
Abstract
Introduction
Children and adolescents suffer from a constellation of physical and psychological symptoms throughout cancer treatment (Withycombe et al., 2019) and into survivorship (Shin et al., 2022). Research has documented the persistence of fatigue, pain, nausea, insomnia, sadness, and worry in response to disease and/or cancer-directed treatment (Hockenberry et al., 2017; Hooke & Linder, 2019; Linder & Hooke, 2019; Montgomery et al., 2022; Weaver et al., 2022). As a result, the Children's Oncology Group Nursing Discipline has recommended routine assessment of these six core priority symptoms given their prevalence across diagnoses and treatment regimens (Withycombe et al., 2019).
Symptom research has highlighted the variation in symptom experiences across patient populations. Some patients experience frequent and severe symptoms while others experience fewer and more tolerable symptoms. Yet, research that provides possible explanations for differences in symptom experiences is scant (Jibb et al., 2022) and has focused primarily on patient demographic or clinical variables. Investigation of the associations between symptoms and a child's cancer diagnosis, demographics, including biological sex, or proximity to treatment have yielded mixed results. For example, Montgomery et al. (2020) and Wolfe et al. (2015) found descriptive differences in the prevalence of symptoms between cancer diagnoses among children with advanced cancer, while Hinds et al. (2021) demonstrated that in earlier stage disease a child's cancer diagnosis did not predict the severity of their symptom burden. Still, other investigators have found relationships between symptom reports and biological sex, race, and time since treatment (Hinds et al., 2021; Wolfe et al., 2015).
Pediatric oncology researchers have infrequently studied potential biological mechanisms underlying cancer symptoms (Jibb et al., 2022; Mandrell & Withycombe, 2019), despite theoretical support and evidence from adult oncology. The Children's Oncology Group Nursing Discipline identified several biomarkers, including oxidative stress, cytokines, melatonin, and cortisol, for inclusion in pediatric oncology symptom research because of their potential to aid in identifying children at risk for symptom suffering and diminished quality of life (Mandrell & Withycombe, 2019). Research examining biological mechanisms of pediatric cancer symptoms is in an early phase and requires foundational evidence to standardize procedures to collect biospecimens across the care continuum and to demonstrate support for specific symptom biomarkers (Mandrell & Withycombe, 2019).
Inflammation and Stress
Inflammatory and neuroendocrine responses to stress are interconnected biological processes of particular interest in pediatrics given the compelling evidence linking their association with cancer risk, tumor growth, and treatment-related tissue damage in adults. Furthermore, there is growing evidence to suggest that physiological responses to acute and chronic stressors are associated with increased future health risk (O’Connor et al., 2021). The presence of inflammatory cells and mediators in the tumor microenvironment is similar to that observed in chronic inflammatory responses (Germano et al., 2008; Mantovani et al., 2008). Chronic inflammation can result from infectious (e.g., human papillomavirus) or non-infectious etiology (e.g., tobacco use), and has been most notably associated with adult carcinomas (Morgenstern & Anderson, 2012). The role of chronic inflammation in pediatric tumor development, however, is less understood. Children do experience infections early in life and have some environmental exposures, but the types of infections and exposures driving inflammation are different compared to adults, and thus merit further investigation (Morgenstern & Anderson, 2012).
In the context of pediatric cancer, disruptions to homeostasis, including disease and tissue damage secondary to cancer treatment, can lead to acute and chronic inflammation, which may disrupt systems designed to return the body to homeostasis (Davis et al., 2023). When inflammatory mediators overwhelm these homeostatic processes, the result is chronic inflammation. C-reactive protein (CRP) and cytokines are biomarkers used to measure chronic inflammation, directly (interleukin-6 [IL-6], tumor necrosis factor-alpha [TNF-α]) or indirectly (IL-1β, IL-2) (Davis et al., 2023). Cytokines may be categorized as pro-inflammatory or anti-inflammatory and can either upregulate (pro) or downregulate (anti) the immune response.
Homeostasis may also be disrupted when a person experiences stress. Stress exposures can trigger different pathways to maintain or restore homeostasis: (a) the sympathetic nervous system and (b) the hypothalamic-pituitary-adrenal (HPA) axis (Davis et al., 2023). The first pathway is commonly referred to as the “fight or flight” response and typically occurs in response to an acute stressor. Activation of the HPA axis may occur in response to acute or chronic stress (Rohleder, 2019), and leads to the release of glucocorticoids (cortisol) from the adrenal glands in response to adrenocorticotropic hormone release from the pituitary gland. In the case of acute stress, the HPA axis may respond without affecting the overall function of the HPA axis. In contrast, there may be changes in the HPA axis function in response to chronic stress, leading to changes in basal levels of cortisol (Herman et al., 2016; McEwen, 1998). Salivary cortisol and salivary alpha-amylase (sAA) are commonly used indices of HPA axis regulation (Kuhlman et al., 2019). Salivary cortisol is a peripheral biomarker of chronic stress, while sAA is considered a measure of an acute stress response (Davis et al., 2023). Cortisol has been linked to adverse stress-related outcomes, including effects on the cardiovascular, metabolic, and immune systems (McEwen, 1998, 2008).
Inflammatory and stress pathways can be concurrently activated when homeostasis is threatened (Kautz et al., 2020), resulting in dysregulated immune and neuroendocrine system responses. Chronic stress has been shown to be associated with increased circulating plasma inflammatory markers (IL-6, TNF-α, and CRP) and increased inflammatory activity (Rohleder, 2019). Tumor progression in children and adults may be one result of increased stress, leading to alterations in some cytokines (Reiche et al., 2004). It is unknown if increased inflammation is associated with cancer-related symptoms in the context of pediatric cancer and treatment. However, if inflammation and stress contribute to tumor progression and treatment-related tissue damage in adults, they may also be related to symptoms of progressing or advanced disease in adolescents and young adults with cancer.
Stress, Inflammation, and Cancer Symptoms
The Sickness Behavior Model (Dantzer, 2001) identifies a complex cytokine network, which plays a critical role in inflammation and infection, as a potential biological mechanism underlying cancer symptoms. Cytokines then activate the HPA axis, resulting in glucocorticoid release and sickness behavior (Dantzer et al., 1998). Pain, fatigue, sleep disturbance, lack of appetite, and depression are associated with sickness behavior (Dantzer, 2001).
In adult oncology patients, evidence suggests that dysregulation in the cytokine network may lead to symptom co-occurrences (Cleeland et al., 2003; Gilbertson-White et al., 2011; Miaskowski et al., 2007; Wang et al., 2010), resulting in patterns of high symptom burden. However, research exploring biomarkers of inflammation and stress in pediatric oncology is limited. A study by (Vallance et al., 2010) identified a single nucleotide polymorphism (rs1800795) in IL-6 that was associated with increased sleep time in children receiving treatment for acute lymphoblastic leukemia. During off weeks from dexamethasone, patients with the homozygous GG genotype, or two copies of the same allele (GG), had increased sleep time and sleep minutes, suggesting the anti-inflammatory properties of steroids may inhibit the effect of IL-6 on sleep (Vallance et al., 2010).
