
Abstract
Background
Children with cancer and their families face complex medical, emotional, and practical challenges. Education delivered by health care providers is a critical component of high-quality pediatric oncology care, yet the scope, feasibility, acceptability, and effectiveness of such interventions are not well characterized. We aimed to synthesize the literature on health care provider–delivered educational interventions for children with cancer and their families, focusing on intervention content, the purpose of interventions; intervention feasibility and acceptability for implementation and evaluation; and intervention effectiveness on participant outcomes.
Method
We conducted a rapid scoping review of empirical studies published between 2013 and 2024 using PubMed, PsycInfo, and CINAHL. Studies included examined feasibility-focused educational interventions delivered by health care professionals to children with cancer and/or their caregivers. Data were extracted and analyzed descriptively using the domains of the Fitch and Steele Supportive Care Framework to categorize educational content.
Results
Thirty-five articles (32 unique studies) were included. Most studies enrolled caregivers, predominantly mothers, and over half of the identified interventions were delivered remotely. Educational content frequently addressed psychological (71%) and social (43%) needs, with less attention tophysical, medical, practical, and spiritual domains. Most (84%) interventions were deemed feasible. Of 24 articles examining effectiveness, 97% reported positive family health-related impacts, particularly on anxiety, stress, and care giver knowledge outcomes.
Discussion
Educational interventions appear feasible, acceptable, and well-received, with early evidence of effectiveness. Future research should prioritize theory-informed design, standardized feasibility/acceptability metrics, inclusive reporting, and the assessment of long-term and equitable impacts across diverse populations of children and families.
Introduction
Over the last several decades, advancements in the treatment of childhood and adolescent cancers have resulted in substantial improvements in 5- and 10-year survival rates for most cancer types (Williams et al., 2021). Despite this overall improvement, a cancer diagnosis remains a life-altering event for the child and family, who face concerns related to managing both immediate and long-term side effects, disruption of roles and responsibilities, day-to-day functioning, and financial and employment-related stress (Rodgers et al., 2016). Families often take on additional roles in caring for their child, including acting as patient advocates, care coordinators, and direct care providers (Jibb et al., 2021; Koch & Jones, 2018; Zupanec et al., 2025). As a result, families must rapidly adjust to the child's diagnosis while learning complex skills and scientific information (Rodgers et al., 2016; Williams et al., 2021).
Patient and caregiver education is central to the provision of high-quality children's cancer care. Families require tailored, specialized education to effectively care for their child and to empower family wellness (Levine et al., 2019). Nurses, physicians, and other health care professionals play critical roles in providing this education (Landier et al., 2016), which can include information about diagnosis and treatment, direct care tasks, symptom management, health monitoring, and guidance on appropriate child and family activities. Despite this, to date, there is very little evidence to support what defines quality patient and family education.
The Fitch and Steele Supportive Care Framework offers a means to conceptualize the types of support that those impacted by cancer may need (Fitch, 2008). The Framework domains for needed educational content are: (1) medical (e.g., cancer biology, treatment), (2) physical (e.g., symptoms and their management), (3) psychological (e.g., coping, mental wellness), (4) social (e.g., maintaining relationships), (5) spiritual (e.g., reflecting on the meaning of life), and (6) practical (navigating finances, school, childcare; Fitch, 2008). A lack of adequate education within these different domains can negatively impact the health of the child with cancer and their family (Landier et al., 2013).
The quality and effectiveness of educational interventions also vary depending on content, understandability, accessibility, audience, and delivery method—all of which relate to the feasibility and acceptability of implementing and evaluating interventions (Beets et al., 2021). Despite this, there is currently no review of the extant literature that synthesizes the content, function, feasibility, acceptability, and effectiveness of educational interventions in pediatric oncology. To address this gap, we aimed to answer the following question: What is known about feasibility-focused studies of health care provider–delivered–educational interventions for children with cancer and their primary family caregivers? To answer this question, we aimed to describe the: (a) content and purpose (including targeted user and delivery method) of such educational interventions; (b) feasibility/acceptability of examination of their effectiveness and/or implementation into clinical practice; and (c) effectiveness on child and family physical and psychosocial health.
Method
Study Design
We undertook a rapid scoping review following the methods by Arksey and O’Malley (2005) and guidance for high-quality rapid reviews (Garritty et al., 2024; Klerings et al., 2023; Nussbaumer-Streit et al., 2023). Reporting for the review is in accordance with the PRISMA-ScR criteria (McGowan et al., 2020; Supplementary Material A). A protocol for this review was not registered; however, a detailed protocol was prepared through group discussion and can be accessed upon request.
Study Identification and Selection
We searched PubMed/Medline, PsycInfo, and Cumulative Index to Nursing and Allied Health Literature on November 8, 2024. Our search strategy was based on that previously used in similar scoping reviews (Papadakos et al., 2022) and was developed with the assistance of a health sciences librarian using synonyms for pediatrics and education (Supplemental B). Given the nature of rapid reviews and the overall broad goal of this review, we limited our search to the last 10 years (2013–2024). Due to the constantly evolving landscape of pediatric oncology and available interventions, this time limitation helped keep the number of identified articles feasible for a rapid review and ensured we identified the most recent and relevant interventions available. This year limitation approach in rapid reviews has been shown as a method to limit workload while simultaneously maintaining accuracy (Xu et al., 2022). We piloted the strategy by ensuring it located five articles that fit our inclusion criteria and were known to our team. Adjustments to the strategy were made until the strategy was inclusive of our five-article test set. In addition to this search strategy, we also included citations published prior to 2013 located in the reference lists of identified studies.
Study inclusion criteria were English-language empirical studies using any methodology and that examined the feasibility/acceptability of health care professional-delivered educational interventions for children with cancer, their family caregivers, and families. We therefore included studies using qualitative and quantitative approaches and a variety of study designs, including but not limited to observational studies, pilot randomized controlled trials (RCTs), and RCTs.
Children with cancer were defined as children 0–18 years of age diagnosed with any form of cancer, in any stage of treatment, care, or survivorship. If a study sample included those both above and below 18 years, studies were included if at least 50% of participants were treated in a pediatric hospital and all participants were under the age of 25 years. Primary family caregivers were defined as the child's parent, legal guardian, or any other informal caregiver responsible for the child's care.
Educational interventions were defined as those including information, behavioral instructions, or advice given regarding cancer or managing cancer-related symptoms, treatment, and lifestyle changes delivered by health care professionals who could be physicians, nurses, social workers, or other interdisciplinary team members, such as child life specialists. Interventions could be delivered in-person, through written communication, or virtually.
Feasibility was defined as whether an intervention is deemed appropriate for further testing (Pearson et al., 2020). A feasibility study asks whether something can be done, should it be done, and how should it be done (National Institute for Health and Care Research, 2023). These studies check that the study processes (recruitment, randomization, treatment, follow-up) are all designed appropriately and can be successfully implemented to assess for effectiveness. Associated outcomes could include attrition, accrual, adherence, acceptability, user or provider fidelity, intervention issues, satisfaction, recruitment, and outcome measure completion. Often, feasibility is evaluated in concert with acceptability, which asseses interventional characteristics like understandability, appeal, and satisfaction (Menard et al., 2014).
