
Abstract
Background
As interest in non-pharmacologic treatments for migraine prevention increases, there is an urgent need to evaluate these treatments in well-designed randomized trials. However, designing a “control” for non-pharmacologic treatments is complex. One possible solution is to design credible educational programs to use as comparators which partially control for natural history, patient engagement, attention and positive expectancy.
Objective
To develop and validate through a modified Delphi process a “Headache Health Education” (HHE) program to be used as the control arm in a pilot study of multimodal chiropractic care for episodic migraine.
Methods
Leveraging existing patient educational materials, we drafted an initial HHE program with 14 modules, each covering a different migraine-related topic. Designed to be delivered by research personnel in a one-on-one video conference, each module provides education using a slide deck and guided conversation that is grounded in adult learning theory. Furthermore, to engage participants, the script-based sessions are informed by the psychological implications of polyvagal theory and motivational interviewing. The program was validated using a modified Delphi process. Modifications were made to the program based on the ratings and feedback, and a second round of review was then performed.
Results
Initial endorsement of the HHE program was generally supportive but included considerable variability. After program refinement, endorsement improved with much lower score variability. Key improvements included the addition of 2 topics, selection of new videos, and training for research assistants/associates in how to use conversational style and specific prompts to engage participants.
Conclusion
Initial development and validation of an HHE program to use as a comparator in trials of a non-pharmacological treatment for migraine has been completed. Future analysis will examine the fidelity and acceptability of the HHE program when used as a comparator in a randomized controlled trial of multimodal care for migraine.
Introduction
Migraine refers to a complex neurological disorder causing recurrent moderate-to-severe headaches, often accompanied by other symptoms such as photophobia, phonophobia, nausea, and fatigue. 1 Migraine is one of the leading causes of disability worldwide. 2 While pharmacotherapy is often a first-line treatment, there is growing interest in non-pharmacologic and integrative approaches to manage migraine attacks. 3 National surveys indicate that approximately half of US adults with migraine report using complementary and integrative health (CIH) therapies, such as mindfulness meditation, Cognitive Behavioral Therapy, lifestyle changes, and manual therapy, including chiropractic care.3,4
To determine the efficacy of potential treatments for migraine, well-designed randomized trials are needed where the intervention of interest is compared to a “control” arm. In studies of pharmacological agents, the “control” is often a placebo pill or saline solution which looks identical to the active treatment. Blinded placebos reduce the risk that therapeutic effects observed in active treatment arms are misattributed to other factors such as expectation of benefit or caring attention of professionals.5,6 In contrast, for CIH interventions, it may not be possible to use placebos or to blind participants to treatment assignment. 7 Further complicating control group options is the multimodal nature of many CIH therapies. For example, a single multimodal chiropractic session can include spinal manipulation, joint mobilization, education, myofascial techniques, posture correction, stretching and strengthening exercises.8,9 Developing credible and inert placebos for each of these components, in addition to controlling for emergent psychosocial therapeutic context effects, is not feasible.7,10 One potential option for a control group in CIH trials is to develop credible patient educational programs provided by a caring professional who elicits patient engagement that generates some expectancy of benefit. 11 These programs engage participants to control for key contextual effects, such as attention, time, and expectancy. 9 They also may provide therapeutically valuable information to participants without activating the specific physiological mechanisms thought to be influenced by specific CIH therapies.
As part of a National Institute of Health/National Center for Complementary and Integrative Health (NIH/NCCIH)-funded pilot study evaluating a multimodal package of chiropractic care for episodic migraine, we developed a Headache Health Education (HHE) program to use as a control intervention. In this paper, after briefly outlining the overall goals of the study, we describe the development of the HHE program, including the theoretical foundations of the program, the assembly of a subject matter expert (SME) panel, and the use of a modified Delphi process to validate and finalize the program. We conclude with a discussion of the strengths and limitations of this educational program, along with the potential application of the HHE program for future research studies.
Methods
Parent Trial Design
The development of the HHE program was part of a two-site, two-arm, randomized, controlled pilot trial designed to determine the feasibility and final design of a future full-scale, multi-site efficacy trial (NCT06229834). The future trial will compare the effectiveness of a validated multimodal chiropractic care (MCC) intervention vs HHE in reducing migraine frequency among individuals with episodic migraine. Details on the design and conduct of the pilot study are briefly summarized below.
