
Abstract
Background
Endoscopic endonasal approach (EEA) has gained widespread acceptance as a surgical approach for treating sinonasal malignancies in the last decade.
Objectives
This study examined the validity of the EEA as a standard modality for the surgical treatment of sinonasal malignancies.
Design
A retrospective multicenter cohort study
Methods
This study included patients with nasoethmoidal malignancies who underwent initial surgical treatment between 2014 and 2016 at 10 tertiary referral hospitals in Japan. The EEA, craniofacial approach (CA), and EEA combined with CA (EEAwCA) were used as the surgical methods.
Results
The total number of participants was 110, with a median posttreatment observation period of 69 months. The olfactory cleft (26%) was the most frequent lesion site. Squamous cell carcinoma (29%) and olfactory neuroblastoma (24%) were the most frequently observed pathological classifications. EEA was performed in early-stage cases, and EEAwCA, which is frequently used for tumors that extend into the orbit and/or intracranial regions, was performed in advanced-stage cases. Negative-margin resection was achieved in 85%, 78%, and 64% of EEA, EEAwCA, and CA cases, respectively; postoperative radiotherapy was performed in 50%, 56%, and 36% of patients with EEA, EEAwCA, and CA, respectively; and the 5-year local control rates were 90%, 78%, and 82% for EEA, EEAwCA, and CA, respectively. En bloc resection for EEA, and postoperative irradiation for EEA and EEAwCA were associated with fewer local recurrences. Validation of the operation time, hospitalization period, intraoperative blood loss, and postoperative complications demonstrated the low invasiveness of the EEA.
Conclusion
The EEA is a minimally invasive surgical modality with preferable oncological outcomes for the treatment of nasoethmoidal malignancies when adequately planned.
Plain Language Summary
Purpose
This study looked at a newer, less invasive surgery called the endoscopic endonasal approach (EEA), which goes through the nose to remove tumors in the nose and nearby areas. The goal was to see if this method could be used as a standard treatment.
How the Study Was Done
Researchers looked back at 110 patients in Japan who had surgery for cancer in the nose and surrounding areas between 2014 and 2016. They had surgery using one of three methods:
EEA (through the nose)
CA (a more traditional open surgery)
EEA combined with CA (used for more serious cases)
What They Found
Most patients had tumors in a part of the nose related to the sense of smell. The most common types of cancer were squamous cell carcinoma and a rare nerve-related tumor. The EEA was mostly used for early-stage cancers, and the combined method was used for more advanced cases. The cancer was completely removed in about 85% of EEA cases, 78% of combined cases, and 64% of traditional cases. People who had EEA had fewer side effects, lost less blood, and stayed in the hospital for a shorter time. After 5 years, the cancer had not come back in 90% of EEA cases, 78% of combined cases, and 82% of traditional cases. Patients who had radiation after surgery or had tumors removed in one piece had better results.
Conclusion
The EEA is a safe and effective option for treating certain nose cancers, especially when it's carefully planned. It causes less harm to the body and works well for early-stage cancers.
Keywords
Introduction
The endoscopic endonasal approach (EEA) has become the standard surgical approach for treating sinonasal malignancies, and endoscopic sinus surgery (ESS) has long been a standard surgical modality for treating chronic sinusitis. Advances in medical engineering technology have contributed to the development of extended surgical procedures for ESS, including Draf type III surgery for refractory frontal sinus lesions. Furthermore, progress in ESS has also promoted the use of EEA in skull base surgeries, particularly pituitary surgery. For the surgical resection of sinonasal malignancies, an open craniofacial approach (CA) is standard. The advantage of EEA is its low invasiveness, which can improve the quality of life of patients by improving postoperative recovery and preserving facial aesthetics, 1 making it a standard surgical approach used in Western countries. 2
To illustrate the current status of EEA for the treatment of sinonasal malignancies in Japan, a multicenter collaborative study was previously performed with support from the Japan Agency for Medical Research and Development (AMED, 16ck0106228h0001). A questionnaire survey was conducted nationwide at 633 facilities accredited by the Japanese Society of Otorhinolaryngology Head and Neck Surgery, 3 which revealed that EEA or EEA combined with CA (EEAwCA) was performed in approximately 20% of the facilities for the treatment of sinonasal skull base malignancies. Based on the results of this survey, we chose 10 tertiary referral hospitals where EEA was routinely used in a relatively large number of patients with malignancies in the nasal and ethmoid sinuses and conducted a multicenter retrospective study to clarify the surgical and oncological outcomes of patients who underwent surgical treatment for nasoethmoidal malignancies using EEA. Nasoethmoidal malignancies were chosen as the focus of this study due to their anatomical suitability for EEA. Unlike maxillary sinus cancer, which predominantly consists of squamous cell carcinoma, nasoethmoidal malignancies exhibit diverse histopathological subtypes, making diagnosis and treatment more challenging. Despite their rarity and the limited number of large-scale studies to date, our study aims to provide valuable insights into the efficacy and limitations of EEA in managing these tumors.
Methods
Study Design and Setting
The reporting of this study conforms to the STROBE statement. 4 This is a retrospective multicenter cohort study conducted at 10 tertiary referral hospitals in Japan (Mie University Hospital, Chiba University Hospital, Kyoto University Hospital, Jikei University Hospital, Nagoya University Hospital, Oita University Hospital, Kumamoto University Hospital, Tsukuba University Hospital, Tokyo Medical and Dental University Hospital, and Kobe University Hospital).
