
Abstract
Objective
To assess the longer-term functional and participation outcomes in survivors with colorectal cancer with peritoneal metastasis (CRCPM) and pseudomyxoma peritonei (PMP) following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy intervention (CRS-HIPEC).
Method
Adult CRCPM/PMP in the community following CRS-HIPEC completed validated questionnaires. Descriptive statistics summarized participant characteristics, while multivariate linear regression (p < 0.05) identified predictors of functional and psychosocial outcomes, and a binary logistic regression model identified factors associated with poorer quality of life (QoL).
Results
Of 100 participants (59 CRCPM, 41 PMP), mean age: 59.1±12.2 years, 52% male, mean time since CRS-HIPEC: 2.4±2.5 years, overall, many reported persistent issues: fatigue (86%), fear of recurrence (79%), pain (58%), insomnia (52%) and bowel dysfunction (32%). Despite this, overall functional recovery was good (Clinical Functioning Information Tool median [IQR]: 28 [19.3–52.5]), with low perceived psychological impact (Depression Anxiety Stress Scale total: 6 [0–17.5]) and relatively preserved QoL (European Quality of Life VAS score: 78 [60–85]). The CRC-specific QoL was poorer (Functional Assessment of Cancer Therapy-Colorectal: 106 [91–115.6]) and community integration was modest (Community Integration Questionnaire: 20.3 [16–24]). The PMP cohort reported a lower persistent symptom burden and a more favourable QoL. Overall, older age and unemployment were strong predictors of poorer outcomes. Employment status and symptom burden independently predicted longer-term functional and participation outcomes in CRCPM survivorship, with female gender, stoma, and radiotherapy as additional influencing factors.
Conclusion
Overall, despite participants being functionally well, many experience substantial longer-term symptom burden and participation-related challenges (especially in CRCPM) following CRS-HIPEC, reflecting significant unmet rehabilitation needs. Systematic integration of rehabilitation across the CRC care continuum is therefore essential to optimise longer-term functional and participation outcomes in this population.
Keywords
Introduction
Colorectal cancer (CRC) accounts for approximately 10% of all cancers, is the third most frequently diagnosed cancer, and the second leading cause of cancer-related mortality worldwide (2022). 1 The global burden of CRC is projected to increase to 3.2 million new cases and 1.6 million deaths by 2040. 2 The incidence rates of CRC are highest in Australia, New Zealand, and Europe, and continue to rise in persons younger than 50 years of age.2,3 CRC imposes a substantial financial burden on patients, health systems, and society, driven by direct medical costs, as well as indirect costs associated with treatment access, productivity loss due to disability, and premature mortality. 4
Advances in CRC screening and treatment have improved overall outcomes, with the 5-year relative survival rate increasing to 73% in 2016-2020. 5 Beyond survival, CRC and its treatments are associated with a broad range of persistent physical and psychological sequelae (e.g., bowel dysfunction, pain, fatigue, anxiety and depression) that translate into substantial long-term functional and participation challenges, including increased care needs, strained relationships, difficulty returning to work and increased financial burden.6-8 A recent Australian observational study highlighted that these challenges may persist over time, with ongoing high symptom burden, reduced health-related quality of life (HRQoL), and diminished community reintegration evident at a mean follow-up time of 2.4 years. 9 Persistent unmet supportive care needs appear particularly prevalent among CRC survivors who undergo complex treatment, are younger, unemployed, have limited social support, and/or come from lower socioeconomic backgrounds. 10
Approximately 10% of CRC survivors are living with metastatic disease. 11 Peritoneal metastasis accounts for 5% of CRC cases at initial diagnosis, and a further 5% develop metachronous peritoneal metastases during follow-up. 12 For patients with CRC and peritoneal metastases (CRCPM), cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) may offer a potential curative option and improved survival. The aim of CRS-HIPEC is complete macroscopic peritoneal surface tumour clearance through peritonectomy and resection of involved organs, followed by a single administration of intraperitoneal chemotherapy to eradicate residual microscopic disease. Since its introduction in the 1980s, CRS-HIPEC has become a cornerstone treatment for peritoneal surface malignancies, with the two most common indications being CRCPM and pseudomyxoma peritonei (PMP).13,14
Survival outcomes following CRS-HIPEC are encouraging in selected patients with CRCPM and PMP. Elias et al 15 reported a 5-year survival rate of up to 51% and a median survival of 63 months in patients with CRCPM who achieved near-complete cytoreduction. In PMP, a study demonstrated a 5-year survival of 62% and a median survival of 92 months after CRS-HIPEC, 16 suggesting a more favourable clinical outcome in this cohort. Despite the survival benefits, CRS-HIPEC remains a highly resource-intensive intervention and is associated with considerable perioperative morbidity, reported to range from 15.1% to 47.2%. 17 Common complications include gastrointestinal dysfunction (anastomotic leak, bowel perforation, pancreatitis), respiratory complications (pneumonia and respiratory failure), thromboembolic events, cardiac dysfunction, wound-related complications, and chemotherapy-related myelosuppression. 18 The severity of the postoperative impairments and prolonged recovery may therefore significantly impact patients’ functional outcomes, societal participation, and overall HRQoL.
