
Abstract
Background
Chronic pain affects one in five Americans, yet rural patients face significant barriers to evidence-based interventions like biofeedback due to geographic isolation and provider shortages.
Objective
This pilot study evaluates the feasibility, acceptability, and preliminary effectiveness of Mind Meter, a virtual neuroscience-based biofeedback group intervention, for rural adults with chronic pain.
Methods
Twenty-nine rural-dwelling adults (mean age 44.9, SD 11.8) with chronic pain (≥3 months) were recruited from a pain management program and twenty-one participants completed a single-session virtual Mind Meter group, integrating pain neuroscience education and biofeedback via affordable equipment (pulse oximeters, skin thermometers). Feasibility was assessed by enrollment (target ≥50%), adherence (≥80%), and completion rates (≥75%); acceptability via a 10-item questionnaire (target ≥80% rating ≥4/5); and preliminary effectiveness via pre-post changes in heart rate, temperature, pain, and anxiety, analyzed with paired t-tests (adjusted P < 0.05).
Results
Enrollment was 22% (29/132 eligible), below target, while adherence reached 100%, exceeding goals. Acceptability was high, with 90.5% rating the intervention ≥4/5 (mean 4.3, SD 0.9), particularly for clarity of directions (95.2% ≥ 4). Statistically significant pre-post improvements occurred in anxiety (mean change −2.2, SD 2.4, P < 0.001, Hedge’s g = −0.886) and temperature (mean increase 4.6°F, SD 6.1, P = 0.003, g = 0.726); pain decreased (mean −0.8, SD 1.5, P = 0.025) but lost statistical significance after correction for multiple comparisons. Heart rate showed no change (P = 0.615).
Conclusion
Virtual Mind Meter is feasible and highly acceptable for rural patients with chronic pain, with promising reductions in anxiety and temperature. Lower than hypothesized enrollment warrants recruitment strategy-adjustments, while preliminary outcomes support further development.
Introduction
Chronic pain is a pervasive and debilitating public health issue, affecting approximately one in five Americans and significantly disrupting their daily lives. 1 As the United States population continues to grow and age, the prevalence of chronic pain and its associated impairments is projected to rise.2,3 The complexity of chronic pain necessitates multimodal, multidisciplinary treatment approaches that address both its physical and psychological dimensions. Among these, biofeedback stands out as a well-established, non-invasive psychological intervention that empowers individuals to modify physiological processesthrough real-time feedback. 4 Research consistently demonstrates that biofeedback reduces pain intensity, enhances coping strategies, and improves physical functioning and quality of life for individuals with chronic pain.5,6 Further, biofeedback can produce improvement in multiple pain related outcomes by addressing the contributions of the autonomic nervous system to pain propagation. 5 Systematic reviews further highlight its benefits, including reductions in depression, disability, and muscle tension, positioning biofeedback as a valuable adjunct to traditional pain management. 7
Despite its potential effectiveness, access to biofeedback remains severely limited, particularly for rural populations. Methods of biofeedback include monitoring autonomic (unconsciously controlled) functions including muscle tension electromyography, heart rate variability, breathing rate and galvanic skin response. This typically requires specialized training, software, and equipment, and is delivered in a one-on-one, in-person setting, often delivered by specialized providers in urban healthcare settings. 8 For rural patients, geographic isolation compounds this challenge, as long travel distances to reach healthcare facilities can impose significant physical, financial, and logistical burdens—particularly for those with chronic pain who require regular care. 9 Rural communities already face systemic healthcare disparities, including higher rates of chronic diseases, lower life expectancy, and shortages of specialized providers, all of which exacerbate inequities in pain management. 10 Many evidence-based interventions, including biofeedback, have yet to be widely adapted for virtual healthcare, leaving rural patients underserved and contributing to poorer health outcomes compared to their urban counterparts. 11
