
Abstract
Background
Adherence to treatment following hematopoietic stem cell transplant (HSCT) is critical, yet the complexity and demands of postdischarge regimens often lead to suboptimal adherence among families unprepared for the transition home. Discharge teaching has been reliably evaluated using the Quality of Discharge Teaching Scale (QDTS) across several health conditions, with higher scores associated with improved parental readiness and pediatric health outcomes. This scale may be helpful in identifying areas for improvement in pediatric HSCT discharge teaching if validated in a pediatric HSCT population.
Method
This study recruited 120 caregivers of children who recently underwent HSCT to complete the QDTS along with measures of parental efficacy/control, psychological distress, and psychosocial risk factors. Confirmatory factor analysis (CFA) was used to examine the factor structure and measurement invariance of the scale, while internal reliability was assessed using Cronbach's alpha and correlations with related constructs.
Results
CFA showed that the QDTS had adequate model fit and was invariant across biological sex and income, but not diagnosis. The QDTS demonstrated good internal reliability (content α = .76; delivery α = .90) and criterion validity, with significant correlations with the subscales of related constructs. Independent samples t-tests revealed that caregivers of children with malignant diagnoses reported worse quality of discharge teaching compared to those with nonmalignant diagnoses.
Discussion
This study supports the use of the QDTS as a valid and reliable tool for assessing the quality of discharge teaching for caregivers of children undergoing pediatric HSCT.
Introduction
Each year, approximately 2,600 pediatric patients in the United States undergo hematopoietic stem cell transplant (HSCT) to treat a range of immunological, genetic, oncological, and hematological conditions. Approximately 2,600 pediatric patients receive an HSCT every year in the United States for a range of immunological, genetic, oncological, and hematological conditions (13–12). While inpatient HSCT care is closely managed by a multidisciplinary medical team, responsibility for a complex and demanding outpatient treatment regimen shifts to the family upon discharge. This transition can be particularly challenging, as families must quickly learn to manage multiple medications with varying dosing schedules and frequent adjustments (Weiss et al., 2017). Suboptimal adherence to this treatment regimen is common (McGrady et al., 2014; Ralph et al., 2023) and is associated with increased risk of life-threatening infections, disease recurrence, and death (Pai et al., 2018; Pereira et al., 2010). Therefore, children and families who are not adequately prepared for the transition from hospital to home are particularly at risk for poor health outcomes (Lerret et al., 2015; Lerret & Weiss, 2011; 37–39). Prior research has shown that medication management training prior to discharge can help families prepare for the transition home (Cody et al., 2020; Tang et al., 2019). However, inadequate or inconsistent training, particularly regarding when and how to administer medications, has been linked to suboptimal medication following pediatric HSCT (Szulczewski et al., 2022). Given the critical role of outpatient medication management, there is a clear need for methods to assess and enhance the training that families receive.
The Quality of Discharge Teaching Scale (QDTS) is a promising measure that can be used to evaluate the proficiency of the training caregivers receive when assuming their child's medical care post-HSCT. This scale was originally developed to measure caregiver perception of the quality of the teaching they receive prior to hospital discharge (Weiss et al., 2008). Results from studies using the QDTS suggest that improved discharge teaching is associated with improved parental readiness for the transition to home and improved pediatric health outcomes following hospital discharge (Gladbach et al., 2021; Lerret et al., 2015; Lerret & Weiss, 2011; Tong et al., 2021). For example, perceived improvements in the quality of discharge teaching among caregivers of children with Type 1 diabetes were associated with improved parental readiness for the transition to home and improved hemoglobin A1C (Tong et al., 2021). In another study, high ratings on the QDTS were associated with greater discharge readiness, improved parent coping, and lower hospital readmission rates among children following hospital discharge (Weiss et al., 2017). Among adult patients, improvements in the quality of HSCT discharge teaching enhanced patients’ preparedness for the transition to home (Gladbach et al., 2021). Therefore, this measure may be helpful in identifying areas of needed improvement in pediatric HSCT discharge teaching to improve parental readiness and child health outcomes.