Despite increasing use of CRS-HIPEC, robust evidence describing the longer-term functional outcomes and survivorship experiences in patients with CRCPM and PMP remains limited. Although short- to medium-term studies suggest that HRQoL may recover to baseline within 12 months following surgery, these findings must be interpreted with caution.19,20 Many studies report attrition rates approaching 50%, raising concerns regarding selection bias and the under-representation of patients with poorer outcomes. 19 Moreover, existing studies have largely focused on survival and global quality of life (QoL) metrics, with limited evaluation of functional disability, participation outcomes and unmet supportive care needs.
Thus, the primary objective of this study is to comprehensively evaluate the longer-term residual physical disability, functional and participation outcomes in an Australian community cohort of patients with CRCPM following CRS-HIPEC. Further, outcomes in a contemporaneous PMP cohort were included to contextualise the findings across patients with peritoneal metastasis after CRS-HIPEC. The results will inform patient selection, enhance pre-operative counselling, guide targeted rehabilitation planning and contribute to improving longer-term CRC survivorship care.
Materials and Methods
Study Design
A cross-sectional study was conducted using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) criteria 21 and approved by the Institutional Research and Ethics Committee (HREC/100818/PMCC).
Participants and Setting
Box 1. Participants’ inclusion and exclusion criteria

Procedure
Data collection. Based on study selection criteria, all eligible patients identified in the PMCC database were invited by a trained research assistant and two authors (MY, AE) to participate via telephone or email. A research officer followed up within a week to provide additional details concerning the study. Those who consented were recruited and interview appointments were scheduled based on availability and convenience. The trained research assistant and two authors (MY, AE) conducted all interviews and assessments (approximately 30–35 min) using a structured format via telephone or online communication platforms (e.g., Skype, Zoom, MS Teams). Data collection used standardized instruments (see Measures). Assistance was offered only when participants experienced difficulty completing the questionnaires, and appropriate rest breaks were provided as required during data collection sessions.
Outcome Measures
Sociodemographic data and CRC-related clinical characteristics data were collected from the electronic medical records by the trained research assistants and two authors (MY, AE). Pain prevalence was defined as the self-reported presence of pain (binary yes/no), irrespective of intensity, while pain severity was assessed separately using a 0–10 Visual Analogue Scale (VAS). The International Classification of Functioning, Disability and Health (ICF) 22 was used as a conceptual basis for the choice of the best outcomes for measurement.
Clinical Functioning Information Tool (ClinFIT) 23 is an ICF-based 30-item tool designed to assess “functioning” and disability: 9 items in the “Body Functions” domain, and 21 items in the “Activities and Participation” domain. Patient functioning in each of these clinically meaningful descriptions was assessed using an 11-point numeric rating scale (0 = no problem to 10 = complete problem). It also includes the ICF Generic-7 Set, which captures a minimum set of functioning information in 7 categories that can be collected across various health conditions and clinical settings. ClinFIT was selected as the primary functioning measure in this study for its broader ICF-based assessment of functioning.
Depression Anxiety Stress Scale- 21 (DASS) 24 comprises three 7-item self-report subscales measuring the negative emotional states of depression, anxiety, and stress. Participants rated the extent to which they experienced each state over the past week on a 4-point Likert scale, with higher scores indicating greater psychological distress. 24
European Quality of Life Scale (EQ-5D-5L) 25 assessed overall QoL in 5 health dimensions: mobility, selfcare, daily activity, pain/discomfort, and anxiety/depression, with responses on 5 ordinal levels: no problems (0) to extreme problems (4). Participants’ current overall health was assessed using the sixth item with a visual analogue scale (VAS) from 0 (worst health state) to 100 (best health state).
