
Abstract
Background
Ambulance services increasingly attend mental health crises, where safe non-conveyance is appropriate but inconsistently achieved. Training gaps and organisational constraints, e.g. unclear guidance, limited referral pathways, and weak interagency collaboration, constrain practice and foster a risk-averse culture that defaults to conveyance in ways that might undermine patient autonomy.
Aim
This study aimed to explore key challenges faced by ambulance clinicians when managing people in mental health crises within the current Norwegian healthcare system.
Methods
We conducted eight semi-structured group interviews across three of four Regional Health Trusts in Norway. Key themes were identified using Braun and Clarke's Reflexive Thematic Analysis (2022) and interpreted in light of Schein and Schein's (2017) theory of organisational culture within a critical realist perspective.
Results
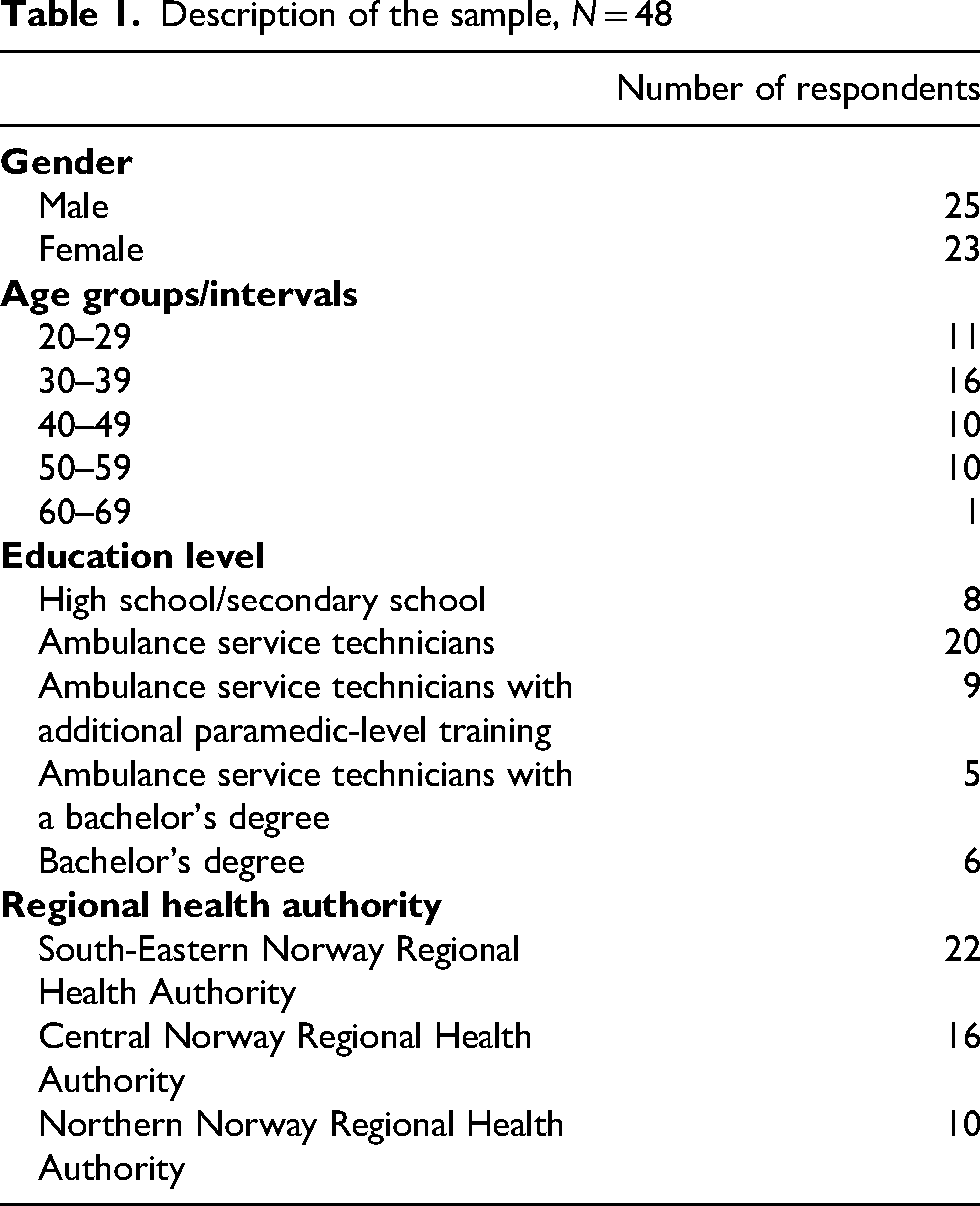
A total of 48 ambulance clinicians participated. Participants reported gaps in formal mental health education and training, lack of guidelines and templates, and limited referral options, which often made conveyance the perceived safer, more straightforward option. This can have consequences for on-scene practices and further care trajectories for patients who do not want the healthcare offered or whose decision-making capacity is in question, and/or there is fear of adverse outcomes if patients are not conveyed. In such situations, the above factors can lead to an over-reliance on conveyance to specialist clinicians, preferably a physician, and also potentially limit patients’ autonomy to remain on-scene when appropriate.
