50%) AYAs, and 5/13 (38%) children. A majority of these participants (23 parents/caregivers, eight AYAs, and four children) described the unexpected worry or problem in an open-ended response. Qualitative analysis of these responses resulted in the emergence of three themes, which capture their experiences: unmet educational needs, with the subthemes of lack of anticipatory guidance and lack of formal process; unmet psychosocial needs; and unexpected physical issues (Table 3).
Qualitative Themes From Children, AYAs, and Parents/Caregivers
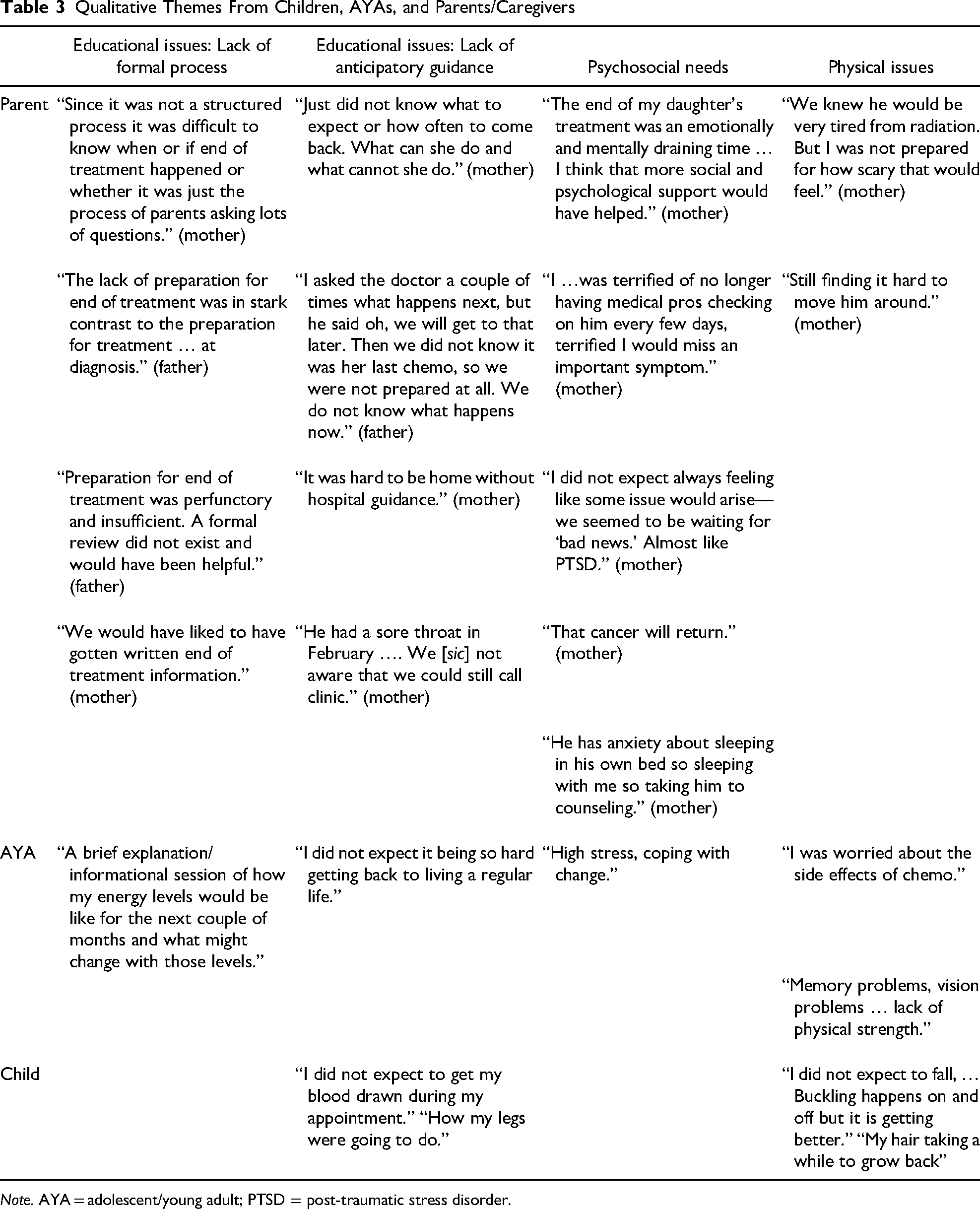
Note. AYA = adolescent/young adult; PTSD = post-traumatic stress disorder.
