
Abstract
Introduction
Cancer is a life-threatening disease and receiving a diagnosis of cancer during adolescence presents unique challenges. For adolescents and their families, navigating this unchartered territory involves confronting and coping with medical, psychosocial, and educational challenges. Adjusting to this “new normal” is compounded by the numerous changes occurring during adolescence, the transitional phase of growth and development between childhood and adulthood. Thus, a cancer diagnosis interrupts adolescent development during the critical formative years and inflicts considerable stress, resulting in unique psychosocial needs different from those of children and adults (Coccia et al., 2018). Historically, adolescents diagnosed with cancer have been an underresearched population (Smith et al., 2019).
With increasing numbers of pediatric cancer survivors, attention has been placed on the need to develop and implement psychosocial care for adolescent cancer survivors inclusive of school-related needs. Adolescents diagnosed with cancer often require intense therapy with repeated and lengthy hospitalizations. Frequent hospitalizations and doctor appointments disrupt attendance at school, social, and community events impacting interactions with peers, family, and community members. Absence from school is common as a result of the disease, treatment, and side effects (Brand et al., 2017), thus affecting school participation and resulting in time spent away from teachers, classmates, and usual support systems. Without close peer relationships, isolation and loneliness can develop (Christiansen et al., 2015). Missing school and classmates can be distressing, especially at a time when peers play an important role in social development and social support. In a scoping review on the importance of the school setting in connecting adolescents with cancer to peers, disruption in peer relationships was a major worry for adolescents on treatment (Greenblatt & Saini, 2019). For many youths with cancer, school attendance is significantly lower during treatment and for some, absences continue even after therapy has been completed (French et al., 2013). Absenteeism, irrespective of cause has been linked to long-lasting negative academic outcomes (Ginsburg et al., 2014), negative health outcomes, social consequences, and risky behaviors (Allen et al., 2018; Eaton et al., 2008; Epstein et al., 2020; Gottfried, 2014).
School plays an essential role in academic and social development. This is evident in two decades of research exploring the protective nature of school connectedness during adolescence. One of the most widely recognized definitions of school connectedness is from the Wingspread Declaration on School Connectedness (2004): “school connection is the belief by students that adults in the school care about their learning as well as them as individuals.” The Centers for Disease Control and Prevention (CDC, 2009) expanded the definition of school connectedness to include the belief by students that, in addition to adults, peers in their school also care about them. Research across multiple disciplines indicates that school connectedness is important in adolescent development. Specifically, school connectedness has been shown to be a protective factor associated with improved health, behavioral, and academic outcomes in adolescents (Blum, 2005; Resnick et al., 1997). For example, the health benefits of school connectedness are supported in a robust body of literature in general and subpopulations (e.g., vulnerable youth), demonstrating that those who felt connected to school were less likely to have emotional distress (Foster et al., 2017; Monahan et al., 2010; Resnick et al., 1997; Steiner et al., 2019) and reported fewer depressive symptoms (Foster et al., 2017; Joyce, 2019; Markowitz, 2017; Wilson et al., 2018; Zhu, 2018). Moreover, adolescents who reported high levels of school connectedness had improved academic performance (Connell et al., 1995; Monahan et al., 2010; Pate et al., 2017; Stewart, 2008).
Importantly, for adolescents newly diagnosed with cancer, decreased contact with the school, teachers, peers, and social networks as well as cancer-related factors may lead to diminished school connectedness. Yet, to date, there is only one published study specifically exploring school connectedness in adolescents recently diagnosed with cancer (e.g., at least 2 weeks from diagnosis but no more than 10 weeks). Dovi et al. (2020) found school connectedness was already lower at baseline in youth with cancer compared to their peers and remained so at the 3-month time point. Notably, the study did not explain why school connectedness was lower, whether school intervention or support services were implemented, or if the level of school connectedness changed upon return to the classroom. Absent from the literature is the meaning, dimensions, and explanation of the phenomenon of school connectedness when one is not physically present at school.
This qualitative study sought to uncover the nature of school connectedness and generate an explanation of the social problems confronting adolescents newly diagnosed with cancer in the context of school. This study aimed to explore how adolescents newly diagnosed experience school connectedness and the nature of connections to school personnel (e.g., teachers, tutors, guidance counselors, coaches), classmates, and peers. Methodologically, dimensional analysis offers an opportunity for an in-depth exploration of school connections by unraveling and then weaving together the meaning of this phenomenon.