Little is known about relationships between physiological stress response and symptoms in pediatric cancer. Research in adult oncology patients has identified associations between symptoms and biomarkers, including cytokines (IL-1β, IL-6, TNF-α) (Himbert et al., 2019; Miaskowski & Aouizerat, 2012; Paulsen et al., 2017; Perez-Tejada et al., 2021; L. M. Thornton et al., 2010; Wang et al., 2010) and cortisol (Schmidt et al., 2016; Sharpley et al., 2017; L. M. Thornton et al., 2010; Weber & O’Brien, 2017). These studies are limited by cross-sectional designs, exclusion of children, and exclusive focus on pro-inflammatory cytokines in contrast to anti-inflammatory cytokines (Condon, 2016; Hulett et al., 2019; Mandrell & Withycombe, 2019; Miaskowski & Aouizerat, 2012; Saligan et al., 2015). Research investigating the relationships among inflammation, stress, and symptoms in children, which may vary from findings identified in adults with cancer, is limited.
Given the different causal mechanisms between inflammation and tumor development in children versus adults (Morgenstern & Anderson, 2012), prospective research is needed that evaluates the contribution of the physiological stress response, reflected in inflammatory and neuroendocrine biomarkers, to the development of symptoms in children with cancer (Bower, 2019; Miaskowski & Aouizerat, 2012). Longitudinal studies are also needed to explore associations between physiological stress response and inflammation in children with cancer. However, before research on the biobehavioral mechanisms underlying pediatric cancer symptoms can be conducted, studies must first demonstrate the feasibility of collecting specimens from children receiving cancer treatment across the care continuum.
Purpose
To fill existing knowledge gaps and advance pediatric oncology symptom science, the purpose of the study was to (a) determine the feasibility of collecting blood and saliva samples to evaluate biomarkers of stress and inflammation at three time points in children with advanced cancer, (b) describe the range and distribution of observed inflammatory and stress biomarkers, and (c) explore the association of biomarkers with symptoms.
Theoretical Rationale
The Dynamic Symptoms (Brant et al., 2016) and Sickness Behavior (Dantzer et al., 1998) Models served as theoretical frameworks for the current study and guided the selection of variables and relationships for the study. The Dynamic Symptoms Model identifies biomarkers of the disease and treatment response as physiologic antecedents to the symptom experience (Brant et al., 2016).
Method
Setting, Participants, and Procedure
For this longitudinal, prospective, repeated-measures study, a convenience sample of children with advanced cancer was recruited from a small children's hospital in the upper Midwest. Children and adolescents were recruited over 13 months from the Division of Pediatric Hematology, Oncology, and Bone Marrow Transplant, which provides care to children newly diagnosed with cancer and advanced cancer. The study was approved by the University of Wisconsin-Madison Institutional Review Board. Children and adolescents were eligible if they were aged 2–18, had a diagnosis of advanced cancer, or cancer that was documented by an oncologist as progressive, recurrent, or non-responsive to treatment, and able to understand English. Those who were otherwise unable to complete study procedures were excluded. The target sample size was 10 children and/or adolescents. The sample size was based on the minimum number necessary to establish feasibility and the limited pool of children treated for advanced cancer at our small center.
Symptoms, biomarkers of physiological stress response (salivary cortisol and sAA) and inflammation (cytokine and CRP), and clinical characteristics (disease and treatment variables) were measured at three time points. Data collection time points were determined by the research team in collaboration with the participants and caregivers to ensure adherence to biomarker storage guidelines and occurred during or near a healthcare encounter. The time points and flexible data collection windows were selected to ensure adequate time to assess the feasibility and acceptability of repeated data collection during the advanced cancer course and balance the potential for participant and caregiver burden in the context of an exploratory pilot study. The first time point (T1) occurred at study enrollment. The subsequent time points (T2 and T3) were scheduled approximately 1 month and 2 months after enrollment. The study schema can be found in Figure 1. Because the primary aim was to evaluate the feasibility of repeated collection of biomarker and symptom data, the timing of measurement was not related to a particular time in cancer-directed treatment. Within a specific time point, symptom and biomarker data were concurrently collected within a 2- to 6-day window. The minimum data collection window (2 days) was selected to allow stress biomarkers to be collected four times per day over 2 consecutive days to align with best practices for measuring indices of HPA axis regulation (Adam & Kumari, 2009). Symptom data and blood could be collected concurrently with saliva or up to 6 days after the start of data collection for the specified time point. The goal was to ensure all biomarker data was collected within the recall period (7 days) for the symptom measure. Information about the child's disease status and treatment was collected to support ad hoc analyses (evaluating the association of disease- and treatment-related inflammation and stress response) and future study designs. Participants received $10 for each completed symptom survey and an additional $25 for collecting saliva at each time point. No remuneration was provided for blood collection.
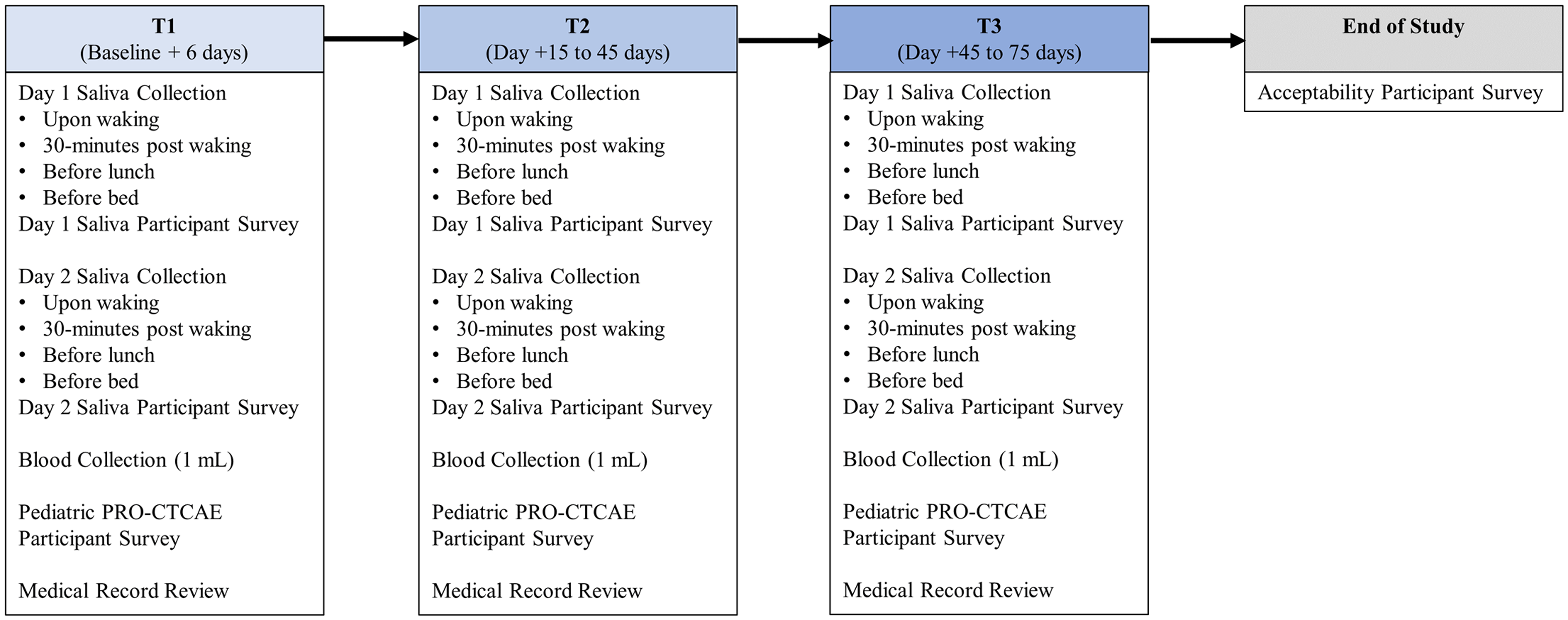
Study schema.