Functional Assessment of Cancer Therapy-Colorectal (FACT-C) scale 26 assessed HRQoL in the following domains: physical, functional, social/family, emotional well-being, and colorectal cancer specific. Participants rated the extent to which each item applied to them during the past 7 days using a 5-point Likert scale (0 = not at all to 4 = very much).
Community Integration Measure-Revised (CIQ-R) 27 assessed community participation across 4 subscales: home integration, social integration, productivity, and electronic social networking.
Data Analysis and Statistics
Descriptive statistics summarized participant characteristics, with continuous variables presented as mean ± standard deviation (SD) or median [interquartile range (IQR)], and categorical variables as frequencies and percentages. Mann-Whitney U tests were conducted to compare scores on each of the outcome measures for CRCPM and PMP subgroups. In addition, multiple linear regression was conducted to evaluate the independent associations between potential sociodemographic and clinical variables of interest (e.g., variables with significant associations or those with theoretical importance) with the outcome measure scores. Assumptions of linearity, normality of residuals, homoscedasticity, and absence of multicollinearity were checked prior to the modelling. A backward selection method was applied, starting with all candidate variables in the model. Variables are removed one at a time, starting with a significance threshold of p < 0.05. The independent variables were categorized as follows: age and time since diagnosis as continuous variables; time since CRS-HIPEC <2 (reference) vs ≥ 2 years, treatment type: chemotherapy or radiotherapy (reference) vs none, comorbidity: present (reference) vs absent; marital status: married (reference) vs single/divorced; employment: employed (reference) vs unemployed/retired/student; symptoms: recurring pain or fatigue (reference) vs no symptoms; and rehabilitation: inpatient or community rehabilitation (reference) vs none. Formal interaction testing between subgroups (CRCPM and PMP) and predictor variables was not undertaken. Given the exploratory nature of this study and the interrelated nature of the outcome measures (functioning, psychological well-being, quality of life, and participation), formal