
Abstract
Background
Healthcare providers’ (HCPs) perspectives on psychedelic-assisted therapy (PAT) are critical to clinical integration but remain underexplored in Canadian palliative and oncology contexts. This study examines HCP attitudes toward ketamine, psilocybin, and MDMA, and the systemic and ethical factors influencing implementation.
Methods
An exploratory qualitative study using semi-structured interviews was conducted with 12 HCPs across Canada. Interviews explored attitudes, perceived barriers, and implementation considerations. Data were analyzed using thematic analysis and interpreted through the Theory of Planned Behaviour (TPB) to examine how attitudes, subjective norms, and perceived behavioural control shape clinical integration.
Results
Attitudes toward PAT ranged from caution to advocacy, with neutral-to-cautious positions predominating. Ketamine was pragmatically accepted for rapid efficacy but raised concerns regarding commercialization and misuse. Psilocybin elicited mixed views, particularly in relation to end-of-life existential distress. MDMA was considered promising for trauma-related indications but was constrained by neurotoxicity concerns and regulatory barriers. Subjective norms were shaped by stigma, media narratives, and institutional culture, while perceived behavioural control was limited by restrictive policies, infrastructure gaps, and funding inequities. An ethical tension emerged between access to medical assistance in dying (MAiD) and restrictions on PAT in end-of-life care, highlighting perceived policy inconsistencies.
Conclusion
Participants expressed a range of attitudes toward PAT, from caution to advocacy, alongside substantial ethical, regulatory, and systemic constraints to clinical integration. A notable ethical tension emerged between MAiD accessibility and PAT restrictions in end-of-life contexts, reflecting broader questions about Canadian health policy. Participants emphasized the need for substance-specific guidelines, interdisciplinary education, and evidence-informed regulatory reform to guide future clinical consideration of PAT.
- The Idiot by Fyodor Dostoevsky
Introduction
As discussions surrounding the legalization and clinical integration of psychedelic-assisted therapy (PAT) continue to evolve, understanding healthcare providers’ (HCPs) attitudes toward these treatments has become increasingly important. Psychedelics encompass psychoactive 1 substances capable of inducing altered states of consciousness with potential therapeutic benefits. 1 Among these agents, three compounds dominate contemporary research and clinical discourse: psilocybin, 3,4-methylenedioxymethamphetamine (MDMA), and ketamine.1-3
Psilocybin, a naturally occurring compound found in Psilocybe mushrooms, acts as a serotonin 2A (5-HT2A) receptor agonist and has shown promise in alleviating existential distress in palliative care and treatment-resistant depression.4,5 MDMA, an empathogen that enhances serotonin, norepinephrine, and dopamine release, is under investigation for trauma-related disorders such as post-traumatic stress disorder (PTSD) due to its ability to facilitate emotional processing. 6 Ketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist with dissociative properties, diverges from classic psychedelics in its glutamatergic mechanism. However, it is increasingly grouped within PAT discussions due to its rapid antidepressant effects and the United States Food and Drug Administration (FDA)-approved esketamine formulation for treatment-resistant depression.7,8
These therapeutic approaches are particularly relevant in oncology and palliative care settings, where practitioners face the dual challenges of managing complex symptomatology and addressing psychological and existential distress.9-11 HCPs, who serve as primary gatekeepers to treatment options, play a pivotal role in determining patient access to innovative therapies. Their perceptions not only reflect individual clinical experiences and knowledge but also influence broader trends in treatment adoption and healthcare policy.
Recent research has uncovered a nuanced landscape in which cancer care professionals recognize the potential benefits of PAT. Surveys and qualitative studies in oncology and palliative care contexts suggest that providers are more inclined to consider referral when faced with patients with advanced or incurable cancer, reflecting cautious but growing acceptance of these modalities for addressing existential distress. 12 Concurrently, many HCPs report significant knowledge gaps regarding the efficacy, mechanisms, and practical implementation of these therapies, underscoring the urgent need for targeted educational initiatives.12-15
Demographic factors further shape this emerging landscape, with younger and less experienced clinicians generally demonstrating greater openness to innovative treatments including PAT. 16 Moreover, increasing social acceptability of treatments such as psilocybin-assisted therapy is fostering a climate where these options are viewed as viable adjuncts to conventional care. 17 This cultural shift is gradually altering clinical narratives, creating opportunities for interdisciplinary collaboration across healthcare fields including nursing, oncology, and mental health. 18
Beyond individual provider attitudes, the integration of PAT into clinical practice requires addressing systemic challenges including resource constraints, regulatory ambiguities, and the need for standardized protocols.19,20 As evidence for the safety and efficacy continues to expand,21,22 ensuring providers have both the knowledge and structural support to navigate these challenges becomes increasingly important. Enhanced interdisciplinary collaboration and the development of standardized treatment guidelines that also support personalized medicine will be essential in overcoming these barriers.23,24
This qualitative study, conducted with HCPs across Canada, aimed to explore their perspectives on PAT across clinical contexts, with particular emphasis on cancer-related care. By examining how clinical experience, cultural influences, and systemic constraints shaped these perspectives, this research sought to inform educational approaches and foster interdisciplinary dialogue regarding the potential role of PAT in clinical practice.
Methods
Study Design
This qualitative study used semi-structured interviews to examine Canadian HCPs’ perspectives on PAT. We adopted a reflexive thematic analysis25,26 conducted within a realist-pragmatic orientation. 27 Ethics approval was granted by the University of Calgary Health Research Ethics Board of Alberta – Cancer Committee (HREBA.CC-23-0004). The study follows the Consolidated Criteria for Reporting Qualitative Research (COREQ) to ensure transparency and rigor. 28
Research Positionality
This study was led by a master’s student with formal training in psychosocial oncology and additional exposure to PAT through graduate coursework, research involvement, and work in private clinical settings offering PAT. The first author acknowledges a personal bias in favour of the safe clinical implementation of psychedelics, which shaped both the motivation for this study and heightened attentiveness to the therapeutic potential of these substances. To counterbalance this perspective, the research team, particularly those directly involved in qualitative analysis, included members with no prior involvement in psychedelic research or clinical practice. The broader interdisciplinary team comprised research assistants, patient partners, and healthcare providers, all of whom contributed to the design of the interview guide and interpretation of findings.
Reflexivity was practiced throughout to acknowledge and mitigate the influence of personal investments in PAT on data collection, analysis, and interpretation. Strategies included reflexive journaling, regular team debriefs, and analytic triangulation across investigators with differing levels of familiarity and involvement with psychedelics. By explicitly attending to positionality, we sought to ensure that participants’ perspectives remained central to the analysis, and that interpretations were grounded in the data rather than researcher assumptions.