Method
Dimensional Analysis
Dimensional analysis rooted in symbolic interactionism was developed by Leonard Schatzman as an alternative method for generating theory grounded in qualitative data (Schatzman, 1991). Using this method, the researcher aims to break down a complex social problem by identifying key dimensions and their relationships, to gain a deeper understanding of the phenomenon under study. In this study, the interactionist dimensional analysis method was used to explore the meaning of school connectedness from the adolescent's perspective. How do adolescents newly diagnosed with cancer see themselves as students and how do they imagine they are seen by others? Research that addresses this question and asks, “What all is involved here?” (Schatzman, 1991, p. 310), lends itself to the dimensional analysis method.
Research Design, Setting, and Participants
Adolescents diagnosed with cancer from a single teaching hospital were recruited to participate in this study. The teaching hospital site included a pediatric outpatient oncology clinic and in-patient oncology unit and was located in a suburban, northeastern area. Inclusion criteria for the study sample were as follows: (a) aged 10–19 years at study entry (b) received the diagnosis of cancer between ages 10–19 years, (c) English-speaking, and (d) able to provide informed consent or assent when necessary. Adolescents interested in participating in the study were asked to contact the researcher via information in the recruitment flyer. Using purposive sampling initially, adolescents diagnosed with cancer who met the criteria were selected to commence interviews. As the study progressed, the data sources were broadened to facilitate full variation and range of concepts through theoretical sampling (Kools et al., 1996). In alignment with dimensional analysis, theoretical sampling, a sampling technique, guided recruitment of participants whose perspective provided additional understanding of developing concepts and emerging theoretical relationships (Conlon et al., 2020). For example, the dimension of school days and ways emerged after interviewing several adolescents who were newly diagnosed while in middle school, the researcher then decided to expand data sources to further expand this dimension by sampling students who were in high school at the time of the new cancer diagnosis.
Ethical Considerations
Institutional Review Board approval was obtained from the researchers’ university and procedures to protect human subjects were followed throughout the study. Statements informing participants of their rights and permission to audio/video record the interview were expressly written in the consent form. Informed consent was obtained from each participant as well as assent and parental consent when necessary.
Data Collection and Procedures
Data collection unfolded using flexible methods aligned with qualitative procedures to (a) gather self-reports via interviews and observation data, (b) record notes and memos, (c) transcribe data, and (d) manage data securely. Data sources consisted of a demographic questionnaire, video/audio interviews, observations, verbatim transcriptions, and theoretical, methodologic, and personal notes. The interview guide consisted of open-ended broadly structured questions and probes to assist the researcher in directing and shaping the interview while allowing for an emergent and flexible approach (Charmaz, 2014). The main questions and probes for participants included comparisons of student life, school participation, school relationships, and academic performance before cancer and at the time of diagnosis. Interview questions focused on school experiences and connections precancer and at the time of diagnosis during their absence from school (prior to school reentry). The interview guide was refined during and between interviews based on participant responses and in alignment with theoretical sampling (Conlon et al., 2020). For example, the initial question asking “Tell me about your school” was expanded and the researcher probed for dimensions of the concept of school environment (e.g., school space, classrooms, atmosphere, and/or vibe). In-depth, one-on-one interviews were conducted remotely via Zoom© from June 2021 to December 2021 and were audio and video recorded with permission. Interviews were conducted from a private office located on the researcher's university campus and participants were instructed to select a private, comfortable, and convenient location. Most interviews were conducted individually (only one participant requested that their mother be present during the interview). Interviews lasted from 25 min to 86 min, averaging 46 min. The transcription process involved using the audio transcript option available in the Zoom© conferencing platform. The transcriptions were downloaded, listened to, reviewed, and corrected by the researcher ensuring word-for-word accuracy. NVivo©, a software program, was used to store, organize, and categorize data obtained in the interviews. Data collection ceased when theoretical saturation was reached (Charmaz, 2014; Conlon et al., 2020).