A Research Electronic Data Capture (REDCap®) system was used to collect symptom data from patients who were aged ≥8 years or from caregiver proxies of children aged ≤7 years and to communicate reminders to participants to facilitate the collection of saliva using the survey functionality. The research team used REDCap® to coordinate data collection activities and document information related to biomarker collection (e.g., reasons for missed samples) and clinical characteristics extracted from the medical record.
Measures
Recruitment rates, missingness of blood and saliva samples, sample sufficiency for assay, and missingness of surveys were evaluated to assess feasibility. To assess participants’ perceptions about the acceptability of the study procedures, a brief 15-item survey was administered to participants at completion of the study. Six questions addressed the frequency and method for obtaining symptom assessments and nine questions asked specifically about procedures used to support saliva collection, including clarity of instructions, ease of using study-provided collection kits, adequacy of the reminder system, and challenges.
Participant demographics were measured by extracting information on age, biological sex, race, and ethnicity from the medical record. Participant clinical characteristics were also collected from the medical record. Information regarding participants’ cancer type, disease status (active, remission, recent progression), cancer-directed treatment, treatment history, treatment toxicities, and medications was extracted from the medical record at each time point using a data extraction form used in previous studies by the research team.
For this study, symptom adverse events (AEs) are defined as unintended disease and treatment-related symptoms and include attributes of presence, frequency, severity, and interference/bother. We measured symptom AEs over the past 7 days using the National Cancer Institute's Pediatric Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE) instrument, which contains 15 core and 47 additional symptom AE items. The number of attributes assessed per symptom is dependent on the symptom AE and can range from a single attribute to three attributes. For symptom AEs with multiple attributes, participants only report on all attributes if the first level attribute is endorsed. For example, if participants endorse some level of nausea frequency, then the participant is asked to report on nausea severity and interference. The Pediatric PRO-CTCAE is available as a self-report (children aged 8–18) and caregiver proxy report (children aged 2–7). Symptom AE items were scored using a 0–3 scale, with higher scores indicating greater presence, frequency, severity, and interference. Data have demonstrated acceptable validity, reliability, and responsiveness of the self-report (Reeve et al., 2020) and proxy (Reeve et al., 2021) versions. Twenty-four items were selected from the Pediatric PRO-CTCAE item library and used to measure symptom AEs.
Inflammatory cytokines (interferon-gamma [IFN-γ], IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IL-12p70, IL-13, TNF-α) were measured from participants’ blood samples using the V-PLEX Proinflammatory Panel 1 Human Kit and state-of-the-art electrochemiluminescence detection (Meso Scale Discovery [MSD]). CRP was analyzed through a single analysis using a CRP assay kit from MSD (Human CRP K151STD). A broad list of pro- and anti-inflammatory cytokines were selected for their importance in inflammatory response and immune system regulation and to conduct an unbiased sampling of the secretome. Inflammatory markers were determined using blood plasma. All specimens were run in duplicate, and every assay included a high pool and a low pool of human plasma to monitor and control for inter-assay variation.
Salivary cortisol and sAA were measured as indices of HPA axis regulation using participant saliva. Salivary cortisol is a sensitive and specific measure of biologically active, unbound cortisol (Hanrahan et al., 2006) and has been successfully collected by other investigators from pediatric patients without a diagnosis of cancer (Hanrahan et al., 2006; McCarthy et al., 2009), and adolescents with cancer in the clinical setting (Ameringer et al., 2012). For each day of saliva collection, participants were asked to complete a brief survey answering questions about their current stress exposures, physical activity, food and drink intake, and new medications. Saliva samples were analyzed at the Assay Services core lab at the Wisconsin National Primate Research Center (WNPRC). Cortisol was measured using a Roche Cobas e411 with ECL technology. Quality control was monitored with a low and high pool of human saliva. The intra-assay coefficient of variation (CV) ranged from 1.7% to 5.0% and the inter-assay variation ranged from 3.0% to 12.95%. sAA was measured using a commercially available enzymatic kit (Salimetrics). Quality control was monitored with one pool of human saliva. The intra-assay CV was 2.75% and the inter-assay CV was 0.65%. Salivary cortisol and sAA values were measured upon waking, 30-min post waking, before lunch, and before bedtime.
Procedures
Symptom Surveys
Symptom measures were sent electronically using REDCap® to participants’ or caregivers of participants’ mobile phones via text or email based on preference. The message contained a unique link to complete the symptom measure. Reminders to complete the survey were sent every 2–3 days, with a final reminder call made by the research team on Day 6.
Blood Collection
Cytokines were measured using blood samples. A Registered Nurse obtained a 1 mL blood sample from the participant's central venous access catheter and labeled the specimen with the participant's name, date, and time of the collection. Personnel from the University of Wisconsin Carbone Cancer Center (UWCCC) Cancer Pharmacology Lab Acquisition Services Cancer Pharmacology Lab Acquisition Services were notified by the Registered Nurse to pick up the sample from the clinical care area. After the sample was picked up, lab personnel centrifuged the sample to extract the plasma, labeled the specimen using a study identifier, and stored the plasma in an ultracold freezer (−80 °C) for batch analysis by the Cancer Pharmacology lab.
Saliva Collection
Participants collected their saliva using a cotton salivette swab (Sarstedt AG & Co. KG, Nümbrecht, Germany) (a) upon waking, (b) 30 min post waking, (c) before lunch, and (d) before going to bed at night for 2 consecutive days at each time point (eight samples per participant per time point). A member of the research team provided one-on-one education to the participant and caregiver on how to collect saliva, including information on the length of time to ensure a swab is sufficiently saturated, restrictions on ingesting food and drink before sample collection, documenting sample collection details (specific date and time of collection, and notes to the research team), and storing samples. Each participant received a collection kit in advance of each time point. The collection kit contained printed instructions on how to collect samples, individually packaged and labeled salivettes with storage details and contact information, a worksheet to document sample collection details, and extra salivettes. Using the REDCap® database, participants received electronic reminders via text message the night before the agreed-upon date for starting saliva collection and mid-day of each collection day. The text reminder included a link to an electronic version of the printed instructions and a phone number to call in the event of questions during collection. Participants were instructed to store samples in their home refrigerator when saliva was collected at home or in an insulated pack with ice packs when saliva was collected in the hospital or for transporting samples to their health care encounter for pick-up. The study team was responsible for picking up the samples, reviewing the sample collection worksheet to confirm date and time of specimen collection, affixing a study identifier to each sample, and storing the samples in an ultracold freezer (−80 °C) for batch analysis by the WNPRC. All collection supplies, including coolers and ice packs, were provided to participants at no cost.