Title and abstract and full-text screening were completed in duplicate on Distiller SR using one human screener (A.K. or R.H.) and one artificial intelligence (AI) screener as per the Nussbaumer–Streit rapid review method (Garritty et al., 2024; Klerings et al., 2023; Nussbaumer-Streit et al., 2023). DistillerSR is an AI-enabled literature review platform which uses a logistic regression classifier that learns from manual screening (one of our authors) decisions by applying a supervised machine learning model. This approach has been shown to drastically decrease the number of reference which require manual screening while simultaneously ensuring appropriate papers are included (Hamel et al., 2020; Rogers et al., 2025). Conflicts were resolved by an additional human screener.
Data Extraction Procedures
A codebook was developed by two authors (A.K. and R.H.) to guide the extraction of data using REDCap. The codebook was piloted and refined before use. We extracted details related to the (a) authors and publication; (b) study rationale; (c) study population; (d) intervention conceptual framework, developer, and program scope and content; (e) feasibility/acceptability outcomes; and (f) intervention effectiveness. All data extraction was completed by a single reviewer (A.K. or R.H.) and checked for accuracy by a secondary reviewer (A.K. or R.H). Discrepancies were handled through arbitration with a third team member (L.J.).
Data Analysis and Synthesis
Data were synthesized using the research aims and the methods established in a scoping review of educational programs for adult cancer caregivers (Papadakos et al., 2022) as guides. Descriptive statistics were computed to report on the frequencies of study outcome categories and to provide an overall summary of the state of the literature. To describe the scope of educational programs, we deductively categorized reported educational program content using an adapted version of the Fitch and Steele Supportive Care Framework (Fitch, 2008). We made a series of changes to the framework to better reflect our findings, including changing the informational category to medical, removing the emotional category, and adding an “other” category.
Intervention feasibility/acceptability and effectiveness outcomes were summarized descriptively due to the heterogeneity of study findings. Feasibility and/or acceptability was classified as low, moderate, or high based on reporting in studies. In studies in which outcomes were quantified, this classification was determined by allocating scores into thirds designating them as “low” (bottom third), “moderate” (middle third), and “high” (top third). If feasibility/acceptability outcomes were not quantified and instead presented in a qualitative manner, the authors’ description of feasibility/acceptability was used to classify the result as feasible/acceptable or not.
Intervention effectiveness was defined as the reporting of an outcome with a positive impact on children, caregivers, or families. For an outcome to be classified as having a positive impact in this review, the original study authors needed to describe a beneficial change and whether or not it was statistically significant. Outcomes are presented in both tables and figures to highlight findings from individual studies as well as overall literature trends.
Results
The literature search identified 4,896 results. After excluding duplicates, 4,736 titles and abstracts were screened for inclusion. Full texts of 83 articles were screened, and 53 were excluded. Five additional texts were identified through hand-searching reference lists. Thirty-five articles, reporting on 32 unique studies, were included in the final analysis (Figure 1).
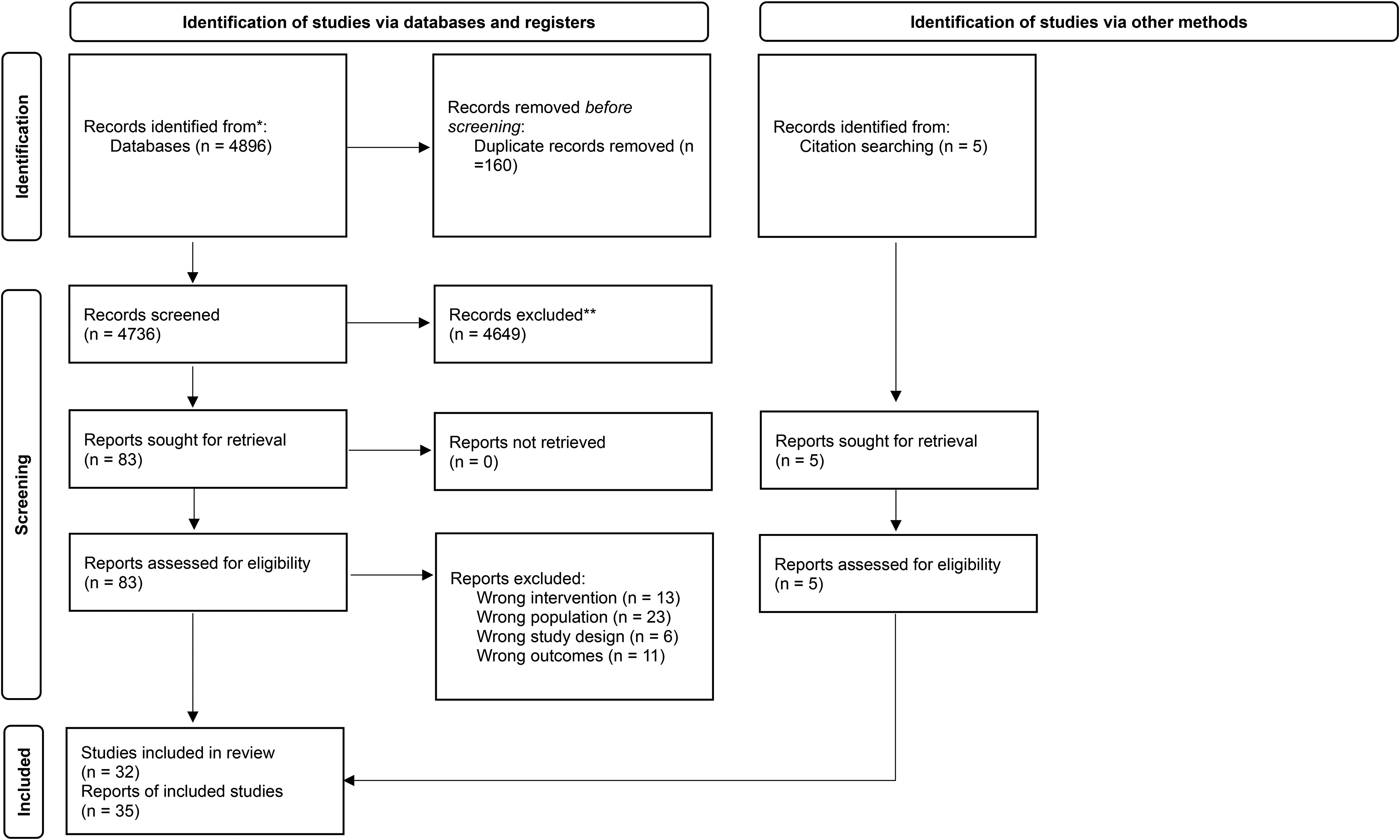
PRISMA 2020 Flow Diagram for New Systematic Reviews That Included Searches of Databases, Registers, and Other Sources.
