
Abstract
Background
Drugs that target the mitogen-activated protein kinase pathway have caused frequent and significant skin toxicity, which has led to increased burden on both patients and their caregivers. Routine skin care products for daily use have been shown to improve skin toxicity. If a patient is provided with basic skin care products for daily use this could facilitate skin management while on these medications.
Method
Participants 0–21 years old who were treated with any medication targeting the mitogen-activated protein kinase (MAPK) pathway were eligible for this prospective, single-site study. Each participant received a complimentary skin care kit consisting of skin, hair, and oral care items. The utilization of these skin care kits was evaluated and participant satisfaction with the items was measured. Secondarily, the participants’ quality of life (QOL) was assessed and the participants’ adherence to their MAPK inhibitor was evaluated.
Results
Seventeen participants (10 male, 7 female) with a median age of 10.5 years were enrolled. Forty-seven percent of participants rated their satisfaction with the kit as excellent, and no patient rated it as poor. Seventy-seven percent of participants rated the kit helpful, and the majority (76.5%) thought the kits should be distributed before the initiation of therapy. QOL changes were not statistically significant.
Conclusions
Participants on MAPK inhibitors who received skin care kits were satisfied with the kits’ ability to help with their skin side effects. Given the high satisfaction and acceptability, future studies should evaluate the effect of these kits on QOL with adequate power to detect improvements.
Background
The mitogen-activated protein kinase (MAPK) pathway is integral to the regulation of cellular activities including cell proliferation, survival, differentiation, and motility and was found to be dysregulated in approximately one-third of all malignancies (Cheng & Tian, 2017). In pediatrics, MAPK inhibitors have been incorporated into treatment plans for several diseases, including brain tumors, plexiform neurofibromas, and histiocytosis.
Drugs targeting the MAPK pathway such as B-Rapidly Accelerated Fibrosarcoma (BRAF), MEK (mitogen-activated extracellular signal-regulated kinase), pan-RAF (Rapidly Accelerated Fibrosarcoma), and ERK (extracellular signal-regulated kinase) inhibitors have provided innovative treatment options. They have commonly triggered side effects involving the skin, mouth, hair and nails. Prior studies demonstrated that 80%–100% of participants who received these drugs exhibited at least one dermatologic side effect (Song et al., 2019). The most frequent included photosensitivity, alopecia, keratosis pilaris-like eruption, acneiform eruptions, mouth ulcers, angular cheilitis, and eczematous eruptions (Klesse et al., 2020; Boull et al., 2021). These dermatologic side effects have caused significant discomfort and/or changes to the patient's physical appearance and sometimes required dose reductions or cessation of the patient's MAPK inhibitor (Lacouture et al., 2011). Additionally, these side effects could lead to undue stress and affect the patient's quality of life (QOL); (Lacouture et al., 2011).
To date, limited prospective data on the treatment of dermatologic side effects caused by MAPK pathway inhibitors exist, especially in the pediatric population. However, in adults who took epidermal growth factor receptor (EGFR) inhibitors there have been several publications regarding the treatment of dermatologic side effects. EGFR inhibitors are another type of medication that has triggered similar dermatologic side effects. Acneiform eruptions have been one of the most common types of dermatologic side effects caused by both EGFR inhibitors and MAPK pathway inhibitors (Gorji et al., 2022). Studies for treatments of acneiform eruptions revealed response rates from placebo creams alone suggesting that restoration of the skin barrier function can by itself prevent these types of side effects (Gorji et al., 2022). These results provided rationale to include a basic skin care routine as prophylactic measures for patients who are at risk of developing dermatologic side effects (Gorji et al., 2022). A basic skin care routine typically consists of three main steps cleansing, moisturizing, and protecting. The first step includes the application of a gentle cleanser morning and night to remove dirt and oil from the skin but not stripping the skin of its natural barrier. Next, a moisturizer should be applied after the skin is cleansed. Lastly, every day regardless of weather, sunscreen should be applied to protect the skin.
Method
Study Design and Setting
This study was prospective, non-randomized, and approved by the Institutional Review Board at Washington University School of Medicine in St. Louis, Missouri. All participants were treated at St. Louis Children's Hospital. Participants enrolled from June 2021 through July 2022. Originally, the patient's medical and dermatologic histories were self-reported within the baseline surveys. However, after an interim analysis discrepancies and blank questions were discovered. The study protocol was then amended to include chart reviews of the medical record to answer the medical history questions.