Data Analysis
Data were analyzed using Statistical Package for the Social Sciences® Version 29 (September 13, 2022) and Stata 17 (2021). Descriptive statistics were used to examine feasibility, acceptability, demographics, and range and distribution of symptom, biomarker, and clinical data. Frequencies of individual symptom AEs were calculated to select AEs for exploratory analyses and to group participants into groups. Participants who reported a score >0 were placed in the symptom group, while participants who reported a score of 0 were placed in the no-symptom group. The cortisol awakening response (CAR) for each day of saliva collection was calculated by subtracting the value at the time of waking from the value 30 min after waking. The CAR values were then averaged across all participants at each time point. The diurnal cortisol slope was determined using linear regression. The Hedges’ g statistic was used to determine the effect size and explore the relationship between symptom and inflammatory biomarker data. The effect size is the magnitude of the difference between the standardized mean inflammatory biomarker values between the symptom and the no-symptom groups. Hedges’ g assumes unequal variances, which are more likely to occur in small samples with heterogeneity and reduces bias by applying a correction factor (Hedges, 1981). Cohen's guidelines were used to interpret the size of the effect, with values of 0.20, 0.50, and 0.80 for Hedges’s g interpreted as small, medium, and large effects, respectively (Cohen, 1977). Analyses were only conducted for the inflammatory markers with adequate plasma concentrations to optimize interpretation of the findings.
Results
Aim 1: Feasibility and Acceptability
Clinicians approached 11 children and adolescents to determine their interest in participating in the study. Only one declined to participate due to infrequent visits with the healthcare team and “too much going on.” Ten participants consented and completed the study. The mean age of the sample was 12.5 years (4–18). The sample was predominantly male (80%), White (100%), and non-Hispanic (90%). Participants were either diagnosed with a hematologic malignancy (40%) or a non-central nervous system solid tumor (60%). The most frequently occurring symptoms of AEs included fatigue, anxiety, pain, nausea, anorexia, and insomnia. Participants’ disease and treatment characteristics were dynamic throughout the study period. Symptom AEs and clinical characteristics are summarized in Table 1.
Frequencies of Symptom Adverse Events, Disease, and Clinical Characteristics
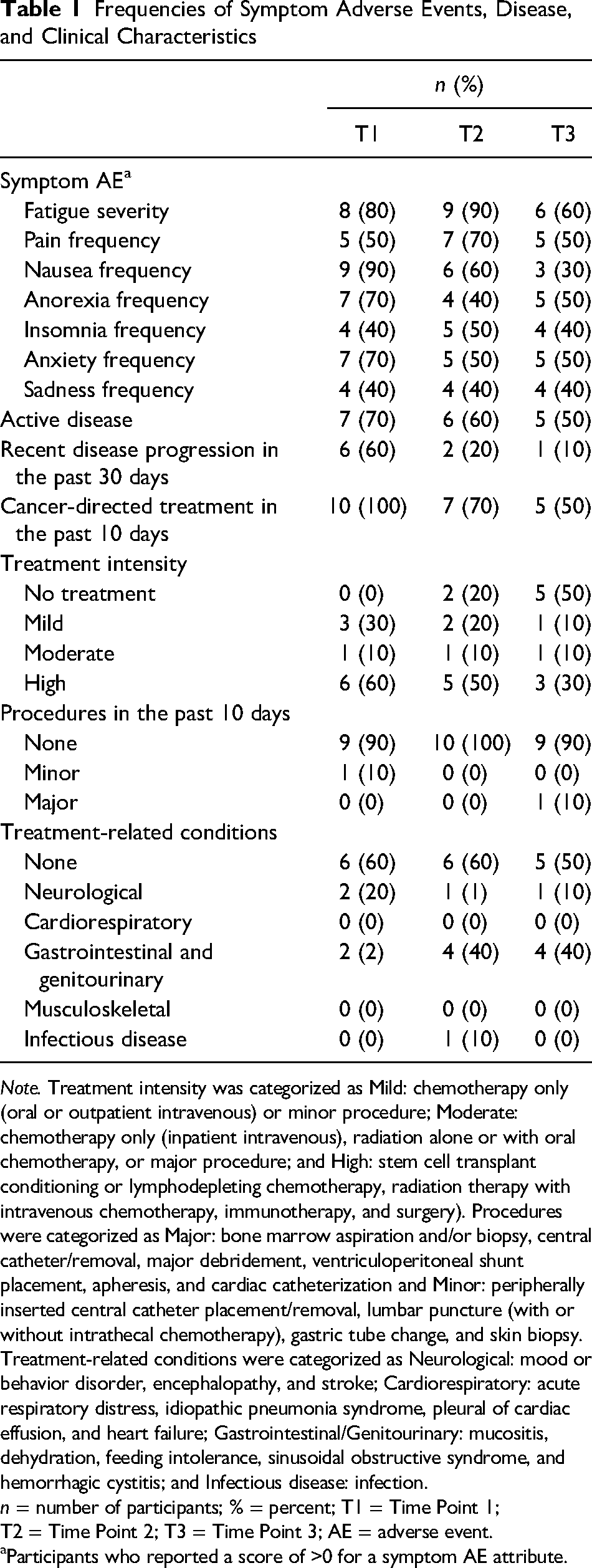
Note. Treatment intensity was categorized as Mild: chemotherapy only (oral or outpatient intravenous) or minor procedure; Moderate: chemotherapy only (inpatient intravenous), radiation alone or with oral chemotherapy, or major procedure; and High: stem cell transplant conditioning or lymphodepleting chemotherapy, radiation therapy with intravenous chemotherapy, immunotherapy, and surgery). Procedures were categorized as Major: bone marrow aspiration and/or biopsy, central catheter/removal, major debridement, ventriculoperitoneal shunt placement, apheresis, and cardiac catheterization and Minor: peripherally inserted central catheter placement/removal, lumbar puncture (with or without intrathecal chemotherapy), gastric tube change, and skin biopsy. Treatment-related conditions were categorized as Neurological: mood or behavior disorder, encephalopathy, and stroke; Cardiorespiratory: acute respiratory distress, idiopathic pneumonia syndrome, pleural of cardiac effusion, and heart failure; Gastrointestinal/Genitourinary: mucositis, dehydration, feeding intolerance, sinusoidal obstructive syndrome, and hemorrhagic cystitis; and Infectious disease: infection. n = number of participants; % = percent; T1 = Time Point 1; T2 = Time Point 2; T3 = Time Point 3; AE = adverse event.
Participants who reported a score of >0 for a symptom AE attribute.
Twenty-nine (97%) blood samples and 199 (83%) saliva samples were collected across all participants and time points. One blood sample was missed because the participant did not have a clinical encounter with the pediatric oncology team during the data collection window. The 29 blood samples were sufficient and included in the analyses. Reasons for missed saliva samples included nausea, forgetting to collect, parent worry about burden, and deteriorating clinical status. Forgetting to collect was responsible for sporadic missing samples across participants, while parent worry and clinical status were responsible for missing time points for specific participants. Of the 199 saliva samples, 43 specimens for salivary cortisol and 70 for sAA were unanalyzable due to insufficient quantity of saliva. Twenty-two of the unanalyzable samples for salivary cortisol (51%) and sAA (31%) were attributed to one participant who reported persistent xerostomia. The final number of saliva samples included in the analysis was 156 (salivary cortisol) and 129 (sAA) from nine participants. Participants completed 84% (n = 52) of the saliva surveys. Missing surveys (n = 8) corresponded with days on which no saliva samples were intentionally collected.