Participants
We included patients who were diagnosed with primary nasoethmoidal malignant tumors, underwent initial surgical treatment between January 2014 and December 2016, and had available postoperative follow-up data. The exclusion criteria were as follows: (1) patients with metastatic nasoethmoidal malignant tumors; (2) those who did not undergo surgical treatment; and (3) cases involving reoperation or revision surgery. This was a retrospective study that included all eligible patients treated during the 3-year period; therefore, no formal sample size calculation was performed.
Data Collection
Demographics (sex and age at the time of surgery), pathological diagnosis, primary site of the tumor, tumor extension (T stage and presence of intracranial or orbital invasion), surgical approach (EEA, EEAwCA, or CA), resection method (en bloc or segmental resection), operation time, intraoperative blood loss, hospitalization period, postoperative complications, pre- and postoperative treatments, and clinical courses after treatment were collected from medical records. The primary outcomes were survival outcomes (overall survival (OS) and recurrence-free survival (RFS)) and local control (LC) rates. Secondary outcomes included perioperative variables and complications. Surgical approach (EEA, EEAwCA, or CA) was the main exposure. Predictors and potential confounders included tumor stage, location, histology, and adjuvant therapy. Although there are specific staging systems for a few pathologies, we used the Tumor-Node-Metastasis (TNM) classification for the Nasal Cavity and Paranasal Sinuses of the Union for International Cancer Control (8th edition). Although cases with missing key clinical or outcome data were planned to be excluded from the analysis, no such cases were identified. We have clarified the definitions and assessment methods of all major outcome variables as follows. Local control was defined as the absence of clinical or radiographic evidence of recurrence at the primary site during follow-up. Recurrence was defined as radiologically or histologically confirmed tumor regrowth after initial curative surgery. Complications such as anosmia and ocular symptoms were evaluated based on patient-reported symptoms and clinical interviews conducted during follow-up visits.
Statistical Analysis
Median values were compared using the Kruskal-Wallis test, and pairwise comparisons were tested using Dunn's method. The distribution of categorical variables was compared using the chi-square test or Fisher's exact test. Survival outcomes (OS and RFS) and LC rates were determined using the Kaplan-Meier method and compared among the surgical approaches using the log-rank test. Statistical significance was set at P < .05. Statistical analyses were performed using the Statistical Package for the Social Sciences software version 29.0 (SPSS Japan Inc., Tokyo, Japan). Due to the limited number of events in the dataset, multivariable regression analyses for survival outcomes and perioperative variables were not feasible. Univariate comparisons were therefore conducted with full transparency, and limitations in statistical adjustment were addressed in the discussion.