Participant Recruitment and Sample
Sociodemographic Characteristics and Participants’ Knowledge and Experience With Psychedelics
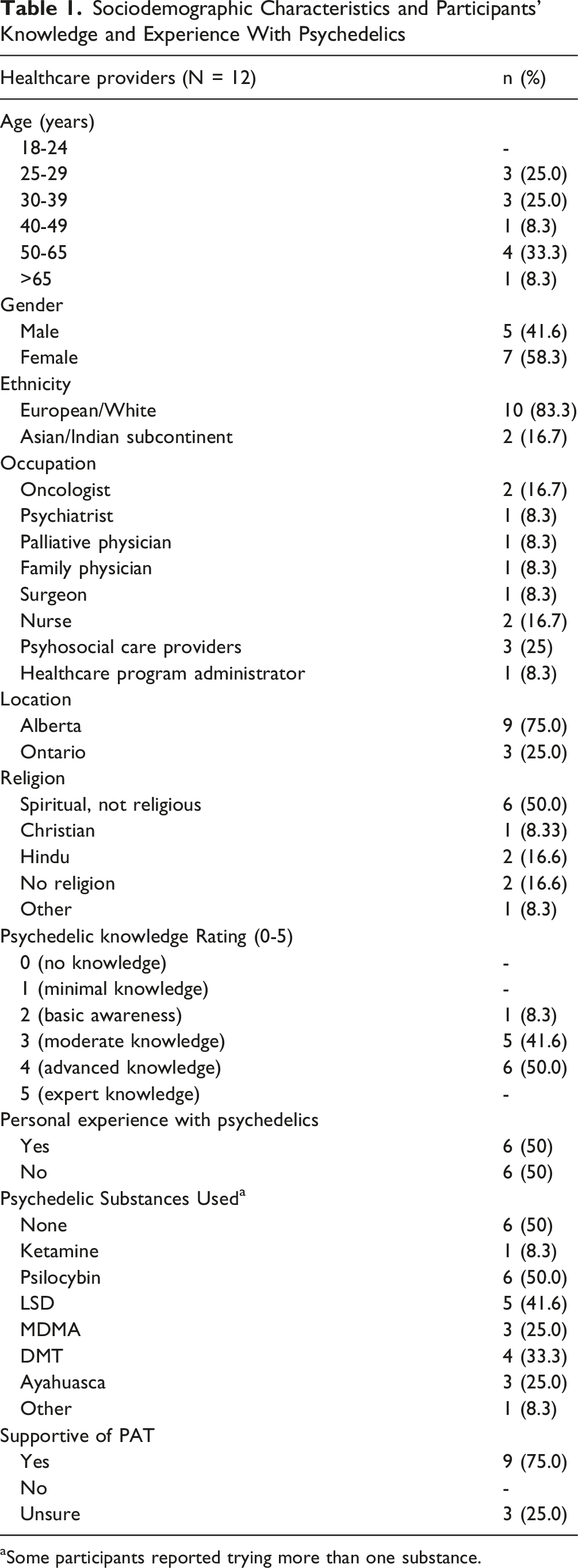
aSome participants reported trying more than one substance.
Data Collection
Individual semi-structured interviews were conducted virtually (average duration of 30-120 minutes). Sessions explored participants’ attitudes, clinical and personal experiences, and perceived barriers/facilitators to PAT. Interview questions were designed to be neutral with respect to PAT. Interviews were audio-recorded, transcribed verbatim, and de-identified for confidentiality. See Supplemental A1 for the interview guide.
Analytical Framework
We adopted a hybrid inductive-deductive reflexive thematic analysis, 25 guided by a realist-pragmatic orientation. 27 The Theory of Planned Behaviour (TPB) 31 was used as a deductive scaffold to map attitudes, subjective norms, and perceived behavioural control, while remaining open to inductive insights not encompassed by TPB. In parallel, we conducted a descriptive content analysis, defined here as the process of quantifying the frequency with which key attitudinal stances appeared across transcripts (eg, “cautious and concerned,” “neutral pragmatism,” “enthusiastic advocacy”). This step did not constitute a separate analytic paradigm but was used to complement thematic analysis by providing a sense of distribution across the small sample. The combination of reflexive thematic analysis and descriptive content analysis enabled us to (1) systematically explore theoretically informed constructs from the TPB and (2) assess how often particular attitudes were expressed, thereby offering both depth and breadth in understanding provider perspectives. Substance-specific distinctions were reported only when participants explicitly contrasted psychedelic agents within the same analytic domain; otherwise, perspectives are presented at the level of PAT broadly.
Overview of Transcript Analysis Method
The investigators followed Braun & Clarke’s 25 six-phase process for reflexive thematic analysis. Three independent coders engaged in iterative coding, supported by NVivo 12 software 32 to facilitate organization and retrieval of data. Content analysis was incorporated as a descriptive step to quantify how frequently key attitudes and concepts appeared across transcripts. A TPB framework provided a deductive lens, alongside inductive coding for novel insights. Data saturation was reached once no additional codes or themes were identified. See Supplemental Table S1 for additional details on this process and Table S2 for a thematic summary.
Results
Twelve participants, recruited from a national online survey on PAT attitudes and beliefs, participated in interviews. 29 Most were White (n = 10) and female (n = 7), with moderate to advanced self-reported psychedelic knowledge. Half had personal experience with psychedelics (n = 6). Of these, all six had used psilocybin, three had used MDMA, and only one had used ketamine — the three agents central to this study. Full details of participants’ psychedelic experience are provided in Table 1. While the majority of participants (n = 9) indicated general support for PAT when surveyed at recruitment, this figure should be interpreted with caution. As illustrated in Supplemental Figure S1, the most frequently endorsed attitude across interviews was Skeptical Curiosity (91.7%), followed by Caution and Concern (75%), indicating that neutral-to-cautious responses were more prevalent across the data than unqualified support. No single attitude was dominant; rather, participants frequently shifted between attitudinal stances depending on substance, clinical context, and patient population.
Analysis identified three overarching themes aligned with the Theory of Planned Behaviour: (1) Attitudes toward PAT, (2) Subjective norms shaping HCP perspectives, and (3) Perceived behavioural control related to implementation. Each theme and its subthemes are described below, supported by representative quotations and tables.
Theme 1: Attitudes Toward Psychedelics: A Continuum From Cautious to Full Advocacy
Providers viewed PAT along a continuum, from cautious concern to enthusiastic advocacy. These attitudes reflected appraisals of psychedelics’ safety, efficacy, and ethical fit with medical practice, and were often expressed in overlapping or context-dependent ways. For instance, some participants who voiced advocacy also raised cautionary notes elsewhere in their interviews. This underscores that no single attitude was dominant; rather, providers shifted between perspectives depending on substance, clinical context, and personal experience. Supplemental Figures S1 and S2 illustrate this continuum: S1 shows the distribution of five core attitudes (sub-themes) — Caution and Concern, Skeptical Curiosity, Neutral Pragmatism, Optimistic Support, and Enthusiastic Advocacy — alongside representative quotes; S2 maps these attitudes’ alignment with key codes. While the categories are distinct, participants could endorse more than one attitude.
