
Abstract
Background
Anxiety is highly prevalent among pediatric oncology patients. Weighted blankets are a potential intervention to address anxiety for pediatric oncology patients. The goal of this work is to assess the effectiveness of weighted blankets in reducing anxiety for pediatric oncology patients.
Method
A randomized 2 × 2 cross-over design was utilized. Newly diagnosed pediatric oncology patients between the age of 4 and 17 were included. All participants also needed to pass seriation screening to be able to eligible for the study. Participants were randomized to one of two arms: weighted blanket on first infusion visit after enrollment then usual care on second visit (WB:UC) or usual care on first infusion visit after enrollment then weighted blanket (UC:WB) on second visit. Anxiety via Children's Anxiety Meter–State (CAM-S) was collected pre- and postinfusion visit. Descriptive statistics were conducted to describe the data. A linear mixed model with interaction effects was conducted to assess the treatment effect of the weighted blanket.
Results
There were 26 participants who were enrolled in the study. Twenty-four with complete information were included in the analysis. Regression models revealed that CAM-S measure reduced by −0.71 (95% CI: [−1.25 to −0.19], p = .02). WB had more impact on the second visit (
Discussion
There was significant reduction in anxiety postinfusion. While further research is needed, this study highlights not only the impact of weighted blankets, but of nursing care on anxiety for pediatric oncology patients.
Background
Every year, tens of thousands of children are diagnosed with cancer (National Cancer Institute, 2017). As cure rates increase, it is critical to also focus on the psychosocial outcomes. Cancer diagnosis and treatment may have a negative psychosocial impact, including anxiety in pediatric oncology patients (Lazor et al., 2017). This also has the potential to negatively impact their overall quality of life, particularly in the immediate postdiagnosis stage when anxiety is high (McCullough et al., 2018). Nazari et al. (2017) showed that pediatric oncology patients have significantly higher levels of anxiety compared to their healthy counterparts. However, little is known about the trajectory of anxiety for the pediatric population across chemotherapy infusions. Addressing anxiety in this population is essential in providing a well-rounded, holistic approach to care. Phongnopakoon et al. (2018) showed that the creation and implementation of interventions designed to meet the complex needs of cancer patients may prevent late referrals to psychological services. Different modalities such as various forms of therapy and pharmacological interventions exist that help to reduce anxiety in pediatric oncology patients. Oncology nurses may have a role in offering a complementary intervention for anxiety, such as weighted blankets.
Weighted blankets provide deep pressure stimulation (DPS) or deep touch pressure (DTP) which has advantages in both physical and psychological domains. This modality shows increasing parasympathetic arousal and concurrent reduction in sympathetic arousal (Eron et al., 2020). DPS can lead to a decrease in cortisol and increase serotonin and melatonin concentrations thus creating a calming effect (Becklund et al., 2020). Parasympathetic nervous system activation is inhibitory to stress and anxiety and slows breathing and heart rate. The touch sensation mimics the feeling of a tight hug, swaddling, holding, or massage.
There is a lack of research specific to weighted blanket use in the pediatric oncology population. There was a previous adult study completed that did show a reduction in anxiety for adult oncology patients during outpatient chemotherapy infusions (Vinson et al., 2020). Weighted blanket use has been studied for adult patients in multiple settings including mental health settings, dental settings, posttraumatic events, and for those with sleep disturbances. Additionally, weighted blanket use has been documented by Occupational Therapists for children with autism-spectrum disorders (Eron et al., 2020). Most of these studies have shown significant benefit for weighted blanket use.
Pediatric oncology nurses are integral in advocating and implementing integrative therapies for patients (Raybin et al., 2020). Other therapies such as animal-assisted, music, and creative art therapy have also shown effectiveness in reducing anxiety and distress for pediatric patients. The access to a weighted blanket adds to the variety of nonpharmacologic modalities nurses could offer to patients to improve their overall experience. Patients and parents often perceive limited decision making capability because much of their care is based on established protocols (Ruhe et al., 2016). By allowing patients control over the application and removal of the weighted blanket, this modality provides patients and families autonomy, while also empowering them to make decisions that may improve their infusion experience. This may provide nurses, patients, and families a unique opportunity to improve patient care outcomes related to anxiety. One disadvantage could be potential problems with access to a weighted blanket. They can be costly and have fewer options for patients requiring lighter options. Weighted blankets could be an adjunct to current standard of care that may include nursing assessment and existing support activities for anxiety such as art, movies, and/or a child life specialist.
While the majority of evidence regarding weighted blanket use for anxiety reduction is in the adult population, the goal of this study is to determine if the use of a weighted blanket in the pediatric oncology population receiving chemotherapy infusions had an impact on anxiety reduction. This goal is in line with the hypothesis (Aim 1) that the use of the weighted blanket in this population will reduce anxiety. Additionally, assessment of quality of life (Aim 2) with comparison between visits and between groups in this population is a focus of this work to discern whether quality of life will increase between visits and also be at an increased level for participants starting with the weighted blanket intervention at first infusion.
Method
Trial Design
This work utilized a 2 × 2 crossover randomized control trial. Participants were randomized to one of two sequences: (a) weighted blanket first then usual care (WB:UC) or (b) usual care first then weighted blanket (UC:WB). The advantages of the cross-over design decrease the potential confounding bias as participants serve as their own controls. The period in between patient treatments will be considered the washout period. This period can go up to 60 days. One major change to the protocol included changing the inclusion criteria of time between appointments from 30 to 60 days. This change expanded the eligible participants.