Conclusion
The findings highlight how organisational culture, particularly weak managerial support and risk-averse norms, are experienced to directly influence conveyance practices. This might indirectly impact the extent to which patients’ autonomy is upheld. Strengthening training, referral pathways, inter-agency agreement and managerial support might help shift current practice towards person-centred care.
Keywords
Introduction
Studies from Finland, 1 the United Kingdom2–4 and Australia5,6 show that ambulance services are increasingly responding to patients in mental health-related crises, yet ambulance clinicians (AC) report difficulties in managing these presentations within current systems. Studies from Norway,7,8 the United Kingdom9,10 and Australia 11 indicate that many clinicians feel unprepared to assess and manage patients in mental health crises, citing gaps in education on critical topics such as communication skills and how to apply complex mental health legislation. Here, ‘mental health crises’ is defined as ‘any circumstance or event of distress occurring, in which support is needed or sought from outside of one's immediate social network’. 12 Nonetheless, ambulance services and emergency medical communication centres, by virtue of their 24/7 availability, frequently fill gaps left by mental health services and serve as a ‘safety net’ for patients in crises.12–14
As prehospital practice has professionalised15–17 and on-scene capability has been enhanced, non-conveyance has become feasible in selected cases. 18 Non-conveyance refers to situations where an ambulance is dispatched but, following assessment and/or treatment at the scene, it is determined that the patient does not require conveyance to specialised clinicians, 19 an approach that may be relevant in mental health crises as well as for patients with injuries and illnesses that can be attended to by ACs at home. 18 Internationally, as healthcare demand rises and health systems face financial pressure, emergency medcial services are increasingly filling gaps in care – often in ad hoc ways and without matching resources.18,20–23 In this context, organisational factors (e.g. guidelines, perceived management support or lack thereof, referral options) appear to shape clinicians’ practices and attitudes towards conveyance versus non-conveyance. Leaving patients at home entails a higher risk for complaints and regulatory investigations, and this might lead some to convey patients to specialist services as a risk-management strategy.7,24,25 These influences intersect with rights-based commitments in healthcare systems, where respect for patients’ rights, human dignity, and autonomy are foundational. 26 Here, autonomy refers to a person's capacity and right to make informed, voluntary decisions about their care, free from coercion or undue influence. Within healthcare ethics, respect for autonomy entails acknowledging individuals as moral agents capable of deliberation and self-determination, and it places an obligation on healthcare professionals to support patients’ informed decision-making through adequate information, understanding, and consent. 27 Autonomy is therefore closely linked to concepts such as informed consent, patients’ decision-making capacity, and respect for personal values.
The expansion of on-scene capability and the growing prevalence of mental-health-related presentations place ACs at the centre of high-stakes decisions regarding patient disposition, including non-conveyance. In mental health crises, these decisions are further shaped by the perceived lack of formal mental health care education among ACs, organisational deficiencies, complex legislation, and the duty to respect patient autonomy within rights-based healthcare systems.
Against this backdrop, this article aims to explore key challenges faced by ACs in managing people in mental health crisis within the current Norwegian healthcare system. 28
Methodology
Study design and theory
Data were analysed using Braun and Clarke's reflexive thematic analysis (RTA), 29 adopting an inductive data-driven orientation. Coding and theme development were grounded in ACs accounts while recognising the researcher's active, interpretative role in knowledge production. 29 In the discussion, Schein and Schein's theory of organisational culture 30 was applied with a critical realist perspective.31,32 From a critical realist standpoint, a mind-independent reality exists, while understandings of that reality are shaped through personal, social, historical, and cultural contexts. 31 Consistent with this stance, our inferential move relied on retroduction – reasoning from observed patterns to the underlying generative mechanisms that would have to exist for those patterns to occur. To operationalise this logic, we drew on Schein and Schein`s (2017) account of organisational culture as the collective learning and shared experiences of a group, that develop through addressing challenges of adaptation and integration. They conceptualise culture at three interrelated levels: artefacts – visible, tangible manifestations such as routines, protocols, physical layout and documented practices; espoused values – the stated beliefs, priorities and goals leaders and members claim to follow; and basic underlying assumptions – deep, often unconscious beliefs that actually guide behaviour. 30 Bringing these perspectives together enabled an analytic focus on the meaning-making processes through which clinicians interpret and respond to organisational demands and constraints.