The pilot includes 2 sites selected because they are representative of prospective sites in a subsequent large-scale trial: VA Connecticut (VACT) and Mass General Brigham (MGB), a large academic medical center. This study is approved by the WCG Institutional Review Board. Sixty individuals (30 per site) aged 18 to 65 years who have been diagnosed with episodic migraine and report 4 to 13 migraine days during the run-in period are being randomized (1:1) to either MCC or HHE. Individuals on medications for migraine or other pain conditions are required to be on a stable dose for at least 2 months prior. Briefly, exclusion criteria include recent use of chiropractic care, cognitive behavioral therapies, botulinum toxin or neuromodulation devices; diagnosis of medication overuse headache; head or neck trauma within the past year causing neurological or musculoskeletal signs or symptoms requiring treatment; recent psychiatric hospitalization; presence of carotid bruits; current alcohol or substance use disorder; significant cognitive impairment; currently pregnant or intention to become pregnant in the next 3 months; history of carotid or vertebral artery dissection; or the presence of contraindications for spinal manipulation or mobilization.
The study duration is 24 weeks including a 4-week run-in phase where participants complete daily diaries to confirm migraine frequency and ability to complete daily diaries, a 16-week intervention period, and a 4-week follow-up period. Participants who remain eligible after the run-in are randomized to either 14 visits of one-on-one multimodal chiropractic care or 14 sessions of one-on-one HHE. Participants were allowed to continue other treatments (eg, medications) prescribed to them prior to study enrollment. Given that this is a pilot study, primary outcomes focus on well-defined feasibility metrics related to recruitment rate, retention, adherence to interventions and assessment protocols.
Initial Development of the Headache Health Education Program Content
The development and validation of the HHE program included several key steps. First, we examined existing educational materials from 2 sources: those used by clinicians at the Osher Clinical Center for Integrative Health at Brigham and Women's Hospital who frequently treat migraine patients 12 and existing patient educational materials from societies such as the American Migraine Foundation and American Heart Association. Next, we assembled a team with a wide range of educational backgrounds, skills and professional experience to create version 1.0 of the HHE program. This team included an occupational therapist and health coach (MBS) and a clinical health psychologist and coach (RQW); both have backgrounds in patient education, communication, and migraine. Moreover, we included researchers with backgrounds in integrative medicine and non-pharmacological or integrative therapy approaches to pain management (PMW, DMV, RQW) and migraine (PMR). Over the course of several months, the team collaborated in drafting an initial version of the program including Power Point slides and accompanying scripts to guide each of the 14 interactive educational sessions.
Theoretical Underpinnings
Team members with expertise in patient engagement, communication, and adult education (MBS, RQW) drafted the modules using several key principles. First, to support rapport with participants and increase their engagement, we crafted scripts that embodied several of the foundational qualities that form the “spirit of motivational interviewing”, specifically, partnership, acceptance, and compassion. 13 We also embedded language using core skills from motivational interviewing to cultivate engagement; these included open questions and summaries. We purposely did not embed affirmations, reflections, or empowerment strategies from motivational interviewing, as the intention of the HHE program is to provide education in an engaging way, but not to empower behavioral change.
In drafting the HHE modules, we also followed core principles to enhance learning that were widely disseminated in tandem with polyvagal theory. In particular, we aimed to promote a feeling of safety for the participants within the education session.14,15 While the neurophysiological components of Polyvagal Theory have been debunked, the psychological safety implications remain. 16 Specifically, we aimed to provide adequate context to support participant self-regulation by providing a clear agenda in lay language and checking in with the participant after each segment to see how the information landed with them. We also worked with the research assistants/associates (RAs) to convey social signals of caring and connection, along with respect for participant choice or autonomy. Through the creation of a safe context, participants are more likely to better engage in education and demonstrate enhanced learning. 15
In addition to supporting learning through these polyvagal strategies, we used core principles of adult learning theory, particularly Knowles’ constructivist theory of andragogy.17,18 This and other adult learning theories emphasize the natural learning process wherein knowledge is provided to a learner in a circular and reciprocal manner through collaboratively sharing information that the learner can apply to their own lived experience. In this view, the learner is an equal contributor to the learning process rather than a passive recipient of information. First, we considered participants as self-directed learners whose individual experiences, needs and interests facilitate learning. Second, we repeatedly invited participants to link the material presented to their own lived experiences and existing knowledge base. Third, we surmised that participants who enrolled in the study had a specific need to learn about migraine and that need generated a readiness to learn.