Participants
The study had the following inclusion criteria: (a) newly diagnosed pediatric oncology patients between the ages of 4 and 17, (b) received outpatient chemotherapy infusions in one of the two designated outpatient locations, (c) have a “liquid tumor” (leukemia or lymphoma), “solid tumor,” or a neuro-oncologic diagnosis, (d) completed a seriation screening, (e) greater than 13.5 kg in weight, (f) whose second and third outpatient chemotherapy occur within 60 days of each other, and (g) English and/or Spanish speaking. The seriation screen determines if the child's ability to rank order by size. They were asked to count to 10, and then answer, “Which is bigger, 7 or 4?” Children were asked to identify the smallest of a series of four stacking cups. Children unable to complete these tasks successfully or cannot understand the instructions will be excluded as this level of understanding is required to accurately and appropriately complete anxiety scales (Ersig et al., 2013). Those who are relapsed, who are undergoing bone marrow transplant or had a previous bone marrow transplant, and who are currently using a weighted blanket at home were excluded. The setting for this research occurred within two outpatient units of a cancer department within a pediatric hospital system in the western United States.
Interventions
The intervention for each group was the use of a weighted blanket. Participants were provided their own weighted blanket that is weighted 10% of their weight as recommended by various studies (Eron et al., 2020). The blankets come in sizes of 3, 5, 7, 10, 12, and 15 pounds. If a participant's weight falls in between, they were rounded up or down to the closest appropriate weight.
Procedures
For the WB:UC group, a member from the weighted blanket research team or a trained infusion nurse administered anxiety, quality of life, and parent perception surveys to the patient and the parent/guardian prior to start of infusion or placement of the weighted blanket. The surveys were administered after Mediport access or other potential anxiety producing procedures (i.e., nasal swab, injection, etc.) because those could directly impact the results of assessing anxiety during chemotherapy infusion. During this weighted blanket intervention visit, the infusion RN or the patient will place the blanket on the patient's body at the infusion start time. The infusion RN also instructed the patient to leave the weighted blanket on for at least 15 min. At completion of infusion, the anxiety surveys were re-administered by the infusion RN, and the weighted blanket collected and stored in the designated patient-specific labeled bag. During their next chemotherapy infusion appointment, study participants received the usual standard of care for the visit. In this visit, collection of anxiety, quality of life, and parent perception surveys remained the same as the weighted blanket visit. Usual care consists of timely monitoring by an infusion nurse, vital signs and assessments as indicated, access to movies, games, activities, and/or a child life specialist. Patients could either be roomed in an infusion room with a bed or in a bay with an infusion chair. For the UC:WB group, the two visit types were reversed and followed the same procedures for each visit.
Outcomes
For Aim 1, the primary outcome measure for anxiety is the Children's Anxiety Meter–State (CAM-S) assessment, which measures anxiety in the moment. The CAM-S is a validated survey and showed significant positive correlation to parent observations and observed behaviors of anxiety (.15 to .26, p < .05) (Ersig et al., 2013). The CAM-S is completed by showing the child a picture of a mercury thermometer and asking the child to Pretend that all of your worried or nervous feelings are in the very bottom down here (point to scale). If you are a little bit worried or nervous, the feelings might come up just a little bit (move finger up). If you are very, very worried, or nervous, the feelings might come up just a little bit (move finger up to the top). Put a line showing how much worry or nervousness you feel right now.
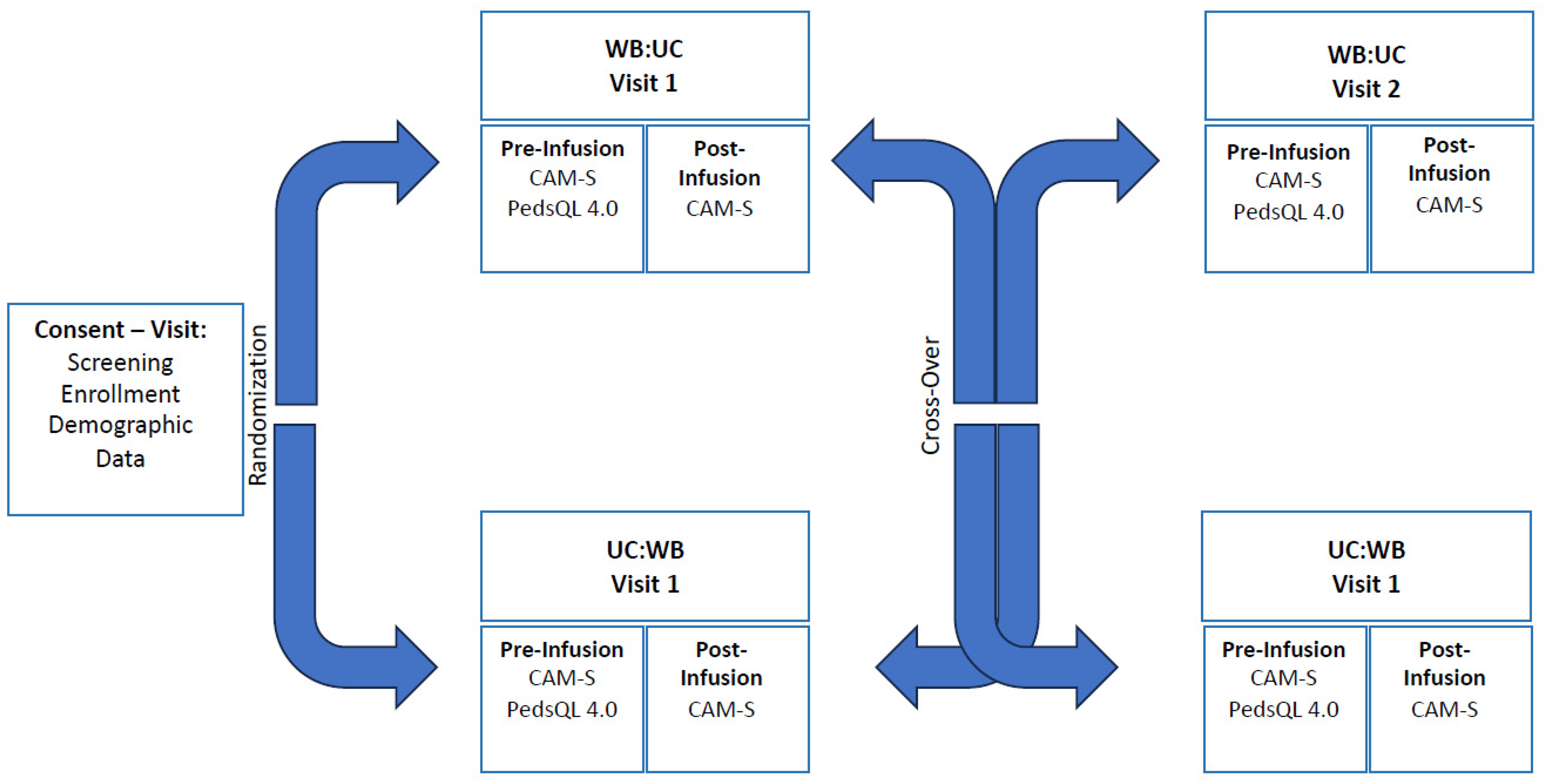
Cross-Over Design and Data Collection Schedule.