Procedures
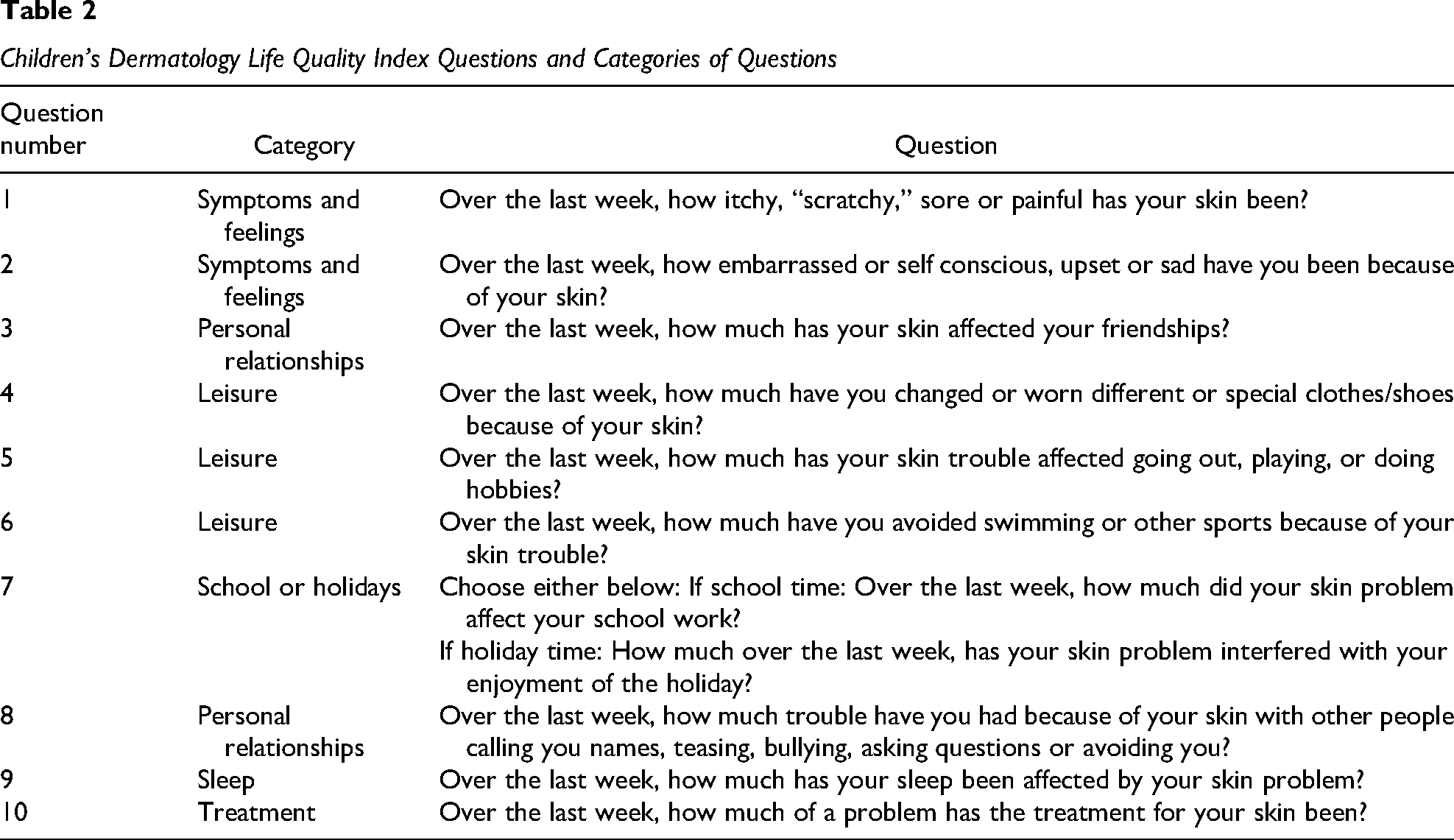
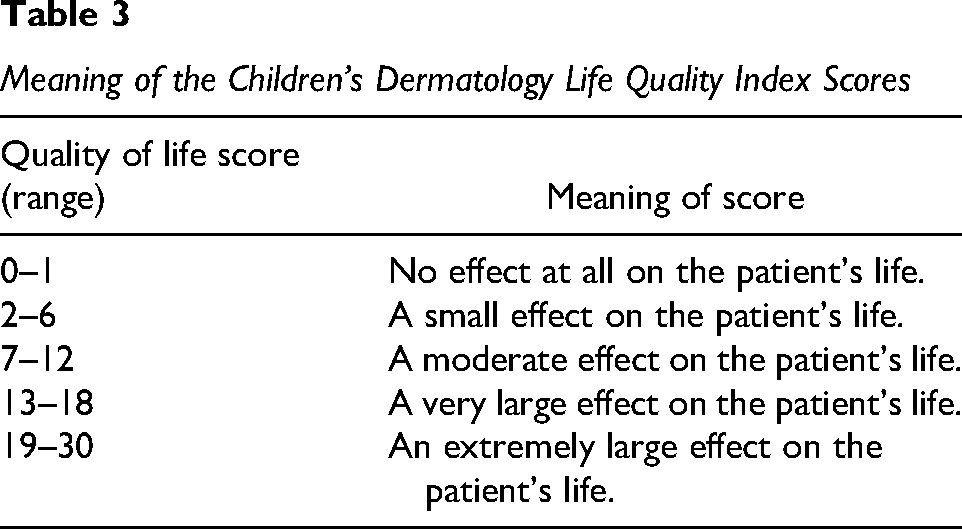
Based on the current available data published, a multi-disciplinary team that consisted of oncologists, a dermatologist, advanced practice providers and nurses assembled a skin care kit which consisted of basic skin, oral, and hair care products. The kits included all basic skin care items and additional products to support patients who may experience the most common types of dermatologic side effects from MAPK inhibitors. Since these products are not prescriptions, purchasing them may be challenging for some patients. The products or the amount of products needed have been expensive, and most are not covered by insurance companies. To improve access, with the support of Friends of Kids with Cancer (https://www.friendsofkids.com/), the skin care kits were provided to the patients free of cost (see Table 1 for contents). These products, along with an instruction sheet explaining their use, were provided to study participants or their caregivers with the intention of preventing and treating dermatologic side effects caused by MAPK inhibitors (Table 1). All products were available over the counter and were full-sized products, not samples. Participants were enrolled into one of two study groups. Group A included participants who were actively taking a MAPK inhibitor but for less than 6 months. Group B included participants who were prescribed a MAPK inhibitor but had not yet started the drug at the time of enrollment. Both groups received the skincare kit, along with written and verbal instructions for product use over the next 3 months. If a participant needed more of the products, unlimited refills were supplied. Baseline surveys included a demographic and health history questionnaire. Additionally, all participants 4 years of age or older completed a baseline QOL questionnaire [Children's Dermatology Life Quality Index (CDLQI) or the Dermatology Life Quality Index (DLQI)] (Olsen et al., 2016). These validated tools were chosen since the CDLQI and DLQI are the most widely used instruments developed to measure the impact of skin disease in children and adults aged 4 and older (Olsen et al., 2016). The CDLQI was developed specifically for patients ages 4–16 since this