Group interviews were chosen because the shared storytelling and interaction among participants can stimulate recall, clarify perspectives, and generate deeper insights into both individual and collective experiences. 33 A semi-structured approach was selected to enable open exploration of relevant topics while ensuring that all groups discussed the same topics. 34 We prioritised breadth in clinical contexts and participant characteristics to yield rich and varied perspectives. Eight interviews were planned for reasons of feasibility and were judged to have generated rich data and well-developed insights to address the research aim, supporting interpretations that move beyond descriptions to offer theoretically informed explanations of clinicians’ experiences, as suggested by Braun and Clarke. 35
Researchers’ positionality and reflexivity
The first author, who conducted the interviews and led the analysis, is a nurse and a paramedic with more than 20 years of experience in the ambulance services. Professional encounters with patients experiencing mental health difficulties motivated the present study and sensitised the interpretative lens applied during analysis. Reflexive journaling and collaborative discussions with co-authors and an advisory board were used to examine how prior experience and assumptions might influence coding decisions and theme development.
This project was supported by an advisory board comprising individuals with lived experience of mental health challenges, substance abuse and caregiving, alongside ACs, legal and psychiatric professionals. The PhD supervisors contributed complementary expertise in sociology, nursing, and general practice. All co-authors took part in advisory board meetings, and together, they have provided critique, guidance and insight which have informed the project's design, recruitment, analysis, and interpretation. We believe this collaborative approach enhances the project's validity and ensures its relevance. 36
Recruitment and interviews
A convenience sample of ACs was recruited using the snowball method. Members of the advisory board helped us engage with the ambulance station managers, clinical ambulance development staff, and ‘local ambulance champions’. These individuals played a key role in the study by distributing invitations to ACs, recruiting participants to the group interviews, and coordinating the scheduling and locations for the interviews.
The interviews were conducted between December 2022 and June 2023 at or in close proximity to the local ambulance station. The interviews were facilitated by the first author and limited to two hours. The interviews were recorded using the Nettskjema-diktafon app. 37 Nettskjema was used as a mediator to store the audio recordings directly on the safe storage in Tjenester for Sensitive Data (Services for sensitive data). 38 Some ambulance services were able to compensate their employees using time reserved for clinical development in their shift schedule. Other respondents participated in their free time.
Participants
We aimed to include participants who were ACs with ≥2 years’ experience and for groups to consist of 4–8 participants and sought to include participants with diverse educational backgrounds. In practice, group interviews included 4–11 participants per session, with experience spanning 0–30 years. One session included a temporary substitute with no prior AC experience. We retained this participant to preserve the naturalistic context of the on-duty team, consistent with our critical realist emphasis on real-world organisational conditions. Two sessions included one participant (each) who also held a management role.
Ethics
The Regional Committees for Medical and Health Research Ethics (reference 516477/REK South-East) deemed that the study was outside the scope of the Health Research Act. The Norwegian Centre for Research Data (reference 903381), the Data Protection Officer at each local health trust (not included for confidentiality reasons), and the management of each ambulance service granted their approval of the study. All respondents voluntarily provided signed informed consent declarations and were encouraged to treat the information disclosed in the interview as confidential. The interviews were transcribed verbatim by the first author and deidentified during the transcription process.
Data analysis
Coding was done inductively with iterative movement between the data, codes and candidate themes. The first author undertook coding and theme construction, with input from the co-authors and the advisory board at multiple stages. NVivo 12 software 1.7.2 (1560) was used to manage and code data. 39 Quotations are labelled by two numerals, the first denotes the group interview and the second the participant (e.g. Resp. 1-2).
The theoretical lens of Schein and Schein's (2017) theory of organisational culture was applied in the discussion to contextualise findings, consistent with our inductive approach.
Results
The next section presents participants' characteristics (Table 1) and the results of the RTA of the group interviews (Figure l). Figure 1 shows the main themes and subthemes that were developed in the data analyses and how these themes are interrelated. We outline their content next.