Caution and Concern
Caution and Concern (sub-theme): Codes, Descriptions, and Representative Quotes
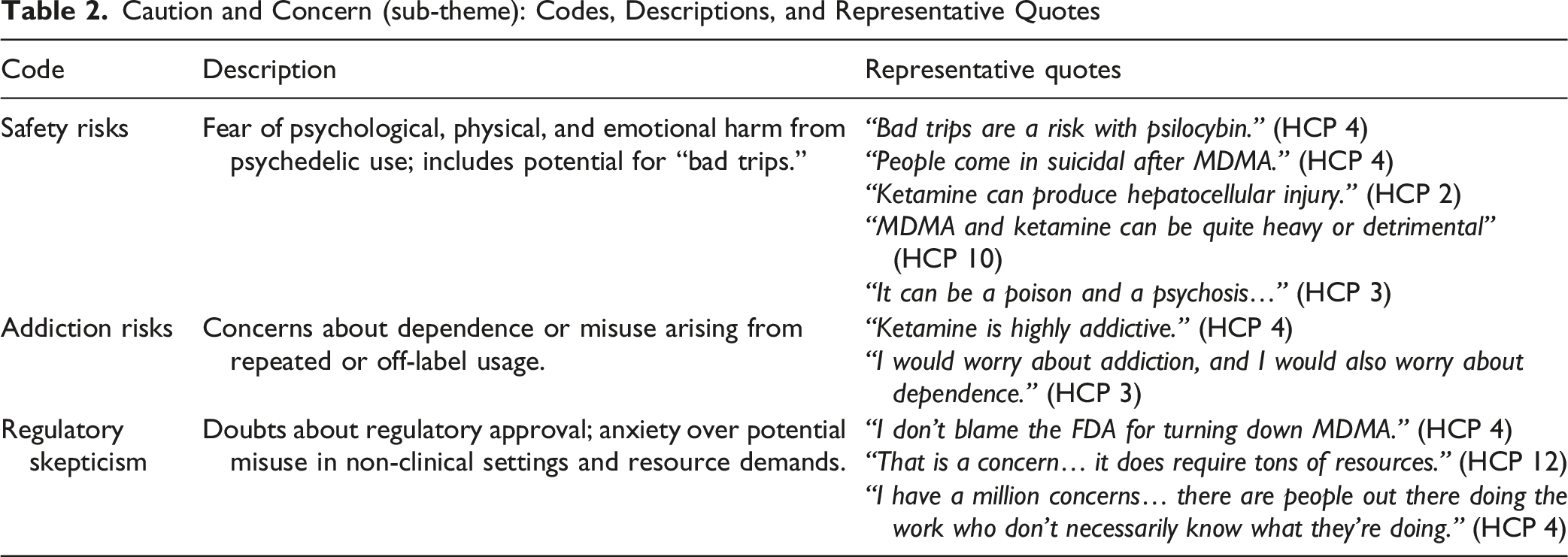
Participants described concerns about PAT, most related to safety risks, potential misuse, and gaps in clinical evidence. They also noted that legal hurdles, limited infrastructure, and stigma contributed to these worries. Psilocybin and MDMA were often linked to uncertainty around regulatory approval, while ketamine was generally seen as somewhat more acceptable given its established medical use, though participants still raised concerns about chronic use and addiction risks.
Skeptical Curiosity
Skeptical Curiosity (sub-theme): Codes, Descriptions, and Representative Quotes
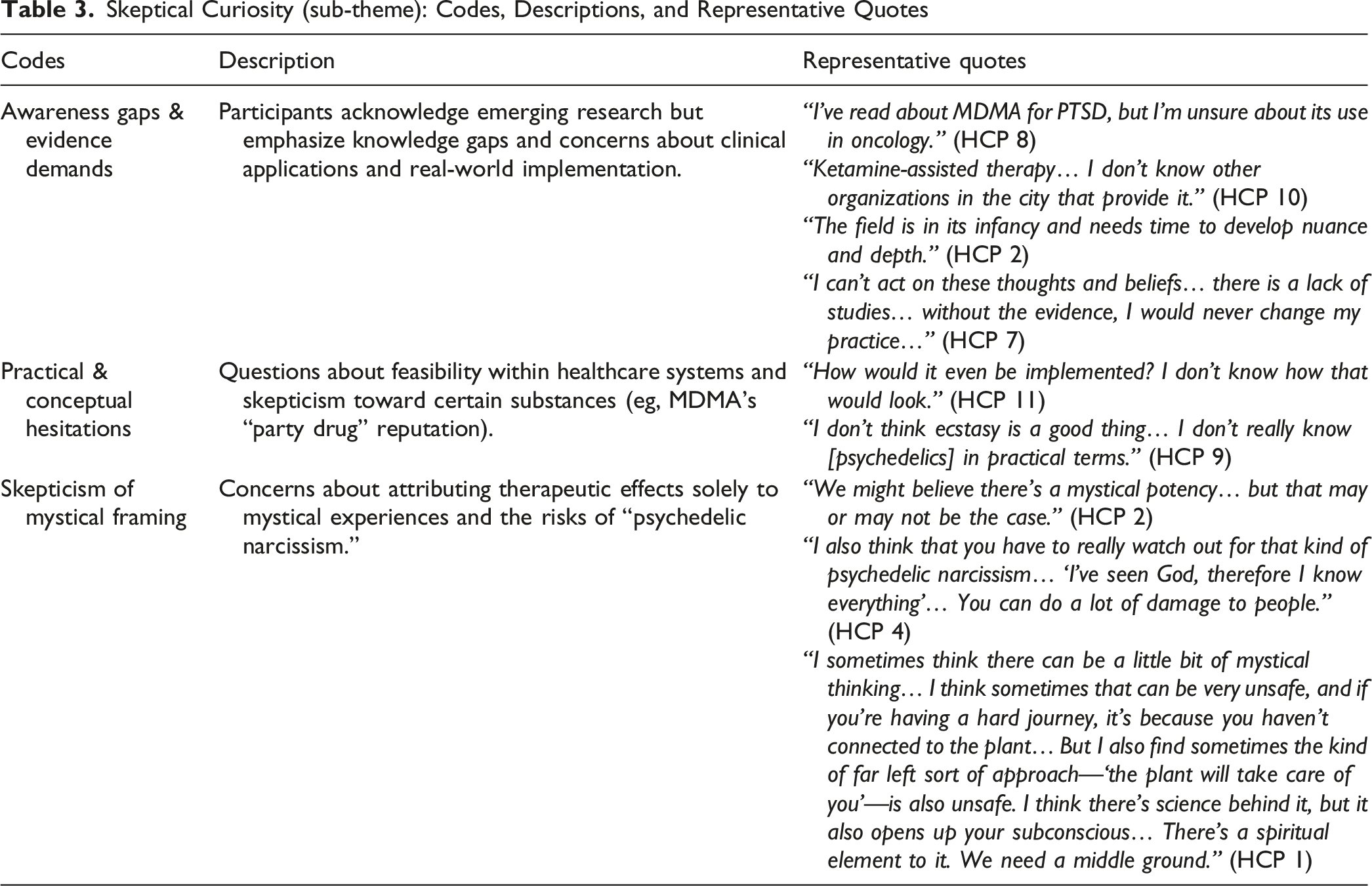
Participants expressing Skeptical Curiosity were intrigued by the therapeutic potential of psychedelics but hesitated to endorse them due to insufficient clinical evidence, unclear implementation strategies, and lingering skepticism toward their framing. Their perspectives reflect gaps in knowledge regarding current research advancements and concerns about overemphasizing mystical or spiritual narratives, which they fear could undermine scientific credibility and lead to unsafe practices.