Data Analysis
The Process of Dimensional Analysis
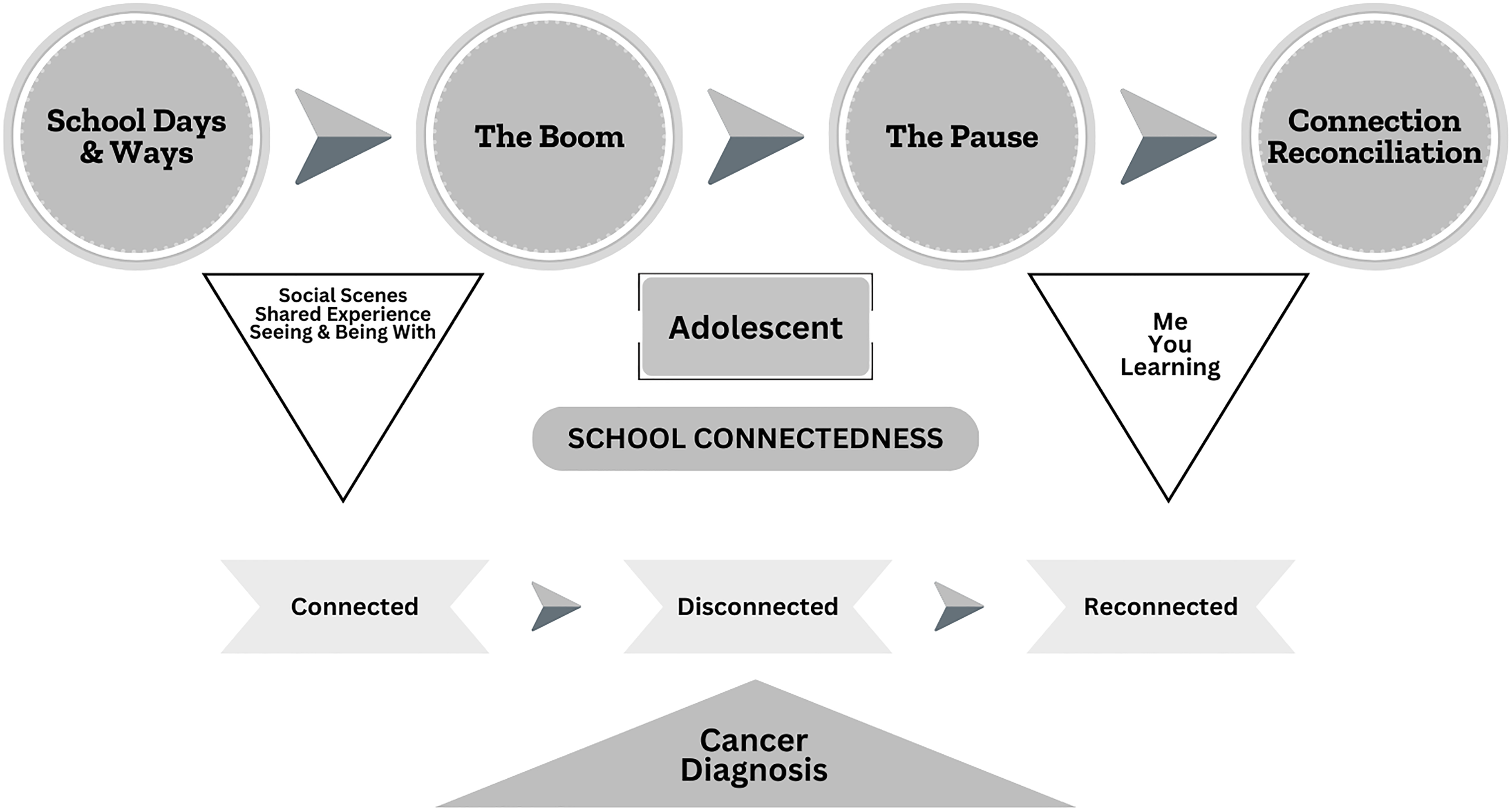
Following the dimensional analysis method, data collection and analysis occurred simultaneously (Kools et al., 1996; Schatzman, 1991). The iterative process of data analysis involved reading and rereading transcripts, coding (e.g., open, axial, and theoretical), and memoing. The researcher used constant comparative techniques and dimensionalizing throughout the analysis to refine the meaning of codes and direct analytic decision-making. This technique allowed for the discovery of concepts by combining data collection, coding, and analysis, and involved comparing data points to one another, across the whole data set, and with emerging theory (Glaser, 1965). Verbatim transcripts were read, interview audiotapes listened to, and transcribed data coded to identify dimensions, which represented emerging concepts and themes. During this early stage of data analysis, word-by-word and line-by-line analysis occurred. After several additional interviews, it became clear that themes were emerging, dimensional analysis began, and continued throughout the analytic process. Through dimensionalizing, data were fractured (e.g., codes broken free from context) with the purpose of building a vast list of words or meaning units directed toward answering the research question. Dimensions were subdimensionalized to fully explore the data and identify the properties of each (Kools et al., 1996). Open codes were sorted, condensed, and grouped into axial codes. Theoretical codes emerged from and through patterns of axial codes and were further refined and differentiated. When no new dimensions served in further explaining the phenomenon under study and in answering the research question, it was determined by the researcher in collaboration with faculty mentors that theoretical saturation was achieved (Kools et al., 1996). In accordance with dimensional analysis, the researcher used Schatzman's (1991) analytic tool, termed, the explanatory matrix to organize and distinguish the dimensions of the nature of school connectedness and advance analysis from description to explanation. The finalized dimensions represent the synthesis and reintegration of school connectedness from the perspective of adolescents newly diagnosed with cancer (see Figure 1).