For Aim 2, the quality of life of participants was assessed using the Pediatric Quality of Life Inventory Generic Core Scales (Peds QL 4.0). The Peds QL 4.0 is a 23-item questionnaire and is broken up into four sections: physical functioning (eight items), emotional functioning (five items), social functioning (five items), and school functioning (five items). These questions are aimed to measure health-related quality of life in children and adolescents who are healthy and those with acute or chronic health conditions (Varni et al., 2003). The parent-proxy questionnaires were used for all ages with responses measured on a 5-point response scale: 0 = never a problem; 1 = almost never a problem; 2 = sometimes a problem; 3 = often a problem; and 4 = almost always a problem. The scale is recoded and summarized to have a score ranging from 0 to 100 where higher values indicate higher quality of life. Cronbach's alpha was utilized to determine internal consistency. The Cronbach alpha for total scale measure was .89–.92. The scale was validated using known-groups method. Groups are divided up by age which include a questionnaire for Toddlers (ages 2–4 years), Young Children (ages 5–7 years), Children (ages 8–12 years), and Teens (ages 13–18 years). Results from the known-groups methods suggest construct validity of the PedsQL 4.0 as evidenced by appropriate comparisons between groups on metrics such as indicators for health care access, days missed from school, days sick in bed or too ill to play, and days needing care (Varni et al., 2003). Unlike the CAM-S, this data was only collected before each infusion as it was not anticipated that the use of the weighted blanket to have an immediate impact on quality of life, but a recent baseline prior to the start of each infusion was desired. Additionally, in this patient population quality of life can be impacted by a variety of factors. To reduce potential variability in the data, it was best to utilize this tool to help clarify end results. For example, a patient who did not have as big of a change in their anxiety (CAM-S) with the weighted blanket but had a lower QOL than an average participant could help clarify why an impact may have not been seen. Aside from the collection schedule, data will similarly be collected and stored to Aim 1.
Sample Size
For the power analysis, a sample size of 26 was calculated for power as 26 was the goal for participant enrollment. In a typical power analysis, the goal is to determine the appropriate power with alpha at .05 and power at .80. Power analysis reveals that a sample size of 26 achieves power for a number of circumstances. Any effect size that is moderate and above (1.3 mean difference) will lead to power. For small mean difference (0.78), power is attained high correlation between CAM-S measurements and low dropout. These assumptions can be reasonably met as there is no expectation that CAM-S will vary widely in-between visits. Further, the second instance of data collection is tied to the participant's second chemotherapy; hence, the likelihood of dropping out in the second instance of data collection is minimized.
Randomization
To provide balance between treatment groups as it relates to baseline variables and unmeasured confounders, a stratified randomization block sequence was developed by the research statistician. Stratification occurred at the location level with 22 at the larger location and 4 at the smaller location. Within the stratum, a block schedule was created to provide adequate equality within randomized assignments. The block size will not be revealed to investigators and will be selected from a small number of choices to prevent prediction of assignments by the investigators. Randomization sequence was conducted using R (R Core Team, 2017). Allocation of random assignment was concealed in a sealed envelope by the research statistician. Randomization occurred during patient enrollment at their first outpatient infusion visit. Study team members, specifically the PI, co-investigators, and study coordinators enrolled participants. Neither participants, care providers, nor statisticians were blinded to study arm following assignment of intervention.