Results
The total number of patients was 110, with ages ranging from 13 to 85 years (median, 60 years), composed of 57 men and 53 women, and observation periods ranging from 2 to 96 months (median, 69 months). The olfactory cleft was the most common primary site of lesions (Table 1). The olfactory cleft and anterior ethmoid sinus were the most common primary sites of T4, whereas the nasal septum and inferior turbinate were the most common primary sites of T1 and T2. The most common histopathological type was squamous cell carcinoma, followed by olfactory neuroblastoma, malignant melanoma, adenocarcinoma, adenoid cystic carcinoma, and chondrosarcoma. Other histopathological classifications include mucoepidermoid carcinoma, acinic cell carcinoma, rhabdomyosarcoma, glomangiopericytoma, basal cell carcinoma, adenosquamous carcinoma, transitional epithelial carcinoma, clear cell carcinoma, neuroendocrine carcinoma, verrucous carcinoma, undifferentiated carcinoma, leiomyosarcoma, angiosarcoma, epithelioid angiosarcoma, biphenotypic sinonasal sarcoma, ameloblastic carcinoma, malignant myoepithelioma, malignant carcinoid tumor, follicular dendritic cell sarcoma, spindle cell carcinoma, and malignant solitary fibrous tumor. Early-stage cases (T1 and T2) were frequently found in squamous cell carcinoma, while advanced cases equivalent to T4b were frequently found in olfactory neuroblastoma.
Subsite Distribution and Histopathological Type by T Stage.
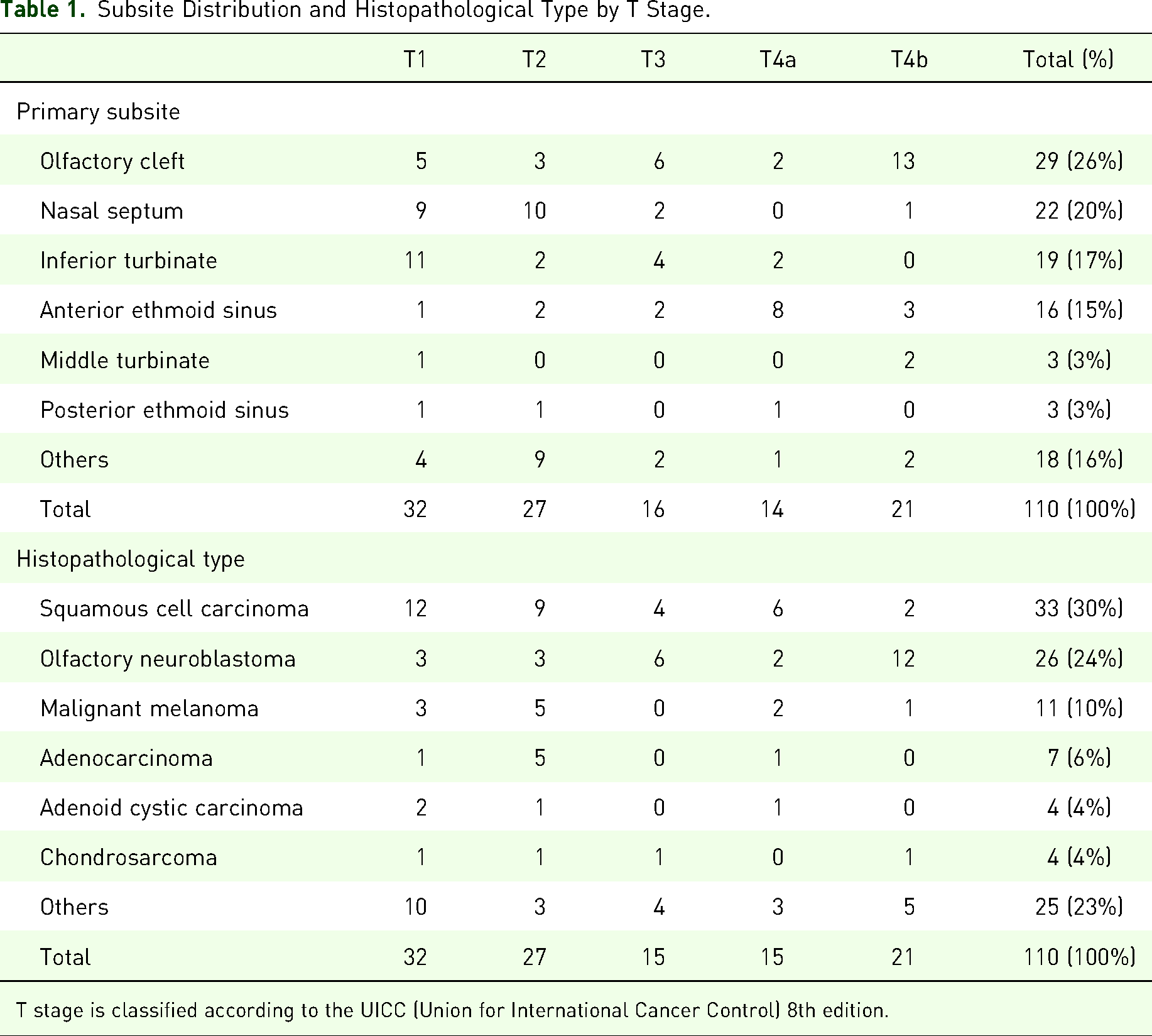
T stage is classified according to the UICC (Union for International Cancer Control) 8th edition.
There were no significant differences in the median age and sex among the surgical approaches (P = .197, Kruskal-Wallis test and P = .558, chi-square test, respectively; Table 2). There was no difference in the distribution of surgical approaches according to histopathological type (P = .272, chi-square test). As for the number of T stages, there was a trend that EEA was more often applied to the early-stages and EEAwCA was more often applied to the advanced stages (P = .007, chi-square test). For tumor extension outside the sinonasal cavity, both orbital and intracranial invasions were more frequently addressed with CA and EEAwCA than with EEA (P < .001, chi-square test).
Patients’ Characteristics by Surgical Approach.
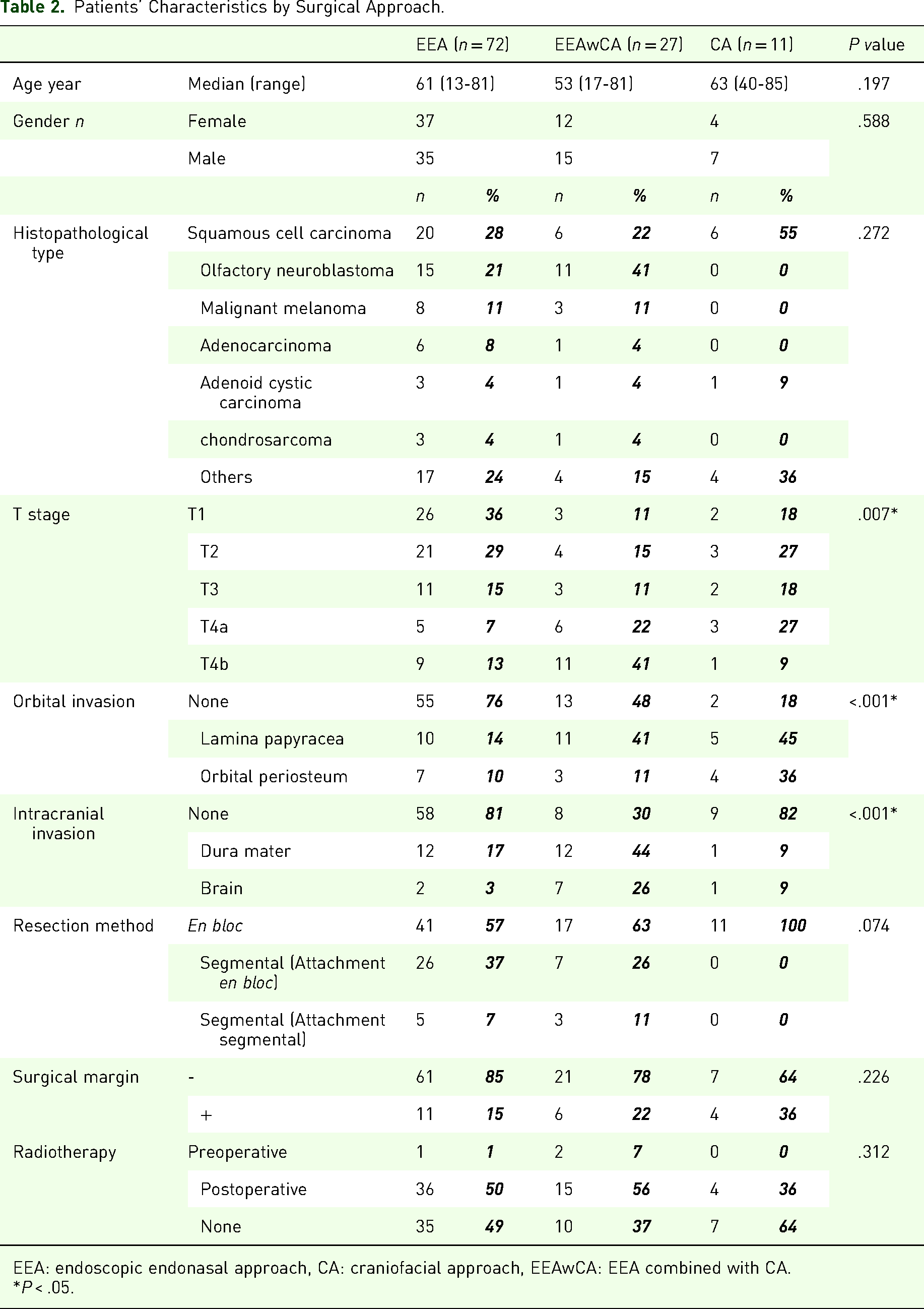
EEA: endoscopic endonasal approach, CA: craniofacial approach, EEAwCA: EEA combined with CA.