The COVID-19 pandemic illuminated the potential role of virtual healthcare in bridging such gaps. Digital health platforms have proven capable of delivering scalable solutions during crises and sustaining routine care in the post-pandemic era. 12 Virtual interventions offer unique advantages, including increased accessibility for remote populations, improved patient engagement, and greater flexibility in treatment delivery. 13 For chronic pain management, adapting biofeedback to telehealth platforms represents a promising strategy to overcome geographic and logistical barriers, ensuring timely access to evidence-based care. This is especially vital for rural patients, who often lack the resources and infrastructure to support in-person interventions. By leveraging affordable technology and scalable group-based formats, virtual biofeedback has the potential to reduce healthcare disparities, lower costs, and enhance patient outcomes—aligning with the Institute of Medicine’s call for equitable pain care regardless of location. 3
Building on this foundation, we developed “Mind Meter: Biofeedback for Chronic Pain,” a brief, neuroscience-based intervention initially delivered in-person within a group setting. Using affordable equipment readily available in outpatient settings, Mind Meter was piloted with adult females diagnosed with hypermobile Ehlers-Danlos Syndrome (hEDS; N = 8), demonstrating increases in thermal body temperature—a key factor in pain modulation—and improvements in patient wellbeing. 14 Following this success, we integrated Mind Meter into routine clinical care at the IU Health Pain Rehabilitation Program (PRP) in January 2024. A retrospective review after one year (N = 35) revealed clinically meaningful pre-post improvements in physiological and subjective symptom severity, with 97% of patients opting to participate and 100% completing the 2-hour intervention. 15 These findings affirm Mind Meter’s feasibility and efficacy in a controlled, in-person context. However, to address the unmet needs of rural patients, further innovation is required to extend this intervention beyond traditional settings.
Expanding access to biofeedback for rural populations necessitates piloting brief, affordable, and scalable virtual interventions. The current study builds on our prior work14,15 by adapting Mind Meter for telehealth delivery, targeting rural patients with chronic pain. This approach leverages simple-to-use equipment and a manual adaptable for allied health professionals, enhancing scalability and reach. Thus, the primary objective of this study is to explore the feasibility, acceptability, and effectiveness of administering virtual biofeedback in a group setting for rural adult patients with chronic pain conditions. By offering Mind Meter virtually and in a group format, we aim to overcome the barriers of distance, cost, and provider shortages, providing a novel solution to improve pain management equity. Accordingly, this research is guided by three aims:
Aim 1: Evaluate the feasibility of the Mind Meter intervention for rural patients with chronic pain. We hypothesize that the virtual group biofeedback intervention will be feasible, as evidenced by (1) enrollment (≥50% of potential rural participants choose to enroll), (2) treatment adherence (≥80% of enrolled participants complete the two-hour intervention), and (3) study completion (≥75% of participants complete pre/post intervention outcome measures).
Aim 2: Evaluate the acceptability of the Mind Meter intervention targeting rural patients with chronic pain. We hypothesize that ≥80% of participants will find the intervention acceptable, as measured by scores indicating adequate to good acceptance (ie, ≥ 4 out of 5) on the Mind Meter Acceptability Questionnaire.
Aim 3: Evaluate preliminary effectiveness data on the virtual iteration of the Mind Meter intervention for rural patients with chronic pain, specifically collecting heart rate, body temperature, pain, and anxiety. We hypothesize results will be statistically comparable to our in-person pilot study of Mind Meter 1 with clinically meaningful pre-post improvements in physiological and subjective symptom severity.
These aims will provide critical data to assess the potential of virtual Mind Meter as a scalable, equitable solution for rural patients, laying the groundwork for future research.
Methods & Materials
Overview
This feasibility study was approved by the Indiana University IRB. The present study involves recruiting rural patients presenting for pain management treatment at Indiana University Health in Indianapolis, IN for a single virtual session using the Mind Meter intervention. The Mind Meter intervention incorporates group neuroscience education with traditional biofeedback training. The present study pairs the reproducible structured Mind Meter intervention with the use of affordable biofeedback equipment that can be easily used in a virtual group format, reducing costs, and increasing scalability. Twenty-nine paticipants were enrolled in the intervention across five, one-time groups; twenty-one participants attended and completed the intervention Each group had a maximum of six participants. Pre-intervention baseline data were collected prior to the start of the intervention during the group. Post-intervention data were collected immediately post-intervention during the group. Follow-up data was collected one week post-intervention.