Statistical Method
Descriptive statistics such as means and standard deviations were conducted to summarize the data. Initial bivariate analysis was conducted to assess differences of outcomes between and within groups utilizing appropriate tests. Test included paired t-tests. Because of multiple tests, p-values were adjusted using the Bonferroni correction. The level of significance was chosen to be p < .05. It was expected that there would be differences in CAM-S scores before and after infusions, between WB and UC, and between visits. Further, it was expected that PedsQL 4.0 would have statistically significant differences between visits and in between WB and UC.
For regression analyses, multiple multivariate linear mixed regression models with interaction effects were conducted to assess the impact of weighted blanket for each primary and secondary outcome.
The linear mixed models conducted where CAM-S was the main outcome were interaction models looking to investigate fixed effects within and between groups (WB vs. UC), infusion timing (preinfusion vs. postinfusion), visit (Visit 1 vs. Visit 2), the interaction between groups and infusion timing, and the interaction between groups and visit. Further, we added PedsQL 4.0 as another fixed effect as bivariate analysis conducted showed a statistically significant relationship of PedsQL 4.0 with CAM-S. Another model was conducted where PedsQL 4.0 was the main outcome. A similar multivariate interaction model was created but without the infusion timing variable. Further, residual analysis for each outcome was conducted to remove outliers. Final models created removed some outliers and, in most cases, only one to two observations were removed. Expectations for the CAM-S model included differences that were statistically significant between groups and infusion timing. For the PedsQL 4.0 model, it was expected there would be statistically significant differences between groups and between visits.
Results
Losses and Exclusions
There were 402 potential participants that were screened, 29 were approached, and 26 were consented. Participants were screened but were excluded based upon age, weight, diagnosis, or treatment plan not meeting requirements of the study, for example, all chemotherapy was inpatient, or appointments were too far apart. Of the 26 participants who consented to the study, 14 were randomized to the WB:UC arm (Arm 1) and 12 were randomized to UC:WB (Arm 2). In the first sequence, one participant had missing outcome information due to not receiving surveys; the remaining 13 subjects completed the protocol. In the second sequence, two participants had missing outcome information due to not receiving surveys. Further, two participants were excluded from the second sequence due to missing infusion visits and receiving treatment at another facility. Figure 2 displays the participant flow.
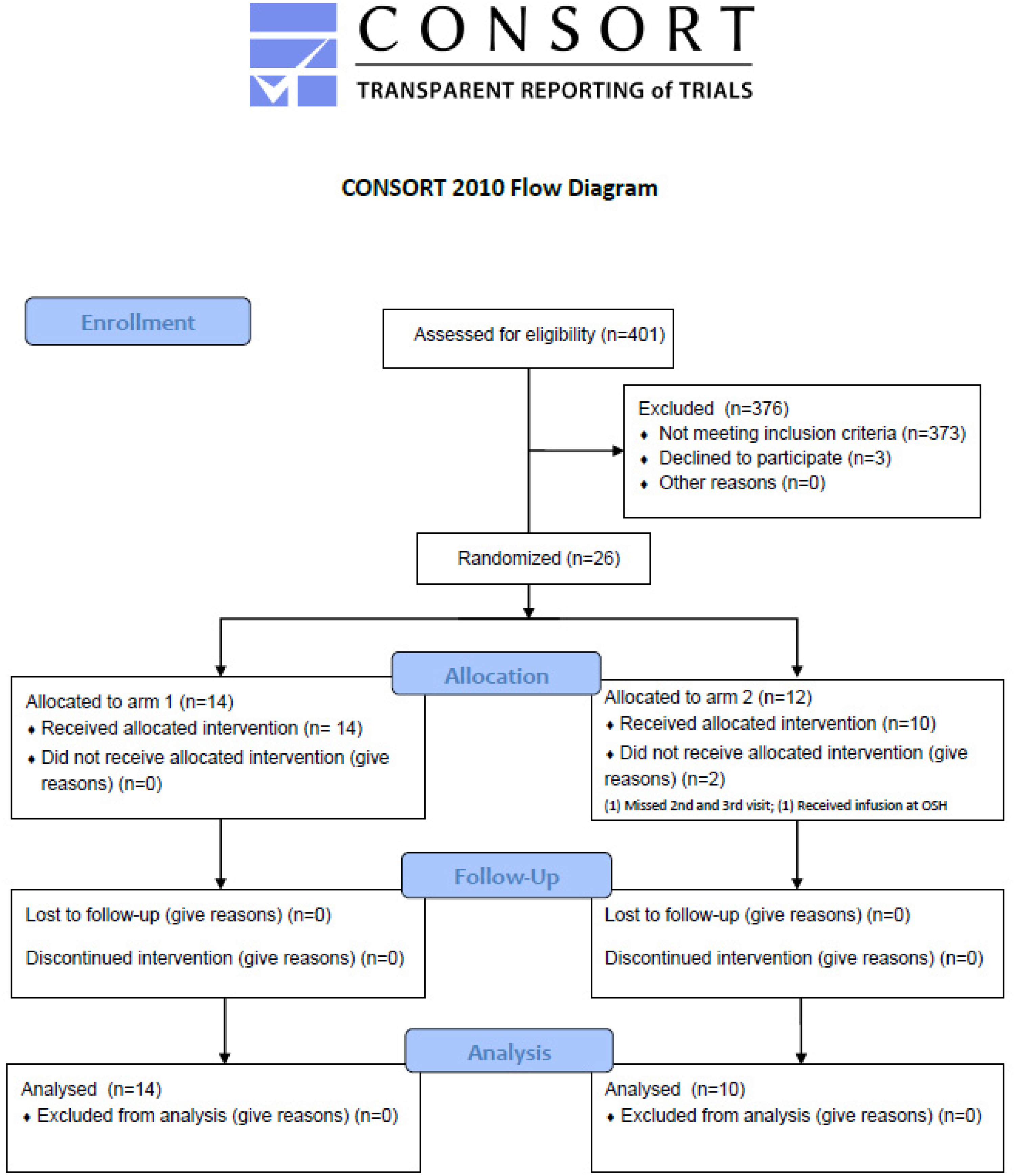
Flow of Participants.