correction for multiple comparisons (e.g., Bonferroni adjustment) was not applied, as such approaches may substantially increase the risk of Type II error and obscure potentially meaningful associations. All statistical analyses were performed using IBM SPSS for Windows, version 22.0 (IBM Corp, Armonk, NY, USA), with statistical significance set at p < 0.05 (two-sided).
Results
Sample Characteristics
Demographic and Clinical Characteristics of the Participants
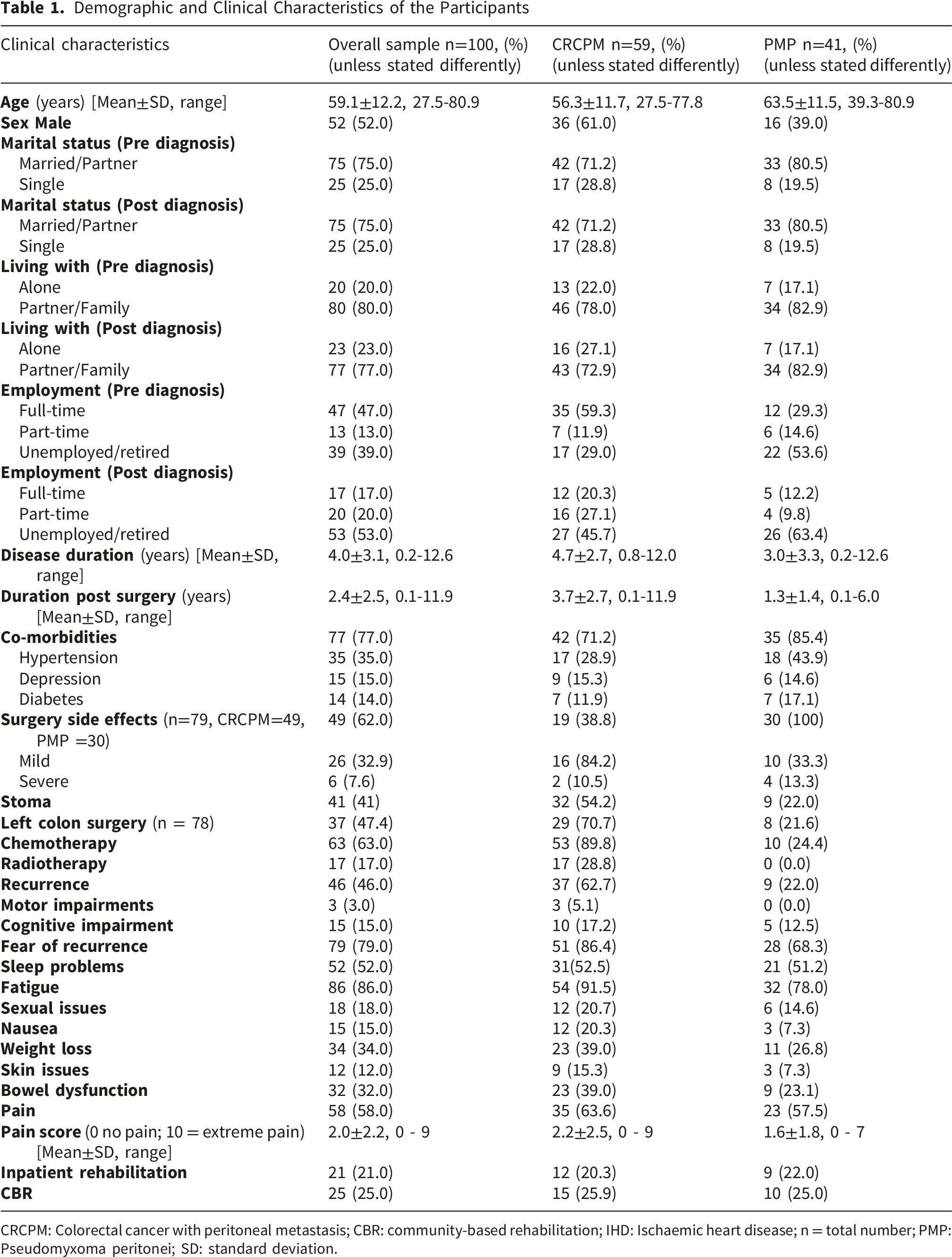
CRCPM: Colorectal cancer with peritoneal metastasis; CBR: community-based rehabilitation; IHD: Ischaemic heart disease; n = total number; PMP: Pseudomyxoma peritonei; SD: standard deviation.
The clinical characteristics of the participants are shown in Table 1. Overall, the mean time since CRS-HIPEC surgery was 2.4±2.5 years. Comorbidities were common in both cohorts (overall 77%; 71% in CRCPM and 85% in PMP), most frequently hypertension (35%), followed by depression (15%). Stoma was present in 41% of the participants (54% in CRCPM and 22% in PMP), and 26% underwent stoma reversal. More participants with CRCPM received chemotherapy (90% vs 24%) and radiotherapy (29% vs 0%) compared with PMP. Further, disease recurrence was more frequent in the CRCPM cohort (62.7% vs 22% PMP). Uptake of rehabilitation was low overall, with 21% participants accessing inpatient rehabilitation and 25% had participated in community-based rehabilitation programmes.
Participant-Reported Symptoms/Impairments
Table 1 shows the persistent symptoms and impairments in the participants. Overall, despite relatively low levels of objective motor impairment, participants indicated a high persistent symptom burden driven by systemic, visceral, and psychosocial impairments in the longer-term after CRS-HIPEC. Over half of participants reported pain (58%), although pain intensity was generally low (mean±standard deviation (M±SD): 2.0±2.2 on a 0–10 VAS scale). As expected, participants with PMP reported a lower burden of persistent symptoms across all domains and fewer impairments than the CRCPM cohort (Table 1). Recurrence was significantly more frequent in the CRCPM subgroup than the PMP subgroup (62.7% vs 22.0%, p<0.05), and fear of recurrence was likewise more prevalent in the CRCPM subgroup (86.4% vs 68.3%, p <0.05).