Parents/caregivers frequently identified educational issues as contributing to worries or problems at the EOT. This was expressed as a lack of anticipatory guidance for navigating through this recovery phase and adapting to life after cancer. This theme was also apparent as parents recommended the EOT process be more structured, or formalized.
Psychosocial needs also emerged as a theme, with parents asking for continued—or increased—psychosocial support to help them through this transition period. Parents who described the anxiety of watching their child or AYA experience physical symptoms, as well as parents expressing fear that the cancer would recur highlighted this theme.
The majority of CCS who answered the open-ended question described physical issues—lingering side effects and even new physical symptoms—as an unexpected worry or problem. Educational issues, specifically the lack of preparation for what to anticipate medically and physically in the period immediately following treatment, were also cited by CCSs as contributing to unexpected worries or problems.
HCPs’ End of Cancer Treatment Practices
The majority of HCPs in this study (12/20; 60%) indicated they “never” or only “sometimes” participate in providing EOT services to CCSs and parents/caregivers. These respondents included some pediatric oncology nurses and APPs, and all child life specialists, social workers, and rehabilitation therapists who completed the survey. Only 6/20 (40%) of HCPs replied “usually” or “always” to providing or participating in an EOT discussion with families. Providers of this service included all oncology physicians, one APP, and two nurses. Thirteen out of 18 (72%) HCPs indicated they provide written information to families, with 15/16 (94%) agreeing that written information would be helpful. Although only 4/15 (26%) stated they provide phone contact or other support to families, 15/16 (94%) indicated that this support would be helpful to families.
Topics parents/caregivers and CCSs recall being included in the EOT meeting/talk aligned closely with the topics HCPs report including. Of the HCPs who responded to this series of questions, 12/16 (75%) stated they always discuss “plan for follow-up,” and 9/16 (56%) review the diagnosis. In contrast, 6/16 (40%) teach about “late effects of treatment,” and 7/16 (47%) discuss “stress/anxiety at the EOT.” Topics identified as least often discussed were “social relationships” (3/16; 19%), and the provision of emotional support and counseling (2/16; 13%), topics encompassed in “finding support” and “community support” in the EOTQ.
HCP Perception of Family Satisfaction and Preparedness for EOT
HCPs gave their impression of family satisfaction with the EOT meeting and how prepared their families were for ending treatment. Twelve out of 21 (57%) HCPs responded that families were “satisfied,” with the EOT meeting/talk, but only 4/21 (19%) stated families were “very satisfied.” HCPs were split on the question of whether they thought families were prepared for EOT, with 9/16 (56%) stating families were “prepared,” and 7/16 (44%) stating families were “not prepared.”
Two open-ended questions elicited further information from HCPs regarding their perceptions of the EOT experience as well as their impressions of patient/family preparedness for potential issues posttreatment. Educational considerations emerged as the main theme of these open-ended responses, with the subthemes of learner readiness/understanding and a call for EOT standardization (Table 4).