Structure of HHE Sessions
All sessions begin with a brief check-in, asking about the participants’ prior week, and following up on any questions that emerged regarding material from the last session. Next, RAs provide an overview of the day’s session. These introductory steps are intended to create a clear context for the session and socially signal a supportive connection, both of which help participants settle into a state that best supports participant engagement and enhances ability to learn. 15 In the spirit of motivational interviewing, RAs nonjudgmentally ask HHE participants to describe what they already know about the session topic, before any information is provided. This question conveys respect of participant’s lived experiences and existing knowledge base, the RA’s desire to serve as a collaborative partner rather than expert, and also supports the participant’s autonomy. 13 This patient-centered collaboration and clear provision of choice are purposed to further help participants self-regulate. 18 Information is often provided via a short video, and there is a brief discussion led by the RA asking the participant open questions about new things they may have learned or personal experiences relevant to the topic content. For example, in Session 6, “Work, Everyday Activities and Migraine”, the participant is asked, “Can you tell me about a time when you had to tell your boss or others that you could not perform your duties due to a migraine attack?” Asking participants such questions intentionally cultivates their learning by making the topics personally relevant to them and inviting them to integrate new information into what they already know from their own experiences – both are key components of adult learning theory.17,18 The HHE sessions end with a reminder about the next scheduled sessions. If participants are unable to make the session or do not attend, the RA will try to reschedule the session to complete all 14 sessions within 16 weeks.
Validation and Further Development of the Headache Health Education (HHE) Program
The validation process of the HHE program was based on the Delphi method, a systematic, consensus-building process using the collective and iterative input of panel members. 19 Key steps in the Delphi process included: (1) drafting version 1.0 of the HHE program; (2) developing a feedback template that includes both numerical scoring and qualitative comments on multiple aspects of the program to allow for assessment of agreement among members of the panel of experts; (3) identifying a panel of clinicians with expertise in the evaluation, management, and education of persons living with migraine to evaluate the program; (4) sharing version 1.0 of the HHE program for the first round of anonymous scoring and feedback; (5) collecting and synthesizing feedback from subject matter experts (SMEs); (6) conducting a concurrent virtual SME panel meeting to review and discuss the feedback; (7) integrating feedback provided by expert panelists to draft a version 2.0 of the HHE program; (8) sharing version 2.0 for the second round of anonymous scoring and feedback from the SME panel; (9) collecting and synthesizing the second round of feedback; and (10) integrating feedback into a final version (3.0) of the HHE program. Details of key steps are below, and the final version of the HHE program is described in the results.
Scoring System and Feedback Template
The scoring system and feedback template used for the Delphi process were based on prior templates used for validation of other non-pharmacological interventions.9,20,21 The final form included 5 statements to be rated on a 7-point scale ranging from 1, meaning “strongly disagree,” to 7, meaning “strongly agree.” Instructions also asked SMEs to provide the rationale for their ratings in the comments section below each question box. The 5 statements were: (1) The HHE protocol is reflective of an evidence-informed approach for education of episodic migraine headache participants; (2) The HHE protocol is feasible to carry out by research assistants/associates (RAs) without additional post-graduate training; (3) The HHE protocol accurately represents a practical approach to education of episodic migraine participants; (4) The HHE protocol lacks an evidence-based component that should be included (reverse-scored); and (5) The HHE protocol appears safe. The fourth statement was reverse-scored to improve the reliability of the responses and decrease response bias. In addition, for each of the HHE sessions, SMEs were asked to provide any specific edits or comments they had about the slides to be shown to participants and the scripts to be used by the RAs leading the interactive HHE sessions.
For our study, a decrease in range and in variability of scores from the first to second round was considered to indicate consensus. Additionally, written feedback was used to determine if additional modifications needed to be made.
Delphi Panel and Meetings
The Delphi panel included 9 experts with diverse expertise such as clinical neurology and migraine, patient education, chiropractic care, clinical trial design, epidemiology and biostatistics, and integrative medicine. Once all experts provided feedback on the program, the study team summarized the findings, including calculating summary statistics for the numerical scores and synthesizing qualitative feedback. The de-identified findings were shared with the SME panel before the virtual panel meeting. Full findings were briefly summarized at the meeting, and the discussion focused on areas with the lowest endorsement and the highest level of variability. Findings and feedback from the meeting were used to draft version 2.0, which was then sent back to the panel (with changes highlighted) for the second round of evaluation. Repeating the same process as described above, the research team reviewed all feedback and created an implementation plan.