The QDTS assesses two different domains—content received and information delivered by a medical team (Weiss et al., 2007). The two subscales were identified using principal component exploratory factor analysis and account for about 54.2% of scale variance in a sample of adult surgical patients (Weiss et al., 2007). The content received subscale consists of six different dimensions: information about at-home care, knowledge about treatment and medication, practice with treatment and medication, knowledge of when to contact the care team, expected emotions, and learning needs of other family members. The information delivered subscale measures parent perceptions of the teaching skill of the instructor (e.g., nurse, pharmacist) in seven dimensions, including listening and answering questions, sensitivity, comprehension, consistency, confidence promotion, managing family anxiety, and providing feedback at convenient times. The scale has been shown to have good reliability (α = .88–.92) in a variety of health conditions, including adult HSCT, pediatric solid organ transplantation, and hospitalized children (Gladbach et al., 2021; Lerret & Weiss, 2011; Weiss et al., 2008). However, to the best of our knowledge, the scale has never been validated in a pediatric HSCT population. Thus, the present study examined the factor structure, measurement invariance, reliability, and validity of the QDTS in a pediatric HSCT population.
Method
Participants
Primary caregivers of children who received an HSCT were eligible to participate if their child was (a) less than 12 years old, (b) discharged from their HSCT inpatient admission less than 2 weeks prior to data collection, (c) prescribed an oral or intravenous medication postdischarge, and (d) if the caregiver was fluent in English. Caregivers were ineligible for the study if the child's medical status or the parent's cognitive status precluded completion of the questionnaires as determined by medical chart review and medical team report. For descriptive statistics, please see Table 1.
Descriptive Statistics
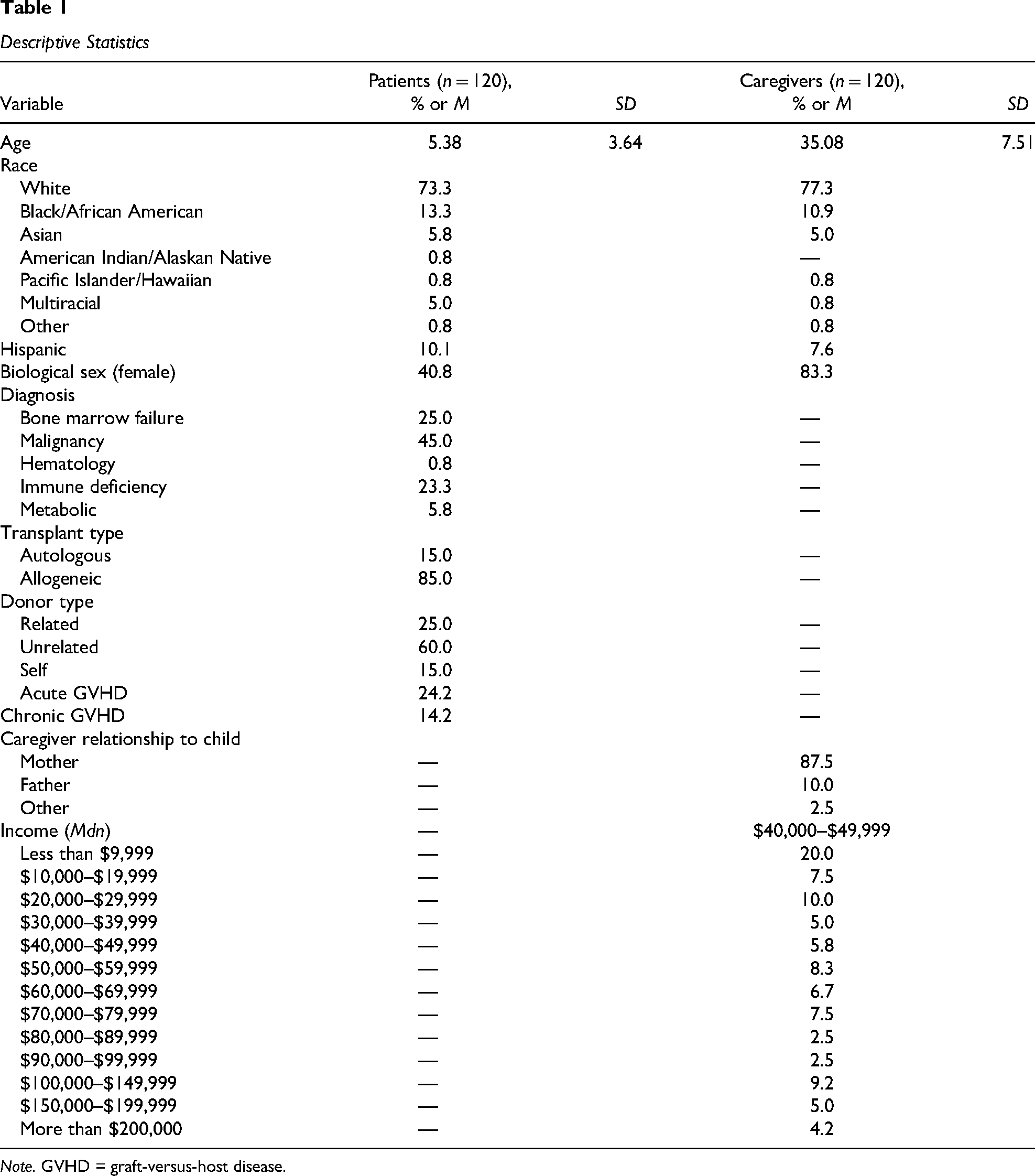
Note. GVHD = graft-versus-host disease.