As one participant noted:“It may have a major role… but we don’t have much to offer until we see real data.” (HCP 3)
Neutral Pragmatism
Defining Attitude: This attitude reflects conditional openness, grounded in evidence-based reasoning and respect for patient autonomy. Participants emphasized support for PAT only if agents are proven safe and effective through rigorous trials and clear protocols. “I’d need to see clear research and evidence before supporting PAT. Knowledge translation is key…” (HCP 12)
Substance-Specific Attitudes Reflecting the Codes of Neutral Pragmatism (sub-theme): Risk-Benefit Assessments and Patient Autonomy
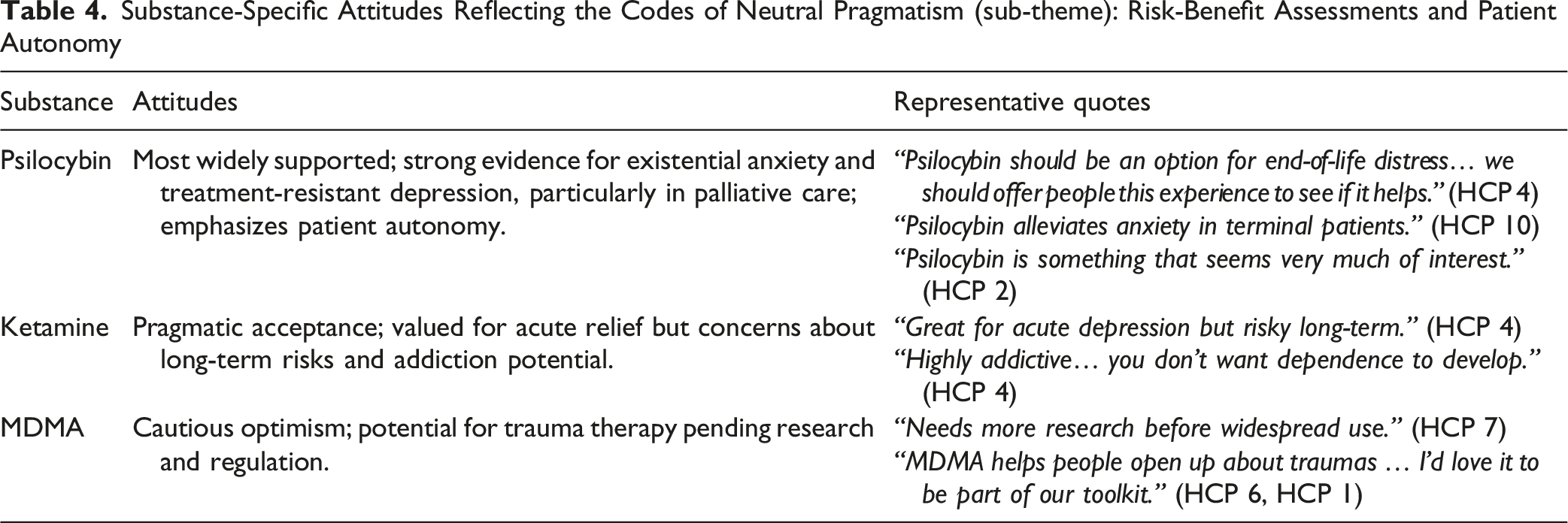
Overall, participants described a pragmatic stance in which willingness to support PAT depended on the presence of strong evidence, safety data, and clear clinical guidelines.
Optimistic Support
Defining Attitude: Participants expressed strong support for the therapeutic potential of psychedelics, citing emerging evidence, clinical experiences, and, occasionally, personal use. Support was particularly high among providers treating patients with persistent, treatment-related side effects. “We see a lot of patient complexity in certain cancer types, like head and neck cancer. These patients often have lifelong side effects from treatment...difficulty speaking, eating, and more. They need a lot of support, and if psychedelics can help, that would be amazing.” (HCP 12)
Personal Experience: Half of the providers (n = 6) acknowledged firsthand use of psychedelics, which reinforced their favourable views. Such encounters appeared to reinforce optimism about therapeutic effects: “I have a very wide interest in it. I think I've had both friends and family use psychedelics with great effect. I've also used quite a number of psychedelics myself over the years.” (HCP 1) “In terms of psychedelics, in terms of what I've tried, I've tried all sorts of things. Years ago, I've tried psilocybin, just actual mushrooms and brewing them to tea, drinking that. I've tried acid, I've tried ayahuasca, I've gone to several ayahuasca retreats at this point.” (HCP 6) “We’ve heard of patients having very powerful journeys … which I think really has changed the field.” (HCP 2)
Overall, optimistic participants highlighted promising therapeutic effects and called for more opportunities to explore psychedelics in clinical settings, while recognizing the importance of safety protocols.
Enthusiastic Advocacy
Defining Attitude: Full endorsement of psychedelics as transformative interventions, urging policy change and widespread acceptance. Participants view current restrictions as morally problematic, especially for those with severe or terminal conditions.
Some HCPs argued that existing restrictions on PAT are both scientifically unfounded and ethically unjustifiable, framing access as a fundamental human right and calling for immediate policy reform.
“This should be a human right… when you see that level of distress and suffering, it’s not a question anymore. …It just seems deeply inhumane.” (HCP 1)
Systemic integration was another key area of concern, with participants calling for the incorporation of PAT into mainstream medical practice. This includes expanding insurance coverage, ensuring professional training, and removing unnecessary barriers to access. “Blocking access is ludicrous.” (HCP 4) “MDMA’s potential for trauma therapy is undeniable.” (HCP 6)
The moral imperative for severe cases was strongly voiced, with advocates expressing frustration over the inadequacy of existing treatments for conditions such as cancer-related existential distress and end-of-life anxiety. They argued that withholding PAT in these circumstances is both ethically untenable and morally wrong. “If you see somebody, a young mom … dying of breast cancer, the existential suffering is absolutely profound… Our tools are horrible.” (HCP 1)
Participants in this group emphasized frustration with current restrictions and called for immediate policy reforms, expanded training, and broader access, particularly for patients facing profound suffering.
Overall, the continuum illustrates how HCPs’ attitudes can shift from cautious skepticism to full-fledged advocacy for distinct substances, depending on (1) perceived safety, (2) clinical evidence, (3) regulatory acceptance, and (4) personal or professional experience with each psychedelic.
Theme 2: Subjective Norms: Social and Cultural Influences on Attitudes
Subjective norms refer to the external pressures that influence HCPs’ attitudes toward PAT. These norms manifest through cultural beliefs, social circles, media narratives, professional expectations, and anecdotal experiences. Five interrelated sub-themes were identified (see thematic map in Supplemental Figure S3).
Cultural Influences
Cultural narratives surrounding psychedelics, shaped by past drug policies and countercultural associations, influenced how some participants perceived their role in medicine. “Some people who are older still have memories of Nixon… so they wouldn’t be as open.” (HCP 1)
Several participants described generational differences, with older providers perceived as more hesitant and younger providers viewed as more open. “The generation coming up now… [is] much more open.” (HCP 6)
Social Influences
Family, colleagues, and peers were described as influential in shaping attitudes toward PAT. “My sister’s life was saved by psychedelics. That’s not something I can ignore.” (HCP 1)
In contrast, workplace dynamics could amplify caution, with some participants expressing the need to self-censor to avoid reputational harm: “I won’t discuss this with someone who could fire me.” (HCP 5) “Nobody would want to be labelled as the prescriber that prescribes hallucinogens.” (HCP 7)
Healthcare System: Institutional Barriers
Participants emphasized how legal status and professional culture restricted their ability to consider PAT in practice. “The fact that it’s illegal… has unfortunately stymied my ability to talk about it.” (HCP 4) “It’s not just the evidence... we also have to deal with the culture of medicine, which is slow to change.” (HCP 7)
Institutional policies act as normative referents, where legal barriers reinforce perceived professional disapproval in participants’ accounts.
Media & Public Perception
Participants described the media as a powerful influence on how psychedelics are perceived by the public and within professional circles. Media coverage was seen as shaping both stigma and legitimacy.