Most participants (80%) completed the final acceptability survey. All participants reported that the instructions for collecting saliva were somewhat (50%) or very helpful (50%) and reported the saliva kits were clearly labeled and very easy to use (100%). Participants reported feeling they received just the right number of reminders and that reminders were either a little (12.5%), somewhat (12.5%), or very (75%) helpful. Participants preferred text reminders (75%) or having the choice for how to receive reminders (25%). Responses to free-text questions related to collecting saliva were collated and included statements reflecting challenges in remembering to collect a sample, collecting a sample at the right time, and not eating or drinking 1½ h before collection. Overall, participants’ comments indicated little difficulty with the collection process. Caregivers of young child participants stated the child's cooperation was important for successful saliva collection.
Aim 2: Range and Distribution of Biomarkers
Only 6 of the 11 inflammatory markers were detectable in the participants’ plasma samples across time points. Pro-inflammatory cytokines IL-8 (Mdn = 46.2 pg/mL), IL-6 (Mdn = 5.6 pg/mL), IFN-γ (Mdn = 48.8 pg/mL), TNF-α (Mdn = 5.3 pg/mL), CRP (Mdn = 3,356 ng/mL]), and anti-inflammatory cytokine IL-10 (Mdn = 4.9 pg/mL) were the most abundant in the study population. Pro-inflammatory cytokines IL-1β, IL-2, IL-12p70, TNF-α, and anti-inflammatory cytokine IL-13 were the least prevalent, with several values below the detectable range (Figure 2).
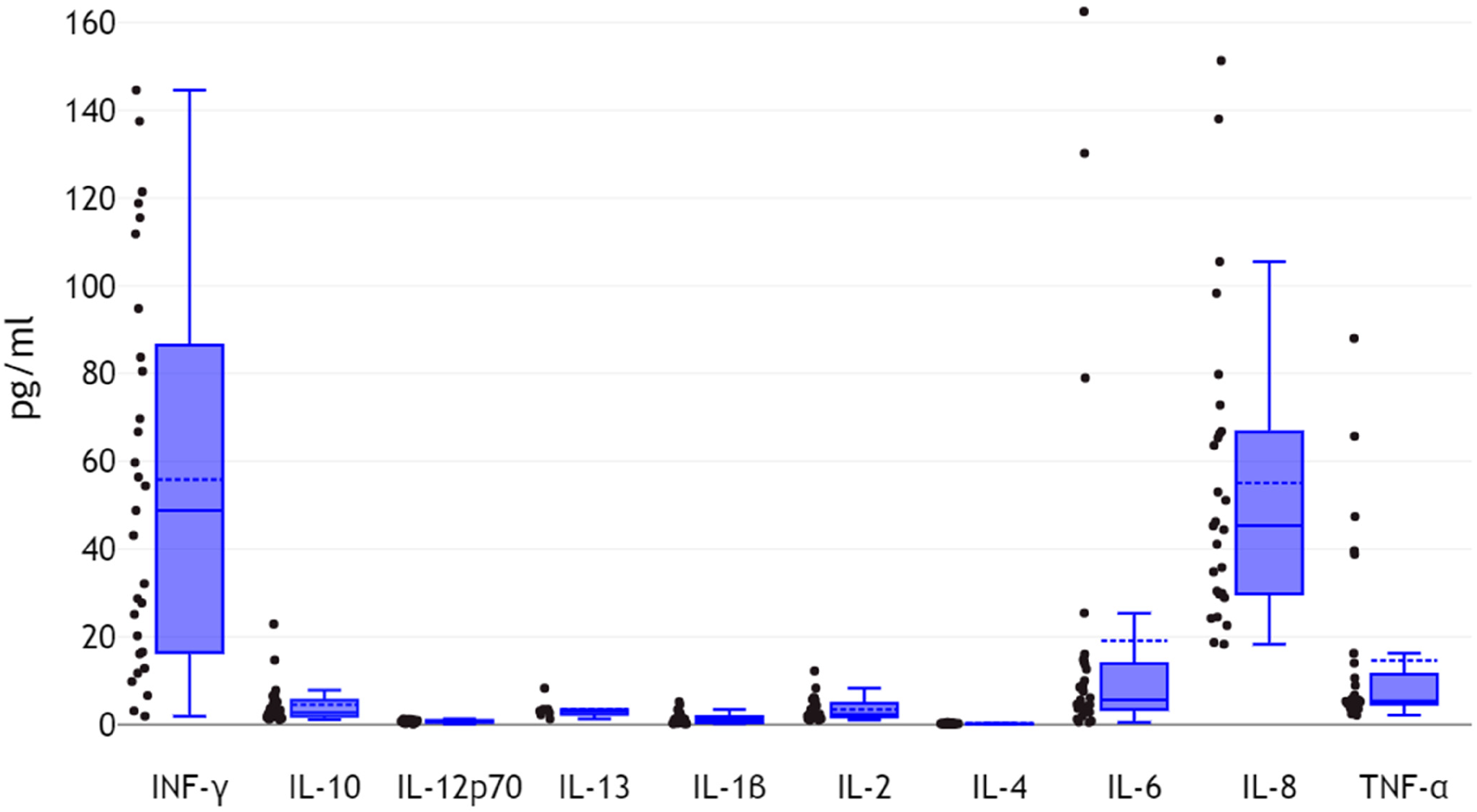
Plasma cytokine values.
Salivary cortisol and sAA values for nine participants with analyzable samples were relatively low and demonstrated mixed patterns across participants and time (Figure 3). Mean cortisol values were highest upon waking (M = 0.54 nmol/L, SD = 0.42) and steadily decreased at 30 min post waking (M = 0.32 nmol/L, SD = 0.15) and before lunch (M = 0.18 nmol/L, SD = 0.15), before rising before bedtime (M = 0.38 nmol/L, SD = 0.70). The average CAR value was 0.24 nmol/L (SD = 0.59). The average linear cortisol diurnal slope value was slightly negative −0.06, 95% CI [−0.18, 0.07] and was characterized as relatively flat (Figure 4). Mean sAA values were highest upon awakening (M = 66.8 U/L, SD = 116.7) and decreased 30 min post waking (M = 38.6 U/L, SD = 24.4). sAA values increased again before lunch (M = 63.0 U/L, SD = 52.9) and decreased before bedtime (M = 54.4 U/L, SD = 37.7). In the context of low salivary cortisol values, a mixed effects multilevel regression model was used to explore for variability in salivary cortisol values across and within participants. The greatest variability in salivary cortisol values was observed between time points (T1, T2, and T3), as opposed to within participants, across day of collection, or across sample collection times. However, this result was not statistically significant.