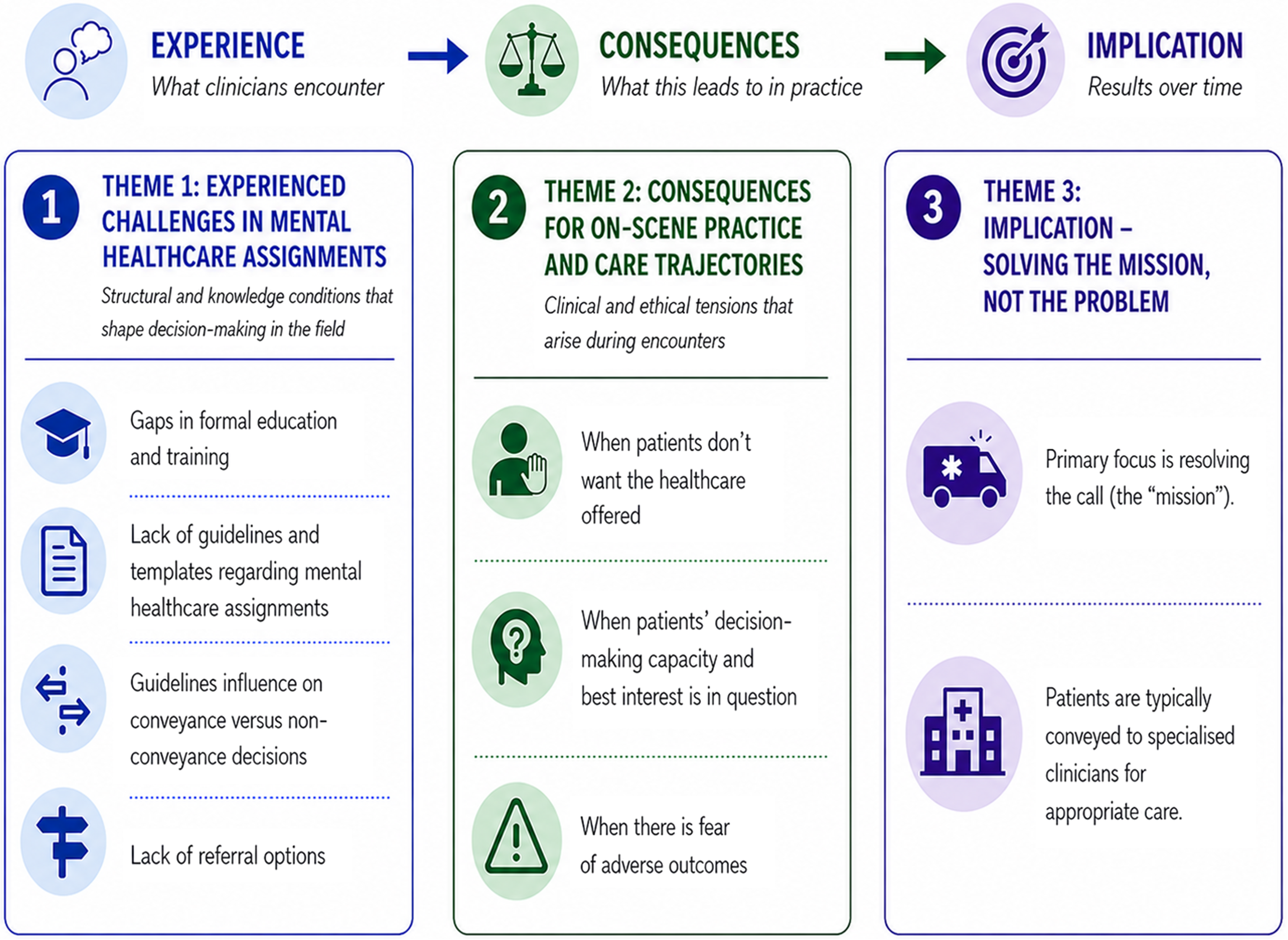
Overview of themes and subthemes – From experienced challenges to practice implications in mental healthcare assignments. (Figure visualisation developed with assistance from ChatGPT (OpenAI).)
Description of the sample, N = 48
Experienced challenges in mental healthcare assignments
Gaps in formal education and training
Respondents commonly expressed uncertainties in cases where mental health problems were the primary concern and explained that their assessment relied on practical experience and on-the-job knowledge more than on formal education and training. In all groups it was noted that formal education placed significantly less emphasis on psychiatry and mental health compared to the treatment of other medical conditions or physical trauma. One respondent summarised this gap, stating: ‘That's where we are weakest – psychiatry’ (resp. 9-4). Many others also highlighted a lack of focus on psychiatry in their ambulance service training. As a result, they often relied on their personal experience, gut feeling, and knowledge acquired from ad hoc sources, as illustrated by this quote: […] What I have learned about psychiatry, I have learned from my sister. She works in the field, you know (resp. 2-3).