School connectedness
Rigor
Steps to ensure trustworthiness were taken throughout this qualitative study. In order to meet standards of rigor, careful attention to credibility, transferability, dependability, and confirmability (Lincoln & Guba, 1985) was rendered. The researcher met weekly with an experienced qualitative researcher to discuss theoretical and methodologic notes and the resonance of findings. Additionally, the researcher engaged in frequent dialogic engagement sessions with faculty experienced in dimensional analysis methodology and its coding techniques. Working closely with faculty mentors, prolonged engagement with the data, use of an audit trail, and following the dimensional analysis method attentively, enhanced methodologic rigor. Engagement with researchers and experts in pediatric oncology, including pediatric nurse practitioners and physicians increased the trustworthiness of this inquiry.
Results
Participants
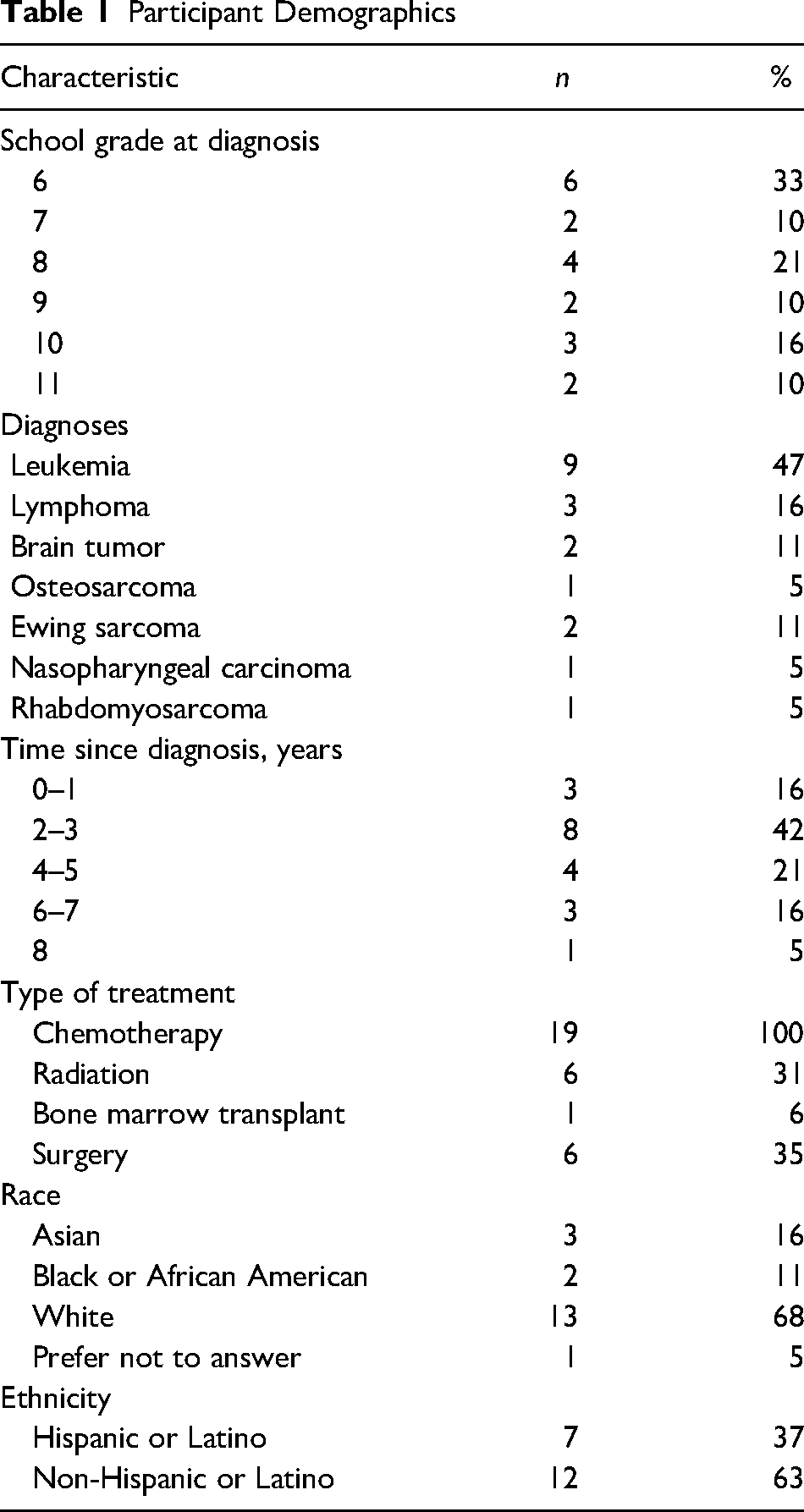
The 19 participants interviewed in this study were adolescents attending middle (n = 12) or high school (n = 7) at the time of their new cancer diagnosis. They ranged in age from 12 to 19 years with a mean age of 16 at the time of the interview. Ten participants identified as male, eight as female, and one as nonbinary. The most frequent diagnosis was leukemia (n = 9, 47%) and most participants had completed treatment (n = 14, 74%). Eight adolescents were diagnosed prior to COVID-19 and received in-person home instruction prior to school reentry. Eleven adolescents were diagnosed during the COVID-19 pandemic school years of 2019–2021 and received home instruction remotely prior to school reentry. Fifteen adolescents had physically returned to school at the time of the interview. Additional demographics are included in Table 1.