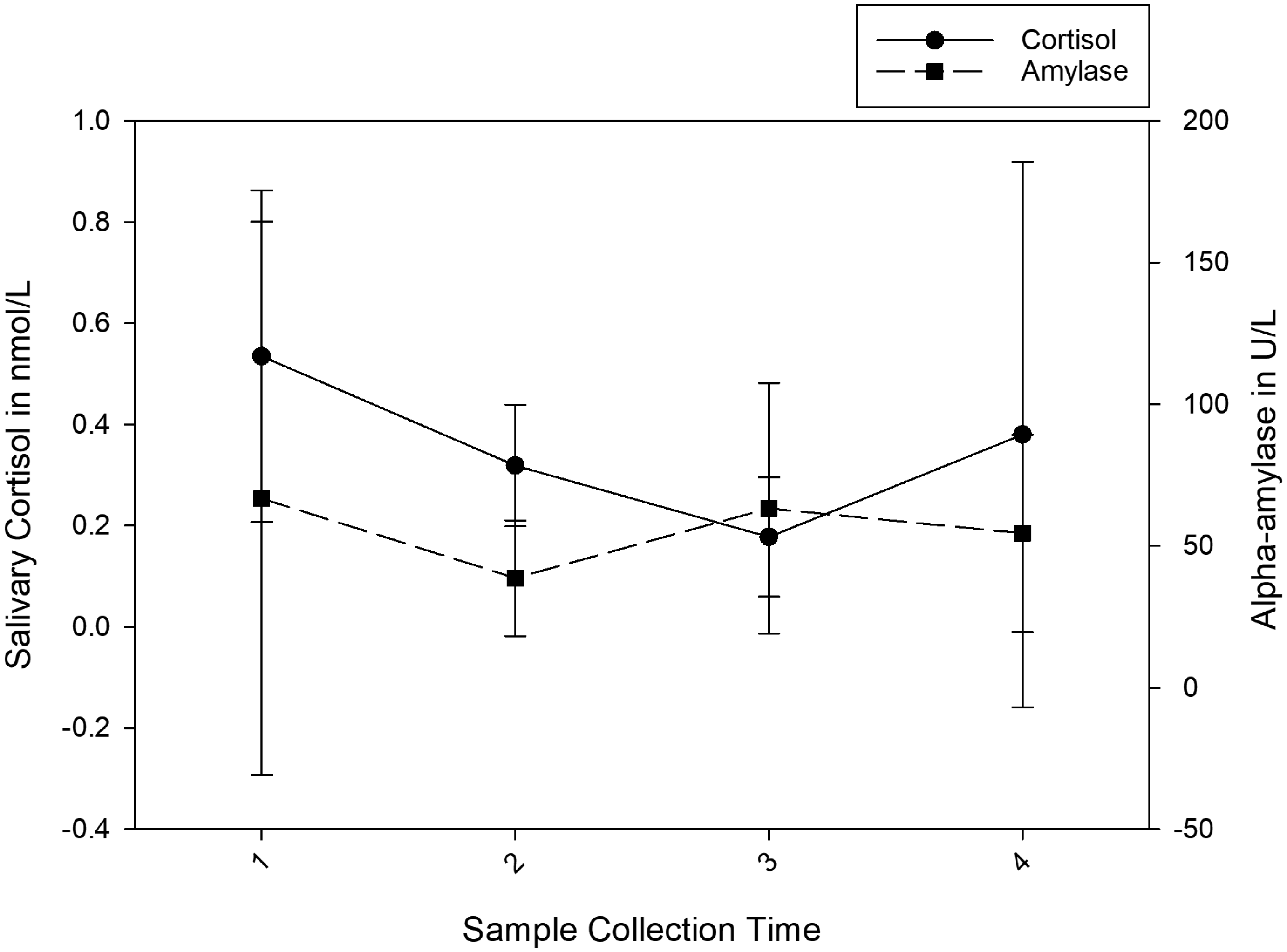
Salivary cortisol and alpha-amylase values.
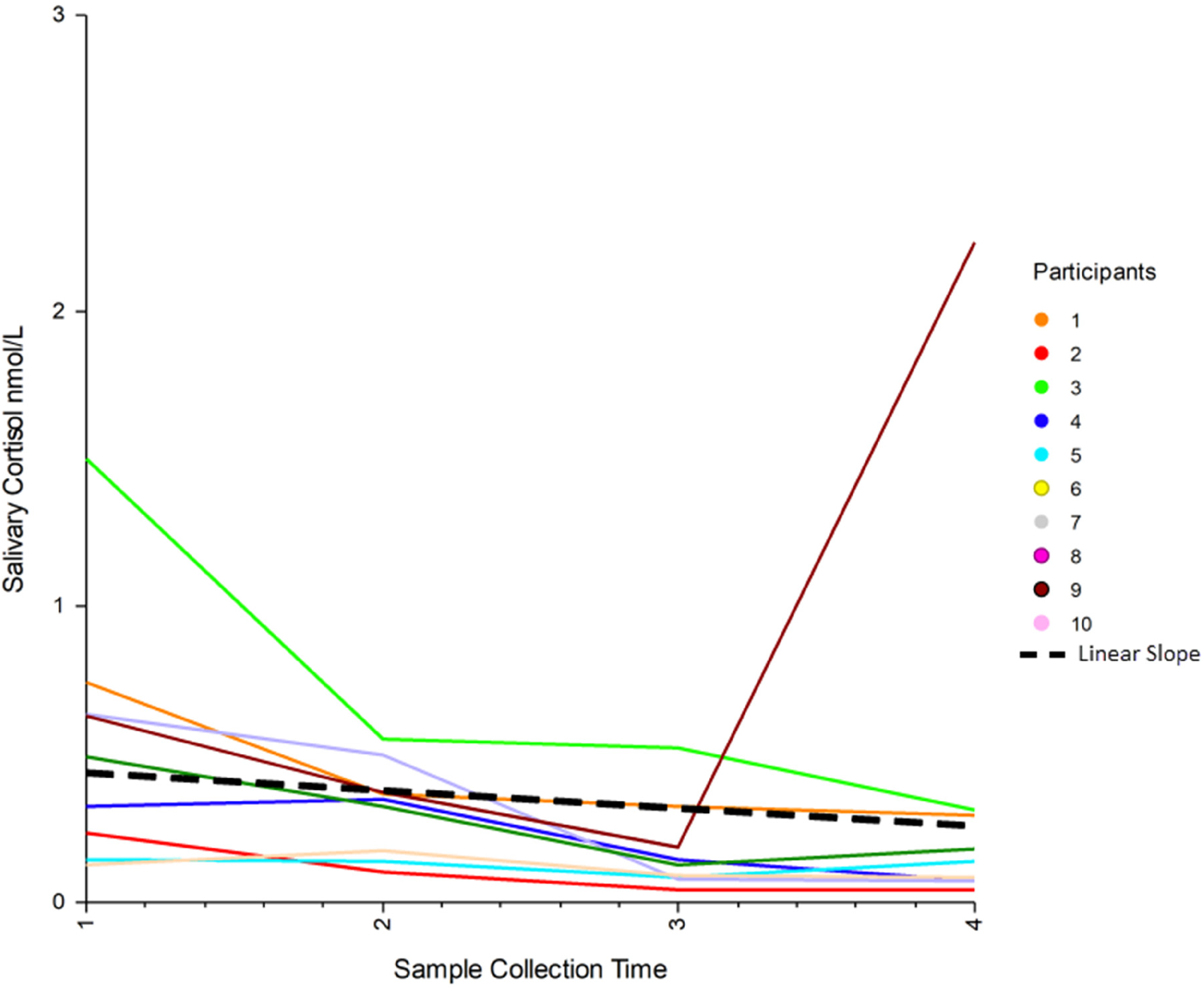
Diurnal cortisol slopes.