Some respondents emphasised that their limited knowledge meant they had difficulty describing or communicating signs and symptoms when assessing mental health conditions. This made it challenging to articulate their impressions of the patient, for example when consulting with a physician. As one respondent noted: ‘[…] I can’t really put it into words properly […]’ (resp. 2-6). Additionally, some respondents explained that this lack of ability to describe and communicate signs and symptoms made it difficult to provide concrete and persuasive arguments for the necessity of care to the patients, as one respondent noted: Resp. 3-3: And then there's also the issue with somatic, because it's easier to argue (for the necessity of care) when you have some findings…. I mean, some concrete findings. You can say to a patient, ‘Look, here's your ECG (electrocardiogram), and here you can see … here it jumps and skips, your pulse is irregular, and your oxygen saturation is low,’ and so on…. You have specific measurement points, like your blood pressure isn’t good, and I think it's clear that we should…. I mean, it's more concrete than just telling someone, ‘You … you're crazy’ (laughs a little). Researcher: Mm. (several laughs, one loudly) Resp. 3-3: It … it's difficult to argue.
Lack of guidelines and templates regarding mental healthcare assignments
In the Norwegian model, ambulances are not staffed by physicians; instead, ACs assess and deliver care independently within the framework of national legislation and the protocols and procedures of each local health trust. Local health trusts are organised within four state-owned Regional Health Authorities that are accountable to the Ministry of Health and Care Services, which, pursuant to national law, sets national policy and allocates funding.
28
In most of the groups, respondents discussed that medical assignments are typically supported by templates and clear guidelines, whereas assignments involving mental health lack such structured guidance: ‘There's no clear procedure or definitive answer for those kinds of assignments [regarding mental health issues]’ (resp. 6-4). Several respondents across groups indicated uncertainty about what to assess and how to proceed with mental health-related assignments. One respondent described these assignments as vague compared to medical ones, explaining: Resp. 1-1: There's nothing for us to document. Resp. 8-1: …no template, I’ve got nothing. Absolutely nothing, actually. (Soft “no”) Resp. 8-1: Like, there's nothing written down anywhere where I can tick a box or say, “Yeah, I’ve done that.” It's that whole vague thing. We don’t have anything…. I haven’t done an ECG (electrocardiogram), or any of those concrete things. Resp. 2-1: But … if we had those kinds of checklists for everything related to psychiatry, where we just tick off that we’ve done this and this and this, I don’t think we’d necessarily always provide the best care for the patient. But we’d protect ourselves. Because we know that if we follow all the steps, the system will back us up if the patient feels it wasn’t enough and ends up taking their own life.
Guidelines influence on conveyance versus non-conveyance practices
From the respondents’ discussions, it appears that organisational guidelines strongly influenced AC's practice, and that choosing conveyance was frequently considered the safer, more straightforward option. One group stated that leaving a patient on-scene was generally considered non-compliant with their guidelines: ‘[…] And again, we are an ambulance service, where we're not supposed to leave anyone on-scene, especially not those [patients with mental health issues]’ (resp.−1).
In contrast, the other groups acknowledged the possibility of leaving patients on-scene but emphasised that such decisions required thorough examination. This process was challenging if the patient refused to cooperate: Yeah, we do have procedures for leaving them (patients) at home, but there's supposed to be a pretty thorough examination, and it has to be cleared with a doctor. But if they also refuse to … let us examine them, for example—because our procedure says we’re supposed to […] and, uh … not all patients agree to that (resp. 3-3).
In all group interviews, respondents expressed that conveyance of all patients – regardless of their condition – to specialist clinicians, preferably a physician, was perceived as the safer option. This approach was largely driven by two overlapping fears: adverse patient outcome (harm, clinical deterioration, or, in the most severe cases, death) and organisational repercussions (complaints and potential regulatory investigations). We use ‘adverse outcomes’ in this broader sense. (The domains are further unpacked in the subtheme ‘When there is fear of adverse outcomes’.) However, they also discussed situations where, after assessing the patient and the circumstances on-scene, they determined that conveyance to a physician might not be necessary. One respondent explained a situation where the immediate crisis had subsided: Resp. 4-6: […] we go out, talk to them, spend a bit of time with them, and then maybe they realise, or we agree, that it's not … maybe not as bad as it seems. You know, it's often like that on the weekends, right? And you’re not solving problems at the out-of-hours clinic for the municipality at 3:30 in the morning on a Sunday, you know? So, then we encourage them to get in touch with their regular GP instead.