Setting
Participants were recruited after presenting for treatment at [Indiana University Health’s Pain Navigation Service (PNS) in Indianapolis, IN. PNS is an in-person multidisciplinary consultation clinic where patients are seen by a medical provider, psychologist, and physical therapist with chronic pain expertise. The psychology team currently completes approximately 15 PNS intakes per week with an estimated 40% of all patients presenting from rural areas.
Recruitment
Patients were invited to participate via flyer included in their intake process at PNS. Patients were also contacted by the research assistant (RA) if they had already completed PNS intake and consented to be contacted for future research opportunities. The recruitment flyer included eligibility information and a link to informed consent. Participants were required to electronically sign and date the consent form before participating in the study. Participants were given an opportunity to ask questions of the study personnel and were provided with a copy of the completed consent form by email. Participants were informed that they were able to withdraw from the study at any time and that withdrawing would not affect their clinical care. Participants were offered an incentive of one $25 Amazon gift card for attending the two-hour intervention and completing the follow-up intervention data 1-week post-intervention. .
Inclusion/Exclusion Criteria
Inclusion criteria were: (1) adults patients (age 18+ years), (2) patients who reported chronic pain (pain ≥3 months), (3) patients who were able to read and speak English, (4) patients who had access to reliable home internet, (5) patients who were rural-dwelling, and (6) patients who had not already received the intervention. To meet criteria for rural-dwelling, a participant’s primary residence needed to be located in a micropolitan or rural county in Indiana as defined by the 2020 US Census data. Live translation over a brief telehealth intervention would lengthen the time of the intervention and not all the self-report instruments used in the present study have been translated nor normed in other languages; thus, offering this intervention to patients who are not proficient in English was outside the scope of this project. Additionally, patients with preexisting conditions with symptoms including cognitive limitations were excluded. Of note, no patients were excluded due to cognitive limitations for this study.
Sample Size
We enrolled 29 participants over four months across five virtual biofeedback group meeting these criteria, of which, 21 attended and completed the scheduled virtual intervention. This sample size is comparable to the existing limited studies on group biofeedback. 30 Groups were scheduled once per month over the course of five months with a maximum of six participants in each group.
Intervention
The Mind Meter intervention includes a physician-led didactic on pain neuroscience and a psychologist-led didactic on biofeedback, followed by a guided autogenic relaxation exercise and collection of pre/post intervention data. The same providers delivered the intervention to each group. The intervention totals approximately 120 minutes, with the first 60 minutes covering Pain Neuroscience Education (PNE). Education emphasizes alterations in the nervous system that occur in chronic pain and the brain’s role in regulating the nervous system. The second half of the intervention includes a 20-minute didactic session covering an explanation of the history and use of biofeedback. The didactic session also includes a description of the application in a clinical setting and how the group delivery method differs. Participants are then instructed to assume a comfortable position and are led through a 10-minute guided autogenic meditation. Lastly, participants are given an opportunity to ask questions and reflect on their experiences in the group setting. Educational content is based on elements from Pain Reprocessing Therapy (PRT) and PNE curriculum.16,17 Adaptations necessary for virtual format included updating slides for the virtual platform, redesigning physical demonstrations, and teaching participants how to measure and report their own heart rate and thermal hand temperature. Participants received an email link to a 10-question acceptability questionnaire for follow up on acceptability several days after the intervention which required an additional 5-15 minutes.
Measures
Data was collected and managed using Research Electronic Data Capture (REDCap).18,19 Participants were asked to complete measures prior to the intervention, immediately post-intervention, and 1-week post-intervention. Feasibility was measured by recruitment proportion (percentage of approached patients who enrolled), treatment adherence (percentage of enrolled participants to complete the intervention), and study completion (percentage of participants to complete pre/post intervention outcome measures).