Participant Demographics
Participants describe the context of school connectedness across three dimensions, “school days and ways,” “the boom,” and “the pause.” Importantly, “school days and ways” unveils the subdimensions “social scenes,” “shared experiences,” and “seeing and being with,” collectively creating the environment that school connectedness (e.g., school connections and relationships) exists for adolescents prior to receiving a cancer diagnosis. “School days and ways” is important contextually because it is universally interrupted and disrupted by the new cancer diagnosis and, subsequently, “the boom” and “the pause.”
School Days and Ways
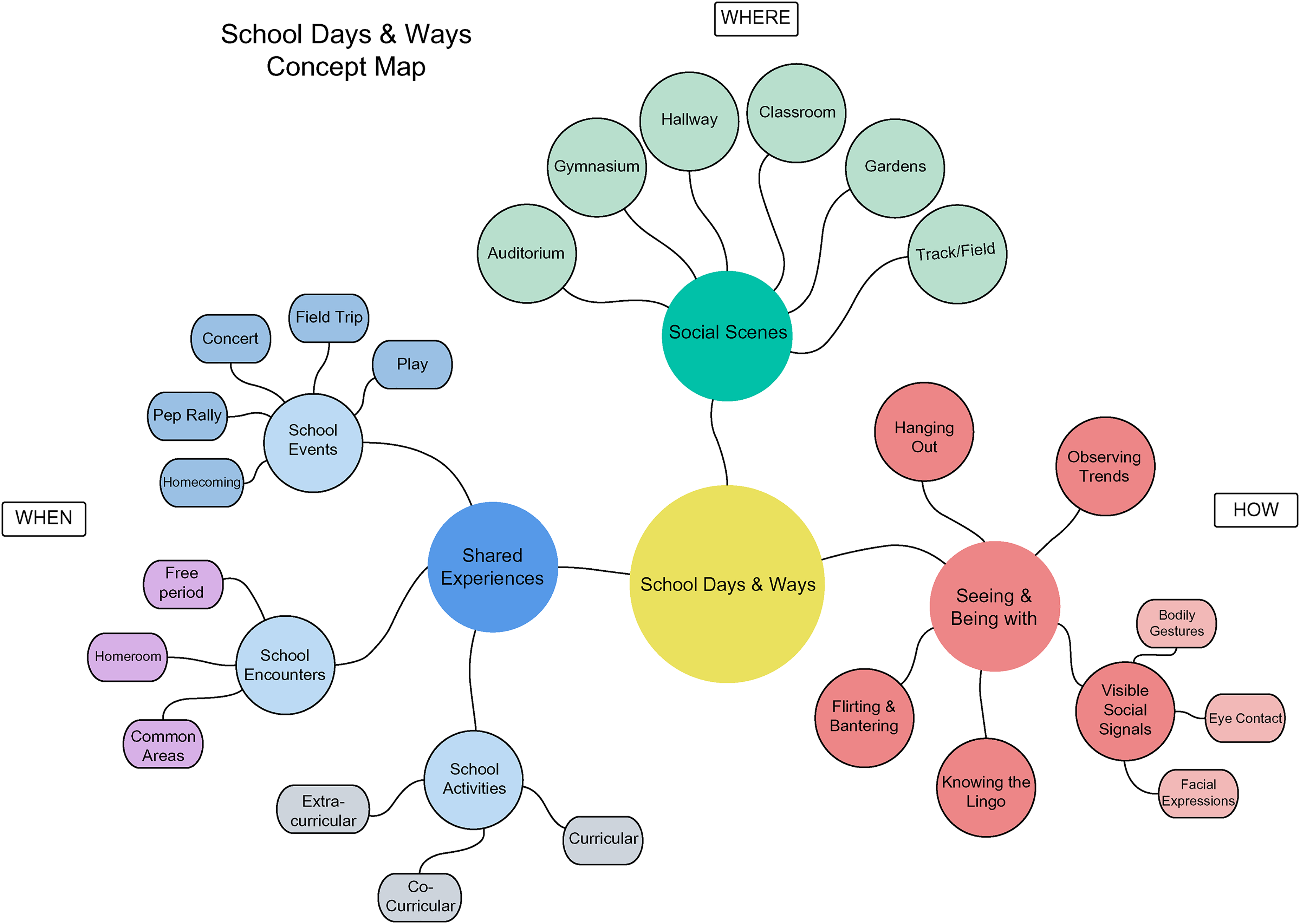
“School days and ways” comprises the expectations of adolescents’ roles and responsibilities pertaining to school life preceding their cancer diagnosis. It reflects typical and predictable school routines as illustrated by one 15-year-old male (03) as he describes school life in the in vivo code, “rinse and repeat.” Specifically, “school days” refers to expectations and routines of time and attendance. It reflects the expected period of time, and the structure of the time adolescents spend at school: (a) duration, the number of hours present in a day, (b) frequency, the number of days in attendance, and (c) schedules, the number of classes and minutes enrolled with traditional, flex periods, or hybrid days. “School ways” characterizes both the manner in which adolescents are expected to behave, and adolescents expect schools to operate. “School ways” embodies social interactions that occur before, during, and after classes in and around the school building. Taken together, school days and ways characterize the context in which adolescents are connected to time, places, people, learning, ideas, or things at school. This contextual dimension is further subdimensionalized into the where, when, and means by which precancer school connections occur (see Figure 2).