tool was more sensitive to a child's developmental level (Lewis-Jones & Finlay, 1995). The DLQI was developed and validated for patients ages 17 and older (Finlay & Khan, 1994). These 10-item questionnaires addressed the following: the patient's symptoms and feelings related to their skin, the impact on leisure time, the impact on school or holiday time, the effect on personal relationships, the impact on sleep, and how treatment for their skin problem has affected them. The individual questions have been included (Table 2). The total QOL scores for all 10 questions ranged from 0 to 30. The scoring and meaning of numerical results are listed in Table 3. If needed, younger children were offered parental assistance when they filled out the questionnaire and a cartoon version of the Children's Dermatology Life Quality Index was available. QOL data from participants younger than 4 years of age were not collected. After 3 months, at the second and final study visit (±4 weeks) all study participants completed a questionnaire in which they were asked whether they used each product in the kit. If the participant used an item, they then rated their satisfaction. Additionally, medication adherence to their MAPK inhibitor was self-recorded and the same QOL survey was completed. The participants answered a questionnaire based on recall regarding medication adherence. Specifically, they were asked to record how many doses they missed each month and the reason for those missed doses. Participants were not required to fill out a diary to record their experience nor was a pill count included.
Contents in the Skincare Kit and Included Patient Instructions
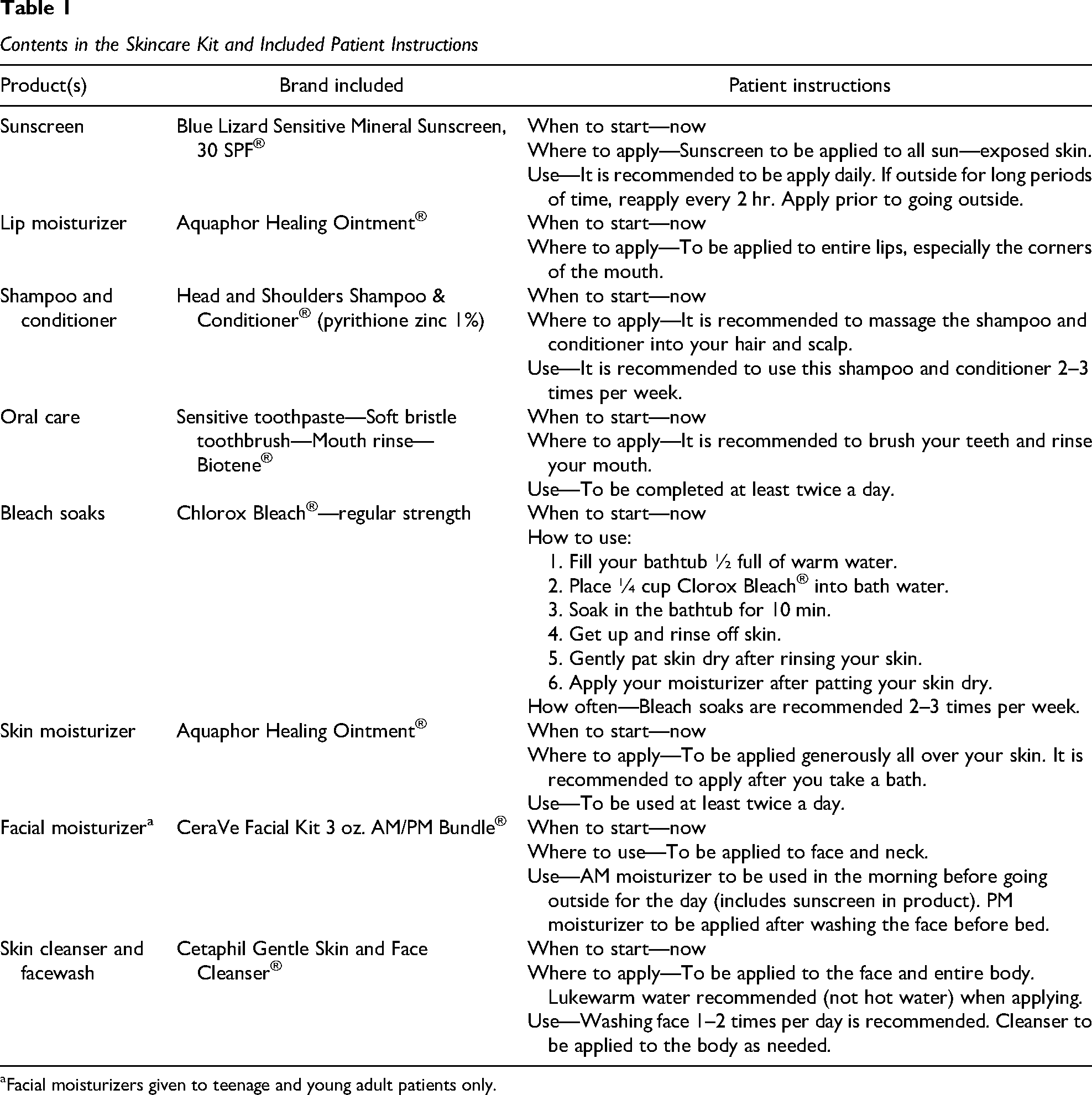
Facial moisturizers given to teenage and young adult patients only.
Children's Dermatology Life Quality Index Questions and Categories of Questions
Meaning of the Children's Dermatology Life Quality Index Scores
Participants
Participants up to 21 years of age were included. Any participant, who was prescribed a MAPK inhibitor and had been on this therapy for less than 6 months, was eligible. If a participant had taken a MAPK inhibitor prior to enrolling in this study, they were still eligible. This included participants who were retreated with the same MAPK inhibitor or had received a different MAPK inhibitor in the past. There was no wash out criteria for those who had been treated in the past.