*P < .05.
The oncological outcomes are shown in Figure 1. Regarding the RFS, a significant difference among the surgical approaches was observed (P = .029, log-rank test). EEA exhibited superior RFS compared to EEAwCA and CA. No significant differences among the surgical approaches were found in the OS (P = .262, log-rank test) or LC rate (P = .216, log-rank test). In total, 21 patients died and 36 experienced recurrences, including 17 local recurrences, 4 lymph-node recurrences, and 15 distant metastases. Given the limited number of events, survival analyses were conducted without adjustment for covariates. The tumor resection methods, preoperative and postoperative radiotherapy, and LC for each subgroup are shown in Table 2. There was no difference in the ratio of en bloc or segmental resections between the EEA and EEAwCA groups (P = .074, chi-square test). In addition, there was no difference in the tumor-positive rate of pathological resection margins between the 2 groups (P = .226, chi-square test). All patients in the CA group underwent en bloc resection; however, the proportion of negative resection margins in the CA group was lower (7/11, 64%) than in the EEA (61/72, 85%) and EEAwCA (21/27, 78%) groups, although the difference was not statistically significant (P = .226, chi-square test). Approximately half of the patients in the EEA and EEAwCA groups received postoperative radiotherapy. Local recurrence was significantly more common in the segmental resection group than in the en bloc resection group in the EEA group (P = .022, Fisher's exact test), but there