Study Designs, Country of Conduct, and Sample Size
Table 1 presents the characteristics of included studies. Articles were published between 1999 and 2024. Most articles were published in 2023 (n = 6/35; 19%; Arpaci et al., 2023; Kilfoy et al., 2023; Landier, Gonzalez et al., 2023; Landier, York et al., 2023; Mehdizadeh et al., 2023; Ringnér et al., 2023), 2022 (n = 3/35; 9%; S. Y. Kim et al., 2022; Liu et al., 2022; Ryan et al., 2022), and 2020 (n = 3/35; 11%; Marsland et al., 2020; Meacham et al., 2020; Wilford et al., 2020). Nine of the 35 articles were classified by authors as randomized controlled trials (26%; Arpaci et al., 2023; Barrera, Atenafu, Schulte et al., 2018; Cernvall et al., 2017; Dijk-Lokkart et al., 2015; Hockenberry et al., 2021; Ozturk & Katikol, 2024; Ringnér et al., 2023; Sahler et al., 2005; Wu et al., 2014), eight as pilot studies (23%; Faith et al., 2024; Kazak et al., 1999; S. Y. Kim et al., 2022; Marsland et al., 2013, 2020; Ryan et al., 2022; Wang et al., 2016; Wilford et al., 2020), three as feasibility studies (9%; Ogez et al., 2019; Tan et al., 2024; Walsh et al., 2014), two as design and development studies (Bailie et al., 2021; Canter et al., 2019), two as qualitative studies (6%; Kilfoy et al., 2023; Nolbris & Ahlström, 2014), and two as usability studies (6%; Liu et al., 2022; Mehdizadeh et al., 2023). The remaining articles were classified as a development and pilot testing study (Donovan et al., 2019), a development and feasibility study (Salem et al., 2017), a user-centered iterative mixed-methods approach (Landier, Gonzalez et al., 2023), a prospective study (Meacham et al., 2020), a sequential two-cohort study design (Landier, York et al., 2023), a time-series design (Barrera et al., 2004), a exploratory study (Sigurdardottir et al., 2014), and a quasi-experimental pre and postdesign study (Wang et al., 2018; n = 1; 3% for each). The final article did not report on study design (n = 1; 3%; Slater et al., 2018).
Study Characteristics

Articles belonging to the same study grouping (32 studies from 35 articles) often examined the impact of the same intervention using different trial factors including different populations (caregivers vs. siblings; Barrera, Atenafu, Sung et al., 2018; Barrera et al., 2004) using different study designs (pilot RCT vs. a parallel pilot RCT; Marsland et al., 2013, 2020) or targeting different outcomes (experience vs. effectiveness; Wang et al., 2016, 2018).
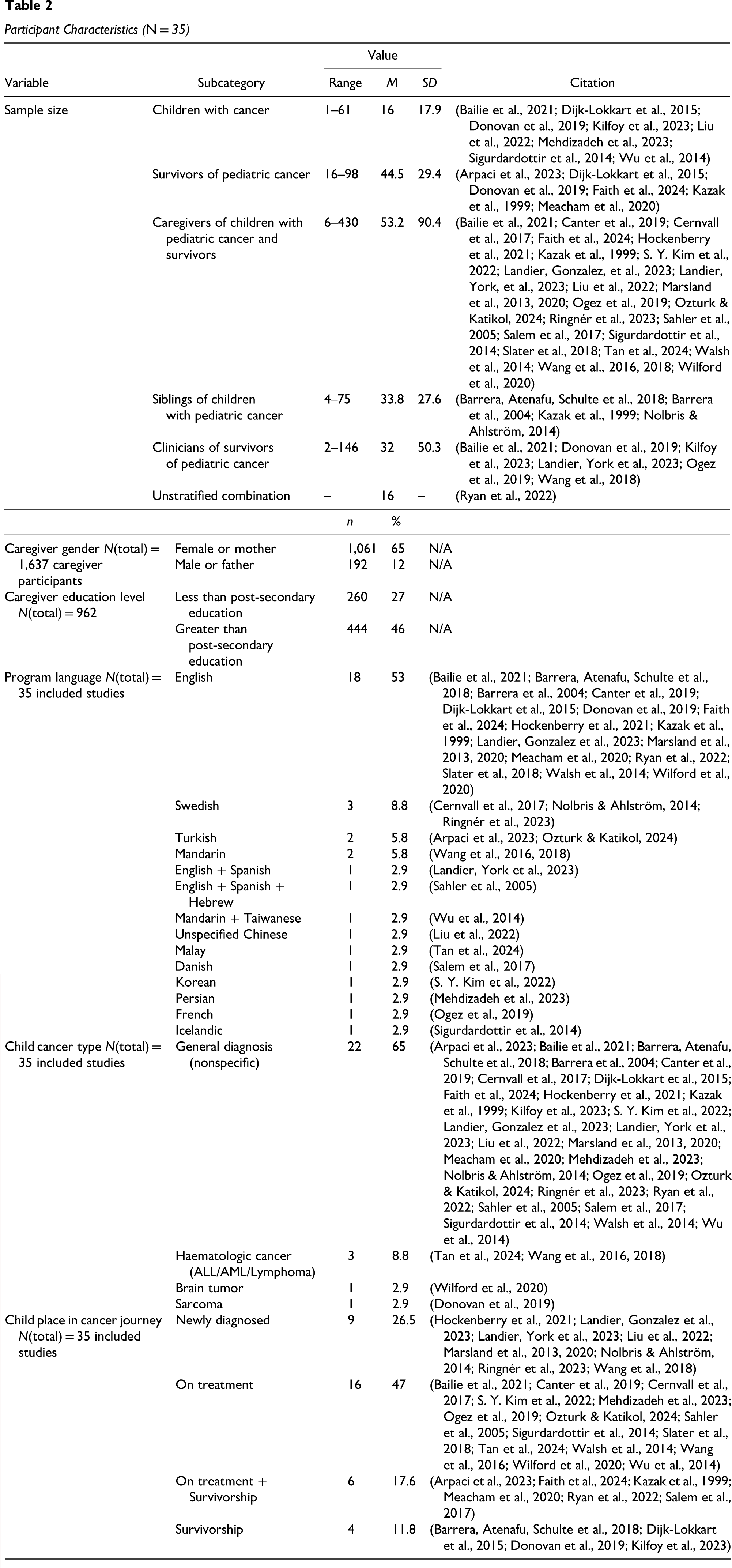
Articles were most frequently published in the United States (n = 10/35; 29%; Canter et al., 2019; Donovan et al., 2019; Faith et al., 2024; Kazak et al., 1999; Landier, Gonzalez et al., 2023; Marsland et al., 2013, 2020; Meacham et al., 2020; Walsh et al., 2014; Wilford et al., 2020), Canada (n = 6/35; 17%; Bailie et al., 2021; Barrera et al., 2004; Barrera, Atenafu, Schulte et al., 2018; Kilfoy et al., 2023; Ogez et al., 2019; Ryan et al., 2022), Sweden (n = 3/35; 9%; Cernvall et al., 2017; Nolbris & Ahlström, 2014; Ringnér et al., 2023), and Turkey (n = 2/35; 6%; Arpaci et al., 2023; Ozturk & Katikol, 2024). Six articles were published by groups from across more than one country (n = 6/35; 17%; Hockenberry et al., 2021; Landier, York et al., 2023; Sahler et al., 2005; Salem et al., 2017; Wang et al., 2016, 2018). All articles (100%) reported on the sample size. As shown in Table 2, on average, 64 participants were included in studies. The article with the smallest sample enrolled 9 parents (Canter et al., 2019), and the article with the largest sample enrolled 430 mothers (Sahler et al., 2005).