Current Level of Functioning, Participation, Psychological Wellbeing, and QoL
Comparative Statistics for Outcome Measures
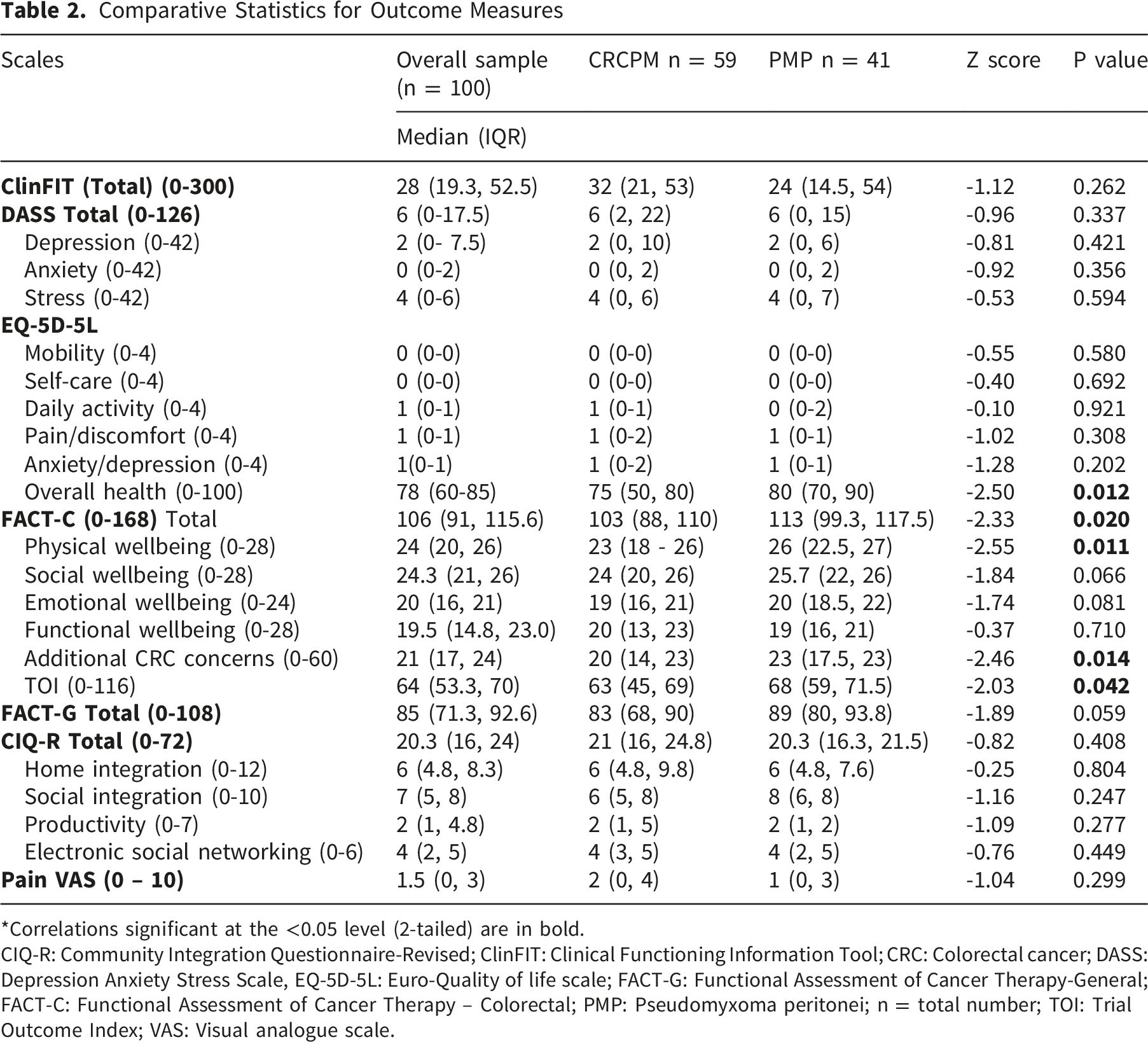
*Correlations significant at the <0.05 level (2-tailed) are in bold.
CIQ-R: Community Integration Questionnaire-Revised; ClinFIT: Clinical Functioning Information Tool; CRC: Colorectal cancer; DASS: Depression Anxiety Stress Scale, EQ-5D-5L: Euro-Quality of life scale; FACT-G: Functional Assessment of Cancer Therapy-General; FACT-C: Functional Assessment of Cancer Therapy – Colorectal; PMP: Pseudomyxoma peritonei; n = total number; TOI: Trial Outcome Index; VAS: Visual analogue scale.
Given the substantial differences in treatment exposure, recurrence rates, and clinical characteristics between the CRCPM and PMP subgroups, between-group comparisons should be interpreted cautiously. Nevertheless, exploratory comparative analyses revealed broadly similar outcomes across most functioning, psychological well-being, and participation domains. Likewise, no significant between-group differences were observed across all EQ-5D-5L domains of mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. However, compared with CRCPM, PMP survivors demonstrated significantly better HRQoL (EQ-5D-5L overall health scores: p = 0.012), and cancer-specific QoL (FACT-C total scores: p = 0.020). This difference was driven primarily by higher physical well-being scores and fewer additional cancer-specific concerns among PMP participants (p = 0.011 and 0.014, respectively). PMP survivors also demonstrated higher Trial Outcome Index (TOI) scores, indicating better combined physical and functional well-being.