Acceptability was measured with the Mind Meter Acceptability Questionnaire (Appendix A). The Mind Meter Acceptability Questionnaire (Appendix A) is a 10-item measure created for the purpose of this research based on existing validated acceptability measures. It is used to evaluate treatment satisfaction and acceptability of Mind Meter that utilizes a 5-point Likert scale. Ratings were collected 1-week post-intervention. Overall and individual item scores ≥4 were considered “acceptable”. The Mind Meter Acceptability Questionnaire was administered electronically via email 1-week post-intervention.
Regarding secondary outcomes, the following variables were measured to assess participants’ biological response to the intervention: Edmonton Symptom Assessment Scale (ESAS), heart rate, and thermal hand temperature. Secondary outcome data were reported by participants to study personnel during the intervention.
Edmonton Symptom Assessment Scale (ESAS)
The full ESAS is a nine-item patient reported symptom numeric rating scale initially created and validated for palliative care patients. 20 The present study utilized an adapted version for chronic pain with five numeric rating scale (NRS) [0-10] items assessing the severity of common symptoms associated with chronic pain: pain, tiredness, anxiety, sadness, and overall well-being. Participants rated each item based on their pain, tiredness, anxiety, sadness and overall well-being in the moment. Higher scores indicated greater severity, including worse well-being. Verbal and written scores were collected pre/post intervention.
Peripheral Skin Temperature Measurement
Skin temperature data was collected pre/post intervention via patients following clinician instructions on how to use medical grade thermal hand thermometer (Bio-Medical Instruments Stress Thermometer SC911) and then displaying results on equipment to the Zoom screen for clinician to document.
Heart Rate Measurement
Heart rate data was collected pre/post intervention via patients following clinician instructions on how to use medical grade thermal hand thermometer (A&D Medical Fingertip Pulse Oximeter) and then displaying results on equipment to the Zoom screen for the clinician to document.
Equipment
After completing informed consent and prior to the virtual group session, participants were mailed the medical grade thermal hand thermometer and fingertip pulse rate oximeter. Patients also received printed instructions on how to use both pieces of equipment and how to use secure Zoom Health online platform. The RA contacted each registered participant to ensure they received the materials and had Zoom Health prepared for the intervention. Participants were trained on the proper techniques for data collection. All group sessions were attended by the RA who was available to individually help participants with Zoom connection and/or equipment issues.
Analysis
Summary statistics of patient characteristics and measure scores include mean, standard deviation (SD), minimum, and maximum. Feasibility analyses include descriptive statistics on participant enrollment, treatment adherence, and study completion. For exploratory effectiveness analysis, pre-post differences were compared by paired-samples Student’s T-tests, with no post - pre differences as the null hypothesis (two-tailed). P-values were adjusted using the Benjamini-Hochberg procedure to control the false discovery rate (FDR). Adjusted P-values <0.05 were considered statistically significant. Sample size for this study was chosen to provide reasonable estimates for our feasibility outcomes.21,22 With measures collected from a sample size of 21, we would have 80% power to detect only large effect size changes (Hedge’s g ≥ 0.7) in outcome measures. Analyses were conducted in IBM SPSS Statistics for Windows, Version 29.0.
Results
Sample Characteristics

Enrollment proportions were lower than the hypothesized proportion of ≥50%. Over four months, 29 of 132 potential participants (22.0%) enrolled. Treatment adherence rates were higher than the ≥80% hypothesized. Of 21 enrolled participants, all 21 (100%) completed the two-hour intervention. Study completion rates were also higher than the ≥75% hypothesized. Of 21 enrolled participants, all 21 (100%) completed the outcome measures.
Mind Meter Acceptability Questionnaire Responses

Response option was from 1 (“I don’t agree at all”) to 5 (“I totally agree”).*n = 19 for this question
Measures Summary, Mean (Standard Deviation)

Note: For wellbeing, higher scores imply worse wellbeing.