Participant Characteristics (N = 35)
Study Participants
Most articles (n = 30/35; 86%) reported information about the child's age (Arpaci et al., 2023; Bailie et al., 2021; Barrera et al., 2004; Barrera, Atenafu, Schulte et al., 2018; Canter et al., 2019; Cernvall et al., 2017; Dijk-Lokkart et al., 2015; Donovan et al., 2019; Faith et al., 2024; Hockenberry et al., 2021; Kazak et al., 1999; Kilfoy et al., 2023; S. Y. Kim et al., 2022; Landier, York et al., 2023; Liu et al., 2022; Marsland et al., 2013; Meacham et al., 2020; Mehdizadeh et al., 2023; Nolbris & Ahlström, 2014; Ozturk & Katikol, 2024; Ringnér et al., 2023; Sahler et al., 2005; Salem et al., 2017; Sigurdardottir et al., 2014; Tan et al., 2024; Walsh et al., 2014; Wang et al., 2016, 2018; Wilford et al., 2020; Wu et al., 2014), regardless of whether the education was targeted at the patient or a caregiver, whereas just over half (n = 18/35; 51%) described caregiver age (Barrera, Atenafu, Schulte et al., 2018; Canter et al., 2019; Cernvall et al., 2017; Landier, Gonzalez et al., 2023; Landier, York et al., 2023; Marsland et al., 2013, 2020; Mehdizadeh et al., 2023; Ogez et al., 2019; Ozturk & Katikol, 2024; Ringnér et al., 2023; Sahler et al., 2005; Salem et al., 2017; Sigurdardottir et al., 2014; Tan et al., 2024; Wang et al., 2016, 2018; Wilford et al., 2020). When reported, most caregivers were described as female or a mother (n = 1061/1637; 65%). Information describing participant race or ethnicity was limited, with 23% of 35 studies providing data for the child (Barrera et al., 2004; Canter et al., 2019; Donovan et al., 2019; Faith et al., 2024; Hockenberry et al., 2021; Kilfoy et al., 2023; Landier, York et al., 2023; Meacham et al., 2020) and 23% of 35 studies reporting data for the caregiver (Canter et al., 2019; Landier, Gonzalez et al., 2023; Marsland et al., 2013, 2020; Sahler et al., 2005; Tan et al., 2024; Wang et al., 2018; Wilford et al., 2020), and 3% of 35 studies reporting data for the family (Kazak et al., 1999). Of the eight studies reporting caregiver race, five (63%) reported a Caucasian majority within their sample, with the remaining three having a significant Han population (Wang et al., 2018), Malay population (Tan et al., 2024), and Hispanic population (Wilford et al., 2020). Eight studies reported child race (Barrera et al., 2004; Canter et al., 2019; Donovan et al., 2019; Faith et al., 2024; Hockenberry et al., 2021; Kilfoy et al., 2023; Landier, York et al., 2023; Meacham et al., 2020), with all reporting a Caucasian majority sample.
Approximately one-third of articles (n = 10/35; 29%) reported any indication of family income (Arpaci et al., 2023; Barrera, Atenafu, Schulte et al., 2018; Barrera et al., 2004; Landier, Gonzalez et al., 2023; Marsland et al., 2020; Ozturk & Katikol, 2024; Sigurdardottir et al., 2014; Tan et al., 2024; Wang et al., 2016, 2018), and those that did provided data in a variety of measures (e.g., annual income in local currency, spending power). The education level of caregivers was described in nearly half the articles (Arpaci et al., 2023; Barrera, Atenafu, Schulte et al., 2018; Cernvall et al., 2017; Landier, Gonzalez et al., 2023; Landier, York et al., 2023; Marsland et al., 2013, 2020; Mehdizadeh et al., 2023; Ozturk & Katikol, 2024; Sahler et al., 2005; Salem et al., 2017; Sigurdardottir et al., 2014; Tan et al., 2024; Wang et al., 2016, 2018; Wilford et al., 2020; n = 17/35; 49%). Most of these (n = 15/17; 88%) provided categorical data related to the level of schooling acquired by the participant (Arpaci et al., 2023; Cernvall et al., 2017; Landier, Gonzalez et al., 2023; Landier, York et al., 2023; Marsland et al., 2013; Mehdizadeh et al., 2023; Ozturk & Katikol, 2024; Ringnér et al., 2023; Sahler et al., 2005; Salem et al., 2017; Sigurdardottir et al., 2014; Tan et al., 2024; Wang et al., 2016, 2018; Wilford et al., 2020), while the remaining articles (2/17 = 12%) reported years of education (Barrera, Atenafu, Schulte et al., 2018; Marsland et al., 2020). Of caregivers with reported education level (n = 962), 46% had at least a high school education (n = 444).
Educational Intervention Characteristics
Educational interventions were delivered as self-guided resources (workbook, mobile app, website; 12/35 = 31%; Donovan et al., 2019; Landier, Gonzalez et al., 2023; Liu et al., 2022; Mehdizadeh et al., 2023; Ryan et al., 2022; Sigurdardottir et al., 2014; Slater et al., 2018; Tan et al., 2024; Walsh et al., 2014; Wang et al., 2016, 2018; Wu et al., 2014), or by nurses (6/35 = 17%; Arpaci et al., 2023; Bailie et al., 2021; Hockenberry et al., 2021; Nolbris & Ahlström, 2014; Ringnér et al., 2023; Zupanec et al., 2024), psychologists (6/35 = 17%; Barrera, Atenafu, Schulte et al., 2018; Barrera et al., 2004; Cernvall et al., 2017; Dijk-Lokkart et al., 2015; Faith et al., 2024; Salem et al., 2017), clinicians (3/35 = 9%; Marsland et al., 2013, 2020; Ogez et al., 2019), child life specialists (2/35 = 6%; Kilfoy et al., 2023; S. Y. Kim et al., 2022), research staff (2/35 = 6%; Ozturk & Katikol, 2024; Wilford et al., 2020), interventionists (2/35 = 6%; Kazak et al., 1999; Sahler et al., 2005), therapists (1/35 = 3%; Canter et al., 2019), and endocrinologists (1/35 = 3%; Meacham et al., 2020). Interventions offered an average of 6.9 sessions (1–12), and when reported, lasted 8 min (brief interaction with a mobile app; Wang et al., 2016) to 4 h in length (in-person community support for children and caregivers; Wilford et al., 2020). Interventions were delivered in as little as one day (all-day workshop; Kazak et al., 1999; Meacham et al., 2020), and as long as 8 months (virtual support group; Kilfoy et al., 2023).