Factors Associated With the Current Level of Functioning and Well-Being - Summary of Univariate and Multivariate Findings
The results from multivariate linear regression models are detailed in Table 3 A-C (Supplementary), and key findings are summarized below: • • • • • • •
Discussion
This study provides a comprehensive overview of longer-term functioning and participation outcomes among individuals with CRCPM/PMP following CRS-HIPEC. Overall, CRCPM/PMP survivors experience a high prevalence of physical symptom burden and participation restriction (in productive and domestic roles), despite relatively preserved basic functioning and a low level of psychological distress. While functional limitation and participation outcomes were broadly comparable between the two subgroups, individuals with PMP reported a lower symptom burden and more favourable perceptions of general health and cancer-specific QoL. These distinctions highlight the importance of considering cancer subtype when evaluating survivorship outcomes and tailoring longer-term supportive and rehabilitation interventions.
This study demonstrates a high prevalence of persisting physical burden (including fatigue, pain, sleep disturbance, fear of recurrence, and bowel dysfunction) in CRCPM/PMP survivors following CRS-HIPEC. Consistent with our findings, Balachandran et al 28 prospectively evaluated a comparable Danish cohort, reported a high prevalence of biopsychosocial late effects at 12 months post-surgery, including fear of recurrence (65%), fatigue (40%), and insomnia (33%). Pain was prevalent after CRS-HIPEC (58%), although its intensity was generally low in this cohort. In line with Balachandran et al, 28 who also found that pain improved over time. Our study demonstrated a higher prevalence of fatigue (86%), similar to findings from another study of CRC survivors, in which 77% participants reported persisting fatigue. 9 PMP is associated with a lower burden of persistent symptoms across all domains and fewer impairments than CRCPM. The difference may partly related to greater treatment burden in the CRCPM subgroup, with more participants received chemotherapy (90% vs 24%) and radiotherapy (29% vs 0%) than those with PMP. Further, this study found that persisting symptom burden independently predicted poorer outcomes across activity, participation, and QoL domains, consistent with a prior study reporting lower QoL among patients with moderate-to-severe residual symptoms. 28 Symptom-related impairments appear to predict worse activity limitation and participation restriction in CRCPM than in PMP, suggesting that the CRCPM subgroup may be more susceptible to the broader impact of physical burdens.
Beyond persistent symptom burden, personal factors (including age and employment status), were also independent predictors of longer-term functioning, psychological well-being, QoL and participation outcomes after CRS-HIPEC. In the context of prior literature reporting higher morbidity and mortality among older patients undergoing CRS-HIPEC, 29 these findings further suggest that older patients constitute a high-risk subgroup and may benefit from targeted rehabilitation interventions delivered peri-operatively and extended into longer-term follow-up. Moreover, participation restriction emerged as a prominent feature amongst participants during longer-term recovery. Despite relative preservation of overall social integration and electronic social networking, participants demonstrated reduced engagement in home-based activities and productivity. Females were independently associated with reduced home integration and higher pain/discomfort scores, which were more evident in the CRCPM cohort than in PMP. Laghousi et al 30 in a cross-sectional study demonstrated similar findings, suggesting women with CRC experience more social functioning difficulties and more fatigue and pain than men. These findings reinforce gender-specific participation challenges in CRC survivorship. Notably, full-time employment rates declined markedly from 47% to 17% after cancer diagnosis. Overall, unemployment was an independent predictor of worse functioning, higher psychological distress, poorer QoL and reduced productivity-related community integration. These findings reflect the broader socio-economic burden of CRS-HIPEC survivorship, with implications for financial security, social role participation and overall wellbeing. This is consistent with qualitative findings by Lim et al, 31 in which advanced CRC survivors who were unable to return to work experienced higher distress and lower QoL. Previous studies reported a higher return to work rate in participants with PMP (90%) than CRC (60%) after cancer treatment,32,33 suggesting a possible higher level of unmet vocational rehabilitation needs in the CRC subgroup. These findings highlight the importance of symptom-targeted and participation-focused rehabilitation strategies to optimise CRCPM survivorship outcomes following CRS-HIPEC. Collectively, these findings underscore the need for age-tailored rehabilitation programme for CRS-HIPEC survivors, including vocational support for younger individuals with employment goals and comorbidity-focused holistic care for older adults.