Qualitative Themes From Health Care Professionals
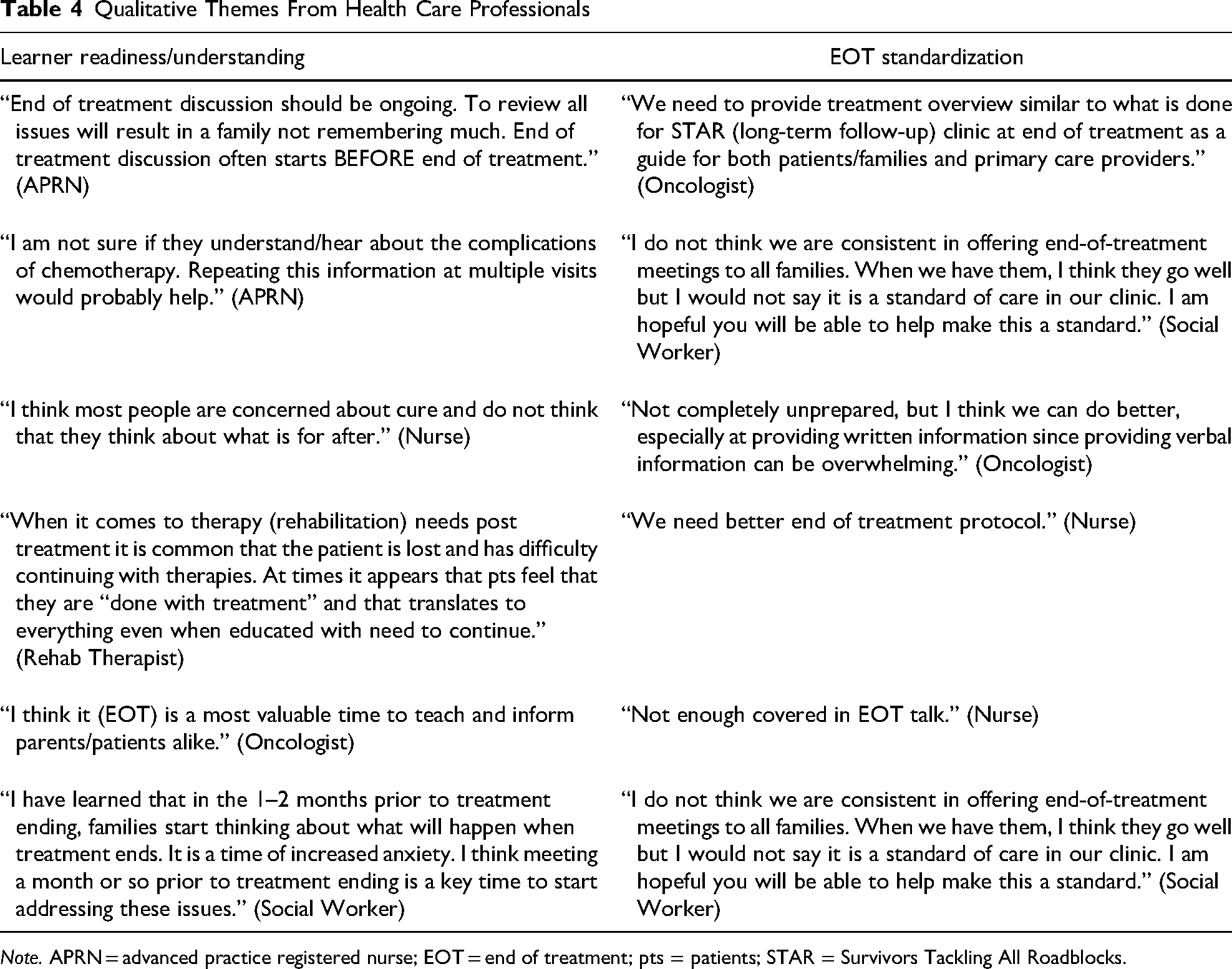
Note. APRN = advanced practice registered nurse; EOT = end of treatment; pts = patients; STAR = Survivors Tackling All Roadblocks.
Concepts of learner readiness and family understanding were identified by HCPs as important considerations when preparing CCSs and parents for EOT and survivorship. Many had suggestions for program timing, which included presenting services at the treatment end or in the 1–2 months prior to treatment ending, as the EOT period was recognized as a time of increased anxiety for families, which they described as negatively impacting learning. Respondents also identified the need to provide EOT information over several visits to improve understanding and recall as well as decrease the chance of overwhelming families with too much information.
According to HCPs, the current EOT education was inconsistently provided to CCSs and families. In an effort to mitigate negative outcomes, such as healthcare service inequity and negatively affecting understanding, HCPs recommended standardizing the EOT process, including content, into a formal and more organized program.
Discussion
This research identified current EOT services from the perspectives of both the recipients and providers of care. It further explored whether the services were meeting the needs of CCSs’ and parents by assessing satisfaction with and preparedness for the EOT transition period.