School days & ways contextual dimension and subdimensions
Social Scenes
These are the locations where school connectedness takes place. In this study, precancer social scenes included the school milieu: classrooms, water fountains, auditoriums, gymnasiums, at the track, or in school gardens. All adolescents described interacting and being physically present at a variety of school social scenes. In addition to the physical setting, a positive school atmosphere also created space for school connections. Most adolescents described their precancer school atmosphere or school vibe in positive terms ranging from “easygoing,” “relaxed and chill,” to “welcoming,” “happy,” and “filled with positive energy.”
Shared Experiences
The next subdimension refers to the instances school connectedness occurs for adolescents prior to the cancer diagnosis. “Shared experiences” reflect times when adolescents interact and exchange with schoolteachers, staff, friends, and classmates, thus building school connectedness. The findings suggest that these opportunities exist during school events, encounters, or activities. School events include school happenings such as field trips, concerts, homecoming celebrations, and/or pep rallies. School encounters may also take place during a free period, during homeroom, or after school. School activities include those that are curricular, cocurricular, and extracurricular. All adolescents in this study participated in some school activities on a regular basis prior to their cancer diagnosis.
Seeing and Being With
The last contextual subdimension refers to the precancer experiences and means through which school connectedness happens. “Seeing and being with” refers to spending time in the presence of, and/or being active with others, objects, and occurrences. Adolescents describe “seeing and being with” examples such as hanging out, observing trends (e.g., fashion, music, technology/social media), and bantering at school. Importantly, this subdimension illuminates the visible social signals, such as facial expressions, body gestures, and eye contact through which school connections develop.
The Boom
The in vivo code “The Boom” reflects the setting in which previously healthy adolescents experience learning about their new cancer diagnosis. It captures the upending, forceful, and sudden knowledge of having cancer. The alarming news and the severity of the illness place adolescents in a vulnerable position, questioning their identity, current situation, and future. One 18-year-old male (010) illustrates “The Boom” as he describes his cancer-related fears and his health, “I was pretty scared at first, because my grandpa had like lung cancer, so I was just kind of like stunned and shocked, it's like a healthy 16-year-old, just like suddenly gets cancer.”
“The Boom” not only interferes with the adolescents’ developing a sense of identity but also their ability to make their own decisions and act autonomously. One 17-year-old male (03) reflects on his feelings of dependency and struggle to make it on his own, “I just felt like, a guy who lives in their parents’ basement.” Moreover, “The Boom” impacts parent–adolescent relationships potentiating tension regarding the adolescents’ need for time, space, and privacy, especially when they are not feeling well.
The Pause
The in vivo code, “The Pause,” the final contextual dimension, occurs when adolescents experience an interruption and disruption in their school life (e.g., the time spent at school and the social interactions that occur during school activities). It reflects the adolescents’ actual or perceived loss of connections to school time, people, and learning. One 17-year-old female (011) illustrates “The Pause” as she describes her lack of movement, both physically and socially: But if I had a sport, like dance, I had to stop doing it because I would be nauseous and like out of breath all the time, so I wasn't able to continue that so it's like everyone's life is continuing and mine was just like pausing. I was very upset that I couldn't do that (go to pep rally), and then I wasn't allowed to go to the chorus concert, because if you stepped foot on the property of the school, then they would stop the homeschooling. So, like I wasn't even able to go like see the concerts or like be a part of it.