Negative portrayals were described as reinforcing fear and skepticism: “A story about somebody who lost their mind… sets things back hugely.” (HCP 1)
At the same time, positive portrayals were highlighted for their role in normalizing psychedelics and sparking interest: “I do try to put them in contact with… Michael Pollan’s [documentary].” (HCP 6)
Overall, participants suggested that this duality, sensationalized stories of harm alongside high-profile advocacy, created a mixed and sometimes confusing public image.
Gossip & Anecdotes
Beyond formal media and institutional influences, word-of-mouth stories that are both positive and negative were frequently described as shaping perceptions of psychedelics. “Integrators… in Canada…who’ve been arrested… those things unfortunately stick in people’s minds.” (HCP 1)
Conversely, firsthand and secondhand stories of healing drive enthusiasm and curiosity. “My sister… changed her life completely around.” (HCP 1) “A single dose led to a complete eradication of depression and elimination of suicidal ideation.” (HCP 2)
These personal accounts serve as compelling motivators for shifting attitudes; participants suggested that anecdotes often function as behavioural beliefs, where vivid stories could outweigh abstract data in shaping perceived outcomes.
Taken together, participants described a range of external pressures that shaped their comfort and openness toward PAT. Cultural narratives, professional environments, media portrayals, and personal stories all contributed to a climate of mixed signals, where caution and curiosity coexisted in shaping provider attitudes.
Theme 3: Perceived Behavioural Control (PBC): Structural and Practical Constraints
PBC refers to the systemic and logistical factors influencing HCPs’ capacity to implement PAT. In oncology and palliative care, where existential distress and Medical Assistance in Dying (MAiD) are central concerns, PBC is shaped by clinical safety protocols, regulatory policies, institutional support, and operational feasibility. Although HCPs acknowledge the promise of psychedelics, structural barriers frequently limit integration into clinical practice. Four sub-themes were identified (see Supplemental Figure S4 for thematic map).
Clinical and Safety Considerations: Risk Management and Implementation Feasibility
Providers emphasized the need for standardized clinical guidelines to ensure safe PAT implementation. The absence of clear protocols for patient selection, dosing, and risk mitigation emerged as a significant barrier. For instance, HCPs described challenges in managing vulnerable populations, such as patients with addiction histories: “We did have a number of patients with addiction… some of them did not do as well.” (HCP 2)
Dosing strategies were another focal point, with providers advocating for cautious, structured approaches: “Start low, go slow—without that, we’re throwing people into intense experiences recklessly.” (HCP 4)
Controlled environments were deemed essential to minimize variability and ensure therapeutic efficacy: “A controlled setting is crucial for therapeutic use of psychedelics. We need feedback from patients to understand outcomes and minimize uncontrolled variables.” (HCP 10)
Perceived Ethical Tensions Between MAiD and PAT Access
It is important to note that the use of PAT in end-of-life contexts, including in relation to MAiD, represents a qualitatively distinct clinical and ethical scenario from its potential application in non-terminal illness. The ethical considerations, risk-benefit profile, and patient autonomy questions differ substantially across these contexts. References to MAiD in the following accounts emerged inductively from participants and were not an a priori focus of the study; they are presented here as individual perspectives rather than evidence of a systematic relationship between MAiD and PAT. “I can offer MAiD, but I can’t prescribe psilocybin. That’s a ridiculous conflict.”(HCP 4) “We are terrible at treating existential suffering at the end of life… And I think psychedelics have a potential… And it’s deeply, deeply sad that it’s not more easily accessible.” (HCP 1)
The tension was compounded by cases where patients were approved for MAiD but denied access to PAT. One provider recounted a legal case involving a terminally ill patient. “There was an individual in [city in Canada] approved for MAiD but denied psilocybin therapy. It’s shocking...psychedelics could offer an alternative to end-of-life suffering, yet the system blocks access.” (HCP 10)
Several participants suggested that psychedelics could reduce reliance on MAiD by addressing existential distress and reframing patients’ perspectives: “If you gave patients psilocybin or MDMA, they might shift from overwhelming grief to focusing on how to live their remaining time meaningfully. This could reduce the desire for MAiD in some cases.” (HCP 5) “The majority of palliative care physicians believe there’s no need for MAiD if we can keep patients comfortable… Maybe psychedelics are part of that.” (HCP 3)
Systemic and Logistical Barriers: Infrastructure, Equity, and Resource Allocation
Distinct from the institutional barriers discussed under Subjective Norms (subtheme 2.2.3), which shaped providers’ perceived professional approval of PAT, the barriers described here concern concrete structural and logistical constraints including physical space, funding, staffing, and time that directly limited providers’ capacity to implement PAT regardless of their attitudinal stance.
Beyond regulatory hurdles, HCPs identified infrastructure deficits, financial constraints, and time pressures as critical obstacles. Dedicated clinical spaces for PAT were scarce: “We have no place for this in a hospital setting… You need a quiet, confidential space.” (HCP 8)
A healthcare administrator emphasized systemic inequities: “Our healthcare system is not equitable. Some hospitals have robust psychosocial teams, while others barely have one social worker. Funding relies on budgets competing with acute care needs.” (HCP 12)
Financial accessibility further complicated implementation. Many patients resorted to illicit means: “She accessed psilocybin illegally. Why should people in crisis resort to the black market?” (HCP 5)
Operational feasibility emerged as a critical concern: “If PAT requires dedicated clinical space, hospitals must prioritize this against cancer treatment capacity. Resource allocation often favours life-saving interventions over psychosocial care.” (HCP 12)
Time constraints also posed barriers: “It’s not just about giving a drug. You need time for preparation and integration. Where in my schedule does that fit?” (HCP 7)
The Role of Structured Integration
Structured integration protocols were identified as a cornerstone of effective PAT delivery. Providers stressed that unresolved psychological distress could arise without proper post-session support: “Psychedelic therapy can be transformative, but only if there’s support afterward. Otherwise, you leave people with unresolved insights.” (HCP 6)
One provider recounted a case involving inadequate integration following the delivery of PAT: “He had an amazing journey. But I feel, looking back at it, he did not get a lot of integration. And then what happened was he just started splitting and he then split the journey that he'd been on as this amazing thing versus the existential distress that he was still in.” (HCP 1)
HCPs underscored the necessity for therapeutic follow-up: “The therapy is necessary to help them sort through what they experienced… A negative experience can still give you positive learning.” (HCP 4)
While participants recognize psychedelics’ potential to address existential distress in cancer and palliative care, structural barriers — such as legal restrictions, infrastructure gaps, and financial inequities — often preclude meaningful adoption. The ethical and moral tension between facilitating access to these therapies and ensuring patient safety highlights the need for stakeholders to work together to reform regulations, improve infrastructure, and address financial inequities, thereby paving the way for more effective and equitable integration of PAT into clinical practice.
Discussion
This exploratory study illustrates the diversity and complexity of HCPs’ perspectives on PAT. Rather than a clear continuum, participants expressed a range of context- and agent-specific views, with individuals often holding both cautious and supportive attitudes depending on perceived risks and clinical circumstances. While many participants recognized the potential of PAT to alleviate psychological and existential distress in serious illness, they also voiced substantial concerns related to safety, regulatory barriers, and the limited evidence base. In addition, our findings highlight how subjective norms—shaped by cultural influences, professional networks, and institutional contexts — interacted with participants’ clinical experiences and perceived systemic constraints. Together, these findings offer preliminary insights into both the opportunities and challenges facing the potential integration of PAT into healthcare practice.