Aim 3: Relationship Between Symptom AEs and Biomarkers
The magnitude of difference between the standardized mean inflammatory biomarker values and the symptom AE group yielded several medium or large negative effects (Table 2). Insomnia (n = 9) and pain (n = 8) had the greatest number of medium or large effects with inflammatory biomarkers, followed by fatigue (n = 7), anxiety (n = 7), sadness (n = 6), anorexia (n = 5), and nausea (n = 4). Biomarkers IL-8 (n = 12), TNF-α (n = 12), IL-6 (n = 10), IL-10 (n = 7), and CRP (n = 3) demonstrated medium or large negative effects with several symptom AEs. Group comparisons were not reported for nausea in Time Point 1 and fatigue in Time Point 2, due to 90% of participants endorsing the symptom AE. These results influence the counts of medium or large effects for those symptom AEs and all biomarkers. In response to limited variability in salivary cortisol values and diurnal cortisol slopes, it was not possible to quantify the relationship between the stress biomarkers and symptom AEs in this study.
Standardized Mean Difference Effect Sizes for Inflammatory Biomarker and Symptom AE Data
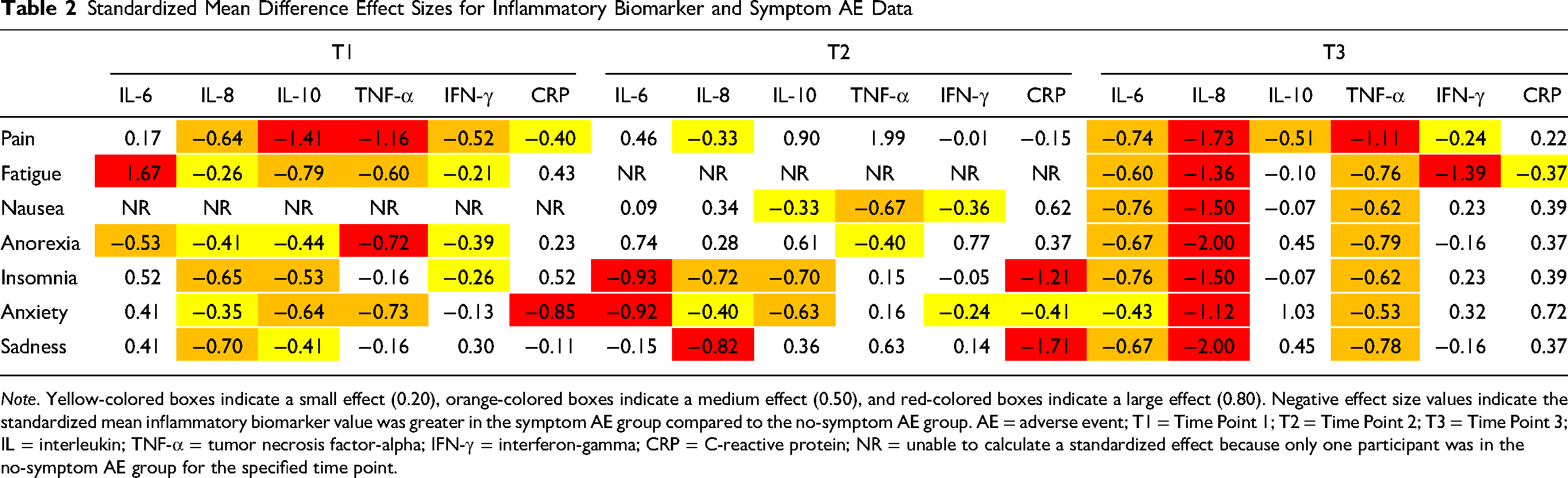
Note. Yellow-colored boxes indicate a small effect (0.20), orange-colored boxes indicate a medium effect (0.50), and red-colored boxes indicate a large effect (0.80). Negative effect size values indicate the standardized mean inflammatory biomarker value was greater in the symptom AE group compared to the no-symptom AE group. AE = adverse event; T1 = Time Point 1; T2 = Time Point 2; T3 = Time Point 3; IL = interleukin; TNF-α = tumor necrosis factor-alpha; IFN-γ = interferon-gamma; CRP = C-reactive protein; NR = unable to calculate a standardized effect because only one participant was in the no-symptom AE group for the specified time point.
Discussion
The results of this study indicate that collection of blood and saliva was feasible and acceptable to study participants and researchers. Coordinating blood sample collection with nurses during previously scheduled patient encounters resulted in high specimen collection rates. A similar approach to collection of blood samples by nurses or phlebotomists during patient encounters has been proposed in a study protocol designed to examine the relationship between inflammation and mucositis in adolescents and young adults with cancer (Thornton et al., 2022). In this study, allowing participants to collect saliva in the hospital, infusion center, and/or at home led to high collection rates for saliva specimens. Similar results were seen in a study of seriously ill adults who were asked to collect saliva using salivettes for two consecutive days (Warth et al., 2022).
Field notes suggested nurses were active partners in supporting the collection of samples for biomarker measurement, both directly, by collecting blood samples, and indirectly, by encouraging collection of saliva samples. In several instances, nurses communicated with the study team when encounters were rescheduled and/or when participants had questions about saliva collection. Additionally, field notes indicated nurses often asked the study team how they could help support data collection when patients were hospitalized. Nurses expressed a commitment to help support caregivers and participants to monitor and replace ice packs for study-provided insulated coolers to keep samples cool. This suggests that nurses should be considered an integral part of the team responsible for study design and procedures when collecting biospecimens.
The quality of the blood specimens was high, with all samples included in the analysis. Procedures employed to maintain specimen integrity and quality included (a) timely sample pick-up post-collection to reduce risk of clotting, (b) timely specimen processing and plasma extraction, (c) storage of plasma samples in deep freezers with quality control monitoring (e.g., freezer alarms), and (d) analysis of plasma samples within a National Cancer Institute-designated comprehensive cancer center laboratory. A critical aspect of the study was establishing clear expectations for communication about specimen collection, pick-up, and processing. For this study, a study-specific university email account was used to communicate to the laboratory staff the anticipated date, time, and location for specimen pick-up, including detailed directions to promote wayfinding. In return, laboratory staff sent an email confirmation once the sample was received, processed, and stored. The closed-loop communication process built trust for specimen collection and created opportunities to identify problems and, if needed, modify to procedures.
The quality of saliva samples was lower than the researchers had expected given the high rate of saliva sample collection completion. Because of this study's unique design, which allowed participants to collect saliva across clinical and home settings, it is difficult to compare the completion rate to other research. In a large study of children aged 8–13, Kuhlman et al. (2019) reported 87.2% (n = 2,204) of saliva samples being returned after being collected at home. Explanations for insufficient quantity of saliva include (a) the participant not placing the salivette in the mouth for the recommended time, (b) a mismatch between the recommended time for the salivette to be placed in the mouth and ability to saturate the salivette, and (c) inability to confirm quality of saturation during participant education and practice sessions. In this study, field notes indicated that one participant, whose samples were all categorized as unanalyzable, stated he had xerostomia. Study procedures required the participant to saturate the salivette by placing it in the mouth for 1–2 min. Xerostomia was also documented as a barrier for saliva collection in a study of seriously ill adult patients receiving palliative care (Warth et al., 2022).