Procedures
The current study is part of a larger longitudinal multisite study examining medication adherence in children who have received an HSCT (Pai et al., 2020). Primary caregivers (i.e., the parent primarily involved in their child's medical care) of children less than or equal to 12 years of age who underwent HSCT were recruited from three different children's hospitals in the midwestern, northeastern, and midsouth regions of the United States. Caregivers of children less than 12 years of age were included in the larger study because they are primarily responsible for managing their child's medication regimen and thus were best positioned to report on adherence-related behaviors and challenges. Recruitment methods and study protocols were the same across the study sites. Additionally, the study was approved by the Institutional Review Board at all sites. Eligible families were identified by the HSCT team at each hospital via electronic medical record review. Next, families were approached by study staff during their initial inpatient admission or during an outpatient clinic appointment within the first 2 weeks postdischarge. Following informed consent, caregivers completed baseline questionnaires. Participants were compensated for their time and effort. Two hundred and thirty-eight caregivers were approached across the three sites between 2013 and 2018, and 120 families agreed to participate. There were no differences in child age or gender in families who participated versus those who declined to participate.
Measures
Quality of Discharge Teaching Scale
Caregivers completed the QDTS. This scale was designed to measure the quality of the content and delivery of education provided by the medical team before discharge. The QDTS consists of a six-item content subscale and a 13-item delivery subscale (Weiss et al., 2007), and responses on the QDTS are on an 11-point Likert scale ranging from 0 (none) to 10 (a great deal). Items for each subscale are summed to create two subscale scores (content and delivery), where higher scores represent a greater quality of discharge teaching (Weiss et al., 2007).
Parental Efficacy and Control Questionnaire (PECQ)-HSCT
The PECQ-HSCT is a 37-item caregiver self-report measure that was developed to assess HSCT-related parental self-efficacy and perceived control across four subscales: medical locus of control (eight items), treatment-specific efficacy (13 items), perception of support (eight items), and expectations of allied health (eight items; Pai et al., 2020). Items are rated on a 4-point Likert scale ranging from strongly disagree (1) to agree (4). Higher scores represent greater HSCT-related parental self-efficacy and perceived control. The PECQ-HSCT has demonstrated acceptable factor structure, high test–retest reliability, and criterion validity in a sample of caregivers of children who received an HSCT (Pai et al., 2020).
Brief Symptom Inventory (BSI)
The BSI was used to assess psychological distress. This 53-item measure consists of nine subscales; however, the current study utilized the depression, anxiety, interpersonal, and global symptom subscales (Derogatis, 1993). Items were rated by caregivers on a 5-point Likert scale from not at all (0) to extremely (4), where higher scores indicate higher levels of distress. Scores were transformed into T-scores, and subscale scores ≥63 are considered clinically significant. The BSI has been shown to have good test–retest reliability, high construct validity, and has been used in research with caregivers of children with complex medical conditions, including HSCT (Bonner et al., 2007; McGrady et al., 2021; Pai et al., 2020).