Integrating Comparative Analysis of Psychedelic Agents and Provider Attitudes
While a number of participants expressed generally positive attitudes toward PAT, consistent with recent surveys showing strong belief in the therapeutic promise of these interventions, 33 participants’ openness and concerns varied notably between specific agents. To contextualize these variations, we compare ketamine, psilocybin, and MDMA below, highlighting how their distinct therapeutic applications, phenomenological experiences, and associated clinical challenges may have shaped participants’ acceptance and concerns.
Ketamine for Acute Relief
In this study, ketamine consistently occupied a middle ground across the attitude continuum, accompanied by a noticeable lack of enthusiasm relative to other psychedelic agents. Its long-standing use as an anaesthetic, legal status, and its established role in acute psychiatric interventions lend it a degree of clinical legitimacy that eases some safety concerns. Several participants remained cautious about its addiction potential and risks of prolonged administration, consistent with existing literature.12,33 As an NMDA receptor antagonist, its dissociative mechanism diverges sharply from the serotonin-driven pathways of classic psychedelics like psilocybin. This neurobiological distinction, coupled with unique clinical risks (eg, ketamine-induced cystitis), underscores its classification within a separate therapeutic and regulatory category.7,34,35 Prior research cautions that conflating ketamine with classic psychedelics risks obscuring these challenges.36,37
Participants highlighted ketamine’s rapid onset and short duration of effects as advantages for acute psychiatric relief. The authors note that these features also present unique challenges for patient integration that are well documented in the literature — specifically, ketamine’s brief dissociative state necessitates specialized therapeutic protocols tailored to its distinctive phenomenology, and the rapid commercialization of ketamine through for-profit clinics and at-home nasal sprays has created significant variability in patient screening, oversight, and integration support.38-40 Consistent with these documented concerns, several participants noted ethical and clinical concerns about patients bypassing integration entirely due to financial barriers or logistical constraints, and emphasized the need for clearer regulatory guidance and standardized integration protocols.
MDMA as a Trauma-Focused Intervention
Among the psychedelics discussed, MDMA elicited the greatest degree of skepticism and stigma from participants. Although viewed as a promising tool for trauma-focused therapy due to its capacity to foster trust and prosocial behaviour in patients processing severe PTSD,41,42 MDMA remains controversial in the literature. Prior research demonstrates sustained remission of PTSD symptoms in treatment-resistant patients, attributed to MDMA’s ability to dampen amygdala reactivity while enhancing prefrontal regulation. 43 However, MDMA’s transient serotonin surge is followed by depletion, raising concerns about post-use crashes and mood destabilization.44,45 Consistent with these concerns, some participants reported instances of patients experiencing severe post-MDMA distress. The FDA’s recent recommendation against immediate approval for PTSD treatment, citing study design concerns and insufficient long-term safety data, 46 further illustrates the contested regulatory landscape surrounding MDMA. Although PTSD occurs less frequently among cancer patients compared to other frequently studied groups such as veterans, it remains clinically relevant, especially for those with advanced illness or traumatic treatment experiences. 47 Several participants favoured psilocybin for oncology-related existential distress; while for MDMA, participants emphasized the urgent need for clearer safety protocols, standardized oversight, and robust long-term evidence to facilitate broader acceptance.
Psilocybin for Existential Distress and Meaning-Making
Psilocybin elicited mixed reactions among participants. Some participants expressed caution about risks such as bad trips, psychological overwhelm, and logistical challenges in settings lacking robust protocols.16,48 Others emphasized its potential to relieve existential and psychological distress where conventional therapies fall short, a perspective consistent with evidence showing sustained reductions in end-of-life anxiety and depression.49,50 Historical work with LSD similarly reported reductions in fear of death and improved acceptance of impending mortality. 51
Several participants noted that psilocybin’s introspective effects may help patients reframe their relationship with mortality, and several advocated for patient choice in accessing this option. This reflects recognition that existential anguish—characterized by loss of meaning, fear of death, and spiritual distress—requires approaches beyond conventional biomedical paradigms.52,53 Prior research suggests that psilocybin’s capacity to induce mystical-type experiences, often described as “ego-dissolving” or “transcendent,” may further enable psychological resolution and emotional catharsis. 54 These perspectives are consistent with reports from oncology and palliative care providers in New Zealand and the USA, as well as cancer patients in the United Kingdom, who similarly recognized psilocybin’s potential to alleviate existential distress, underscoring the cross-national relevance of these findings.13,55
Still, some participants cautioned that integrating psilocybin into clinical practice demands rigorous validation. This reflects ongoing debates about whether its benefits arise from neurobiological changes (eg, serotonin-driven neuroplasticity), 56 subjective mystical experiences, 54 or therapeutic context. 57 Prior research notes that overemphasizing spirituality risks exploitative practices, 58 while purely clinical frameworks may neglect existential insights central to its therapeutic potential. 59 Several participants advocated for a balanced approach, harmonizing empirical rigor with respectful engagement of subjective experiences, 60 emphasizing the need for protocols that honour both psilocybin’s biological action 61 and its capacity to mediate psychological transformation. 49
In summary, participants emphasized that these substances cannot be evaluated under a single “psychedelic” framework. To advance PAT responsibly, stakeholders must develop agent-specific clinical guidelines, provider education programs, and regulatory frameworks that reflect each substance’s distinct safety profile. Equitable access must also be prioritized to prevent commercialization from outpacing evidence. Recent reviews of the psychedelic industry highlight both the rapid growth of investment and the ethical, regulatory, and access challenges that commercialization poses, underscoring the importance of ensuring that market forces do not eclipse patient safety and equitable care. 62
Subjective Norms
Cultural narratives surrounding psychedelics, historically intertwined with counterculture movements and criminalization, continue to affect HCPs’ receptivity to their medical use.63,64 This historical stigma contributes to generational divides in provider attitudes. For instance, Sholevar et al. 65 found that older providers, shaped by Nixon-era policies, expressed greater hesitancy, while younger generations, influenced by contemporary research and shifting societal attitudes, appeared more open. In the present study, some participants similarly referenced historical stigma as a barrier to clinical adoption, though generational divides were less pronounced than in previous studies, with institutional norms and regulatory concerns playing a more dominant role in shaping attitudes.
Interpersonal networks and professional circles further shape provider attitudes. Sholevar et al. 65 found that palliative care providers often emphasized transdiagnostic and growth-oriented applications of PAT, whereas psychiatrists more frequently questioned its legitimacy outside traditional psychiatric frameworks. Oncologists, recognized the importance of addressing existential distress, while other practitioners prioritized conventional symptom management. 65 These disciplinary patterns were broadly reflected in the present study, where participants’ professional contexts appeared to shape their conceptualisation of PAT’s risks and benefits, though the small and heterogeneous sample does not allow profession-specific conclusions. Such professional divides mirror broader literature on referent groups influencing behavioural intentions.66,67 Prior research also suggests that personal experiences with non-ordinary states of consciousness can shape provider attitudes toward PAT, with positive experiences often linked to greater advocacy and adverse or limited experiences associated with skepticism. 65 These findings align with broader evidence highlighting the heuristic power of anecdotal experience in shaping clinical perspectives.68,69
Institutional barriers present another formidable challenge, as reported in the literature. The medical system’s slow adaptation to novel therapies, combined with legal and professional constraints, has been shown to foster systemic inertia that frames psychedelics as “risky” within traditional medical culture, consistent with research indicating that institutional policies often act as normative referents where legal and regulatory hurdles reinforce a culture of conservatism in clinical settings. 70 Several participants echoed these dynamics, describing how legal status and professional culture restricted their willingness to discuss or endorse PAT in practice.