Data Analysis
Demographic information and medical histories were extracted from the medical record and analyzed using descriptive statistics. Skin care product use was quantified as counts (frequencies) derived from the 3-month follow-up questionnaire. Patient satisfaction was assessed with ratings (excellent to poor) using a 5-point Likert scale. Utility results were reported as counts (frequencies). Free-text comments about preferences for different products were reported from this questionnaire, as well. Scores (means) from the CDLQI and DLQI at baseline were compared to those at the 3-month time point (paired t-test). Higher scores showed a more impaired QOL. Medication adherence was quantified by self-report of the number of doses missed.
Results
Baseline and 3-Month Follow-Up Questionnaire Results
Twenty participants, ages 2-21 were enrolled in this study (12 in group A and 8 in group B). Ten participants (83%) completed all evaluations in group A and 7 (88%) in group B, which yielded an 85% retention rate. Fourteen participants (82%) took MEK inhibitors, and 3 (18%) took pan-RAF inhibitors. All participant characteristics are listed in Table 4. Initially baseline information was obtained from handwritten self-reported surveys completed in an outpatient clinic during existing clinic visits. Discrepancies were identified after the study team had reviewed these baseline surveys. Additionally, some questions were left blank, some handwriting was illegible, and some questions that did not apply to the participant were completed. The study protocol was amended to allow for chart reviews to confirm the accuracy of the completed survey data. This data included questions about the participant's diagnosis, past medical history, current medications, past skin problems, and the current MAPK therapy they were prescribed. After the amendment, 14 participants’ baseline surveys were cross checked against their medical chart. Of those participants, 11 (79%) had discrepancies. The most frequent discrepancies were related to skin problems followed by current medications, diagnosis, past medical history, and then lastly the current MAPK inhibitor therapy.