Saliva samples can be collected through a variety of methods (Mandrell & Withycombe, 2019), including use of salivettes, filtered paper, and passive drool. Filtered paper was shown to produce inferior results for quantifying sAA compared to passive drool (Ameringer et al., 2012). Collection of passive drool, with cotton swab alternatives, has been shown to be feasible and acceptable in a sample of ethnically diverse school-aged children (Condon et al., 2020), while pre-school children did not endorse a preference for collecting saliva via passive drool, cotton swab, or hydrocellulose microsponges (O’Farrelly & Hennessy, 2013). Cortisol can also be measured using other body tissues, including hair and nails (Mandrell & Withycombe, 2019). Because the target population in this study was children with advanced cancer, many participants were experiencing alopecia as a side effect of cancer-directed treatment. However, nail samples may be considered for future study designs to reduce data missingness.
Although the study assessed 11 biomarkers of inflammation, only 6 were detected in subjects’ samples. Measurable elevated values were obtained for four pro-inflammatory cytokines (IL-8, IL-6, IFN-γ, TNF-α), one anti-inflammatory cytokine (IL-10), and CRP. Other biomarkers of inflammation were at levels too low for detection. These results partially support previous findings of elevated baseline inflammatory markers (IL-2, IL-4, IL-6, IL-8, IL-10, and IFN-γ) among adolescents and young adults with cancer compared to healthy peers (Chan et al., 2023).
Wide variability was also evident in neuroendocrine biomarkers measured in saliva samples. In this study, the mean salivary cortisol and sAA values were lower than values reported among critically ill children (Tzira et al., 2018) and healthy children (Kuhlman et al., 2019). Explanations for the variability in values could include potential mismatch in the participant-reported collection time and actual collection time or lack of adherence to instructions (e.g., sample collected outside designated time). Another possible reason for the relatively low cortisol values may be adrenal insufficiency, which has been described in children diagnosed with acute lymphoblastic leukemia following treatment with corticosteroids (Einaudi et al., 2008) and in some pediatric cancer survivors receiving various treatment modalities (Patterson et al., 2009). Because this study included children with advanced cancer, treatment history, in addition to current treatment, may be important, as it could indicate participants’ risk for adrenal insufficiency.
Indices of HPA axis regulation, including salivary cortisol and sAA, have been shown to be highly variable within individuals over time (Kuhlman et al., 2019). The stability of these measures, including waking cortisol levels and measures of the CAR, are impacted by important biological variables, including age, sex, and pubertal development. In a longitudinal study of healthy children in middle childhood and early adolescence, Kuhlman et al. (2019) found indices of HPA regulation were more stable in children who were younger, male, and earlier in their pubertal development. Age, sex, and developmental variables should be considered when determining sample sizes of future studies exploring cortisol as a biomarker of stress in large-scale pediatric cancer research.
This study found blunted CAR and flattened diurnal cortisol slopes among a small sample of children with advanced cancer. Blunted CAR and cortisol reactivity has been shown in children and adolescents with functional neurological disorders, compared to healthy controls (Chung et al., 2023), and in adults who report high levels of chronic stress and have poorer health outcomes (O’Connor et al., 2021). Flattened diurnal cortisol slopes have been reported in adult with breast cancer (Schmidt et al., 2016) and are associated with diminished emotional and physical health outcomes among adults (Adam et al., 2017). However, there may also be methodological explanations for the study's findings. Jones et al. (2020) emphasized that mistimed saliva samples may underestimate peaks in cortisol and sAA reactivity.
Select inflammatory markers demonstrated moderate or large negative effects with priority symptom AEs, consistent with reports from studies of adults with cancer. However, in this small sample, the effect sizes were variable across all time points. Results of foundational studies examining the associations between cancer symptoms and pro- and anti-inflammatory markers and CRP suggest positive relationships between IL-1β, IL-2, IL-4, IL-6, IL-8, TNF-α, and CRP and pain, fatigue, and sleep disturbance (Miaskowski & Aouizerat, 2012). The effects between inflammatory marker values and the presence of select symptom AEs may provide preliminary evidence to support the theorized sickness behavior response in response to cancer and treatment. Overall, the results of this study should be interpreted with caution should be interpreted with caution given the small sample size. However, moderate and large effect sizes for biomarkers IL-6, IL-8, IL-10, TNF-α, and CRP merit further investigation in a larger population of children with advanced cancer.
Limitations
This study has several notable limitations related to its exploratory nature. First, the sample size was insufficient to provide confirmatory evidence of biomarkers for fatigue, anxiety, pain, nausea, anorexia, sadness, and insomnia symptom AEs. Second, the ability to account for important covariates, like race, ethnicity, disease and treatment variables, and participant medications, was hindered by small sample size, over-representation of White non-Hispanic participants, and heterogeneity of diagnoses and treatment plans. Third, the procedures used to collect blood samples did not include a process for home health collection. Fourth, caution should be used when interpreting salivary cortisol and sAA results because of the low number of analyzable salivary samples. Finally, the study did not evaluate biomarker collection procedures in participants who are not English literate. These limitations warrant consideration in future research.
Implications for Future Research
Research identifying mechanisms underlying pediatric cancer symptoms is in an early stage. A stepwise approach is required to identify biological mechanisms within a broader biopsychosocial context. First, reliable procedures that are informed by nurses and can be applied across institutions and clinical settings to maximize biospecimen collection in large-scale multisite research must be established. Second, research examining the relationships between biomarkers and symptoms, while accounting for important biological and clinical covariates, is needed to generate preliminary evidence of biological correlates of cancer symptoms. Together, tested procedures and evidence indicating a relationship between biomarkers and symptoms can inform large-scale multisite research. Third, multisite collaborations that facilitate large-scale studies are necessary to confirm biomarkers of pediatric cancer symptoms. Once confirmed, biomarkers may serve as clinically meaningful indicators for risk-stratified approaches to symptom assessment and management. Finally, there are opportunities to synthesize existing literature on the relationships between biomarkers and symptoms through a scoping review or meta-analysis. In summary, to develop the next generation of novel symptom management strategies in pediatric oncology, research exploring upstream factors, including biological mechanisms, is required. Without knowledge of variables and relationships that help explain why two children with the same disease and treatment experience drastically different symptoms, advancements in symptom interventions may stagnate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Authors disclose the following financial support: School of Nursing at the University of Wisconsin-Madison (2019-20 Research & Scholarship Committee Award), Office of The Director, National Institutes of Health (Award P51OD011106 to the Wisconsin National Primate Research Center, University of Wisconsin-Madison), UW Institute for Clinical and Translational Research and the Clinical and Translational Science Award (CTSA) Program (for the REDCap database), through the NIH National Center for Advancing Translational Sciences (NCATS; grant UL1TR002373), and University of Wisconsin Carbone Cancer Center Cancer Pharmacology Lab (CPL; P30 CA014520).