Paired-Samples Student’s T-Test Comparison of Change in Measures
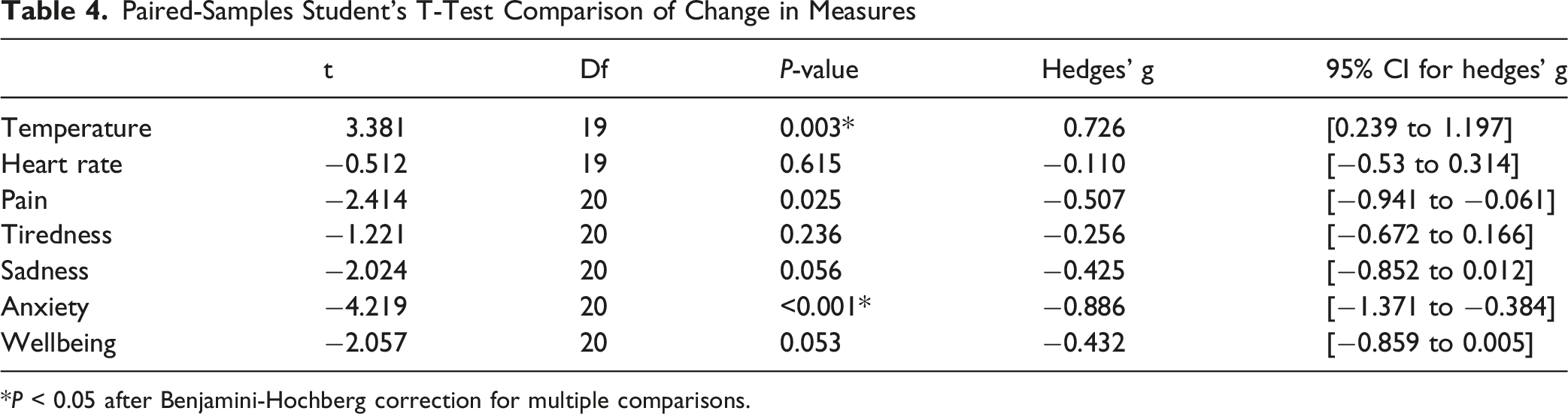
*P < 0.05 after Benjamini-Hochberg correction for multiple comparisons.
Discussion
This study was designed to assess the feasibility and acceptability of a novel virtual neuroscience-based biofeedback group in rural patients with chronic pain. We know that early activities, such as piloting intervention strategies and study logistics, gathering information about feasibility and acceptability, and gathering feedback and making iterative refinements, produce highly valuable information for the scientific community and are critical for efficiently constructing an intervention that is effective and valued. Research on virtual biofeedback service delivery for chronic pain is scarce and our research had several key findings. Overall, we found that Mind Meter, which has already been established as a valid brief biofeedback intervention, can be successfully adapted to a virtual format with high acceptability. A few specific findings include that first, recruitment was more challenging than anticipated, with only 22.0% of eligible patients consenting. Second, adherence and completion rates were higher than anticipated, with 100% of attending participants completing both the intervention and the follow up measures. Third, acceptability was high, with 90.5% of participants rating acceptability ≥4 out of 5. We encountered several challenges in the virtual delivery of Mind Meter related to participation, equipment and technical factors that may have affected outcomes and are discussed in detail below. Finally, preliminary analysis of potential future outcomes for a fully powered trial found statistically significant changes in hand temperature and anxiety, with large effect sizes.
Our lower-than-expected enrollment proportion of 29 participants out of 132 contacted (22%) is likely multifactorial. While reasons for declining participation were not collected, some possibilities include schedule conflicts and lack of interest. The intervention was offered on a weekday during daytime hours and required active participation, which may limit those working full time. Increased enrollment may be possible in a future trial if a variety of timeslots, including evenings and weekends, are offered. Despite these lower-than predicted enrollment proportions, our enrollment rate of 5.3 participants/month was favorable compared to the <1 participant/site/month benchmark that has been reported for similar trials, suggesting our recruitment benchmark was likely set too high23,24 Taken together, this feasibility data suggests that our recruitment processes should be adequate to support a fully powered trial as long as we have a large enough catchment.