was no significant difference between the 2 resection methods in the EEAwCA group (P = .613, Fisher's exact test; Table 3). The results of the pathological margin studies showed no correlation with local recurrence in any group (P = .704 for EEA, P = .502 for EEAwCA, and P = .152 for CA, Fisher's exact test). In the EEA and EEAwCA groups, there were significantly fewer cases of local recurrence in patients who received postoperative radiotherapy (P = .045 and P = .043, respectively, Fisher's exact test); however, in the CA group, postoperative radiotherapy showed no significant correlation with local recurrence (P = .721, Fisher's exact test). Table 4 shows a list of histopathological types in cases of local recurrence. None of the histopathological types had a particularly high incidence of local recurrence.
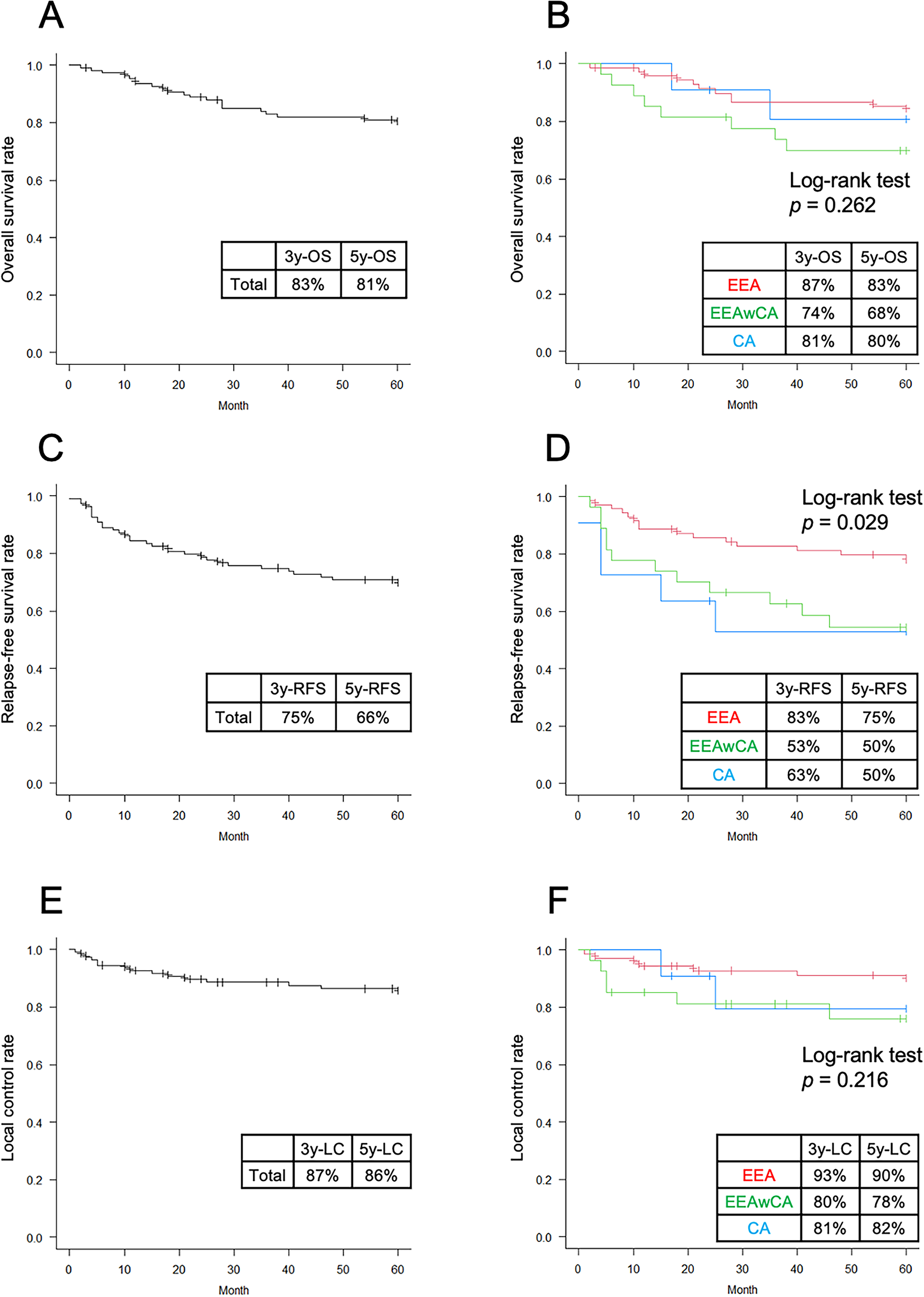
The 5-year survival and local control rates. The OS, RFS, and LC rates for all cases are shown in panels A, C, and E, respectively, and those for each surgical approach are shown in panels B, D, and F, respectively. The red, blue, and green lines indicate the EEA, CA, and EEAwCA approaches, respectively. OS, overall survival; RFS, recurrence-free survival; LC, local control; EEA, endoscopic endonasal approach; EEAwCA, endoscopic endonasal combined with craniofacial approach; CA, craniofacial approach.
Prognostic Factors for Local Recurrence by Surgical Approach.
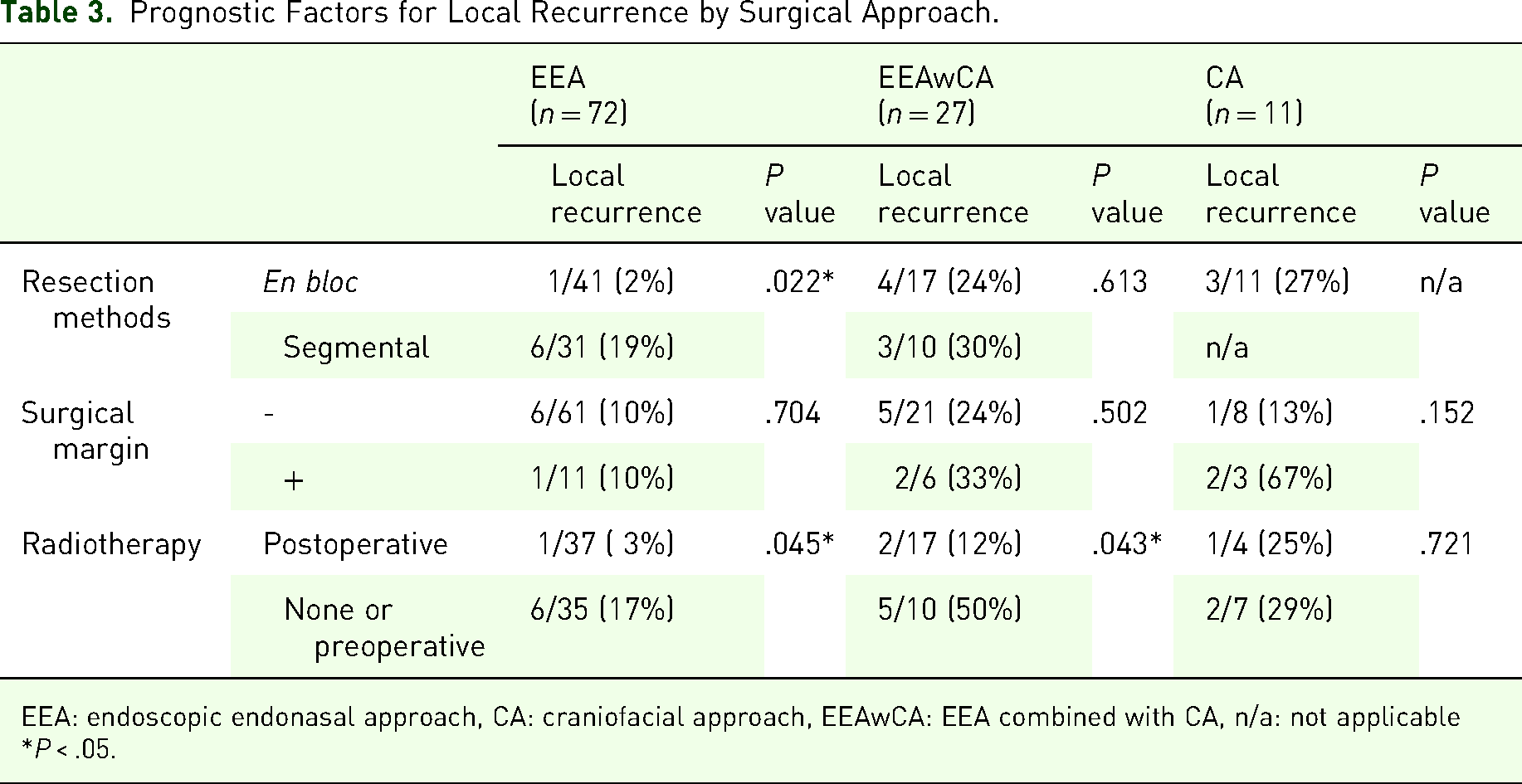
EEA: endoscopic endonasal approach, CA: craniofacial approach, EEAwCA: EEA combined with CA, n/a: not applicable
*P < .05.