Lack of referral options
Across groups, there seemed to be a consensus that the available referral options for patients with mental health issues were limited to the general practitioner (GP) or the out-of-hours emergency primary healthcare services. When asked about contacting other municipal healthcare services, such as district psychiatric centres or assertive community treatment teams, some respondents said: Resp. 6 -1: “… [wève tried] several times.” Resp. 3 -1: “During the opening hours, we’ve done that.” Resp. 1 -1: “Called the psychologist too.” Resp. ?-1: “But they’re usually available until 3:30, and then it kind of falls apart after that.” Resp. 8 -1: […] The point is, for that patient, they have a psychologist, a contact person at the DPS (District Psychiatric Center), and that's between eight and three. So, it works then. Maybe you get an emergency appointment with the psychologist and take them there.” Resp. 2 -1: “But it's often … like we say, it usually happens in the evenings, on holidays, or at night, and in many cases, as I’ve experienced, it's because the DPS or the psychologist isn’t available, so they end up calling us. Or they end up with us.” (Several sounds of agreement)
In challenging situations, such as when patients expressed suicidal thoughts but refused conveyance, respondents found it extremely helpful to call a physician to the scene. Some respondents noted that certain out-of-hours emergency services operated an emergency response car staffed with a physician, which was described as important support: ‘It's gotten a lot easier now that we have the emergency response car (with a physician on call)’. The presence of a physician on-scene shifted responsibility from the ACs to the physician, who had the authority to refer patients directly to mental health services. This transfer of responsibility alleviated the ACs’ decision-making burden and expedited the admission process, where necessary.
Consequences for on-scene practice and care trajectories
When patients don’t want the healthcare offered
Across groups, respondents emphasised that one of the main challenges ACs face when attending to patients with mental health issues is managing those who refuse the healthcare offered and/or decline to cooperate. As explained previously, leaving patients on-scene requires thorough examination, and not all patients agree to that. Respondents described several factors influencing these challenging interactions, including the acuity of the patient's condition, what was perceived to be in the patient's best interests, distance to the emergency clinic, and collaboration with relatives and other clinicians. Persuasion was frequently discussed as a strategy to secure a patient's consent for conveyance to a physician. Respondents’ accounts illuminated how ACs often navigate a spectrum between persuasion and the use of force or coercion, with some reflection on how this could threaten a patient's right to self-determination: ‘People can end up agreeing to do things they wouldn't have wanted to unless … if we hadn't used a significant degree of persuasion’ (resp. 3-2). Lack of knowledge about how to apply legislation to real-life situations complicates knowing what actions are permissible: ‘[…] I think the real problem is those who absolutely refuse. […] What are we actually allowed to do?’ (resp. 1-1).
As the quotes above illustrate, ACs struggle to balance role expectations with making ethically and legally sound decisions. This tension is particularly pronounced in cases where patients refuse care. A recurring theme across the groups was a lack of knowledge about how to apply legislation to real-life scenarios, leaving clinicians feeling the weight of the responsibility while being uncertain about what actions were permissible.
When patients’ decision-making capacity and best interest is in question
Discussions in several interviews pointed to that balancing the respect for patient autonomy with respect for the patient's best interest from a healthcare perspective was experienced as difficult. Several respondents across groups addressed the dilemma of patients who clearly needed help, but whose situation was not urgent enough to justify the use of force. One respondent explained: ‘You can see that maybe they actually need more help, but it's maybe not so urgent … not urgent enough to justify using force’ (resp. 1-3).
Across groups, several respondents expressed the belief that patients who do not understand what is best for themselves, lack decision-making capacity. Some argued that in these cases ACs not only had the right to intervene but a duty to do provide care. One respondent described this stance: […] reduced awareness, confusion, or dementia. I mean, patients who don’t understand what's best for them for one reason or another. In those cases, we not only have the right but also the duty to help them … and to take care of them (resp. 2-2). Resp. 6-4: […] you probably don’t know the patient, also [often a] less critical setting, where you have to evaluate more. You don’t know the patient, you don’t know their baseline. Family members or healthcare staff might say one thing, but you’re not really sure what's accurate or how much knowledge they have. So, then you have to make that judgment about what they’re capable of deciding for themselves and what they’re not, considering the situation as a whole. Resp. 8-4: And assessing their decision-making capacity, or how competent they are to consent, that's hard. Researcher: Yeah, does anyone find it easy to assess decision-making capacity? Resp. 11-4: No (several people laugh a little).