Finalization of the HHE Program and Training
Once the HHE program was finalized, including slides and scripts, RAs were trained to deliver the HHE program. Study staff attended an initial session led by an expert in qualitative methods (KK) who provided advice on interacting with participants, including the importance of asking open questions as worded in the scripts, and providing summaries to participants (core skills used in motivational interviewing) as well as displaying a warm and respectful demeanor towards study participants. RAs practiced delivering each of the 14 HHE sessions with study team members serving as mock study participants.
In parallel with fidelity monitoring processes in the MCC group, the HHE group is monitored throughout the trial by having a fidelity monitor attend ∼10% of the HHE sessions. As shown in Supplemental Figure 1, we developed a brief checklist to assess both content fidelity as well as communication style. Fidelity at both sites is being monitored by one of the study investigators (PMR). If an RA is not adhering to the protocol for either content or communication style, retraining will occur.
Results
Delphi Panel Results
Summary of Expert Panel Responses From Round 1 and Round 2 of the Delphi Process. A Score of 1 Indicates “Strongly Disagree” While a Score of 7 Indicates “Strongly Agree”
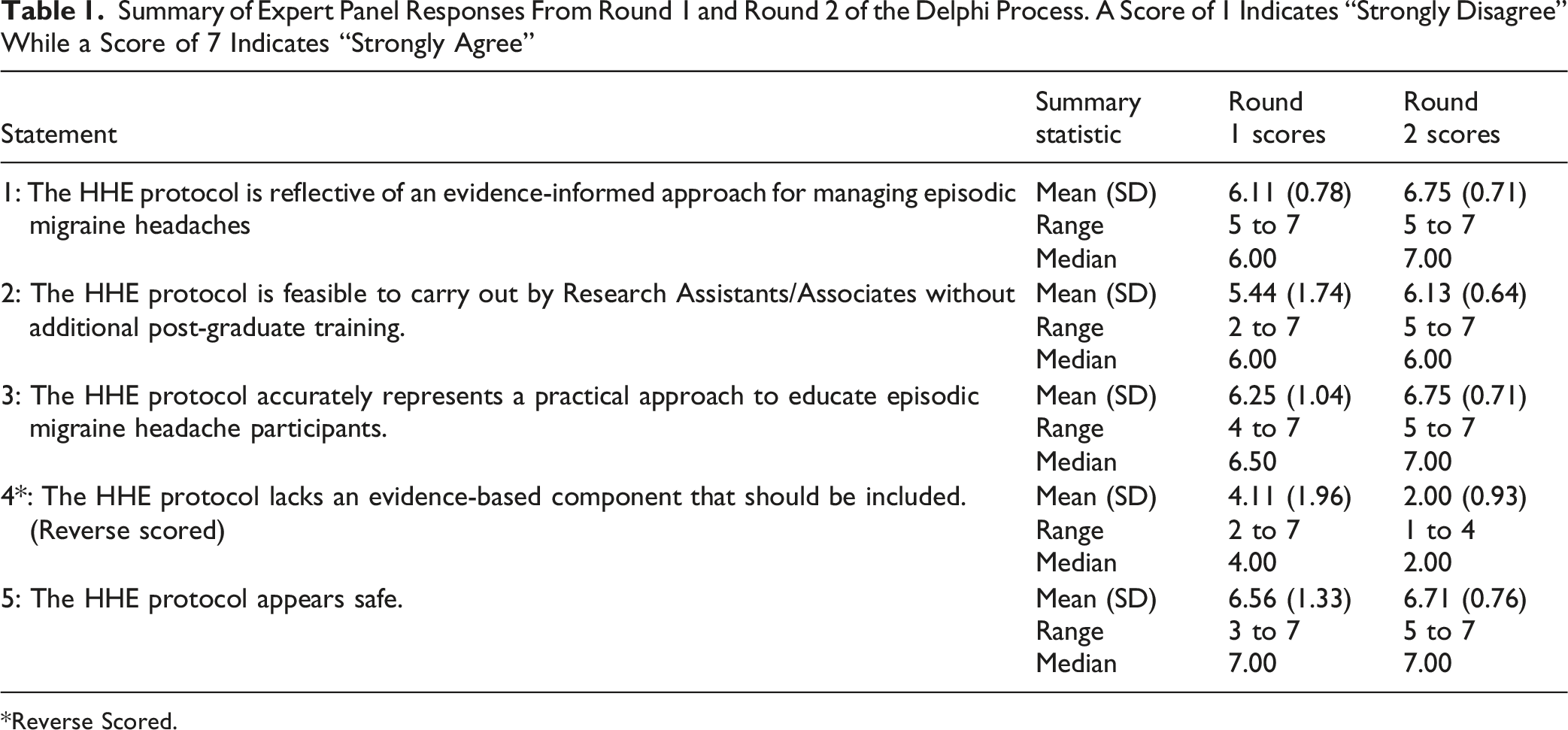
*Reverse Scored.