Further, the findings demonstrated different factors in predicting survivorship profiles between CRCPM and PMP following CRS-HIPEC. In PMP survivors, longer-term functional and participation outcomes are primarily driven by age and symptom-related impairments. While in CRCPM survivors, employment status and symptom burden have more persistent influence across functioning, participation, and QoL domains. From an ICF perspective, participation restrictions and inferior QoL in CRC survivors are more strongly shaped by personal and contextual factors, while in PMP survivors, physical impairments and aging play a more central role. These findings reinforce the need for tailored rehabilitation and survivorship care models based on cancer subtypes and highlight the importance of addressing the contextual factors in improving longer-term survivorship outcomes.
Interestingly, despite the high prevalence of persistent symptom burden observed in this study, overall QoL appears largely preserved in both cohorts. This finding aligns with prior studies reporting that QoL following CRS-HIPEC either improves or remains stable beyond 6-12 months of surgery.19,20,34 Existing studies showed additional negative predictors of HRQoL following CRS-HIPEC include female sex, extensive or residual disease, postoperative complications, stoma placement, adjuvant chemotherapy and disease recurrence.19,35 In our study, the presence of stoma demonstrated some increased association with emotional stress and CRC-specific concerns in CRCPM but not in PMP, indicating differential psychosocial impacts of disease- and treatment-related bodily changes. Further, a notably high prevalence of fear of recurrence (79%) was observed in this cohort and in the study by Balachandran et al, 28 more than the broader CRC populations (48-50%),9,36 suggesting heightened psychological concern among survivors after CRS-HIPEC. In contrast, overall psychological distress levels measured by DASS were low in this study (Median [IQR]: 6 [0–17.5]) and comparable to normative values. 37 Despite ongoing physical and functional limitations, the overall QoL and psychological wellbeing remains relatively preserved. This may reflect complex psychological adaptation processes following surgery, including response shift phenomenon and post-traumatic growth, as previously described in cancer survivorship literature.9,35 These psychological changes may be influenced by reassurance derived from the perceived survival benefit of CRS-HIPEC, as well as shifts in priorities and life philosophy following intensive cancer treatment.35,38 Further research is needed to better understand these adaptive processes and to address the unmet physical, psychological, functional and social integration needs within CRCPM/PMP survivorship care.
Importantly, the high prevalence of persistent symptom burden and participation restrictions contrasted with the low uptake of inpatient rehabilitation and community-based rehabilitation programmes, indicating substantial unmet rehabilitation needs after CRS-HIPEC. Similar levels of unmet need have been reported in the broader metastatic CRC cohorts, 39 highlighting this population as a priority group for rehabilitation interventions. Low rates of referrals to cancer rehabilitation programmes have also been observed in prior studies, potentially reflecting under-recognition of rehabilitation needs in cancer care and limited integration of rehabilitation services within existing cancer care models.40,41 A similar gap existed at PMCC, where no standardized rehabilitation referral criteria or systematic screening processes were in place. In parallel, published CRC guidelines provide little rehabilitation guidance despite acknowledging the importance of multidisciplinary survivorship care, and the lack of specific rehabilitation recommendations further impedes the routine incorporation of rehabilitation into clinical practice. 42 Future CRC rehabilitation pathway should incorporate specific referral triggers, such as poorer functioning on ClinFIT, increased psychological distress on the DASS, reduced QoL on EQ-5D-5L or FACT-C, lower participation on CIQ-R and higher risk contextual factors including older adults and unemployment. Collectively, this study highlight the persisting gaps in the rehabilitation delivery across the CRC care continuum, from the time of diagnosis through to longer-term community survivorship. Further efforts are required to improve access to and integration of rehabilitation services to address the substantial unmet needs of this growing survivor population.