While adherence was high, of the 21 people that participated, ten participants needed to be contacted more than once (for various reasons such as not being at home with materials when RA called, not answering phone, etc) to be walked through how to use the materials. Some participants were not instructed on how to use the materials before participating in the group due to not answering the phone. Despite this, the 100% adherence rate was exceptional. This was aided by the requirement of completing the final survey to receive the incentive payment and we would expect to use a similar incentive schedule for a fully powered trial.
The virtual Mind Meter biofeedback group intervention was well-received by participants, as evidenced by post-intervention questionnaire scores averaging ≥4 out of 5 across all categories. This high level of acceptability aligns with findings from other pilot studies of digital mental health interventions, particularly those leveraging virtual platforms for psychological care. For instance, a prior study (N = 22) investigated home-use and portable biofeedback devices in a remote program for managing chronic pain. The researchers demonstrated that a majority of participants experienced improvements in both anxiety and pain levels, suggesting the acceptability and effectiveness of the intervention in chronic pain management. 25 Another recent study (N = 52) found that 43% of participants who used an app-based HRV biofeedback intervention endorsed that they would likely recommend it to someone else. 26 Additionally, higher engagement with the app was associated with greater benefits; thus, when individuals were able and willing to use the devices regularly, the intervention was more positively received. The consistency of these findings suggests that the virtual Mind Meter intervention’s acceptability is comparable to other innovative digital health pilots, particularly those integrating biofeedback or virtual delivery.
Despite the complexity of the Mind Meter intervention, which involved a virtual platform and two separate monitoring devices, participants found the directions clear and understandable. This is reflected in the high post-intervention survey completion rate (4.8 on question asking about clarity of directions), which mirrors trends in other telehealth studies. For example, Donnelly et al. reported high usability and acceptability, with detailed, clear instructions facilitating engagement despite technological complexity. 27 The clarity of instructions in the Mind Meter intervention likely contributed to its accessibility, a critical factor in pilot interventions where participant burden can undermine feasibility. Participants also reported that the intervention content was applicable and useful, with favorable responses to the virtual group setup and the 2-hour format. The positive response to the group format in the Mind Meter intervention may reflect the social connection facilitated by virtual platforms, a factor often cited as enhancing engagement in digital mental health interventions.
The lowest-rated acceptability question pertained to the virtual format itself, which warrants further exploration given that the primary innovation of this intervention is its virtual delivery compared to the in-person Mind Meter program. While still rated positively (≥ 4 out of 5), this lower score suggests potential challenges in fully translating the in-person experience to a virtual setting. Recent literature highlights that virtual formats, while scalable and accessible, can sometimes be perceived as less engaging or personal compared to in-person interventions. For example, a systematic review of digital mental health interventions outlined barriers to and facilitators of user engagement. Researchers noted that some participants prefer face-to-face interaction to facilitate social connectedness, which may influence acceptability ratings. 28 Similarly, a study on the acceptability and usability of digital health interventions found that personalization of treatment and personal support are major components to the success of digital health interventions. 29 The slightly lower rating for the virtual format in the Mind Meter intervention may reflect these dynamics, but the overall high acceptability suggests this is not a major barrier to engagement.
The acceptability results provide insight into the intervention’s potential success. High acceptability is a strong predictor of intervention adherence and engagement, which are critical for efficacy in larger trials. A bibliometric analysis of digital mental health interventions emphasized that acceptability is a multifaceted construct influencing sustained adoption, with pilot studies like this one playing a key role in refining interventions before scaling. 30 The positive feedback on content applicability and usability aligns with findings from a meta-review of digital health interventions, which reported that flexibility, functionality, content, and interface are valued by participants. 29 Thus, research suggests that participants value applicable and personalized interventions, which likely contribute to sustained engagement and positive outcomes. However, the slightly lower rating for the virtual format suggests that future iterations should address potential barriers, such as enhancing the sense of personalization or interactivity in the virtual environment as well as addressing technical issues. 28
The fact that the virtual format received the lowest acceptability rating should not be overemphasized, as it still scored highly and did not detract from the overall positive reception. Literature suggests that initial skepticism toward virtual formats often diminishes with increased familiarity and technological refinement. For instance, prior research suggests that while participants initially may have negative expectations regarding virtual formats, including skepticism about the helpfulness of the intervention, this can largely decrease once the intervention is delivered and therapeutic relationships are established remotely. 29 These findings suggest that the virtual Mind Meter intervention’s lower rating for the virtual format may reflect a learning curve rather than a fundamental flaw, and targeted improvements—such as enhanced user training or more immersive virtual elements—could further elevate acceptability.