Psychosocial Assessment Tool 2.0 (PAT 2.0)
The PAT 2.0 is a screening tool used to assess psychosocial risk factors among families of children newly diagnosed with cancer. The current study utilized a portion of this caregiver-report measure to capture demographic factors, including caregiver education, marital status, and caregiver relationship to the patient. Family annual income and race and ethnicity of the caregiver and child were also measured using a general demographic questionnaire.
Electronic Medical Record Review
Patients’ electronic medical records were reviewed by study staff to obtain medical information, including diagnosis, transplant type (i.e., allogeneic, autologous), and biological sex.
Data Analyses
Data analysis occurred in two phases—a factor analysis followed by a validation phase. In the first phase, confirmatory factor analysis (CFA) was used to examine the factor structure of the QDTS. Rather than employing exploratory methods, the current study tested the published factor structure established in prior research (Gladbach et al., 2021; Lerret & Weiss, 2011; Weiss et al., 2008). This structure was retained based on its prior validation in other pediatric populations (Weiss et al., 2017). Next, measurement invariance was assessed using multigroup CFA across groups based on biological sex (male/female), income (below/above median income), and diagnosis (malignant/nonmalignant). Measurement invariance was analyzed for all groups in three stages: configural, metric, and scalar (Gregorich, 2006). Configural invariance was tested by freeing factor loadings for all items across groups, freeing thresholds for all items across groups, holding scale factor means at 1 across groups, and freeing factor variance for all items across comparison groups (Kamody et al., 2014; Millsap & Yun-Tein, 2004; Muthén & Asparouhov, 2018). Metric invariance assumed configural invariance, which confirmed that factor loadings were equal across groups. Scalar invariance assumed metric invariance, which confirmed that the indicator threshold was equal across groups (Millsap & Yun-Tein, 2004; Muthén & Asparouhov, 2018).
To account for ordinal response format and missing data, CFAs were conducted using mean- and variance-adjusted weighted least squares estimation (Asparouhov & Muthén, 2010). Model fit was evaluated using the model chi-square, root-mean-square error of approximation (RMSEA), standardized root-mean-square residual (SRMR), and the comparative fit index (CFI). Generally, higher chi-square values indicate a poor model fit (Browne & Cudeck, 1993), RMSEA values less than .05 indicate good model fit and values between .05 and .08 indicate acceptable model fit (Hu & Bentler, 1999; Steiger, 1990), SRMR values of ≤.08 indicate good model fit (Hu & Bentler, 1999), and CFI values ≥.9 representing adequate model fit (Bentler, 1990; Bollen, 1989). RMSEA, SRMR, and CFI values were used to supplement model chi-square fit, as these indices are more sensitive to slight misspecifications in model structure and sample size (Bollen & Long, 1993). Regarding invariance testing, invariance is supported at the metric and scalar levels if the model fit is not worse than the previous level of invariance based on the change in CFI values (Gregorich, 2006; Kamody et al., 2014; Kline, 2015). To be considered invariant across groups, the change in CFI must be ≤−.01 (Millsap & Yun-Tein, 2004; Muthén & Asparouhov, 2018). As a final step, independent samples t-tests were used to determine group differences among scales found to be variant across.
Internal reliability was assessed during the second phase of analysis using Cronbach's alpha. Additionally, criterion validity was analyzed using Pearson's correlations to compare the QDTS to the PECQ-HSCT, and the BSI. CFA and invariance analyses were conducted in Mplus Version 8.9, and Cronbach's alpha, correlations, and t-tests were conducted in SPSS 29 (IBM Corp., 2023).
Results
CFA and Measurement Invariance
As shown in Table 2, CFA and measurement invariance were examined for both subscales of the QDTS. The factor structure of the QDTS yielded adequate model fit (χ2 = 634.2, p < .001; RMSEA = .11; CFI = .71; SRMR = .11) and was found to be invariant across biological sex and annual income but not diagnosis (ΔCFI > .01). See Figure 1 for the factor structure of the QDTS.