Recruitment
Recruitment began on January 3, 2022, and ended on July 11, 2023. All study procedures and data collection were completed by July 25, 2023. Recruitment ended once the desired enrollment number was reached; the trial ended following all participant study procedures completion.
Baseline Data
There were 26 total participants who were enrolled in the study. On average, participants were 11.9 years old (SD = 3.5), female (n = 14, 54%), non-Hispanic (19, 73%), spoke English (24, 92%), and white (20, 76%). For the CAM-S, there were a total of 92 observations analyzed comprising 88% of the possible observations. There were 48 observations (100%) that were analyzed for the PedsQL 4.0.
Binary Outcomes
Overall mean for CAM-S was 3.4 (SD = 1.3). The overall mean for PedsQL 4.0 was 68.1 (17.0). Table 1 summarizes bivariate results across all outcomes. For the CAM-S, there was a statistically significant difference between pre- and postinfusion for those in the UC at Visit 1 (4.4 [SD = 0.8] vs. 2.8 [SD = 1.5], p = .03). In general, those who received WB had lower preinfusion CAM-S compared to those who received UC (4.0 vs. 4.4, 2.9 vs. 3.5). In the second visit, those who received WB had lower CAM-S scores compared to those who received UC (2.7 [1.7] vs. 3.5 [0.9], p = .07). This was not statistically significant. Figure 3 displays CAM-S scores.
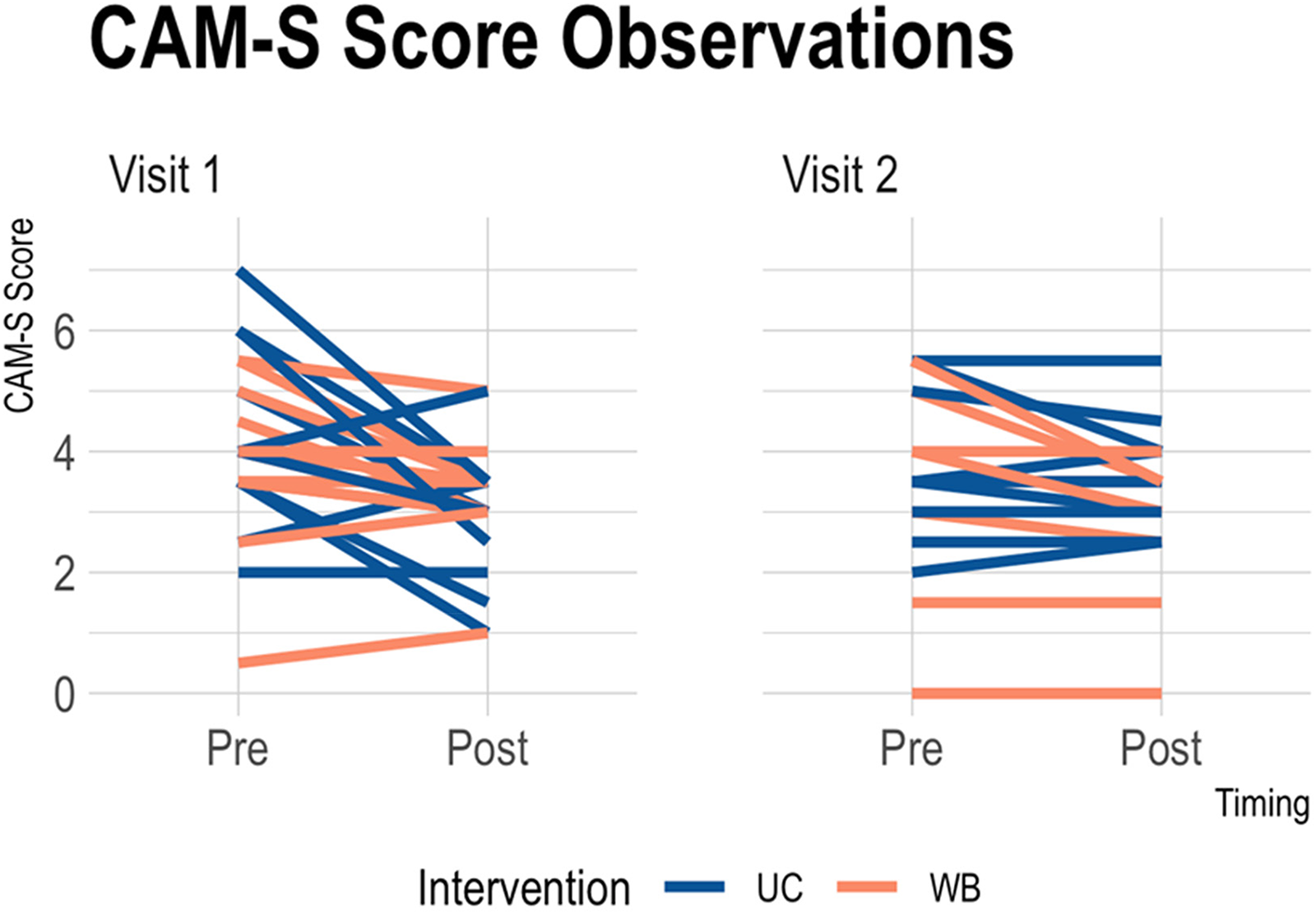
CAM-S Scores by Infusion Period, Visit, and Intervention Group.