Characteristics of the Patients at Baseline (N = 17)
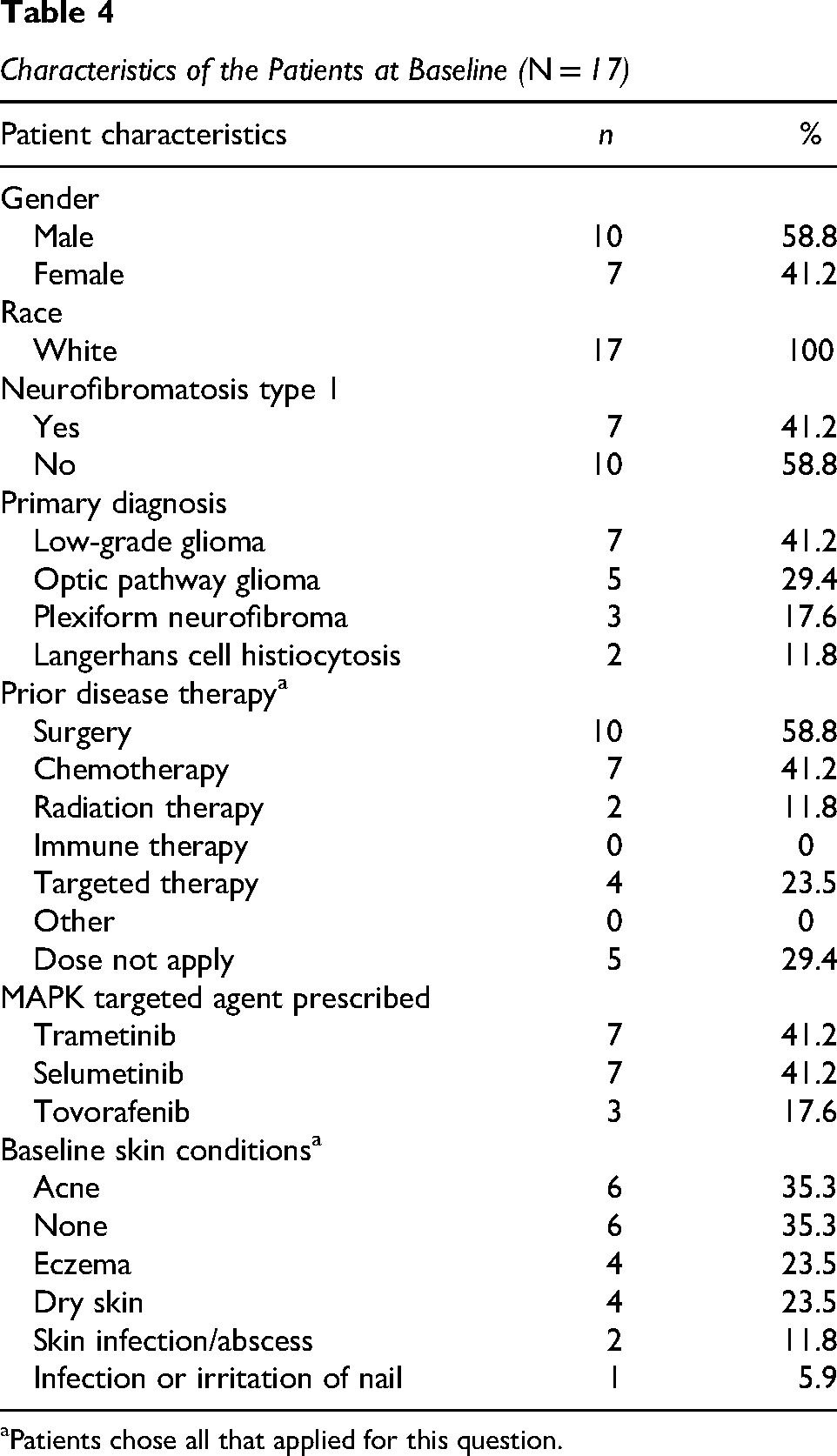
Patients chose all that applied for this question.
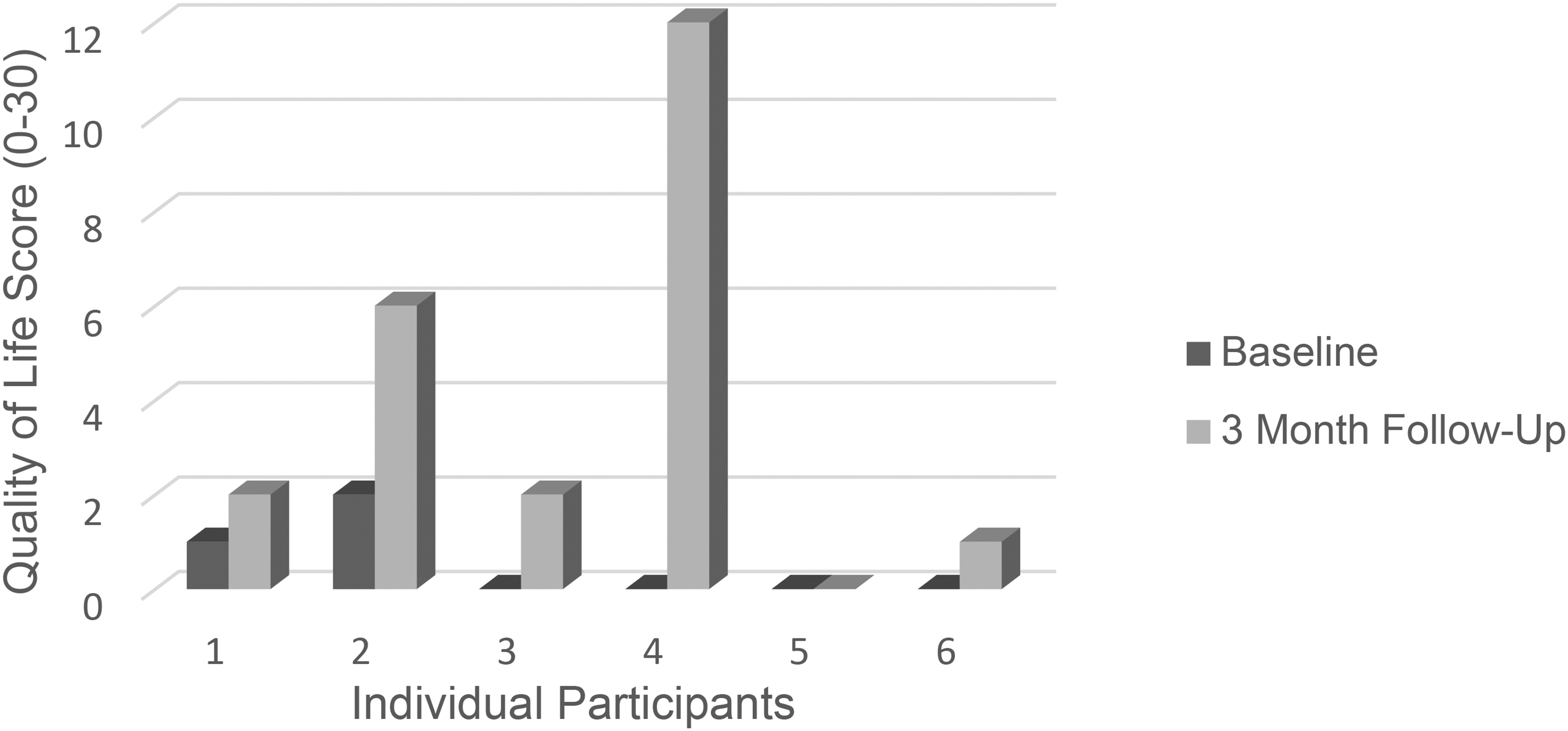
At the 3-month time point, 8 participants (47%) rated the skincare kits as excellent; 6 (35%) very good, 1 (6%) good, 2 (12%) fair, and none of the participants rated them poor. Thirteen participants (77%) thought the kits should be provided to participants when they start their MAPK inhibitor versus after developing a dermatologic side effect. Thirteen participants (77%) stated that the instructional sheet was helpful, and only 1 participant (13%) reported not using it. Individual product utilization and satisfaction results are reported (Table 5). Most participants reported using each of the following products within the kit: sunscreen, lip moisturizer, shampoo, mouthwash, skin moisturizer, skin cleanser, and face moisturizers. The bleach for diluted bleach baths and Biotene® mouthwash were used the least. Of all the participants who reported