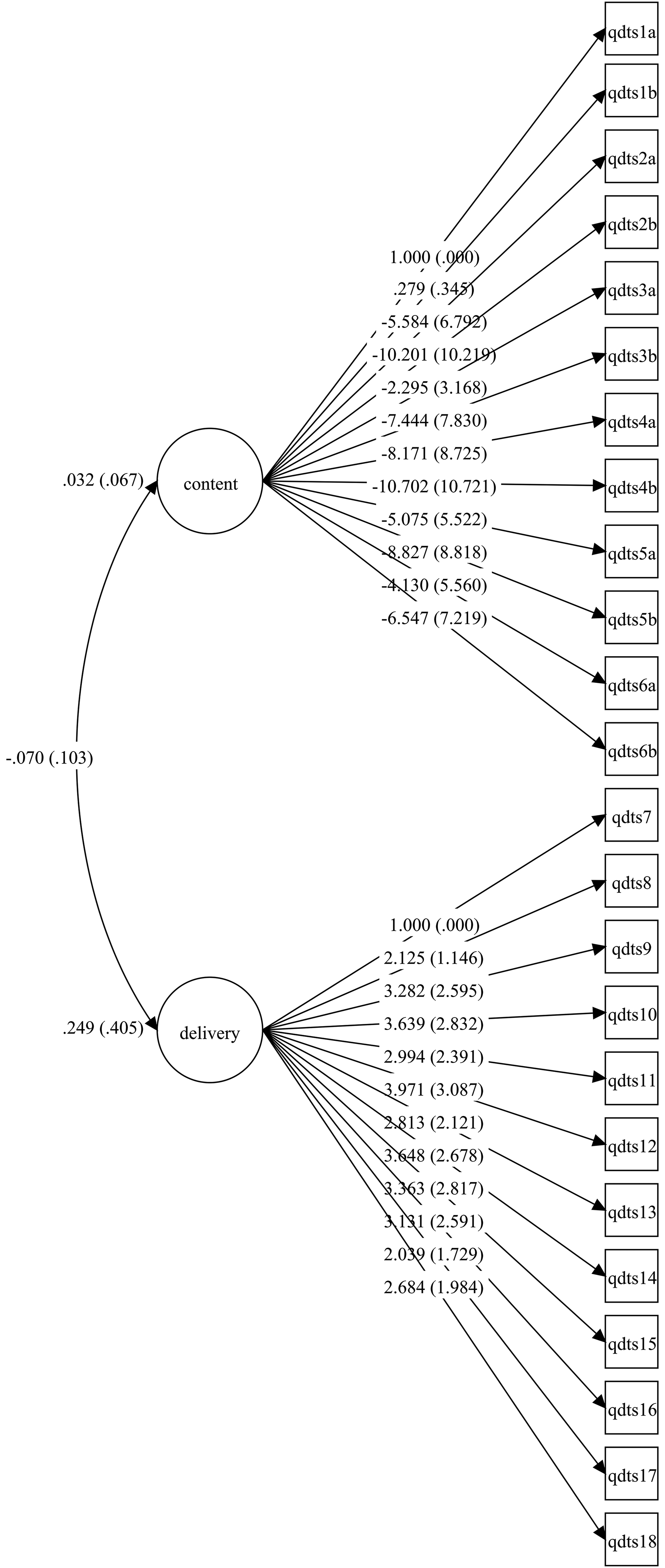
Factor Structure of the QDTS.