Statement 2 focused on the feasibility of the HHE protocol being delivered by RAs. As described in their open-ended comments, some SMEs rated Statement 2 lower as they believed, “while they do not need post-graduate training, the RAs will need additional training and will also need to ‘role play’ this a few times to become comfortable with the topics and discussions.” Several potential solutions were discussed by the SME panel, and implemented during the revision process, including: (1) addition of text to session scripts to clarify the role of the RA; (2) encouraging participants to speak with their healthcare providers if participants’ asked questions regarding material not covered in session; and (3) practice sessions for the RAs with “mock” participants. In round 2 of the Delphi process, average scores improved for Statement 2, and their variability decreased (Table 1).
Statement 4 focused on the evidence-based components of the HHE protocol. Experts highlighted that the sessions were missing information on medications, devices, and use of other integrative therapies. In addition, some experts noted that a few specific components lacked adequate evidence; these included instructions to “avoid” certain foods, and a video on breathwork. To illustrate, one expert stated, “the session on breathwork, for example, does not have an evidence-based component and I feel there needs to be more substantiation around this element.” Based on these expert panel suggestions, the final list of topics was modified to include 2 new topics: the SEEDS of migraine management – sleep, exercise, eating healthy, dehydration/diary, and stress management – and connections between migraine and the neck. The study team also identified new videos, including one demonstrating box breathing for Session 9, “Stress and the Relaxation Response.” In round 2, scores and their variability improved for Statement 4, supported by comments such as “the material has been reviewed to reflect evidence-based components across questions and in the presentation style.”
In addition to the concerns outlined above, specific to Statements 2 and 4, feedback from round 1 of the Delphi process identified additional modifications that were made. These included: (1) clarification of the sources of the videos and photos on the slides; (2) diversification of video sources while leveraging existing patient education videos from Mass General Brigham; and (3) modification of the script to prompt RAs to ask, “What do you already know?” prior to video viewing to activate knowledge and convey respect for the participant’s autonomy and existing knowledge. 13
Content of HHE Program
Topics for the 14 Sessions of the Headache Health Education Program
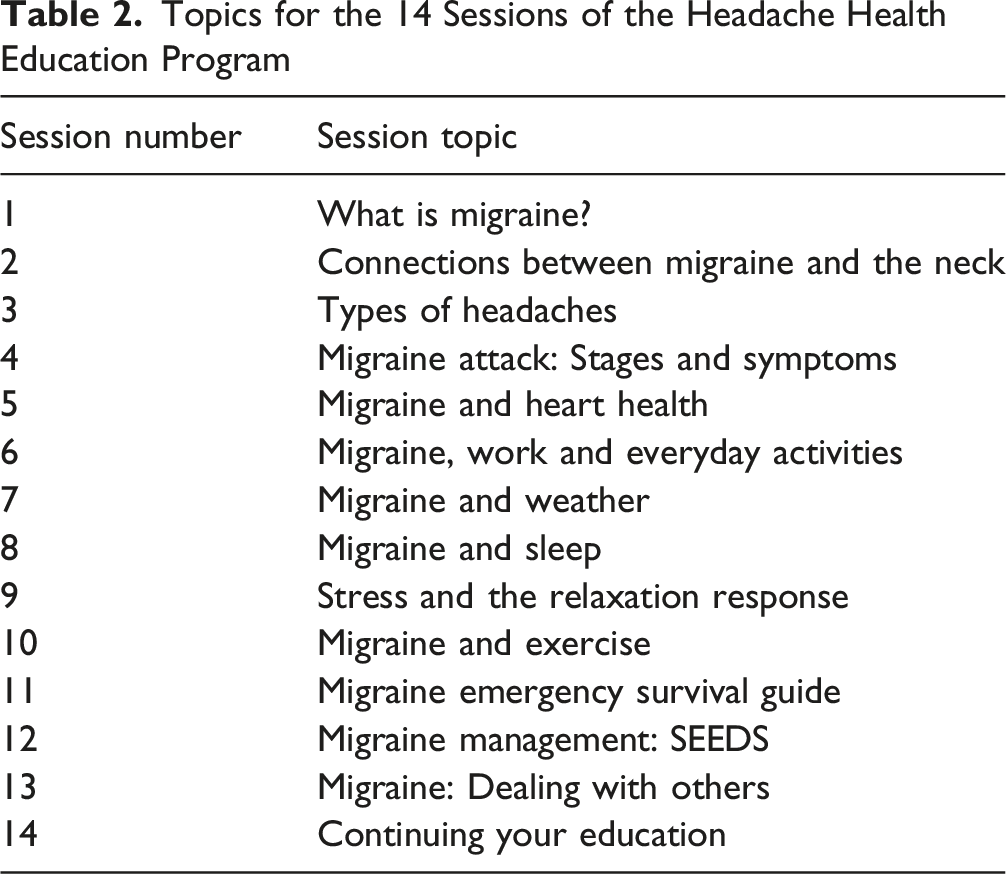
Each weekly session features educational material developed by our study team using resources from the American Migraine Foundation, the American Heart Association, the Association of Migraine Disorders, Mass General Brigham, Veterans Health Administration VA/Department of Defense (DoD) Headache Clinical Practice Guideline, and other sources, accompanied by time for questions and discussions. In each one-on-one session, RAs are provided with a slide deck while also using a script that is embedded with prompts to engage participants and provide education based on adult learning theory. The PowerPoint slide deck for Session 7: Migraine and Weather is provided in Supplemental Figure 2 as an illustrative example of the overall format of a typical session.