using each skincare product, the majority reported that they would reuse those products, which included the mouthwash and bleach for diluted bleach baths. Most participants stated that they liked every product included in the kit and the majority thought each product made them feel better compared to feeling worse or feeling the same.
Product Use and Satisfaction (N = 17)
Rating was completed by those who used product. Participants were asked whether they like or dislike each product and whether the product made their skin feel better, worse, or no change was experienced.
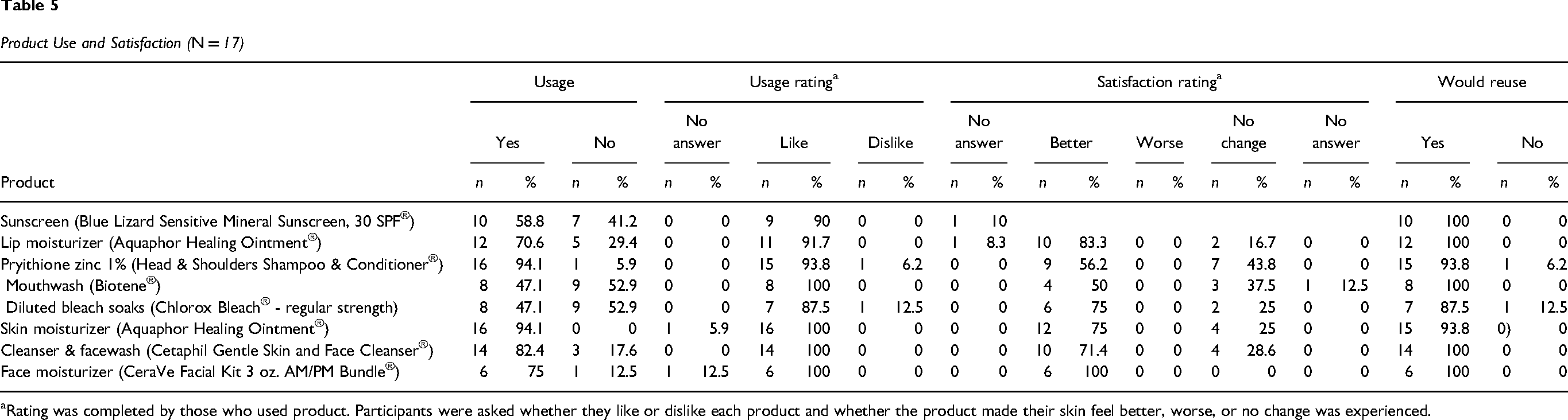
Quality of Life
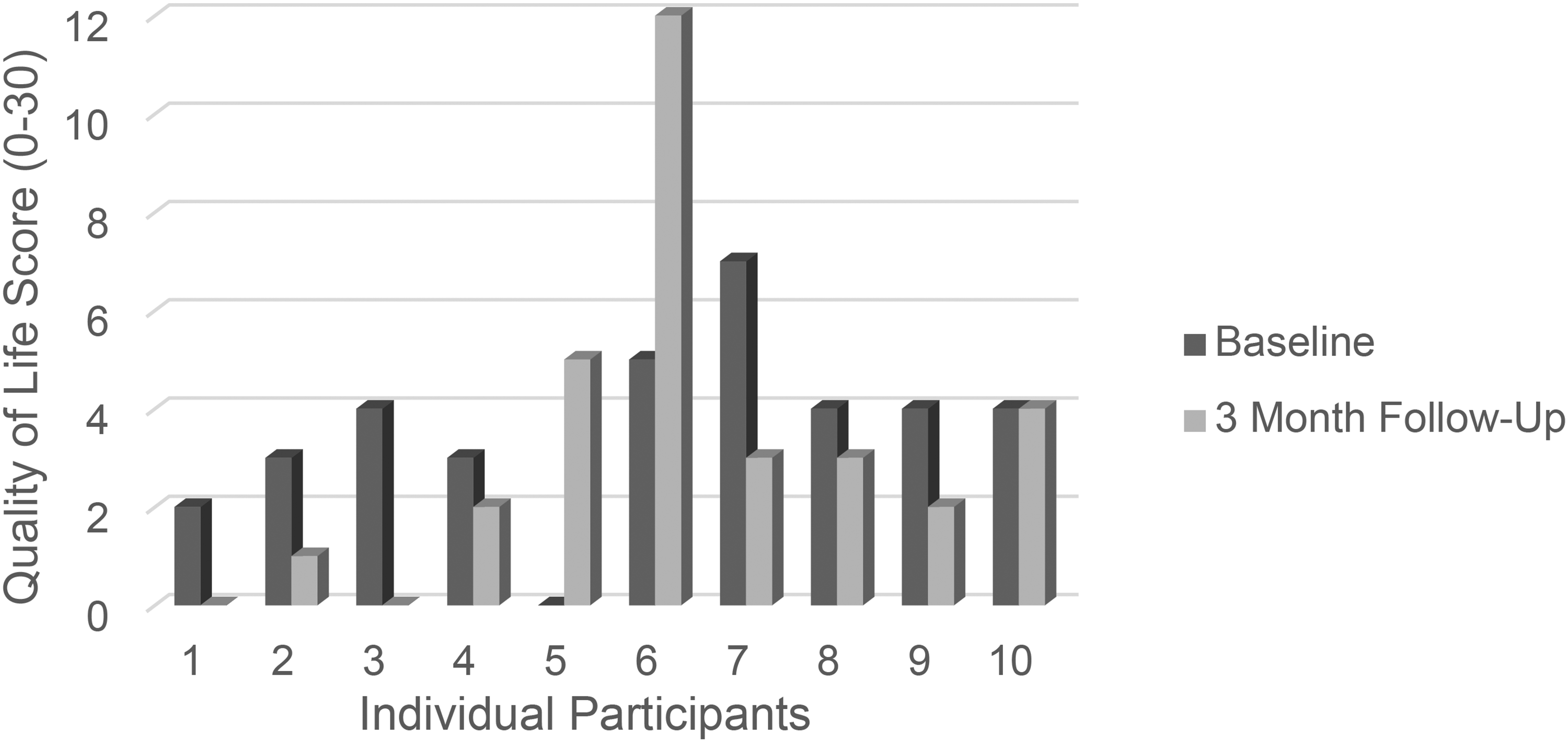
Ten participants (100%) completed QOL surveys in group A. At baseline, having already started a MAPK inhibitor, the mean total QOL score was 3.6 (SD = 1.8). During the 3-month follow-up visit, the mean QOL score decreased to 3.2 with a standard deviation of 3.5 (p = 0.74). These scores are within a “small effect” range for this tool, and there was no significant difference between the change in scores. The individual QOL scores for each study participant in group A were included (Figure 1). In group B, 6 participants (86%) completed QOL surveys. At baseline, before starting a MAPK inhibitor, the mean QOL score was 0.5 (SD = 0.8), and this increased to 3.8 (SD = 4.5) at follow-up (p = .13). Thus, scores changed from “no effect” to a “small effect” on QOL. This change indicates that the participants’ QOL may have worsened due to the experience of dermatologic side effects. However, the change in QOL was not statistically significant. The individual QOL scores for each study participant from group B were also included (Figure 2). The individual scores of each QOL question were then analyzed for the participants who completed the CDLQI. Participants scored the highest (worse reported QOL) on questions 1 and 2 (Table 2), which asked about the participants’ feelings and symptoms caused by their side effects from their MAPK inhibitor. Fifteen participants (66%) scored these 2 questions as the highest.