Histopathological Types of Local Recurrence Cases.
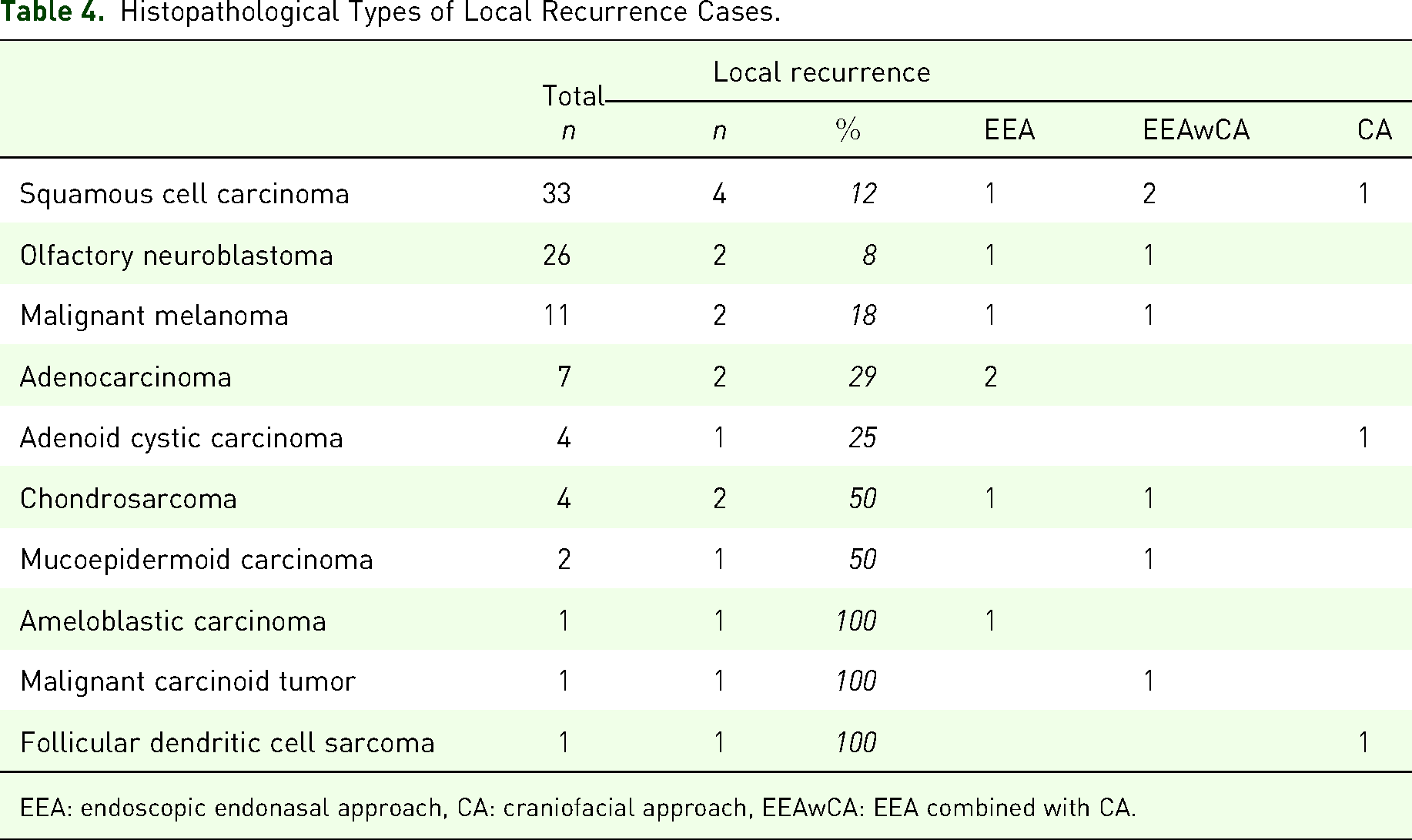
EEA: endoscopic endonasal approach, CA: craniofacial approach, EEAwCA: EEA combined with CA.
The median operative time, amount of intraoperative blood loss, and hospitalization period after surgery for each surgical approach are shown in Table 5. The operative time was significantly shorter in the EEA and CA groups, and the longest in the EEAwCA group (P = .001, Dunn's method for the post hoc test after the Kruskal-Wallis test). Intraoperative blood loss was significantly lower in the EEA group than in the other groups (P < .001, Dunn's test). The postoperative hospitalization period was also significantly shorter in the EEA group than in the CA group (P < .001, Dunn's test). The EEA group had a significantly lower incidence of postoperative complications than the other groups (P < .001, chi-square test). Main complications, such as cerebrospinal fluid leakage and meningitis, had a low incidence in all surgical approaches. The incidences of ocular symptoms and anosmia were significantly lower in the EEA group than in the other groups (P = .003 for ocular symptoms and P = .007 for anosmia, chi-square test).
Intraoperative Metrics and Postoperative Complications by Surgical Approach.