While the majority of parents/caregivers and AYAs recalled receiving care at EOT, results from this study highlight that formal, comprehensive EOT services were not universally provided or received. This inconsistency can lead to inequities in health services and less timely delivery of needed care (Lea et al., 2020). It is estimated that family education and support needs at EOT are at a similar level to what they are at diagnosis (Wakefield et al., 2012). Several parents and HCPs in the current study compared psychoeducational needs and services received at diagnosis to services received at EOT, echoing other studies’ findings that preparation is better at the beginning of treatment than at treatment completion (Greenzang et al., 2016; Walker et al., 2020; Wilford et al., 2019).
Participants who received EOT care in this study tended to report greater satisfaction than those who did not and were more likely to feel very prepared for inherent challenges faced during this period of transition. These findings suggest the importance of care offered and received at treatment completion, confirming the conclusions of Shea et al. (2019) that having a specific EOT transition visit with the oncology team is valuable. Almost all family participants wished to receive more EOT services and in various formats. This was echoed by the vast majority of HCPs who agreed, even if they were not providing the EOT services themselves, that services were helpful to families. Verbal and written information, as well as supportive care, are desired and thought to be helpful. Parents/caregivers and, in particular, AYAs in this study favor having more HCPs provide these EOT services, as suggested by the increased satisfaction when a greater number of team members were involved.
The content of the EOT education delivered was characterized by family and HCP participants as being more medically than psychosocially focused, which is likely a result of EOT services being primarily provided by oncologists. Being prepared medically for EOT has been found to be important. Greenzang et al. (2016) concluded that EOT information and support from oncologists are critical when preparing parents for life after cancer treatment. Feeling better prepared for challenges typically faced at EOT can, in turn, decrease parental and AYA anxiety levels (Carlsson et al., 2019; Lea et al., 2021). Results from this study indicate that while important, medical needs are only one area families wish to be addressed at EOT.
While simply recalling an EOT meeting or talk did not predict increased family satisfaction, the amount and content of provided psychoeducational services were significant. Parent/caregiver and AYA satisfaction with a formal EOT experience increased significantly with the number of topics discussed. Conversely, satisfaction significantly decreased in these two groups when topics related to psychosocial support and the late effects of treatment were not discussed. These results offer further evidence regarding the psychoeducational needs of CCSs and parents, and the importance of utilizing a multidisciplinary approach to meet these needs (Jones et al., 2020; Karst et al., 2018; Lea et al. 2020; Thompson & Young-Saleme, 2015).
Half the parents and AYAs and a third of children in this study had unexpected problems or worries after completing treatment, identified through qualitative analysis as unmet educational and psychosocial needs and unexpected physical concerns. These findings are consistent with those of other researchers. Jones et al. (2020) noted physical, practical, and emotional concerns among young adult cancer survivors completing treatment. Parents of CCSs also have unmet informational needs and needs for continued psychological and emotional support following EOT (Carlsson et al., 2019; Walker et al., 2020; Yeung et al., 2021). The self-reported experiences of participants in this study offer rich evidence of the multifaceted concerns and needs of CCSs and their parents/caregivers at the time of EOT.
It should be noted that very few children participating in this study recalled having an EOT talk following the completion of their treatment. This may indicate services were not provided, or that when services were offered to families, young children were not the intended recipients. Offering developmentally appropriate EOT information and support to all CCSs is important and necessary, as indicated by the many children in this study who identified worries for which they felt unprepared.
Interestingly, HCPs were more likely to talk about the EOT process in their open-ended responses; that is, when or how often information should be presented, standardization of the service, and learner readiness and understanding. This is in contrast to the responses of parents and CCSs, which are overwhelmingly related to program content. Survivors and parents felt unprepared for new or lingering side effects and for the anxiety and fear they experienced, requesting continued psychosocial support. CCSs of all ages, and their parents, described situations which could have been mitigated with the provision of anticipatory guidance. These responses suggest that families are not overwhelmed with the amount of information they receive, as some HCPs feared in their open-ended responses. Families are asking for more information and support, and are likely to be more satisfied the more they know and have an opportunity to discuss.
Limitations
Despite the high participation rate in this study, the overall sample size was small. This limited the number and strength of correlations and conclusions drawn from participants’ responses. Almost 68% of CCSs were male, which is higher than the international average of 58% (Steliarova-Foucher et al., 2017). At the time of this study, 59.5% of the pediatric oncology program patients on active treatment at this institution were male. However, more males happened to complete therapy during the study period than females.