Study Limitations
This is a descriptive analytical study without a control group, limiting the ability to establish causal relationships. The study cohort comprised a selective group of participants who agreed to participate from a single tertiary metropolitan institution listed within a CRCPM and PMP database following CRS-HIPEC, potentially restricting the generalizability of the findings to other settings or populations. For instance, the findings may not fully reflect the experience of rural patients, who may face reduced access to specialised multidisciplinary cancer care. However, the cohort included all CRCPM episodes since 2013 and PMP episodes since 2021, covered a wide geographical area, making it broadly representative of patients living with peritoneal metastasis in the community. Additionally, the demographic and clinical characteristics of participants are comparable to those reported in other metastatic CRCPM/PMP cohorts. Our study cohort comprises a high proportion of CRCPM, which is the primary group of patients referred to the CRC rehabilitation clinic at PMCC and the primary interest in this study. Analysis of the underlying differences in outcomes between the CRCPM and PMP subgroups was beyond the scope of this study. Several potentially influential factors on patient outcomes, such as pre-diagnosis functional and cognitive levels, socioeconomic status, and cultural considerations, were not evaluated in this study. Furthermore, this study did not employ a defined minimum post-discharge interval as part of the inclusion criteria, which may have limited the comparability of participants’ community reintegration experiences. Establishing such a criterion could improve consistency in future research and is an important consideration for study design. Despite employing a comprehensive set of validated tools to assess functioning, QoL, and community reintegration, some relevant issues may fall outside the domains of captured by these measures and therefore could not be reliably assessed. To minimize recall bias, all outcomes were limited to the participants’ current status, and clinical and demographic data were cross-verified using electronic medical records. The large number of multivariate regression analyses performed also warrants cautious interpretation. This analytical approach aligns with the study’s exploratory nature and the cross-sectional design, which prevents any inference of causality. Potential confounders and interaction effects were not explored in depth, and no correction for multiple comparisons was applied, which may increase the risk of Type I error.
Conclusion
This study demonstrates that CRCPM/PMP survivors experience a high prevalence of persistent symptom burden (such as fatigue, pain, emotional distress) following CRS-HIPEC. The findings align with the WHO ICF framework, demonstrating that these physical symptoms translate into longer-term activity limitation and participation restriction, shaped by contextual factors such as personal (age, employment, gender) and treatment-related (stoma, radiotherapy, etc). Older age and unemployment emerged as independent predictors for poorer functional outcomes overall, suggesting the need for tailored age-specific support programmes and integrated vocational interventions in this patient population. Compared to CRCPM, PMP has a lower burden of persistent symptoms and a more favourable QoL profile. In CRCPM, the longer-term functional and participation outcomes were particularly influenced by unemployment, high symptom burden, female gender, presence of stoma and history of radiotherapy. These findings emphasise the need for integrated cancer survivorship care models that prioritise the higher-risk subgroups and optimise longer-term outcomes for CRCPM survivors following CRS-HIPEC. Beyond post-operative follow-up, these findings may help inform patient selection for CRS-HIPEC and strengthen pre-operative counselling, by supporting cancer-specific and shared decision-making regarding expected recovery trajectories and longer-term outcomes. Notably, rehabilitation uptake remained low despite high unmet supportive care needs after CRS-HIPEC, underscoring the need for improved rehabilitation service integration. Future research should focus on strengthening rehabilitation services delivery and integration across the CRC care continuum by early identification of rehabilitation needs in high-risk patient subgroups, development of routine referral triggers within CRC care pathways, and incorporating specific rehabilitation recommendations into CRC clinical practice guidelines.
Supplemental Material
Supplemental Material - Functional and Participation Outcomes of Colorectal Cancer With Peritoneal Metastasis and Pseudomyxoma Peritonei Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (CRS-HIPEC): A Cross-Sectional Survivorship Study
Supplemental Material for Functional and Participation Outcomes of Colorectal Cancer With Peritoneal Metastasis and Pseudomyxoma Peritonei Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (CRS-HIPEC): A Cross-Sectional Survivorship Study by Mengzhe Yang, Bhasker Amatya, Alaeldin Elmalik, Krystal Song, Helen Mohan, Alexander Heriot, Fary Khan in Advances in Rehabilitation Science and Practice
Footnotes
Acknowledgement
The authors thank all participants in this study and Loren Oscari for conducting participant interviews and data entry. The authors acknowledge Dr Amanda Liesegang and the Colorectal Cancer Care team at Peter MacCallum Cancer Centre for their invaluable support.
Ethical Considerations
This project was approved by the Peter MacCallum Cancer Centre Research and Ethics Committee (HREC/100818/PMCC).
Consent to Participate
All participants provided informed consent prior to participation in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through internal resources of the Rehabilitation Department, Peter MacCallum Cancer Centre, and Royal Melbourne Hospital, Australia.
Declaration of Conflicting Interests
The authors declare no conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The data associated with the manuscript are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.