Overall Model Fit and Invariance Testing of the QDTS
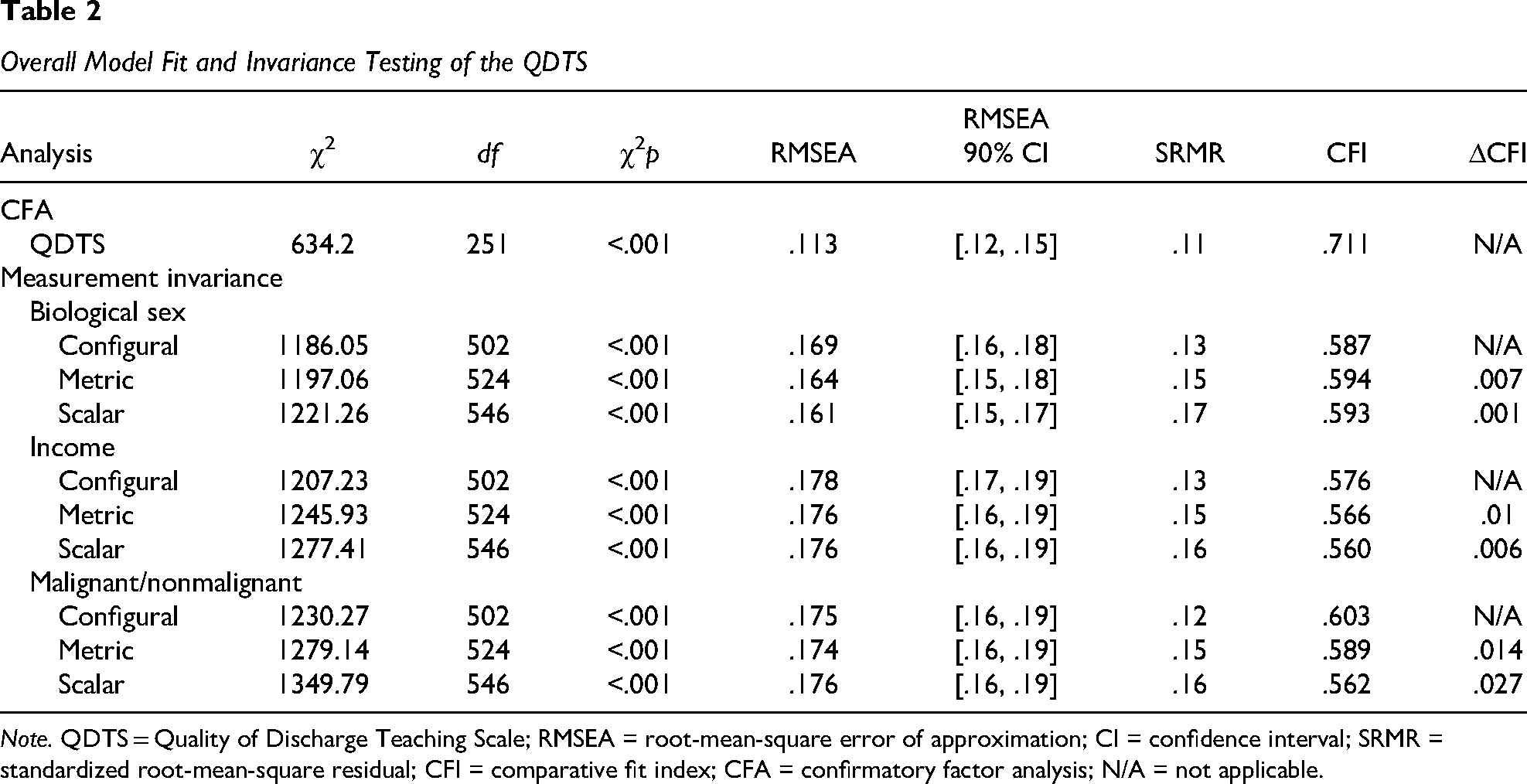
Note. QDTS = Quality of Discharge Teaching Scale; RMSEA = root-mean-square error of approximation; CI = confidence interval; SRMR = standardized root-mean-square residual; CFI = comparative fit index; CFA = confirmatory factor analysis; N/A = not applicable.
Internal Reliability and Criterion Validity
Following the completion of the first phase of analysis, the second phase of analysis examined the internal reliability and criterion validity of the QDTS for the entire sample. Subscales demonstrated good internal consistency (content α = .76; delivery α = .90). The QDTS showed good criterion validity, as shown in Table 3. Generally, QDTS subscales correlated in the expected direction with the subscales from both the PECQ-HSCT and the BSI. More specifically, the content subscale significantly correlated with the treatment-specific efficacy (r = .33), perception of support (r = .59), and expectations of allied health subscales (r = .35) of the PECQ-HSCT but not the medial locus of control (r = .17) subscale. Additionally, the content subscale correlated with interpersonal (r = −.24), anxiety (r = −.32), and global symptom (r = −.31) subscale T-scores on the BSI, but not the depression subscale (r = −.20). The delivery subscale significantly correlated with the perception of support subscale (r = .34) on the PECQ-HSCT, but not the medial locus of control (r = .04), treatment-specific efficacy (r = .06), or expectations of allied health (r = .03) subscales. The delivery subscale was not significantly correlated with interpersonal (r = −.03), depression (r = −.11), anxiety (r = −.14), or global symptom (r = −.12) subscale T-scores on the BSI.