Bivariate Results for Outcomes (N = 24)
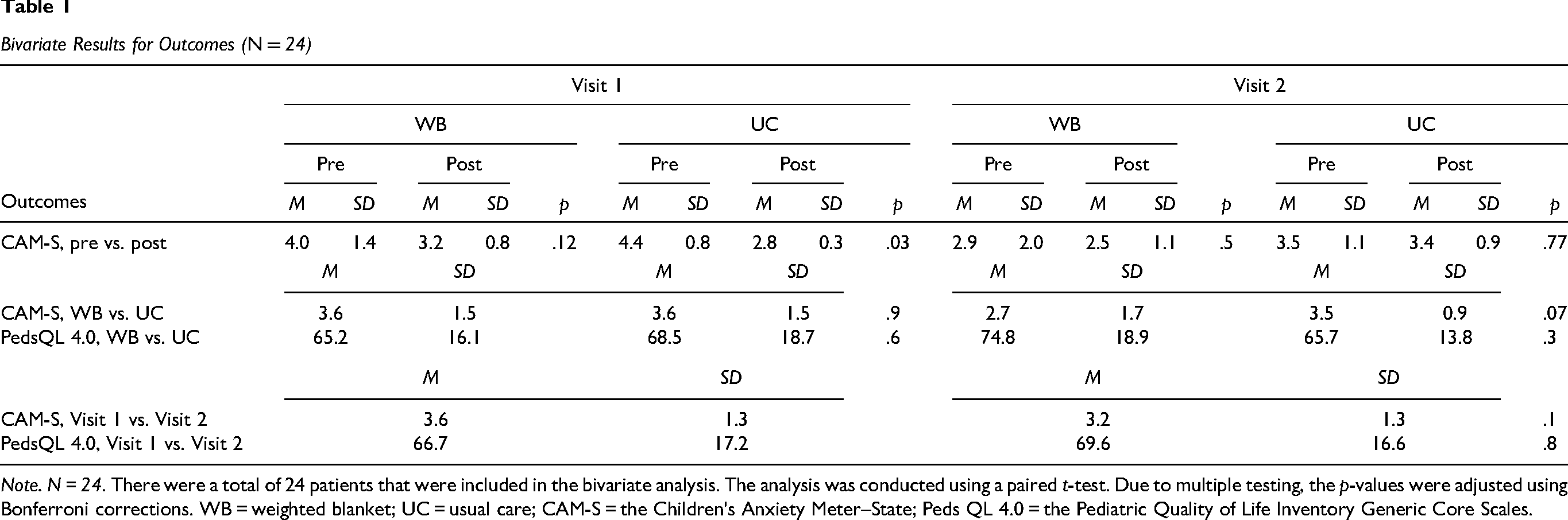
Note. N = 24. There were a total of 24 patients that were included in the bivariate analysis. The analysis was conducted using a paired t-test. Due to multiple testing, the p-values were adjusted using Bonferroni corrections. WB = weighted blanket; UC = usual care; CAM-S = the Children's Anxiety Meter–State; Peds QL 4.0 = the Pediatric Quality of Life Inventory Generic Core Scales.
PedsQL 4.0 increased from 66.68 (SD = 16.1) to 69.57 (16.6) between Visits 1 and 2. This was not statistically significant (p = .8). During the second visit, those that received a WB had a higher PedsQL 4.0 (74.84, 18.9) compared those in the UC visit (65.72, 16.6). This was not statistically significant (p = .8).
Ancillary Analyses
For CAM-S scores, interaction models revealed that postinfusion reduced scores by 0.71 (B = −0.71, 95% CI: [−1.25 to −0.17], p = .02) from preinfusion. Further, PedsQL 4.0 scores had a statistically significant negative association with CAM-S scores (−0.03, −0.05 to −0.01, .001). Those in the WB at the second visit had a lower average pre- and post-CAM-S score compared to those in UC at the first visit (−0.51, −1.92 to 0.88, .49). This was not statistically significant. Table 2 summarizes these results.