When there is fear of adverse outcomes
Across interviews, several respondents emphasised that the threshold for leaving a patient on-scene is high, particularly if the patient has mentioned thoughts or plans related to suicide. As the following quote illustrates, this reluctance is not always solely motivated by concern for the patient's well-being but also by a desire to protect themselves from the consequences of adverse outcomes: ‘[…] It's a judgment call in the moment, but the threshold for leaving someone at home after they’ve said something about planning to take their own life is pretty high for me. Honestly, it's about covering my own ass’ (resp. 3-3). The fear of adverse outcomes for the patient, as well as regulatory investigations that could negatively affect the ACs themselves, was a recurring theme across four group interviews. One respondent articulated this fear: ‘I think there's a general fear of lives being lost or of significant harm occurring, or even of regulatory investigations if we make mistakes or misjudgements’ (resp. 6-4). Discussions pointed to the fact that being the last clinician to interact with the patient weighed heavily on ACs, as this placed significant responsibility on their shoulders. This responsibility was described as particularly challenging when clinicians experienced difficulties obtaining timely support from physicians. When local guidelines required clinicians to obtain a physician's assessment, but the patient refused conveyance and support from a physician was difficult to secure, many described the situation as a ‘catch-22’: ‘…when they [the physicians] won’t come [do field visits], you’re just left standing there, but the responsibility for the patient is on you – you’re the last one who saw them. And if something happens, it's … it's uncomfortable’ (resp. 3-2).
There was general agreement across groups that consulting a physician by phone is standard protocol when considering leaving a patient on-scene. However, respondents expressed uncertainty about the extent of their responsibility following such consultations. Some respondents suggested that consulting a physician relieved them of responsibility, while others perceived these consultations as merely advisory, leaving them with the same level of accountability: Resp. 8-4: “We are the one that see the patients”. Resp. 6-4: “And we're supposed to make the final assessment, but … consulting with a doctor is just advisory”
Variations in guidelines between trust areas were reflected in differences across group discussions, along with differing perceptions of legal and ethical responsibilities. This highlighted how organisational factors, such as guidelines and training, can affect clinicians’ practises. Furthermore, several respondents expressed a lack of confidence in the support provided by their management. They voiced concerns that, in the event of adverse outcomes, the management would not advocate for or stand behind them: Resp. 3-5: […] I personally think that related to […] some of the decisions we make, we know that if something were to happen afterwards based on the decisions we make, no one in management would be there to back us up. Researcher: No (pause). You experience that? Resp. 3-5: No one. They’re just looking for a scapegoat to throw under the bus, and we end up standing there all alone. That's why, I think, we feel things are done a bit forcefully from our side, to cover our own backs. Because we know that when something happens, our employer isn’t going to support us.
Implication – solving the mission, not the problem
In their everyday work, ACs respond to both interfacility transfers – moving patients between locations – and emergency calls initiated through the emergency medical number or by healthcare professionals requesting on-scene assessment or treatment.
28
Across all groups, participants discussed their approaches to handling or resolving the calls, sometimes referred to as ‘missions’, particularly those involving patients experiencing a mental health crisis. Many ACs expressed that during these calls, they often felt unable to provide direct assistance. Instead, they viewed their primary role as conveying patients to physicians to assess and determine whether hospital admission was required. One respondent explained their approach as follows: Resp. 2-1: No, we’re not solving the problem [of the person being mentally ill], and we’re really not supposed to solve it either, because we don’t have that training, you know, or the authority for it. Basically, our job is just to pick someone up and drive them to the people who can actually do something about it, in one way or another.
Discussion
This study examined key challenges faced by ACs in managing patients in mental health crises in Norway. Some key challenges were found to include what ACs experienced: gaps in formal education and training, lack of guidelines and templates regarding mental healthcare assignments, guidelines’ influence on conveyance versus non-conveyance practices, lack of referral options, and lack of managerial support. The substantial responsibility of deciding to leave a patient on-scene, amplified by fears of adverse outcomes and potential regulatory scrutiny, made situations where patients declined and/or refused healthcare particularly challenging. Consequently, these factors collectively encouraged more frequent conveyance of patients to a physician, which may potentially have limited patients’ autonomy regarding remaining on-scene when appropriate. While autonomy is closely intertwined with informed consent, decision-making capacity, and best-interest judgments, owing to word limits, this article does not explore these constructs in depth and instead centres its analysis on autonomy and how organisational culture influences it.
Organisational culture's influence on ambulance clinicians’ practices
To better understand the underlying drivers of ACs’ practices, we will now discuss our results through the lens of Schein and Schein's (30) theory of organisational culture, within a critical realist perspective, which we argue can illuminate how organisational cultural mechanisms shape ACs’ reliance on conveyance of patients to specialised clinicians.