For an 18-year-old female (06) “The Pause” presented through her realization that she may not be part of her previous social group due to the fact she was away receiving cancer treatment:
But for the most part, when I wasn’t, you know, when I kind of went MIA, they were like ooh, what's going on with [her]? You know is she okay? They had no idea what was going on with me. I kinda had the sense of like, okay, well I know they don’t understand.
Moreover, some adolescents self-impose restrictions intensifying “The Pause” as they prefer to socially isolate due to personal distress related to perceived changes in their appearance and/or bodily functioning. In particular, adolescents express apprehension regarding hair loss. Because of body image concerns, adolescents are reluctant to be seen, as one 19-year-old female (013) shares her reasons for socially isolating, “I didn’t want them to see me without hair. I didn't post or let anyone see me for a while, without hair, that was like the one thing that I didn't want people to know.” Being isolated and/or being unable to relate to others as previously is distressing for adolescents who are trying to fit in and find acceptance amongst peers.
Importantly, school absences, nonexistent class or group participation, social isolation, and lack of proximity, all contribute to losses (e.g., of time, place, or opportunity) that impact adolescents’ ability to feel close to others at school. Unsurprisingly, almost all adolescents in the study verbalize that they miss being with and seeing teachers, classmates, friends, and/or other school personnel. This analysis uncovers that adolescents want, need, and expect to participate in particular experiences in order to connect to school. However, the new cancer diagnosis interrupts and disrupts school relationships, halting the adolescents’ opportunities to connect and impeding their ability to do so.
Connection Reconciliation: Me, You, and Learning
The central code, “Connection Reconciliation: Me, You, and Learning” characterizes adolescents’ desire as social beings, to establish meaningful relationships and their intention to restore harmony and balance while confronting a new cancer diagnosis. “Connection Reconciliation: Me, You, and Learning” speaks to the adolescents’ drive for normalcy, continuity, stability, structure, and a sense of purpose. It is a dynamic state, encompassing the circumstances and motives, wherein adolescents reconcile connections with self, others at/from school, and learning amid a new cancer diagnosis. For clarity, each aspect is described separately.
Connection Reconciliation: Me
This aspect captures the adolescents’ drive to see themselves, identities, and roles coherently. “Connection Reconciliation: Me” embodies the restoration of adolescents’ relationship to self in the midst of hardship. One 18-year-old male (010) recalls: And it's just kind of a shock, but it was just more, it was like a lesson. I will call it a lesson, it taught me a lot about myself, and what I can do, and what I have to do to be like successful in life. It was a stressful time, I could say that. But I knew, when I was going through it at the very beginning, I just knew I had to keep on going, no matter what. I decided to support myself with good positive thoughts. I talked more, I became more sociable with people around and I started to act myself, more than when I was in school. I gotta be honest with that, like even though cancer is a diagnosis, it helped me a lot throughout my journey, in my life.
Importantly, “Connection Reconciliation: Me” captures the adolescents’ new understanding of self as a student living with cancer.
Connection Reconciliation: You
Along with restoring relationships with self, this aspect illuminates the adolescents’ desire for social acceptance, and the need to fit in and relate to peers and others at/from school. A 19-year-old female (013) shares how hospital visits helped her reconnect to classmates, “If I was having like a bad day or If I was upset, and they would come over and try to cheer me or come to the hospital and distract me.” “Connection Reconciliation: You” embodies the adolescents’ restoration of school relationships. This is illustrated by a 16-year-old female (019) as she describes how she enjoyed her science teacher's individualized instruction: But I think the most fun was science because my science teacher would bring like a microscope to the hospital, and she would bring like these lab experiments for me to do, so I’d be able to take the Regents.
Connection Reconciliation: Learning
The last aspect speaks to the adolescents’ need for competence, productivity, sense of purpose, and academic achievement. “Connection Reconciliation: Learning” characterizes the adolescent's desire to grow and develop, to move forward intellectually and academically. It embodies the restoration of adolescents’ relationship with learning. Despite the new cancer diagnosis, reconnecting to learning is presented in the adolescents’ endeavor to put forth their best effort. As one 17-year-old (08) describes their determination to reach their highest potential, “Because I really wanted to be the best version of myself, I could be, and I really worked hard for it, even if I failed, a lot of the times, especially in math.” Even though adolescents describe academic challenges related to falling behind with schoolwork, most are able to “catch up” and maintain or improve grades by reconnecting to learning through homebound instruction. “Connection Reconciliation: Learning” reflects the adolescents’ drive for structure, stability, continuity in education, and academic progress and their need to reconcile changes in their learning abilities, learning environment, and instructional delivery.