CAM-S Multivariate Mixed Linear Regression Results
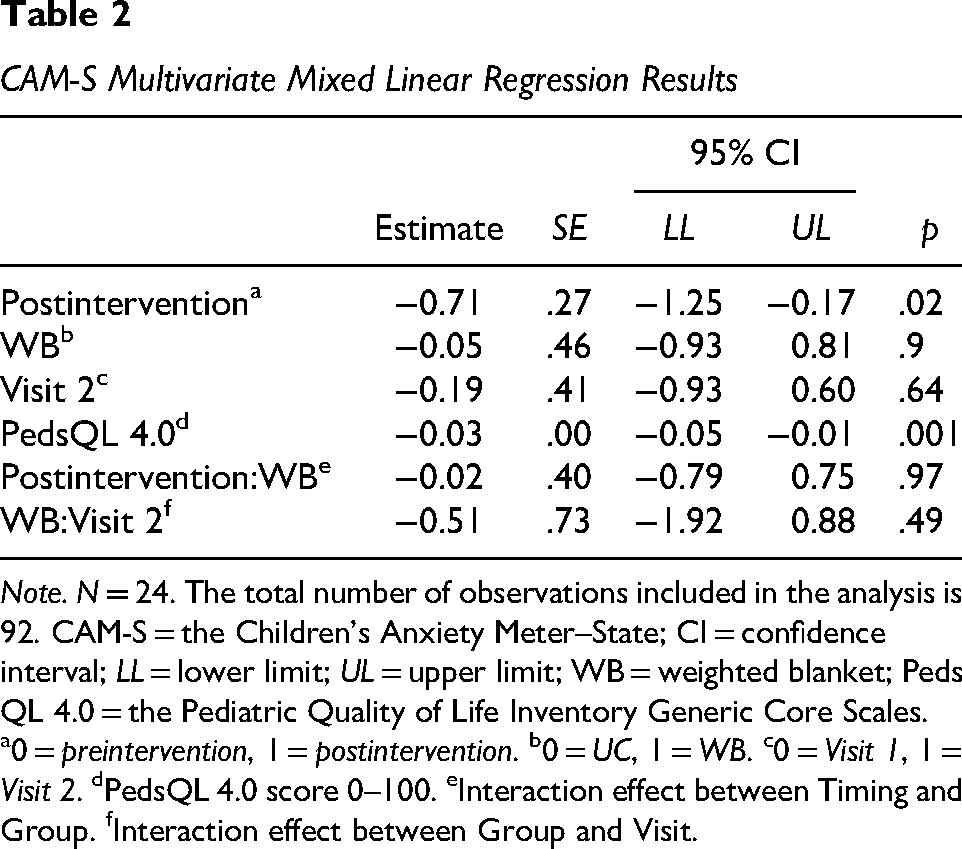
Note. N = 24. The total number of observations included in the analysis is 92. CAM-S = the Children's Anxiety Meter–State; CI = confidence interval; LL = lower limit; UL = upper limit; WB = weighted blanket; Peds QL 4.0 = the Pediatric Quality of Life Inventory Generic Core Scales.
0 = preintervention, 1 = postintervention. b0 = UC, 1 = WB. c0 = Visit 1, 1 = Visit 2. dPedsQL 4.0 score 0–100. eInteraction effect between Timing and Group. fInteraction effect between Group and Visit.
For the PedsQL 4.0, those in the WB group had lower scores compared to those in the UC group (B = −4.4, CI: [−18.4 to 9.56], p = .53). Visit 2 also had lower scores compared to Visit 1 (−4.6, −18.6 to 9.39, .54). However, those in the WB at Visit 2 had higher scores compared to those in the UC at Visit 1 (9.94, −17.0 to 36.8, .48). These were all not statistically significant. Table 3 summarizes these results.
PedsQL 4.0 Multivariate Mixed Linear Regression Results
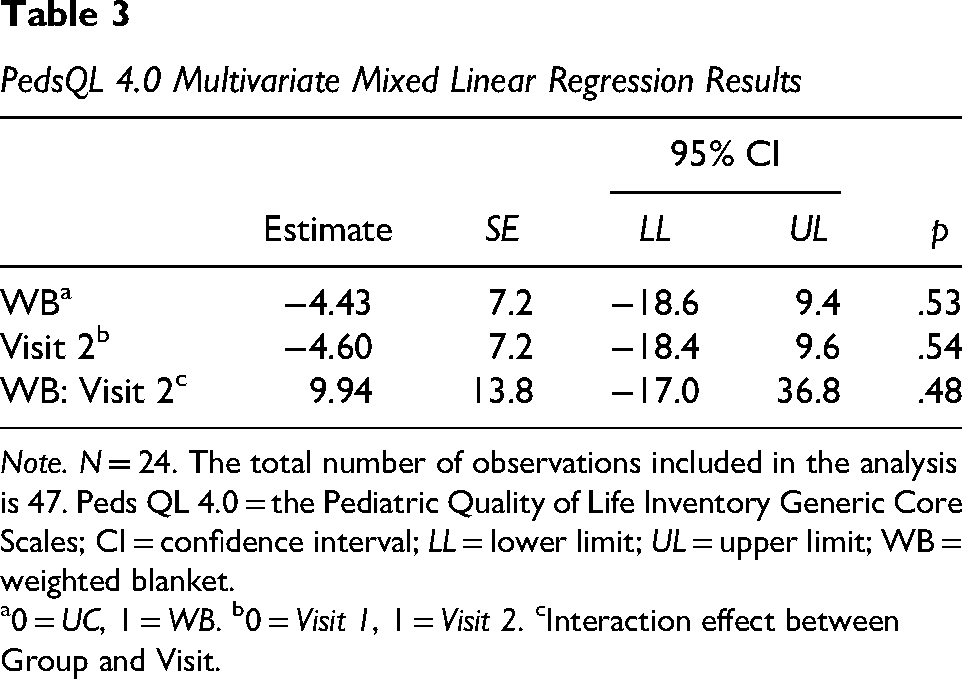
Note. N = 24. The total number of observations included in the analysis is 47. Peds QL 4.0 = the Pediatric Quality of Life Inventory Generic Core Scales; CI = confidence interval; LL = lower limit; UL = upper limit; WB = weighted blanket.