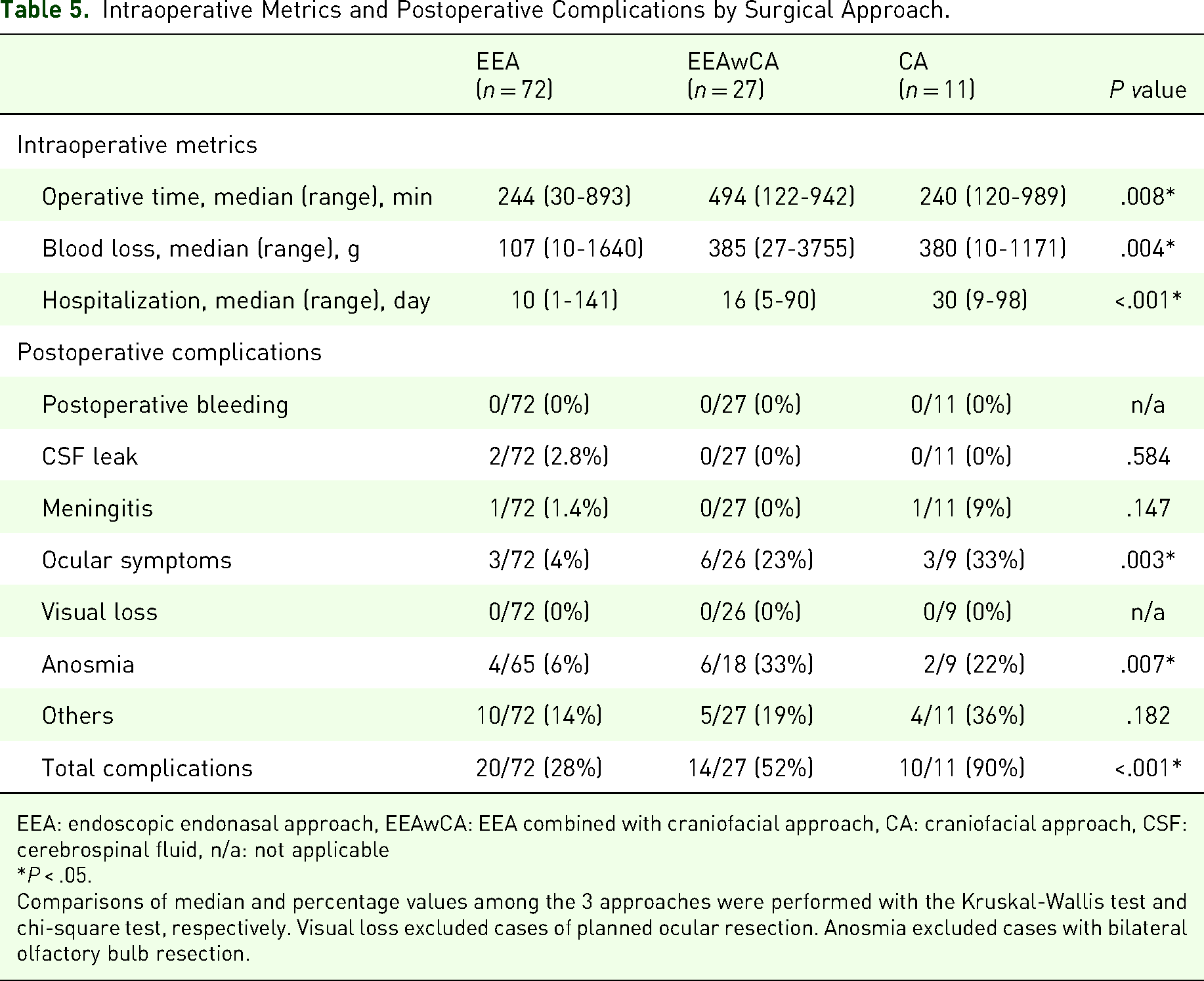
EEA: endoscopic endonasal approach, EEAwCA: EEA combined with craniofacial approach, CA: craniofacial approach, CSF: cerebrospinal fluid, n/a: not applicable
*P < .05.
Comparisons of median and percentage values among the 3 approaches were performed with the Kruskal-Wallis test and chi-square test, respectively. Visual loss excluded cases of planned ocular resection. Anosmia excluded cases with bilateral olfactory bulb resection.
Discussion
The sample size of the present study was comparable to previous reports from Europe and the United States in the early 2000s. Nicolai et al 5 analyzed 184 patients with sinonasal malignancies, wherein EEA and EEAwCA were used in 134 and 50 cases, respectively. Hanna et al 6 reported the utility of EEA by analyzing 120 patients with sinonasal cancers, including 93 treated with EEA and 27 treated with EEAwCA. The proportions of primary sites and clinical stages in the present study showed the same trends as those in previous reports. The olfactory cleft is the most common primary site of the tumor because olfactory neuroblastoma is exclusively a cleft primary tumor and second only to squamous cell carcinoma in histopathological distribution, accounting for approximately one-fourth of all cases. The diversity of histopathological types was also similar to that reported in Europe and the United States. Although squamous cell carcinoma is the most common type of head and neck cancer, it was found in only approximately 30% of cases in the nasal cavity and ethmoid sinus, while the remaining 70% had various epithelial and nonepithelial tumors, which is because of the high prevalence of small round cell tumors among malignant tumors arising in the medial region of the nasal cavity and ethmoid sinus. This is consistent with reports from the United States, where olfactory neuroblastoma was the most common histological type, and the nasal cavity, including the olfactory cleft, was the most common primary site. 6 However, in European countries, such as Italy, adenocarcinoma is more predominant, 5 suggesting that the histopathological types of sinonasal tumors may vary by race, ethnicity, and region.
The survival outcomes in this study were also comparable to those in previous studies, wherein Nicolai et al 5 reported 5-year OS, RFS, and LC rates of 85%, 82%, and 85%, respectively, and Hanna et al 6 reported 5-year OS and LC rates of 76% and 85%, respectively. In the present study, no significant difference in the OS or LC rates was observed among the surgical approaches classified by surgical approach (Figure 1), suggesting that the choice of surgical approach according to tumor extension may be adequate. EEAwCA was frequently used in advanced-stage cases, while EEA was frequently used in early-stage cases, which could explain the significant difference in RFS among the surgical approaches in the current study. This indicates the utility of EEA for the treatment of nasoethmoidal malignancies when its application is adequate.