Intervention content was informed by conceptual frameworks in 19/32 (59%) instances (Arpaci et al., 2023; Barrera et al., 2004; Cernvall et al., 2017; Donovan et al., 2019; Faith et al., 2024; Kazak et al., 1999; Landier, York et al., 2023; Liu et al., 2022; Meacham et al., 2020; Ogez et al., 2019; Ozturk & Katikol, 2024; Ringnér et al., 2023; Ryan et al., 2022; Sahler et al., 2005; Salem et al., 2017; Sigurdardottir et al., 2014; Wang et al., 2018; Wilford et al., 2020; Wu et al., 2014). Interventions targeted education at parents or caregivers of children or adolescents with cancer (n = 12; Canter et al., 2019; Cernvall et al., 2017; Hockenberry et al., 2021; S. Y. Kim et al., 2022; Landier, Gonzalez et al., 2023; Landier, York et al., 2023; Marsland et al., 2013; Ringnér et al., 2023; Sigurdardottir et al., 2014; Walsh et al., 2014; Wang et al., 2016, 2018), children with cancer and their parents (n = 6; Liu et al., 2022; Mehdizadeh et al., 2023; Salem et al., 2017; Slater et al., 2018; Tan et al., 2024; Wilford et al., 2020), adolescent and young adult survivors of childhood cancer (n = 3; Arpaci et al., 2023; Faith et al., 2024; Meacham et al., 2020), mothers only (n = 3; Marsland et al., 2020; Ozturk & Katikol, 2024; Sahler et al., 2005), and siblings of children with cancer (n = 3; Barrera, Atenafu, Schulte et al., 2018; Barrera et al., 2004; Nolbris & Ahlström, 2014). The remaining studies targeted parents/caregivers and health care professionals (n = 2; Bailie et al., 2021; Ogez et al., 2019), adolescents with cancer (n = 2; Donovan et al., 2019; Kilfoy et al., 2023), children with childhood cancer (n = 2; Dijk-Lokkart et al., 2015; Wu et al., 2014) adolescent survivors of childhood cancer and their families (n = 1; Kazak et al., 1999), and survivors of childhood cancer (n = 1; Ryan et al., 2022). No studies targeted bereaved caregivers or family members or patients at end of life.
Interventions were most frequently delivered remotely (n = 16; Arpaci et al., 2023; Canter et al., 2019; Cernvall et al., 2017; Donovan et al., 2019; Faith et al., 2024; Kilfoy et al., 2023; Landier, Gonzalez et al., 2023; Liu et al., 2022; Mehdizadeh et al., 2023; Ringnér et al., 2023; Ryan et al., 2022; Sigurdardottir et al., 2014; Slater et al., 2018; Wang et al., 2016, 2018; Wu et al., 2014) followed by in-person (in a clinical setting or at home; n = 10; Barrera et al., 2004; Barrera, Atenafu, Schulte et al., 2018; Dijk-Lokkart et al., 2015; Kazak et al., 1999; S. Y. Kim et al., 2022; Meacham et al., 2020; Ogez et al., 2019; Sahler et al., 2005; Salem et al., 2017; Tan et al., 2024) or as a hybrid of the two modalities (n = 9; Bailie et al., 2021; Hockenberry et al., 2021; Landier, York et al., 2023; Marsland et al., 2013, 2020; Nolbris & Ahlström, 2014; Ozturk & Katikol, 2024; Walsh et al., 2014; Wilford et al., 2020). All but one remote intervention (Ryan et al., 2022) were delivered using digital means including mobile applications (n = 4; Landier, Gonzalez et al., 2023; Mehdizadeh et al., 2023; Ringnér et al., 2023; Slater et al., 2018) or websites (n = 3; Cernvall et al., 2017; Sigurdardottir et al., 2014; Wu et al., 2014). Five of the remote interventions used multiple digital means to deliver interventions to parents. Most interventions were only offered in one language (29/32 = 91%), with two interventions offered in two languages (English and Spanish; Taiwanese and Mandarin; 2/32 = 6%; Landier, York et al., 2023; Wu et al., 2014), and one intervention offered in three languages (English, Spanish, and Hebrew; 1/32 = 3%; Sahler et al., 2005).
Intervention Educational Domains
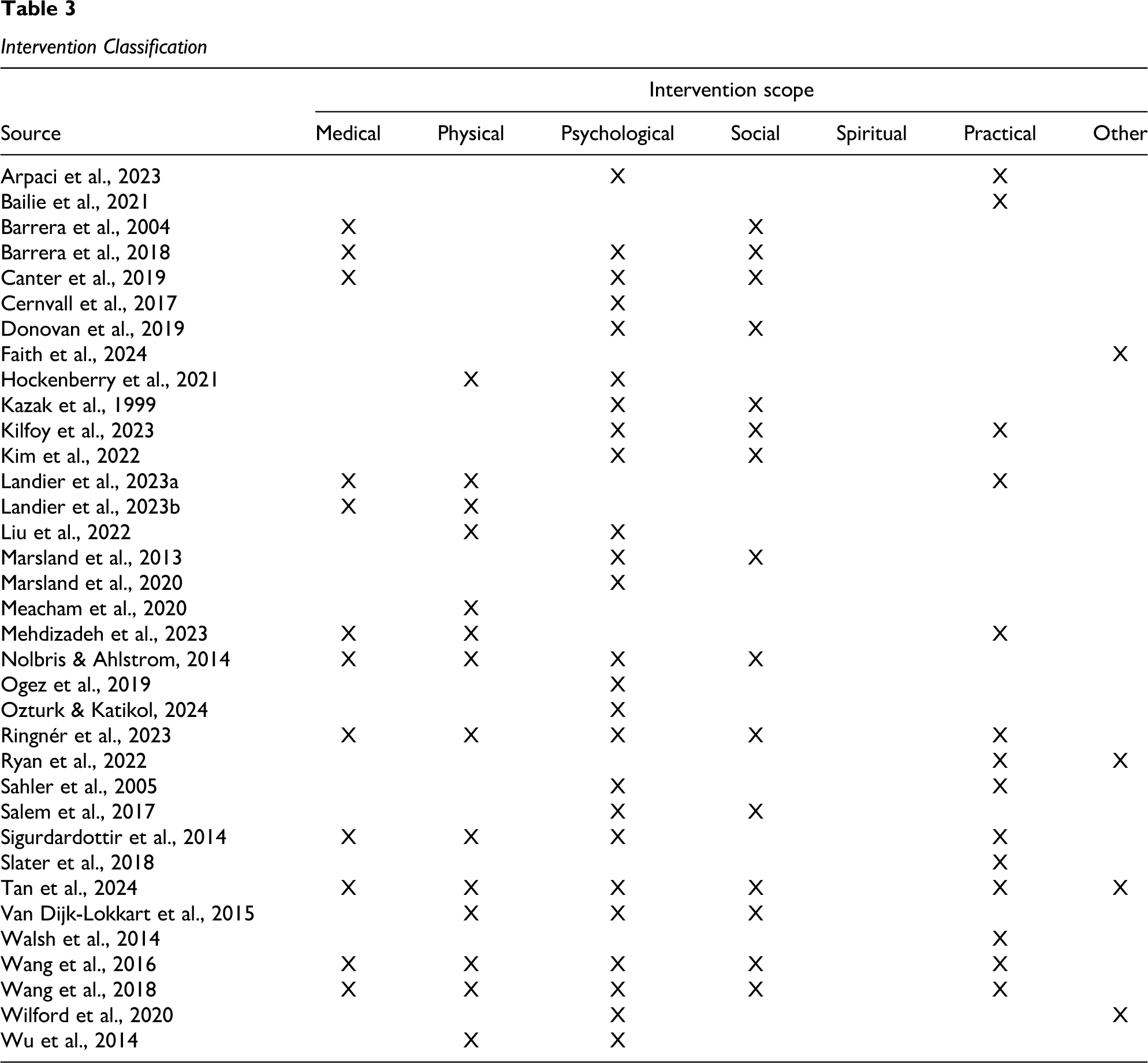
Table 3 outlines the Fitch and Steel Supportive Care Framework-associated educational domains identified in each study intervention. Most papers reported on interventions that integrated two or more elements from the Framework (n = 25/35; 71%; Arpaci et al., 2023; Barrera et al., 2004; Barrera, Atenafu, Schulte et al., 2018; Canter et al., 2019; Dijk-Lokkart et al., 2015; Donovan et al., 2019; Hockenberry et al., 2021; Kazak et al., 1999; Kilfoy et al., 2023; S. Y. Kim et al., 2022; Landier, Gonzalez et al., 2023; Landier, York et al., 2023; Liu et al., 2022; Marsland et al., 2013; Mehdizadeh et al., 2023; Nolbris & Ahlström, 2014; Ringnér et al., 2023; Sahler et al., 2005; Salem et al., 2017; Sigurdardottir et al., 2014; Tan et al., 2024; Wang et al., 2016, 2018; Wilford et al., 2020; Wu et al., 2014), with the range of included domains being one to six. Most interventions addressed the psychological domain (n = 25/35; 71%; Arpaci et al., 2023; Barrera, Atenafu, Schulte et al., 2018; Canter et al., 2019; Cernvall et al., 2017; Dijk-Lokkart et al., 2015; Donovan et al., 2019; Hockenberry et al., 2021; Kazak et al., 1999; Kilfoy et al., 2023; S. Y. Kim et al., 2022; Liu et al., 2022; Marsland et al., 2013, 2020; Nolbris & Ahlström, 2014; Ogez et al., 2019; Ozturk & Katikol, 2024; Ringnér et al., 2023; Sahler et al., 2005; Salem et al., 2017; Sigurdardottir et al., 2014; Tan et al., 2024; Wang et al., 2016, 2018; Wilford et al., 2020; Wu et al., 2014), including education on coping strategies, relaxation techniques, or problem-solving approaches. The second most integrated domain was social (n = 15/35; 43%; Barrera et al., 2004; Barrera, Atenafu, Schulte et al., 2018; Canter et al., 2019; Dijk-Lokkart et al., 2015; Donovan et al., 2019; Kazak et al., 1999; Kilfoy et