Discussion
From the perspective of adolescents, this study reveals the nature and context of school connectedness prior to and following a cancer diagnosis. It expands the breadth and depth of the meaning of school connectedness and adds to the body of knowledge in adolescent, cancer, and education literature. One of the most salient findings uncovered in this research is that adolescents newly diagnosed with cancer reconnect to self by accepting and embracing their identity and dual roles of both patient and student. They create reality through interactions with self and others and create shared meanings of the world around them. Through these interactions, adolescents develop a sense of identity based on their interpretations and how they make sense of their cancer and school worlds. These findings align with symbolic interactionism theory (Blumer, 1969), whereas individuals have an innate desire to belong and are constantly striving to maintain their identities. The adolescents in this study, as social beings attempted to figure out how to fit in with and reconnect to their peers, teachers, and others at/from school. In a more recent study, An and Lee (2019) examined the return to social life in 14 adolescent and young adult leukemia survivors using grounded theory methodology. The researchers identify the core category as fear of recurrence which was not found in the current analysis. However, their findings illuminated concepts and processes (e.g., catching up with others, discovering myself, and planning my future) consistent with the findings of the current analysis. For example, discovering myself was characterized by completing one thing at a time, discovering abilities, accomplishing tasks, belonging, and appreciation for peers, teachers, family members, and healthcare providers (An & Lee, 2019). Moreover, the findings of this analysis are similar to the phenomenon of school connectedness most often described in the literature involving healthy students and having relational elements (Bowles & Scull, 2019; CDC, 2009; García-Moya et al., 2019; Goodenow, 1993; Wingspread 2004) and performative elements (Bowles & Scull, 2019). However, this vast body of research measures school connectedness by items representing school relationships, environment, and participation in school activities and/or athletics, in the context of physical school presence and/or involvement. For example, numerous school connectedness instruments include various questions regarding school attendance (Woolley & Bowen, 2007), feeling safe at school and happy at school (Loukas et al., 2010; Prado et al., 2009) or enjoyment at school (Karcher, 2011), and participation in sports or other school activities (Lohmeier & Lee, 2011). However, these measures and their frame of reference do not align with school connectedness in adolescents newly diagnosed with cancer who are not attending school. Regarding the results of this analysis and its relationship with the theory of adolescent connectedness (Karcher, 2011), several distinctions should be noted. Karcher's theory (2011) suggests that adolescents connect to others through affective (e.g., caring) and behavioral engagement (e.g., actions), comparable to the findings of the current study. Important to Karcher's theoretical framework are the concepts of adolescent worlds or social ecology (e.g., self, school, family, friends), temporal orientation (e.g., present and future-oriented), and the notion that connectedness is the adolescents’ response to feelings of belonging and relatedness (Karcher, 2011), again similar to the current study. According to Karcher and colleagues (2008), connectedness is characterized by adolescents’ relationships, activities, and contexts, which are meaningful (e.g., positive, valued, and significant).
Importantly, the findings of this study have implications for nursing practice and may guide nursing care provided by pediatric oncology nurses and school nurses. Nurses are positioned to support the medical, educational, and psychosocial needs of these adolescents. Nurses can provide anticipatory guidance and screening for school-related issues. By building rapport, nurses can teach self-advocacy and encourage adolescents to practice articulating their wishes, wants, and expectations for school so they stay on track academically. Importantly, nurses can collaborate with hospital psychologists, social workers, and child life specialists, to support the adolescent in brainstorming ways to engage with school life during home-schooling. Moreover, acting as a liaison between family, treatment team, and school, pediatric oncology nurses can provide information and updates to school educators and school nurses bridging the gap during school absences.
While this research contributes to the understanding of school connectedness from the perspective of adolescents newly diagnosed with cancer, there are several limitations. This study was limited to a select sample of 19 adolescents diagnosed with cancer and treated at one university hospital, living and attending school in a geographically similar location. Notably, the sampling goal sought to include a diverse population of adolescents. And in fact, there was heterogeneity regarding types of cancer, age, and grade at diagnosis. However, the final sample consisted of predominantly White (68%) and non-Hispanic adolescents (63%). Thus, the sample may not be representative of the overall population. Future research exploring school connectedness in additional samples that include more diverse populations, geographically, ethnically, and socioeconomically will deepen knowledge of the phenomenon. The understanding of school connectedness and school relationships is timely and of paramount importance as educators and mental health practitioners respond to the isolating effects of the COVID-19 pandemic and its impact on the mental, behavioral, and academic well-being of our youth. Future studies exploring how to help adolescents newly diagnosed with cancer feel supported and connected to school are warranted.
Footnotes
Acknowledgments
The author gratefully acknowledges the adolescents who agreed to participate in this study. Special thanks to Carol Della Ratta and Clare Whitney, for their expertise and thoughtful critique in developing this manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.