Selection bias due to the requirement that participants speak and read English, and due to the study being performed at a single institution, led to a fairly racially and ethnically homogeneous study sample. This limits the generalizability of results. The EOTQ instrument is relatively new and needs further testing for validation in broader populations. For example, many children answered questions regarding topics they recalled being discussed as part of the EOT talk, even though they had not, or did not remember, having that EOT talk. The reason for this discrepancy is not known. Children may have received information and support in a format not recognized by them as a structured “talk,” or they were not included as full participants in the discussion, and gleaned these services informally, or they may have tried to answer all questions, rather than skip those that did not apply to them. EOTQ sensitivity when used in this younger age group needs to be explored more closely.
Due to small variations in the wording/rating scales of the EOTQ-HCP from the other instruments, a direct comparison analysis of some responses between those of HCPs and those of CCSs and parents was not possible. Revisions to the instruments will correct these variations and improve the usefulness of these instruments to compare responses between groups.
Implications for Practice
The responses of CCSs, parents, and HCPs in this study are universal in their request for more EOT education and support services. Multidisciplinary team members are being called to work together to provide formal services that meet the complex needs of CCSs and parents at this critical transition point. Development of postoncology care guidelines and standardization of comprehensive EOT services, which could better prepare families for posttreatment challenges and improve medical and psychosocial outcomes (Chan et al., 2019; Greenzang et al., 2016; Jones et al., 2020; Karst et al., 2018; Lea et al., 2020; Walker et al., 2020), could help resolve these service gaps.
This study provides information to consider when developing and tailoring EOT services to meet the expressed needs of CCSs and parents/caregivers. Quantitative results suggest that offering services that provide health care education, anticipatory guidance, and psychosocial assessment and support will increase satisfaction, and may improve the reintegration process into life after cancer treatment. Qualitative results reinforce these findings and offer specific suggestions for developing program structure, timing, and content. Nurses, who are often coordinators of care, are in a key position to develop and implement these services and make them a routine aspect of follow-up care.
With many children and AYAs reporting worries following treatment completion, an opportunity exists to incorporate appropriate anticipatory guidance, support, and information to CCSs of every age and developmental level, including young survivors.
The potential for EOT services to have positive, health-promotive effects should also be explored. Further research is needed to identify the benefits of/barriers to addressing the social and emotional needs of CCSs and parents at EOT, and how services influence short and long-term coping, resilience, HRQOL or engagement in future long-term survivorship care.
Conclusion
Based on the experiences described by CCSs and their parents/caregivers who participated in this study, the end of cancer treatment requires a more standardized, comprehensive approach with increased education and support services to promote the successful navigation of all families through this period of transition. Services offered at EOT impact family members’ satisfaction. This has implications for adaptation and coping. Recognizing EOT as an important time point along the cancer-survivorship pathway and marking the occasion with psychosocial and educational services provide CCSs and parents recognition of their accomplishments while offering guidance and support for the significant transition from treatment to recovery and into longer-term survivorship (Al Ghirwati et al., 2020; Shea et al., 2019; Walker et al., 2019). The results of the quantitative portion of this study are strengthened by the elicitation of HCP's practices and impressions, and comparing these with experiences from CCSs and parents, including the experiences of children as young as 8 years, as described in their own words. The voices of those who participated, providers and recipients of care, alike, and the quality and thoughtfulness of responses, add to the understanding of the pediatric oncology and survivorship experience. Results from this study highlight the unique opportunity HCPs have to help prepare CCSs and their families for the physical and psychosocial challenges commonly faced during the EOT transition period.
Footnotes
Acknowledgments
We sincerely thank the child cancer survivors, their parents, and our oncology colleagues, who participated in this study. We also thank Drs. Ruth Lucas and Stephen Walsh for guiding us as we developed this research project and for assistance with data analysis. We gratefully acknowledge Courtney King and Tiffany Ruiz, two nurses who helped launch this study and worked so well with research participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Authors disclose the following financial support: DAISY Foundation (grant: JPB-2017–11A).