Regarding feasibility of tracking the physiologic markers of peripheral temperature and heart rate utilizing the equipment described above, we discovered several potential barriers. A few participants reported difficulty attaching the probe for peripheral temperature to their digit and required additional instruction and guidance during the session. We embedded extra time in the intervention in anticipation of this and would continue to do so in future sessions. Additionally, we utilized a finger pulse oximeter which reported both oxygen saturation and heart rate. A few patients initially reported their oxygen saturation when collecting heart rate data. This led to a change in the collection process after the initial session where patients were thereafter instructed to hold up their device to the camera so that a clinician could collect the information to minimize the chance of error. There were only very small changes in HR, with an effect size around 0.1. There are a few potential confounders here to consider. Underlying medical comorbidities such as arrhythmias or medications that may affect heart rate were not inquired about or noted. We believe these challenges and the minimal observed change in HR, suggest that collection of this variable can be omitted from future iterations of the virtual Mind Meter intervention. There were also 2 instances of device failure. One participant identified a non-working thermometer prior to the intervention and was mailed a new one. Overall, the technical challenges we encountered with virtual setup occurred at a low enough rate and did not seem to greatly impact patient experience as demonstrated by a mean score of 4.8 in the “Directions were easy to understand” survey item.
The virtual format revealed several unexpected opportunities for troubleshooting which should indicate an extended timeline in planning of further research. On two occasions, participants experienced problems with internet connection and Zoom Health utilization. In those instances, the RA was able to connect with each patient to ensure adequate connectivity to continue to participate. One scheduled session with 5 participants enrolled had to be postponed due to an unexpected mail delay in which participants did not receive their equipment. All patients were able to participate at the rescheduled time.
As is evident, the virtual adaptation of the Mind Meter intervention introduced layers of complexity. A notable success was its ability to offer a solution to the problem of access in chronic pain care to rural dwelling individuals. Mind Meter has potential to be added to the chronic pain treatment option menu as a psychological intervention that includes objectively observable biological phenomena. This may be more appealing for patients who have already attempted traditional talk therapy and are open to a new non-pharmacological approach. Future research of a virtually delivered Mind Meter biofeedback group should include a larger sample and a control group to be able to draw conclusions about true intervention effect size and pain related outcomes. While the sample size was adequate for feasibility aims, the study was underpowered to draw meaningful conclusions from the ESAS outcomes. Nonetheless, the statistically significant changes in both temperature and anxiety and promising trends in pain, sadness, and well-being suggest that these outcomes may be worth exploring in a larger trial. These results are consistent with our prior research on an in-person version of Mind Meter, in which we saw a reduction in pain intensity of over 1 point, along with clinically important and statistically significant changes in sadness, anxiety, and well-being. 15 Lastly, the lack of a comparator group further limits interpretability of these findings as there is no control to account for the placebo effect. Due to the brief duration of the intervention, collecting pain related outcomes and autonomic measures virtually from a waitlist control group would be appropriate and helpful in understanding the true effect size of this intervention.
Conclusion
We found that our novel virtual neuroscience-based biofeedback intervention had high adherence, completion, and acceptability in rural patients with chronic pain. Recruitment was achievable, albeit at a lower rate than hypothesized. Preliminary effectiveness data from this pilot is encouraging that this intervention may lead to clinically meaningful improvements in target symptoms, though this study was not powered to definitively test effectiveness.
Footnotes
Ethical Considerations
This work was approved by the Indiana University Institutional Review Board (IRB): 23808. Participants provided written electronic consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a small internal pilot grant by the Indiana University School of Medicine Department of Psychiatry.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon reasonable request from the corresponding author.