In the EEA group, the local recurrence rate for segmental resection was significantly higher than for en bloc resection; however, in the EEAwCA group, no significant difference in the local recurrence rate between en bloc and segmental resection was noted. Postoperative radiotherapy contributed to low local recurrence rates in both the EEA and EEAwCA groups. The EEAwCA group included more advanced-stage cases than the EEA group; hence, the highly invasive nature of advanced-stage tumors could be a possible cause for the differences in the effects of en bloc resection between the EEA and EEAwCA groups. The efficacy of postoperative radiotherapy could be as effective as the rescue of close-margin cases because almost all cases with positive resection margins were treated with postoperative radiotherapy, and the results of the pathological margins did not show a significant difference in the local recurrence rate between the groups with and without postoperative radiotherapy. This is congruent with findings from previous studies that have demonstrated good results using postoperative irradiation after endoscopic surgery.5–9
In contrast, a previous study on CA reported that the factor responsible for local recurrence is positive resection margins, not the resection method. 10 In addition, recent studies on EEA in the treatment of sinonasal malignant tumors have demonstrated the importance of negative-margin resection for preferable oncological outcomes.7,11 The concept of segmental resection or multilayer resection, wherein tumor tissues other than the attachment of the tumor are resected first to secure well-operable surgical fields, followed by an en bloc resection with a sufficient safety margin around the tumor attachment area, has become popular in recent years, and good outcomes have been reported.12–14 In the present study, most segmental resections were performed according to the concept of multilayer resection, and the negative resection margin rate of the EEA was comparable to that of the CA. Therefore, to clarify the usefulness of resection methods in the future, multiple factors, such as histopathological characteristics of the tumor, differences in tumor stage, and standardization of evaluation strategies for pathological examination, should be verified in cases without postoperative treatment, which might be difficult to implement when the benefit of postoperative radiotherapy has been established.
In this study, we examined the invasiveness of each surgical approach. In general, EEA was expected to be minimally invasive and preserve sensory functions. The aesthetic value of avoiding external incisions was also included in EEA advancement. In the present study, significantly fewer postoperative complications were observed in the EEA group than in the other groups. The significantly lower incidence of ocular and olfactory disorders indicated that EEA is an excellent approach for preserving sensory function.
The clinical outcomes at the 5-year follow-up in the present study were favorable; however, locoregional recurrence after a longer period is well known, especially in olfactory neuroblastomas.8,15 Therefore, longer observation periods are required to determine clinical outcomes of nasoethmoidal malignancies. Studies with long observation periods have demonstrated the importance of controlling delayed cervical recurrence, especially in lateral retropharyngeal lymph nodes.8,16,17 Previous reports have also demonstrated good results in multidisciplinary treatment using endoscopic surgery and locoregional postoperative irradiation.8,16 Together with an adequate choice of surgical approaches, a regimen of postoperative radiotherapy according to the histology and extension of tumors should be established in the future.
Limitations
This study has several limitations. First, although we intended to compare oncological and perioperative outcomes across different surgical approaches, the limited sample size and small number of events prevented the use of robust multivariable analysis or matching procedures; residual confounding due to differences in tumor stage, histopathology, and adjuvant therapy may remain.
Second, certain complications, such as ocular symptoms and anosmia, were assessed based on patient-reported outcomes rather than objective testing. However, this approach reflects the standard clinical practice in many institutions.
Third, nasal cavity and ethmoid sinus carcinomas are rare cancers, and the histopathological diagnoses were extremely diverse, making it difficult to conduct a detailed analysis by histopathological type. Nevertheless, no specific histopathological subtype demonstrated a particularly high rate of local recurrence in this cohort, as shown in Table 4, suggesting that the findings remain informative.
Finally, the retrospective multicenter nature of this study inevitably introduces a degree of heterogeneity and uncertainty in data collection, surgical decision-making, and follow-up protocols across institutions. As a result, the study may be limited to identifying only the most apparent and consistent trends. Despite these limitations, we believe this study serves as a meaningful snapshot of current practice in Japan and provides a valuable foundation for the broader integration and prospective evaluation of endoscopic surgery for nasal malignancies.
Conclusion
The present findings demonstrate the utility of EEA for the treatment of nasoethmoidal malignancies when applied with appropriate case selection. To establish standardized treatment protocols for these rare tumors, long-term follow-up and standardization of pathological assessments are essential. Achieving this goal will require the collaboration among multidisciplinary experts, including endoscopic sinus surgeons, head and neck oncologists, radiation oncologists, and pathologists. 18
Footnotes
Ethics Approval and Consent to Participate
This study was approved by the Ethics Review Committee of Tokyo Medical and Dental University, a representative institution (M2016-156). Informed consent for participation in this study was obtained from patients through an opt-out procedure approved by the ethics committee.
Consent for Publication
Publication of the clinical data was conducted under an opt-out consent process, in accordance with institutional ethical guidelines and approved by the ethics committee.
Author Contribution(s)
Declarations
We thank Professor Richard M. Costanzo (Virginia Commonwealth University School of Medicine, United States) for reading the draft of the manuscript and providing invaluable comments and suggestions.
Funding
This work was supported by a grant from the Japan Agency for Medical Research and Development (AMED, grant number: 16ck0106228h0001).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to privacy or ethical restrictions but may be available from the corresponding author upon reasonable request and with appropriate institutional approvals.