al., 2023; S. Y. Kim et al., 2022; Marsland et al., 2013; Nolbris & Ahlström, 2014; Ringnér et al., 2023; Salem et al., 2017; Tan et al., 2024; Wang et al., 2016, 2018), which included education pertaining to navigating relationships with parents, spouses, other children, and school or employment issues. The Framework's physical domain of support was addressed in 14/25 studies (40%; Dijk-Lokkart et al., 2015; Hockenberry et al., 2021; Landier, Gonzalez et al., 2023; Landier, York et al., 2023; Liu et al., 2022; Meacham et al., 2020; Mehdizadeh et al., 2023; Nolbris & Ahlström, 2014; Ringnér et al., 2023; Sigurdardottir et al., 2014; Tan et al., 2024; Wang et al., 2016, 2018; Wu et al., 2014) and involved education on symptom management support strategies. The practical domain was included in 14/35 interventions (40%; Arpaci et al., 2023; Bailie et al., 2021; Kilfoy et al., 2023; Landier, York et al., 2023; Mehdizadeh et al., 2023; Ringnér et al., 2023; Ryan et al., 2022; Sahler et al., 2005; Sigurdardottir et al., 2014; Slater et al., 2018; Tan et al., 2024; Walsh et al., 2014; Wang et al., 2016, 2018) and the medical domain in 12/35 (34%; Barrera, Atenafu, Schulte et al., 2018; Barrera et al., 2004; Canter et al., 2019; Landier, Gonzalez et al., 2023; Landier, York et al., 2023; Mehdizadeh et al., 2023; Nolbris & Ahlström, 2014; Ringnér et al., 2023; Sigurdardottir et al., 2014; Tan et al., 2024; Wang et al., 2016, 2018). These included education related to chemotherapy administration information and cancer biology, classifications, or treatment, respectively. Four studies included educational foci outside of the six domains of the Framework, with topics including transitioning to adult care (Ryan et al., 2022), healthy lifestyle choices (Ryan et al., 2022; Wilford et al., 2020), and assessing trustworthiness of information (Tan et al., 2024). Notably, no studied interventions addressed the Framework's spiritual domain.
Intervention Classification
Feasibility Acceptability of Educational Interventions
Overall, the interventions and their evaluations were reported to have a high degree of feasibility/acceptability, though varying definitions of feasibility and/or acceptability-related constructs such as acceptability or usability were used. As seen in Table 4, 98 feasibility and/or acceptability-related outcomes were measured across the 35 identified articles. Of the 98, 82 (84%) were classified as demonstrating high feasibility/acceptability, 15 (15%) as demonstrating moderate feasibility/acceptability, and one (1%) as demonstrating low feasibility/acceptability. The only outcome indicating low study feasibility/acceptability was reported by Ringner et al. (2023) and pertained to a poor accrual rate for parents (i.e., 20% of those eligible parents were recruited; Ringnér et al., 2023).
Study and Intervention Feasibility

Note. Feasibility is classified as low, moderate, or high based on study reports. In studies in which outcomes were quantified, this classification was determined by allocating scores into thirds, designating them as “low” (bottom third), “moderate” (middle third), and “high” (top third). If feasibility outcomes were not quantified and instead presented in a qualitative manner, the authors’ description of feasibility was used to classify the result as feasible or not.
The most frequently assessed feasibility/acceptability outcome was satisfaction, measured in 30 of the 35 articles (86%). Of these 30 articles, a variety of satisfaction measurement tools were used and included the Sibling Group Satisfaction Questionnaire (n = 1; Barrera et al., 2004), the Mobile Application Rating Scale (n = 1; Landier, Gonzalez et al., 2023), qualitative interviews (n = 4; Bailie et al., 2021; Kilfoy et al., 2023; Landier, Gonzalez et al., 2023; Slater et al., 2018), open-ended surveys or questions (n = 4; S. Y. Kim et al., 2022; Marsland et al., 2013; Meacham et al., 2020; Wang et al., 2018), Client Satisfaction Questionnaire (n = 2; Marsland et al., 2013, 2020), and research-team generated scales (n = 10; Dijk-Lokkart et al., 2015; Hockenberry et al., 2021; Kazak et al., 1999; Landier, York et al., 2023; Ogez et al., 2019; Salem et al., 2017; Sigurdardottir et al., 2014; Walsh et al., 2014; Wilford et al., 2020; Wu et al., 2014). All these studies reported a high-level of satisfaction, except one (Marsland et al., 2020), which showed end-user satisfaction to be moderate. Other frequently assessed feasibility/acceptability outcomes were intervention attendance or adherence (n = 12; Barrera, Atenafu, Schulte et al., 2018; Canter et al., 2019; Cernvall et al., 2017; Donovan et al., 2019; Hockenberry et al., 2021; Marsland et al., 2013, 2020; Ozturk & Katikol, 2024; Salem et al., 2017; Slater et al., 2018; Walsh et al., 2014; Wilford et al., 2020), study recruitment (n = 9; Kilfoy et al., 2023; Landier, York et al., 2023; Marsland et al., 2013, 2020; Nolbris & Ahlström, 2014; Ringnér et al., 2023; Salem et al., 2017; Sigurdardottir et al., 2014; Tan et al., 2024), attrition (n = 5; Cernvall et al., 2017; Dijk-Lokkart et al., 2015; Sahler et al., 2005; Salem et al., 2017; Wang et al., 2018), and retention (n = 2; Barrera, Atenafu, Schulte et al., 2018; Salem et al., 2017), as well as intervention usability (n = 4; Canter et al., 2019; Landier, Gonzalez et al., 2023; Liu et al., 2022; Wilford et al., 2020). Table 4 shows feasibility and/or acceptability outcome-related findings.