Discussion
We developed and validated a Headache Health Education Program, guided by a Delphi process, to be used as the control in a non-pharmacologic intervention trial for migraine. This comparator was designed specifically to be delivered by trained RAs to control for multiple non-specific factors, including natural history, attention, time, patient engagement, and positive expectancy. Overall, initial endorsement of the HHE program was strong, but variability in SME ratings was a concern. Ratings and variability improved in round 2 of the Delphi process. The final version of the HHE program included 14 modules, each covering a different topic, in the form of a PowerPoint presentation and accompanied by a script with embedded prompts to engage patients and leverage tenets of adult learning theory and motivational interviewing.
We grounded the program in 3 of 4 components of the “spirit of motivational interviewing,”: partnership, autonomy, and compassion. We omitted the fourth component - empowerment – since this comparator was designed to provide education without catalyzing behavior change. Similarly, we did not use empowerment strategies from motivational interviewing as the intention of the HHE program is to provide education in an engaging way, but not to empower behavioral change. For this same reason, we originally avoided almost all open questions that pull for change talk, but the expert panel during the Delphi process was concerned that participants would not get enough benefit from the HHE program. Hence, we tried to balance open questions that cultivate change talk with those that are more likely to elicit neutral or sustain talk. We acknowledge that these modifications may potentially result in behavioral changes among some participants. As described below, analyses are planned to formally explore the impact of the HHE program on behavior changes and clinical outcomes (such as migraine days).
Often, trials of non-pharmacologic interventions employ “usual care” as a comparator or provide control patients with printed educational.23-26 However, some studies have designed more complex comparators to control for factors such as attention but are not designed to impact clinical outcomes. For example, Schuman-Olivier et al, in a recent 2 × 2 factorial trial of 8-week Mindfulness-Based Stress Reduction with concomitant Respiratory-gated Auricular Vagal Afferent Nerve Stimulation (RAVANS) transcutaneous auricular vagal nerve stimulation for migraine, investigators used a “Nature Education control”, which involved watching nature videos, as one of the components of the control group. 27 Building on prior studies, we aimed to design a comparator that would engage participants, relay useful information, and provide some control for expectation by providing educational material, and attention through additional contacts with RAs trained to demonstrate strong communication skills and convey cues for participant safety to enhance engagement and learning. However, it should be noted that the trial was not designed as a comparative effectiveness trial, and thus the HHE program was not specifically designed to improve clinical outcomes.