Correlations Between Subscales of the QDTS
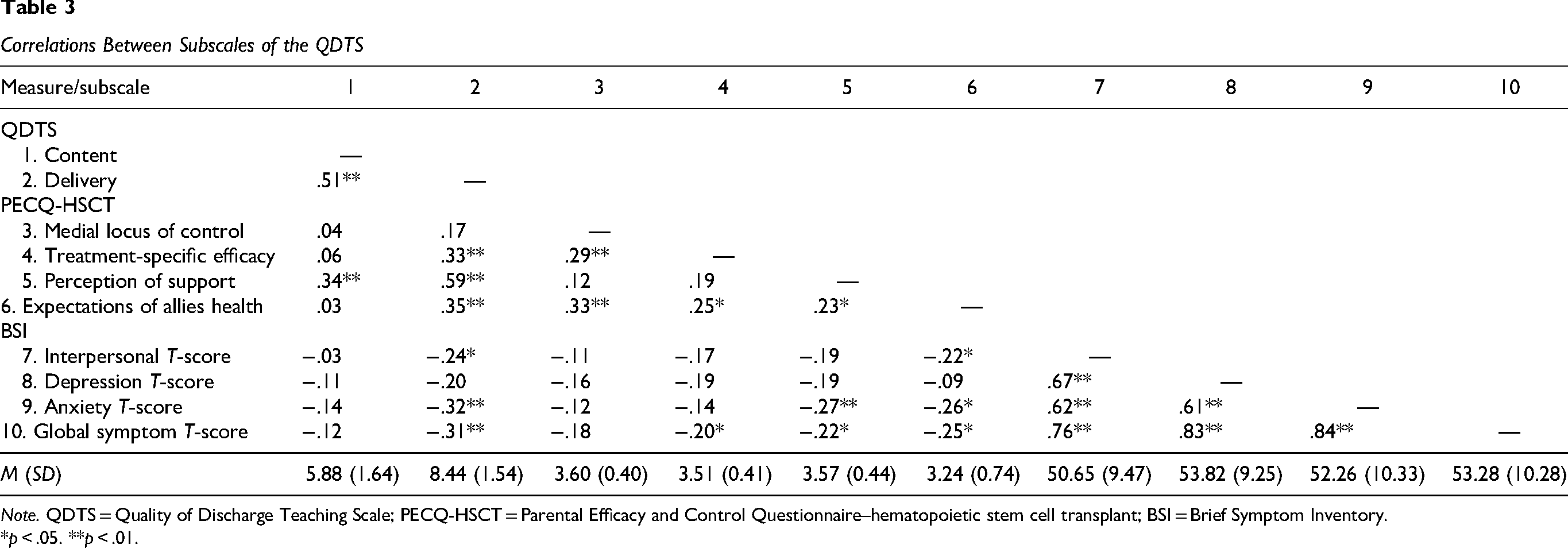
Note. QDTS = Quality of Discharge Teaching Scale; PECQ-HSCT = Parental Efficacy and Control Questionnaire–hematopoietic stem cell transplant; BSI = Brief Symptom Inventory.
*p < .05. **p < .01.
Independent Samples t-Test
An independent samples t-test was conducted to examine differences in QDTS scores among caregivers of children with and without a malignant diagnosis. Analyses revealed differences in content, t(93) = 2.6, p = .01, and delivery, t(93) = −1.9, p = .03, subscales, with caregivers of children with a malignant diagnosis reporting worse quality of discharge teaching (M = 5.4–8.8) compared to those with a child with a nonmalignant diagnosis (M = 6.2–8.2).
Discussion
Overall, the QDTS demonstrated adequate model fit and measurement invariance across biological sex and annual income, along with strong internal consistency and criterion validity. These findings suggest that the QDTS is a valid and reliable tool for assessing the quality of discharge education provided to families following pediatric HSCT.