Media narratives have also been shown to play a critical role in shaping perceptions of PAT. Sensationalized coverage can reinforce stigma and hinder research progress, whereas positive portrayals by public figures can legitimize therapeutic applications. Historical evidence illustrates this impact: a 1968 survey of LSD investigators reported that negative publicity directly disrupted participant recruitment, altered subject attitudes, and contributed to the discontinuation of studies. 71 Participants described similar dynamics, noting that sensationalized media stories reinforced public fear, while figures such as Michael Pollan helped legitimize psychedelics as potential treatments. Finally, informal narratives such as gossip and personal anecdotes were described by participants as strongly shaping their own attitudes and those of their colleagues, often exerting a stronger influence than abstract clinical data. This phenomenon is supported by research into the role of anecdotal vs statistical evidence,68,69 and underscores the need for strategic knowledge translation efforts that integrate robust empirical findings with relatable real-world experiences to foster more balanced and informed attitudes toward PAT.
Perceived Behavioural Control
The majority of participants described numerous constraints on their perceived ability to implement PAT, despite recognizing its potential for addressing existential distress. Key barriers identified included inadequate clinical infrastructure, insufficient trained personnel, and lack of standardised protocols for patient selection, dosing, and integration. Consistent with existing literature, effective implementation has been shown to require both regulatory reform and enhanced logistical support systems.
Clinical and Safety Considerations
Some participants expressed concerns about the addictive potential of psychedelics. However, existing evidence indicates that classical psychedelics like psilocybin have low abuse liability; as unlike psychoactive substances that trigger direct dopamine activation, classical psychedelics engage serotonin receptors, which significantly mitigates their potential for addiction. 58 Research further indicates that most psychedelics do not lead to the compulsive drug-seeking behaviour characteristic of addictive substances,72,73 and consistent with these concerns, a survey of psychiatrists found that worries about addictive potential were among the strongest predictors of opposition to medical legalization of psychedelics. 74
Participants’ concerns about addiction potential, particularly linked to substances like ketamine and MDMA, highlight the need for proactive education to differentiate their risks from classical psychedelics. 75 This is consistent with existing knowledge translation frameworks aimed at clarifying evidence-based risk profiles and reducing stigma. 76
For vulnerable populations (eg, those with bipolar I/II disorder or schizophrenia), existing literature emphasises that stringent screening and risk mitigation are critical, as psychedelics may exacerbate symptoms without controlled protocols.21,77,78 Consistent with this, participants reinforced the need for structured dosing frameworks mirroring safety principles of controlled settings and guided integration.58,79 Participants also emphasized that structured post-session protocols are equally vital to sustain therapeutic gains and prevent unresolved distress, consistent with existing literature. 80
Finally, some participants noted that clinical competence in PAT requires formal training. Lived experience with psychedelics is not sufficient to guide patients therapeutically, just as lack of such experience does not equip providers to understand the challenges of non-ordinary states of consciousness. Both groups therefore require structured, interdisciplinary education and supervision to deliver PAT safely and ethically, as supported by existing literature.81-83
Systemic and Logistical Barriers
The growing prevalence of psychedelic use, including microdosing, underscores systemic and logistical barriers to implementing PAT documented in the literature. 84 Studies reveal that informed providers are more likely to adopt favourable attitudes toward PAT, yet many lack foundational understanding of psychedelics’ risks, benefits, or pharmacology,85-87 and without targeted education, misconceptions persist, potentially driving patients toward illicit use and away from evidence-based care.16,88 Participants described these challenges as compounded by infrastructure deficits (eg, scarce clinical spaces), financial inequities, and time constraints, which prioritised acute care over innovative psychosocial interventions. Consistent with the literature, limited access exacerbates systemic disparities, as cost barriers push marginalised groups toward unregulated sources. 89 Collectively, these barriers reflect a healthcare system ill-equipped to equitably integrate PAT without addressing provider knowledge gaps, resource allocation, and institutional biases. 90
Regulatory and Ethical Tensions With MAiD Accessibility and PAT Restrictions
The policy inconsistency identified by some participants — whereby Canadian clinicians can legally facilitate MAiD yet remain unable to offer psychedelics for existential suffering — raises important questions about the coherence of Canadian end-of-life care policy. It is worth noting that this tension was not raised by the majority of participants, but emerged unprompted from a subset of HCPs, suggesting it reflects a genuinely felt ethical contradiction rather than a researcher-imposed framing. It is also critical to note that PAT and MAiD are not equivalent interventions, nor should they be treated as such; one addresses existential and psychological distress as part of ongoing care, while the other facilitates a medically assisted death. Nonetheless, the fact that some participants perceived these as existing in ethically contradictory regulatory space reflects a broader tension in how Canadian policy currently conceptualises patient autonomy and access to relief at end of life. This tension is particularly salient in the Canadian context, where MAiD has been legal since 2016 yet psilocybin remains restricted except through Health Canada’s Special Access Program or Section 56 exemptions. A Canadian population-based survey found high social acceptability for psilocybin-assisted therapy at end of life, with 79.3% of respondents considering it a reasonable medical choice for existential distress and 84.8% supporting public health system coverage, 17 suggesting the restrictive regulatory environment may be increasingly out of step with public values.
This tension is not unique to Canada. Scholars have argued that PAT fundamentally challenges prevailing biomedical models of death by shifting focus from symptom suppression toward existential meaning-making — a reorientation that healthcare systems and regulatory frameworks have been slow to accommodate. 65 From a bioethical standpoint, restrictive policies that deny patients access to evidence-supported interventions for existential suffering may inadvertently violate the principle of beneficence, particularly when the harm potential of classical psychedelics has been shown to be substantially lower than that of many legally accessible substances such as alcohol or opioids.70,91 This concern is particularly pressing given that current palliative care interventions for end-of-life distress have shown inconclusive evidence of effect, with benefits limited to the short to moderate term, and often require months to take effect, 92 whereas psilocybin-assisted therapy has demonstrated rapid and sometimes sustained reductions in existential distress, depression, and death anxiety in patients with life-threatening illness.9,92,93 A 2025 JAMA Psychiatry viewpoint directly addresses this contradiction, noting that psychedelics may target key conditions driving requests for assisted dying and raising the question of whether suffering can be considered truly irremediable when potentially effective treatments exist but remain legally inaccessible. 94
This ethical contradiction is compounded by the practical barriers that Schedule I classification creates for establishing research programs, including the need for specialised government approvals, institutional buy-in, and secure infrastructure, 95 which in turn limits the very evidence base that regulators require before reconsidering policy. Such contradictions may also contribute to moral distress among clinicians whose professional obligation to alleviate suffering conflicts with restrictive legal frameworks, 95 particularly when patients cannot make fully informed decisions about MAiD without access to all potentially effective treatments for existential distress. 94
We interpret these perspectives as reflections of ethical frustration rather than evidence that PAT is a substitute for MAiD. Further research is needed to examine how PAT may inform care at the end of life and whether it holds relevance for existential distress more broadly.