Effectiveness of Educational Interventions
As shown in Table 5, 24 of the 35 articles (69%) explored educational intervention effectiveness. All except one (Donnovan et al., 2019) article (23/24; 96%) demonstrated a positive impact on at least one participant-level outcome. Commonly assessed outcomes were anxiety (measured in 35 instances across 12 articles; Barrera et al., 2004; Barrera, Atenafu, Schulte et al., 2018; Cernvall et al., 2017; Kazak et al., 1999; S. Y. Kim et al., 2022; Marsland et al., 2013, 2020; Ozturk & Katikol, 2024; Ringnér et al., 2023; Wang et al., 2016, 2018; Wilford et al., 2020), depression (nine instances across nine articles; Barrera et al., 2004; Cernvall et al., 2017; S. Y. Kim et al., 2022; Marsland et al., 2013, 2020; Ringnér et al., 2023; Sahler et al., 2005; Wang et al., 2018; Wilford et al., 2020), stress-related outcomes (28 instances across nine articles; Cernvall et al., 2017; Kazak et al., 1999; S. Y. Kim et al., 2022; Marsland et al., 2013, 2020; Ozturk & Katikol, 2024; Ringnér et al., 2023; Sahler et al., 2005; Wang et al., 2016), knowledge (11 instances across five articles; Meacham et al., 2020; Nolbris & Ahlström, 2014; Ringnér et al., 2023; Wang et al., 2016, 2018), and quality of life (13 instances across four studies; Arpaci et al., 2023; S. Y. Kim et al., 2022; Sigurdardottir et al., 2014; Wilford et al., 2020). Positive participant impacts were noted in a high percentage of each of these outcomes: anxiety (24/35; 69%), depression (6/9; 67%), stress-related outcomes (22/28; 79%), knowledge (6/11; 55%), and quality of life (5/13; 39%).
Effectiveness Outcomes
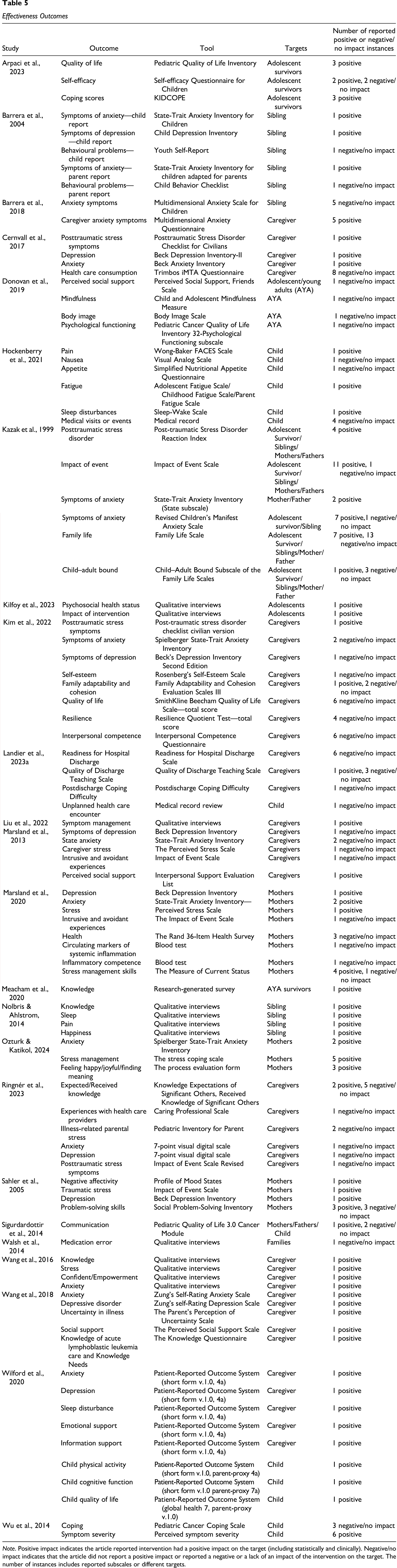
Note. Positive impact indicates the article reported intervention had a positive impact on the target (including statistically and clinically). Negative/no impact indicates that the article did not report a positive impact or reported a negative or a lack of an impact of the intervention on the target. The number of instances includes reported subscales or different targets.
The methods to assess effectiveness outcomes ranged widely across articles, with 19/24 (79%) using quantitative measures and the remaining five (21%) using qualitative interviews. The most commonly used quantitative tools for parents were the State-Trait Anxiety Inventory (n = 6 articles; Barrera et al., 2004; Kazak et al., 1999; S. Y. Kim et al., 2022; Marsland et al., 2013, 2020; Ozturk & Katikol, 2024), the Beck Depression Inventory (n = 5 articles; Cernvall et al., 2017; S. Y. Kim et al., 2022; Marsland et al., 2013, 2020; Sahler et al., 2005), and the Impact of Event Scale (n = 5 articles; Kazak et al., 1999; Marsland et al., 2013, 2020; Ringnér et al., 2023; Sahler et al., 2005). A quantitative tool for children (patients or survivors) was only used once in more than two articles. This tool was the Pediatric Quality of Life Inventory (n = 2 articles; Arpaci et al., 2023; Sigurdardottir et al., 2014). Post-intervention effectiveness was measured once in 13/24 (54%) articles, with longitudinal follow-up assessments conducted in 11/24 (46%).
Discussion
We aimed to synthesize and characterize the content, function, feasibility, acceptability, and effectiveness of health care provider-delivered educational interventions for children with cancer and their families. Our findings highlight several key insights about the current state of the literature in this area, as well as important gaps and opportunities for future research and intervention development.
Breadth and Focus of Educational Interventions
The 35 included articles described a wide range of educational interventions targeting different family members (e.g., parents, siblings, survivors) and cancer stages using various delivery methods. Notably, many studies enrolled mothers, reflecting caregiving roles that often fall disproportionately on women (Y. Kim et al., 2019). While this focus is practical, the underrepresentation of fathers, siblings, and extended caregivers in both intervention targeting and reporting limits understanding of whether and how these interventions may benefit these groups. Future work should consider family systems approaches and the needs of diverse caregiver configurations (Kazak et al., 2018; Porter et al., 2019).
Educational content most frequently addressed family psychological and social needs, including training on coping strategies, communication, and relationship management. Fewer interventions addressed the physical or medical domains of supportive care in childhood cancer, such as symptom management or direct care-focused education, and only a small proportion addressed practical concerns such as family finances or transitions in care. Given shifts in pediatric oncology care toward a more outpatient-based model with increasingly complex treatments delivered with family support outside the hospital, provision of high-quality education focused on domains such as symptom management or direct care is critical for safe care. Future research, therefore, should focus on the development and evaluation of these types of educational interventions and with careful consideration of the selected outcomes.