0 = UC, 1 = WB. b0 = Visit 1, 1 = Visit 2. cInteraction effect between Group and Visit.
Discussion
Limitations
There were some limitations to the study. Anxiety is complex and multifactorial. Pediatric oncology patients experience higher levels of anxiety than healthy counterparts at baseline. Chemotherapy infusions are just one aspect that may contribute to anxiety. Measuring anxiety for more than two visits might have given a more comprehensive understanding of if and how a weighted blanket specifically impacts anxiety. It cannot be ruled out that anxiety lessens with the passage of time or with repeated chemotherapy visits. This could be another area of future research. Another limitation to the study was it was not blinded. Results showed that this was a benefit to the patient as shown by those who started with a weighted blanket came in with lower anxiety, but blinding could have strengthened the results of the study. The study was also completed at a single site, which lessened the opportunity to have a larger sample size. It may also reduce external validity. Lastly, the study had a small sample size. The goal was to accrue 120 participants, assuming a 35% accrual rate. After a year, the accrual rate was approximately 5%. Accrual decreased to 26 participants, which was enough to hit power in the analysis. Based upon the sample size and single site, the study generalizability is limited to this population. Additional research is needed to be generalizable to broader populations.
Interpretation
This study indicates that anxiety was reduced during chemotherapy infusions. Multitudes of interventions, such as art therapy and virtual reality, have been cited in literature to ameliorate or reduce pain and anxiety in the pediatric oncology population (Raybin et al., 2024; Semerci et al., 2021; Wong et al., 2021). Additionally, providing patient-centered or person-centered care has positive impacts on care impacts and perceptions of quality of care. This type of care includes respecting, acknowledging, and responding to the patient's individual needs. The effective communication of the nurse to the patient has been considered more important than the physical care provided (Kwame & Petrucka, 2021). Connecting with patients is the backbone of providing high quality care, additional modalities, such as weighted blankets, to reduce anxiety further enhance their experiences and can lead to improved outcomes.
Quality of life (QoL) has been studied for both healthy children and those with chronic health conditions. This study showed an overall QoL score of 66.68 for Visit 1 and then increasing to 69.57 for Visit 2. Those getting a weighted blanket in their second visit rated their quality of life at 74.8. Varni et al. (2002) showed a QoL score of 69.7 for the pediatric oncology patients they studied, compared to a score of 87.61 for their heathy counterparts. Additionally, Smyth and Jacobson (2021) reports QoL scores ranging from 80.5–89.17 for healthy children. This study aligns with previous studies done as participants had slightly better QoL than the average oncology patient, but lower than their healthy counterparts.
This research aligns and is comparable to other studies in which weighted blankets were assessed to understand their impacts on anxiety. Weighted blankets have the implication to be a safe, supportive, adjunct therapy for anxiety in adults and pediatric patients in a clinical setting. There is a growing body of research showing the positive impacts of weighted blankets with users self-reporting a more relaxed feeling, reduced stress and less anxiety symptoms (Eron et al., 2020). Weighted blankets and their use as a therapeutic tool have been well established and documented through credible research (Eron et al., 2020), and these results do align in a general sense. Limitations within this study are due to sample size, inconclusive evidence, and limitations in the strength and correlation due to study design. There should be consideration for future studies to continue to examine the effectiveness of weighted blankets throughout different domains such as physical and psychological impact or biomarkers (saliva or blood testing) to further understand and improve quality of life for those that experience anxiety either in a medical setting or at home. Additionally, further research could examine the effect of other usual care interventions in conjunction with weighted blankets on anxiety.
Footnotes
Author Contributions
Jennifer Olson: conceptualization, methodology, validation, investigation, resources, writing–original draft, writing–review and editing, visualization, supervision, project administration, funding acquisition; Leanne Adamson: conceptualization, methodology, validation, investigation, resources, writing–original draft, writing–review and editing, visualization, funding acquisition; Cassie Lang: conceptualization, methodology, validation, investigation, resources, writing–original draft, writing–review and editing, visualization, funding acquisition; Kelly Miller: conceptualization, investigation, resources, writing–original draft, writing–review and editing, visualization; Flori Legette: investigation, resources; Elizabeth Phillips: software, formal analysis, data curation, writing–original draft; Figaro Loresto: conceptualization, methodology, validation, software, formal analysis, resources, data curation, visualization, writing–original draft, writing–review and editing, funding acquisition.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose the following financial support: DAISY Foundation (grant number: JPB-2021-858).
Protocol
COMIRB-21-3150
Registration
ClinicalTrials.gov: NCT05041075