Group A Quality of Life Scores.
Group B Quality of Life Scores.
Adherence
The participants’ adherence to their MAPK inhibitor was evaluated, and 11 out of 17 total participants (64.7%) reported that they missed no doses, 4 (23.5%) missed 1–5 doses, and 2 (11.8%) missed greater than 10 doses. Three participants provided reasons why they missed doses. Two (67%) reported “I just forgot” and 1 (33%) reported “the other side effects (not skin related) were so bad that I needed a break from my medications.” Complexity of the medication regimen, traveling or staying at multiple homes, and the skin-related side effects were not reported as reasons why participants missed doses of their MAPK inhibitor.
Discussion
The skin care kits consisted of essential skin and hair products for a basic, routine skin care regimen. This study revealed that most study participants utilized and were satisfied with their skin care regimen. However, it was unclear why some products were not used and unfortunately the post-survey did not include rationale for unused products. Children as young as 2 years old were enrolled. Potentially young age and developmental stage posed utilization challenges. Also, participants may have been unfamiliar with diluted bleach baths, and thus focusing education on the recipe, instructions for use, and background rationale may improve usage rates. Additional barriers to use like not having a bathtub or being able to soak in a bathtub should be considered. Modifications and personalization should be implemented for the usage of all products. Within the skin care kit, an instructional guide on how and when to use each product was supplied. All but one participant used the instructional guide and those who utilized the guide reported it was helpful. Given the acceptability of the guide and the complexity of care for this patient population, a detailed instructional sheet should be included. Healthcare providers must also recognize that topical medications may be prescribed to treat dermatologic side effects along with a basic routine skin care regimen. Guidance on how to apply multiple topical products and the order of application should be provided.
A skin-specific QOL tool was used to explore the impact of dermatologic side effects caused by MAPK inhibitors. Of those participants who were taking their MAPK inhibitor at both study timepoints (baseline and the 3-month post-survey) there was no change in their QOL scores. The remaining participants started a new MAPK inhibitor after taking their baseline survey. All but one participant had a worse QOL score on their 3-month survey. This change was not statistically significant, suggesting QOL might have been impacted after starting MAPK therapy. The QOL surveys are divided into six categories. The category with the highest (worst) scores asked about the participant's symptoms (itchy, sore, and painful) and feelings (upset, embarrassed, self-conscious, and sad) related to their skin changes. This suggested dermatologic side effect may be more than just a physical change in the appearance of the skin, hair and nails. These symptoms and psychological impact should be assessed for anyone taking a MAPK inhibitor.
Limitations
There were limitations to this study. It was conducted as a single-institution study, resulting in a small sample size. Participants from all racial groups were not represented. Participants primarily self-reported as White. Given differences in hair type and skin tones, a more diverse population could have impacted the utilization and satisfactory rates of skin care products. Medication adherence was only measured by self-report, rather than by pill count or drug diaries. Dose modifications of the MAPK-inhibitor were also not recorded. All evaluations were collected from handwritten surveys during clinic visits. The study team discovered discrepancies within the baseline surveys. It was unclear why these discrepancies occurred but suspected this might be from errors due to distractions during clinic visits. Future studies should consider alternative ways of filling out surveys like electronic versions and should be offered at a variety of timepoints other than only during scheduled clinic visits.
Conclusion
A routine, daily skin care regimen is one strategy to prevent and treat dermatologic side effects caused by MAPK inhibitors. Given the complexity of a skin care regimen and the patient's underlying diagnosis, upfront and continued education, both verbal and written, regarding pediatric oncology patients’ diagnosis, treatment, potential side effects, side effect management strategies, and skin care products are needed. Both researchers and clinicians should also consider the impact on the patient's QOL from dermatologic side effect exposure. Instead of recording only the visible changes in the skin, hair and nails, physical symptoms and the psychological impact from these side effects should be routinely assessed. Additional research on this type of skin care regimen is needed to optimize the management of these side effects. Given the skin care kits’ high satisfaction and acceptance rates, future research studies should evaluate the effect of these items on QOL with adequate power to detect changes. Lastly, patients of different skin tones and hair types should be included to evaluate the most appropriate products based on these differences.
Footnotes
Ethics Approval and Informed Consent
The questionnaire and methodology for this study was approved by the Washington University School of Medicine Institutional Review Board; IRB ID: 202104060. The study was conducted with the principles of the Declaration of Helsinki. Written informed consent was obtained for each study participant, and the informed consent document was approved by the IRB.
Author Contributions
All listed authors contributed to the conduct of this research and the writing of this manuscript.
Funding
The authors disclose the following financial support: Friends of Kids with Cancer.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bryan A. Sisk is a consultant for Novartis. Mohamed S. Abdelbaki has consultant agreements with DayOne Pharmaceuticals and Citi Pharmaceutricals. He is a chair of a DSMB for Bexion, Advisory Board Member for DayOne, and a study chair in which that study has funding from Novartis. Ashley Meyer participated in a one-time Advisory Board for AstraZeneca on December 14, 2021. The other authors have no relevant financial or non-financial interests to disclose.