Additionally, no intervention explicitly addressed spiritual concerns, despite evidence suggesting that spirituality can be a source of support and meaning-making for many families facing pediatric cancer and the lack of such support may limit coping (Grossoehme et al., 2020; Robert et al., 2019). This suggests an opportunity to design more holistic interventions that align with the full spectrum of supportive care needs described by Fitch and Steele's Framework.
Intervention Feasibility and Implementation Potential
Most studies reported high feasibility/acceptability across a range of metrics—including satisfaction, recruitment, adherence, and usability—underscoring the potential for real-world implementation. Satisfaction, in particular, was the most assessed outcome and overwhelmingly rated highly, suggesting that both caregivers and children are receptive to educational interventions when well-designed, deemed relevant, and delivered appropriately. Nonetheless, feasibility/acceptability studies often lacked standardization in how these outcomes were measured, with many relying on author-generated tools and with constructs operationalized using different definitions across studies. Standardizing metrics to evaluate educational intervention feasibility/acceptability in future research could help improve comparability across studies and streamline a path toward large-scale implementation across centers (Beets et al., 2021; Richesson et al., 2020).
Considering education delivery modality, over half of the identified interventions were administered remotely, usually as mobile applications or websites. This finding aligns with a broader shift in health care toward digital and hybrid delivery models (Kickbusch et al., 2021) and one cited as of value by busy families of children with cancer and their nurses (Jibb et al., 2024; Zupanec et al., 2024). However, few studies reported detailed demographic information on participants’ socioeconomic status, digital literacy, or access to technology, all of which could impact the effectiveness and equity of remote education. Addressing these digital divides is critical to ensuring that educational supports are not only scalable, but also equitable.
Intervention Effectiveness
Nearly 70% of included studies evaluated some aspect of educational intervention effectiveness, and among these, the majority reported positive impacts on at least one participant-level outcome. Evaluated outcomes included anxiety, depression, stress, and cancer-related knowledge—consistent with prior literature identifying these as key areas of need among pediatric oncology families (Aldiss et al., 2023; Gibson et al., 2021). Outcome measurement approaches, however, were heterogeneous and often lacked longitudinal follow-up, limiting conclusions about sustained impact or comparative effectiveness across interventions. Notably, studies that did measure knowledge reported universally positive gains, suggesting that educational interventions can effectively improve caregiver understanding and confidence—a key goal of supportive cancer care (Chow et al., 2023; Rothausen et al., 2025).
The absence of theoretical grounding in many studies is a critical gap. Only a minority reported using conceptual frameworks to guide intervention development. Incorporating theory—such as self-efficacy theory, the transactional model of stress and coping, or implementation science frameworks into educational interventions and their evaluations could enhance rigor, replicability, interpretability, and impact (Damschroder et al., 2022; Xie et al., 2025).
Limitations of the Literature and the Current Review
The existing literature related to health care provider-delivered educational interventions for children with cancer and their families remains fragmented in terms of population, content, outcomes, and methods. Demographic data, particularly related to key characteristics that may impact education utility, such as participant education, rurality, and gender diversity, were inconsistently reported. This limits our understanding of intervention reach and effectiveness in diverse populations, and may perpetuate health inequities. Only a minority of studies examined siblings or addressed the needs of survivors, and none explicitly discussed interventions tailored to culturally and linguistically diverse groups, despite their well-documented unique needs in pediatric oncology (Robles et al., 2024).
Limitations of this review include those inherent to rapid scoping methods. While our review was guided by rigorous scoping review methodology, the use of AI-assisted screening and a single screener per article may have increased the risk of missing eligible studies. However, our piloted search strategy and duplicate verification processes were designed to mitigate these risks. In addition, the year restriction in our search strategy limits the number of interventions we identified. Given the rapidly changing landscape of pediatric cancer treatment, this approach ensured we identified the most relevant and recent interventions.
Implications for Practice and Future Research
This review demonstrated that educational interventions in pediatric oncology are both feasible/acceptable to implement or study and potentially effective, especially for improving caregiver psychological well-being and knowledge. The prominence of digital delivery modes presents a scalable opportunity but also underscores the importance of digital equity and infrastructure. To advance the field of pediatric cancer-focused educational interventions, we propose the following priorities: (a) Interventions should be informed by behavioral theory and co-developed in collaboration with end users to enhance relevance, uptake, and sustainability (Kilfoy et al., 2024); (b) research should prioritize inclusive recruitment strategies including bereaved caregivers and families, and children at the end of life, detailed demographic reporting, and adaptation for diverse linguistic and cultural contexts; (c) robust, longer-term trials are needed to understand the sustained impact and comparative effectiveness of different educational modalities and contents; and (d) consensus on feasibility/acceptability outcomes and measurement tools is required to improve cross-study synthesis and implementation planning.
Conclusion
Educational interventions delivered by health care providers in pediatric oncology show strong potential to support families during the challenges of treatment and survivorship. Identified interventions appear feasible and/or acceptable and are well-received by children and caregivers, with initial evidence suggesting benefits for psychological well-being and knowledge. However, more rigorous, inclusive, patient and family-driven, and theoretically informed research is essential to optimize the impact of these interventions and ensure they meet the complex, evolving needs of all children with cancer and their families.
Supplemental Material
sj-pdf-1-jpo-10.1177_27527530261424175 - Supplemental material for Health Care Provider–Delivered Educational Interventions in Pediatric Oncology: A Rapid Scoping Review of Content, Feasibility, Acceptability, and Effectiveness
Supplemental material, sj-pdf-1-jpo-10.1177_27527530261424175 for Health Care Provider–Delivered Educational Interventions in Pediatric Oncology: A Rapid Scoping Review of Content, Feasibility, Acceptability, and Effectiveness by Alicia Kilfoy, Rachel Hamilton, Melissa Howlett, Benita Yi, Sue Zupanec and Lindsay Jibb in Journal of Pediatric Hematology/Oncology Nursing
Supplemental Material
sj-docx-2-jpo-10.1177_27527530261424175 - Supplemental material for Health Care Provider–Delivered Educational Interventions in Pediatric Oncology: A Rapid Scoping Review of Content, Feasibility, Acceptability, and Effectiveness
Supplemental material, sj-docx-2-jpo-10.1177_27527530261424175 for Health Care Provider–Delivered Educational Interventions in Pediatric Oncology: A Rapid Scoping Review of Content, Feasibility, Acceptability, and Effectiveness by Alicia Kilfoy, Rachel Hamilton, Melissa Howlett, Benita Yi, Sue Zupanec and Lindsay Jibb in Journal of Pediatric Hematology/Oncology Nursing
Footnotes
Ethical Approval
Ethics approval was not needed for this review.
Author Contributions
All authors contributed to the study conception and design. Literature search and data analysis were completed by Rachel Hamilton, Alicia Kilfoy, and Lindsay Jibb. The first draft of the manuscript was written by Alicia Kilfoy, Lindsay Jibb, and Rachel Hamilton, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.