Strengths and Limitations
Our study has several methodological strengths. First, our HHE program was validated through a Delphi process and leveraged pre-existing materials from credible sources such as the American Migraine Foundation. This approach enabled the development of the program in a cost-efficient manner, while ensuring content validity and that the material was designed for patient use. Second, by grounding the education modules in adult learning theory with attention to psychological safety, and some aspects of motivational interviewing, we aim to enhance the educational experience without necessarily catalyzing significant behavior change. Third, throughout the trial, we are tracking clinical outcomes (such as migraine days), and use of other therapies, medications and lifestyle habits to gain insights into possible impacts of the HHE program. Examining within-group changes will allow us to determine if the HHE intervention may have impacted clinical outcomes or elicited lifestyle changes (such as changes in exercise) that may impact clinical outcomes. Our qualitative interviews will also inquire about the impact of the HHE on habits and lifestyle changes. Finally, fidelity is being monitored to help achieve consistent content delivery. The use of multiple RAs will parallel the experience in the chiropractic care arm (where multiple providers are involved) and represents a scalable approach for a future fully powered trial.
Despite these strengths, several limitations should be considered. First, the HHE program was designed to control for some key variables, such as natural history, attention, and positive expectancy, but was not designed to control for all potential influences. While not explicitly designed to be therapeutic, the program could result in some lifestyle, behavioral, or mindset changes that may impact clinical outcomes. Second, the program itself is being delivered by multiple RAs across 2 study sites which may introduce heterogeneity. This, however, is balanced by an increase in generalizability and thus rigor. Third, assessment of the acceptability of the program to participants and the feasibility and fidelity of intervention delivery have not yet been determined. Our ongoing pilot study will provide metrics on retention in the HHE group and number of sessions attended as well as qualitative feedback from participants to address these components.
Conclusion
A HHE comparator program developed for use in a pilot RCT study of chiropractic care for episodic migraine was endorsed to have content validity. This comparator may also be useful in other trials of non-pharmacological treatment for migraine. Data from the ongoing randomized clinical trial will provide important information on fidelity of HHE delivery and the feasibility and acceptability of the HHE program. Qualitative interviews with study participants will provide additional insights into patient experiences in the program. These findings will inform future iterations of the HHE program.
Supplemental Material
Supplemental Material - Development and Validation of a Headache Health Education Program to Serve as a Control Intervention for Non-Pharmacological Studies in Migraine
Supplemental Material for Development and Validation of a Headache Health Education Program to Serve as a Control Intervention for Non-Pharmacological Studies in Migraine by Kristina Twaalfhoven, Ruth Q. Wolever, Meredith Beaton-Starr, Carolyn Bernstein, Karen Kilgore, Anthony J Lisi, Matthew H. Kowalski, Cynthia R. Long, Dennis Muñoz-Vergara in Global Advances in Integrative Medicine and Health
Footnotes
Ethical Considerations
The multisite study was approved by the WCG Institutional Review Board #20243139; both Mass General Brigham and VA Connecticut IRB’s formally ceded to WCG’s oversite.
Author Contributions
PMW, PMR, JJS, MHK, and AJL conceived of and designed the overall study, and obtained funding. PMR, DMV, RQW, and MBS contributed to the content and conceptual framework of the HHE intervention. KT, RQW, PMR, and PMW contributed to first draft of the manuscript and interpretation of data. MBS, CB, KK, AJL, MHK, CRL, DMV, KM, VN, MR, RV, and JJS critically revised the manuscript for important intellectual content and assisted with interpretation of data. KT, PMR, and PMW take responsibility for all aspects of the work integrity and accuracy. All authors approved the final version of the manuscript to be submitted.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by National Center for Complementary and Integrative Health (NCCIH) (R01 AT012228) (PMW, PMR, JJS—MPIs). The funder did not have a role in the study design; in the collection, analysis, and interpretation of the data; in the writing of this manuscript; and in the decision to submit the paper for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PMW, MHK, CL and AL have received support from NCMIC Foundation for investigator-initiated research studies and for training fellows. MHK is a member of the board of directors of NCMIC. PMW, MHK, CL, AL, and RV have received support from the Inter-Institutional Network for Chiropractic Research (IINCR) through Palmer College Foundation for investigator-initiated research studies. PMR has received support from the American Heart Association and from Mars Edge for investigator-initiated research studies on migraine. RQW serves on the Scientific Advisory Council for WONDR, Inc. and consults for TakeCare through PIRE.
Data Availability Statement
Deidentified data related to the findings reported in this manuscript will be made available upon request to the study Principal Investigators.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.