Limitations, Reflexivity, and Future Directions
This study has several important limitations. First, participants were primarily drawn from similar geographic contexts in Canada, which limits the generalizability of findings. With 12 participants across 8 disciplines, the study was designed as an exploratory qualitative inquiry and findings should therefore be interpreted as preliminary insights rather than generalizable conclusions. The absence of perspectives from historically underrepresented or marginalized communities, who may harbour deeper mistrust of medical interventions, 96 means key attitudes toward PAT may not have been captured.
Second, recruitment through a national survey explicitly focused on PAT likely introduced self-selection bias toward providers already familiar with or positively inclined toward these therapies. Despite efforts to include participants varying in psychedelic experience, this bias likely skewed results toward more favourable attitudes overall, and findings should be interpreted with this in mind.
Third, despite rigorous methodological practices such as reflexive thematic analysis and continuous research team debriefs, our interpretations inevitably reflect our academic backgrounds and personal biases. Transparent acknowledgment of this influence underscores the importance of including diverse research team members in future qualitative analyses. Finally, as an exploratory study situated within a realist-pragmatic orientation, the findings should be interpreted as applied insights to inform practice and policy rather than as theory-generating claims.
Future quantitative and longitudinal studies are essential for validating and expanding upon these preliminary findings, particularly given the rapid pace of developments in psychedelic research, policy, and clinical practice. A proposed thematic model (see Figure 1) illustrates recommended strategic actions for key stakeholders, policymakers and regulators, healthcare institutions, healthcare providers, and researchers, to support safe, ethical, and evidence-informed consideration of PAT integration into clinical contexts. Proposed thematic model illustrating recommended strategic actions for key stakeholders (policymakers and regulators, healthcare institutions, healthcare providers, and researchers) to support safe, ethical, and evidence-informed integration of PAT into clinical contexts. The visualization was created using RStudio (version 2024.12.1 + 563)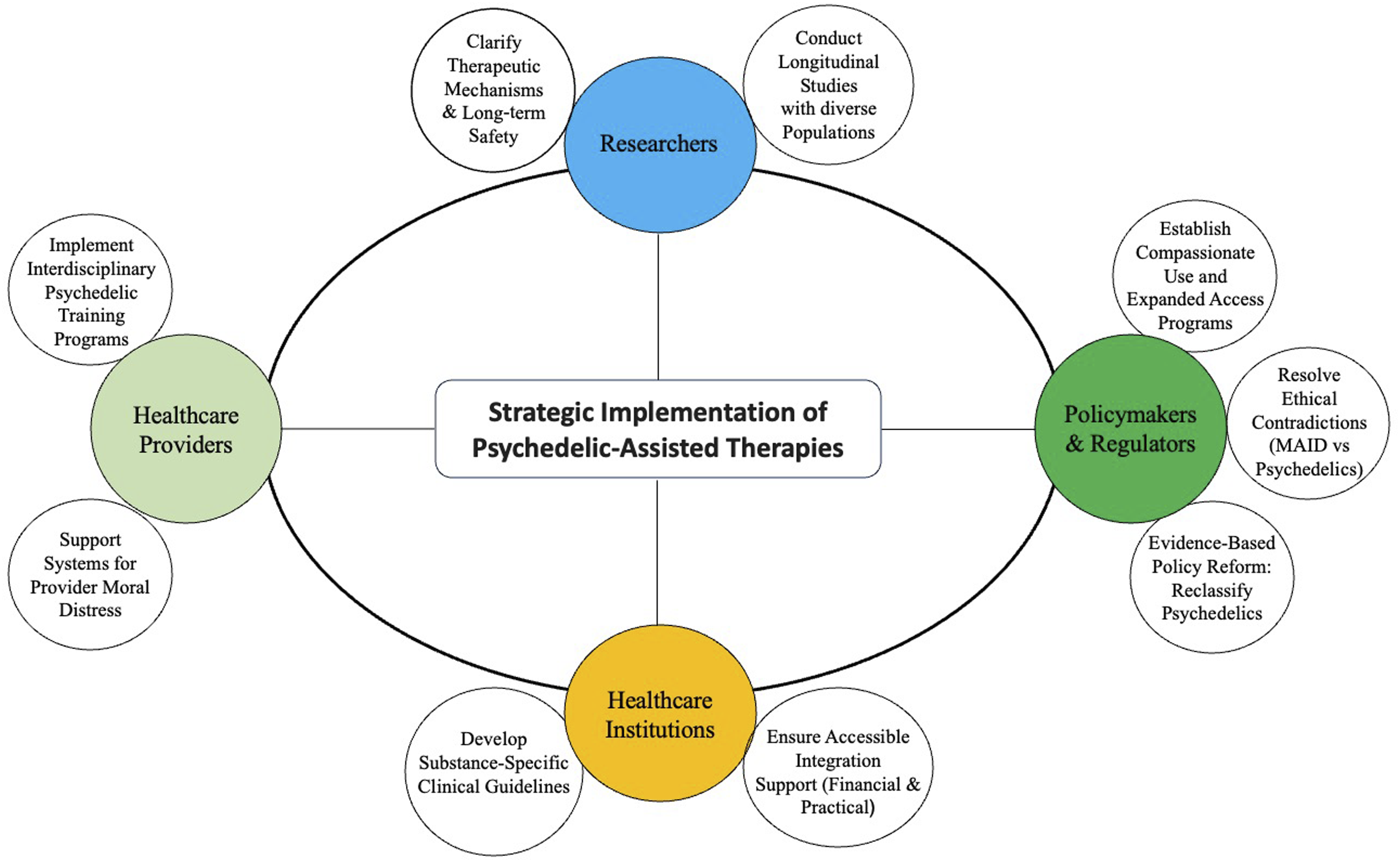
Conclusion
This exploratory qualitative study provides preliminary insights into Canadian HCPs’ perspectives on PAT across clinical contexts. Participants expressed a range of attitudes shaped by substance-specific distinctions, subjective norms, and perceived structural barriers. A notable ethical tension emerged among a subset of participants between MAiD accessibility and PAT restrictions, reflecting broader questions about the coherence of Canadian end-of-life care policy. These findings underscore the need for agent-specific guidelines, interdisciplinary education, and evidence-informed regulatory reform to responsibly guide future consideration of PAT in clinical practice.
Supplemental Material
Supplemental Material - Healthcare Providers’ Perspectives on Psychedelic-Assisted Therapies Across Clinical Contexts: “I can Offer Them Medical Assistance in Dying, but I can’t Prescribe Psychedelics”
Supplemental Material for Healthcare Providers’ Perspectives on Psychedelic-Assisted Therapies Across Clinical Contexts: “I can Offer Them Medical Assistance in Dying, but I can’t Prescribe Psychedelics” by Haley D. M. Schuman, Raèf Mina, Sofia Barkova, Tina Nguyen, Julie M. Deleemans and Linda E. Carlson in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgements
We sincerely thank the healthcare providers for taking the time to openly share their experiences for this research. We also thank Chantal Savard for assistance with reference management, and Sheila and Bronwyn Schuman for editorial support.
Ethical Considerations
Ethics approval was granted by the University of Calgary Health Research Ethics Board of Alberta – Cancer Committee (HREBA.CC-23-0004).
Consent to Participate
Informed consent was collected from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Linda Carlson holds the Enbridge Research Chair in Psychosocial Oncology, co-funded by the Canadian Cancer Society and the Alberta Cancer Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.