Pediatric HSCT is a crucial and potentially life-saving treatment for children with rare immunological, genetic, oncological, and hematological conditions (D'Souza et al., 2020). However, post-HSCT discharge care is complex, demanding, and often challenging for caregivers to manage effectively (Weiss et al., 2017). Caregivers frequently report difficulties adhering to their child's medical regimen after transitioning from hospital care to home, which can place their child at greater risk for adverse health outcomes (Chardon et al., 2022; Morrison et al., 2017; Pai et al., 2018). As such, it is critical for caregivers to receive high-quality discharge instructions prior to transitioning home. This is especially true when the negative health outcomes associated with suboptimal discharge teaching instructions are considered; these outcomes can include an increased risk of life-threatening infections, disease recurrence, and death (Pai et al., 2018; Pereira et al., 2010). Therefore, tools are needed that can quickly and accurately assess caregivers’ perceptions of the quality of the discharge teaching that they receive as a method to identify areas of needed intervention. The QDTS was originally developed to assess the quality of discharge teaching received by caregivers of hospitalized children, and this measure was previously shown to have good reliability in other populations (Gladbach et al., 2021; Lerret & Weiss, 2011; 37–37).
Results from the current study provide preliminary support for the QDTS as a useful tool in assessing the quality of discharge teaching pediatric HSCT caregivers receive before transitioning home. More specifically, the QDTS was found to have an adequate factor structure in our sample, and it was found to be invariant across biological sex and income. However, after additional statistical probing, the QDTS was found to be variant across malignancies. When evaluating group differences, caregivers of children with a malignant diagnosis reported receiving worse quality of discharge teaching. This may be due to several potential factors. Most likely, this is at least in part due to treatment-related differences of HSCT for children with malignant diseases including, but not limited to: more intensive conditioning regimens, higher prior toxicities, timing of treatment being disease-driven, and benefits of mild graft-versus-host disease. These factors can be associated with higher mortality and morbidity and more complex treatment regimens upon discharge (Armenian et al., 2011; Michel et al., 2007). Additionally, there may be some psychosocial factors that could be contributing. Frequently, children with a malignancy have had lengthy and extensive hospitalizations immediately prior to HSCT, whereas children with a nonmalignancy have a much wider range of experiences leading up to HSCT. There may also be higher concerns with risk of relapse, further treatments required following HSCT discharge, and uncertainty regarding prognosis (Perez et al., 2019). Cumulatively, it would be reasonable to conclude that these factors may overshadow the technical aspects of discharge education. Finally, caregivers’ previous experience managing their child's cancer treatment prior to transplant or expectations regarding follow-up needs (i.e., caregivers may anticipate more extensive follow-up care needs, which may accompany a desire for more comprehensive discharge information that they feel they did not receive) may influence their perceptions of care quality. As such, caregivers of children receiving HSCT for a malignant diagnosis may require more comprehensive discharge teaching or other supports to enhance their ability to assume their child's medical regimen postdischarge.
Findings from this study must be interpreted in light of several limitations. First, authors of the present study chose to examine the published factor structure of the QDTS (Gladbach et al., 2021; Lerret & Weiss, 2011; Weiss et al., 2008) instead of using exploratory methods to systematically evaluate the underlying theoretical structure. The factor structure was retained as it has previously been validated in other pediatric populations (Weiss et al., 2017). Second, the study sample consisted primarily of White non-Hispanic children who received an allogeneic HSCT. For this reason, measurement invariance of the QDTS across race, ethnicity, and transplant type could not be evaluated. Third, while this study was able to extend knowledge on many psychometric properties of the QDTS, we were not able to examine test–retest reliability or stability. As such, future research is needed to further explore the psychometric properties of this measure in a more diverse sample of patients.
Ultimately, findings from this study provide support for the use of the QDTS as a means of assessing the quality of discharge teaching that caregivers receive following their child's HSCT. The QDTS was found to be valid, reliable, and invariant across biological sex and annual income, indicating that this measure has the potential to be a useful tool in assessing the quality of HSCT discharge teaching caregivers receive. However, the underlying construct being measured, or the quality of discharge teaching, may vary between children with and without a malignant diagnosis, a distinction that warrants further exploration. Additional research is needed to further examine the QDTS in this population prior to implementation.
Footnotes
Ethical Approval
This study received ethical approval from the Institutional Review Board at Cincinnati Childrens Hospital Medical Center (Approval No. 2011-1566) on December 6, 2011.
Consent to Participate
Participants gave written informed consent before beginning questionnaires.
Funding
The authors disclose the following financial support: National Institutes of Health, the National Cancer Institute (Grant No. R01 CA157460-01; awarded to Ahna L. H. Pai).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.