Schein and Schein 30 argue that shared assumptions, values, and norms can develop within groups as they adapt to internal and external challenges. These cultural elements become embedded in daily practices, shaping members’ perceptions, attitudes, and behaviours – often without conscious awareness. From a critical realist perspective, such embedded cultural elements can be understood as generative mechanisms that produce the observed practices. Participants reported feeling unprepared to manage mental health cases, relying instead on experience, intuition, and informal knowledge rather than formal training, findings consistent with previous research.10,14,41,42 ACs’ reliance on conveyance appears as an adaptive response to organisational gaps in training and support that, over time, has crystallised into a default norm. Thus, frequent conveyance can be seen as a group-level coping strategy compensating for limited confidence and knowledge in how to manage mental health calls. This raises critical questions about the contextual and organisational factors that continually reproduce these clinical practices.
Conveyance practises
In many countries, patients experiencing mental health crises are directed to the emergency department (ED), where they often face long waiting times and a stressful environment poorly suited to their needs.14,42 Respondents described how in Norway, ambulance services typically convey patients with mental health needs to their GP. When GPs are unavailable, the out-of-hours service becomes the default option. This pattern was primarily attributed to challenges in referring patients to other appropriate primary healthcare resources and points to insufficient collaboration and misaligned pathways between municipal primary healthcare services and ambulance services, as noted in previous research.42,43
While conveyance to the ED or out-of-hours primary care may satisfy ACs’ need to transfer responsibility to other clinicians, these services frequently do not address patients’ broader psychosocial needs, such as financial insecurity, housing instability, lack of social support and safeguarding concerns. These services’ primary mandate is to provide immediate emergency care to meet the population's urgent medical needs. 20 Consequently, conveyance may provide a resolution for the ACs but does not necessarily provide the most appropriate or therapeutic pathway for patients in mental health crises. Numerous studies emphasise the need for improved interagency referral processes and the development of alternative, tailored care pathways for individuals experiencing mental health illness.14,20,42–45 Although person-centred alternatives to emergency department care have been shown to offer safe and valuable support, 46 their availability varies widely. Such variation is produced by local municipal provision and inter-organisational arrangements; where alternatives do exist, their referral pathways must be accessible and operational for ambulance services. 47
The role of organisational culture in shaping non-conveyance practices
A systematic review by Ebben et al. 19 reported wide variations in non-conveyance rates across studies from multiple countries, ranging from 3.7% to 93.7%. They show how the factors influencing decisions of non-conveyance are multifaceted and associated with the clinician, the patient and their relatives, the healthcare system or processes, as well as the availability of supportive tools.46,48–61 Professional factors include competencies, where additional training increased non-conveyance rates,52,62 risk assessment, fear of litigation,59,60 experience and intuition, 61 and pragmatism (conveyance being an easy option compared to non-conveyance). 61 Patient factors include health status,46,53,55,58,60,63,64 specific conditions such as resolved or minor injuries,46,53,58 and refusals..46,58 Patient wishes and best interests also play a role. 57 Organisational factors include access to GPs or alternative care46,59 and availability of patient information, with a lack thereof leading to less appropriate care. 54 Supportive tools such as online medical control or high-risk cards increased conveyance in high-risk or refusing patients.49–51
Our findings align with this complex picture. Respondents emphasised the significant responsibility of being the last healthcare professionals to interact with patients left on-scene, echoing the study of Rees et al. 65 In some cases, decisions to convey were motivated both by concern for patient welfare and by a desire to safeguard themselves against the potential consequences of adverse outcomes. This defensive practice was intensified where managerial support was perceived as weak, consistent with Knowles et al.'s study. 24 Similarly, the present findings show that lack of support may reinforce risk-averse practices and that managerial attitudes vary between promoting person-centred non-conveyance and preferring a more risk-averse approach.
Our results and theoretical orientation in interpreting the results can shed light on these processes and suggest potential causal connections. We have shown how artefacts, espoused values and basic underlying assumptions might shape how leadership priorities, measurement systems, incident response and shared narratives become embedded as relatively enduring mechanisms. On this basis, these cultural elements function as generative mechanisms (e.g. historical emphasis on conveyance, managerial risk aversion, weak interagency pathways, limited training) that produce and reproduce the observed non-conveyance patterns. 31
Balancing autonomy, risk, and organisational pressures in non-conveyance practices
Drawing explicitly on Schein and Schein's organisational culture model 30 and a critical realist stance,30,31 we have considered how organisational culture, through its mechanisms and underlying assumptions, shapes the balancing of autonomy, risk, and organisational culture in non-conveyance practices. We have shown that organisational culture likely affects clinical practises and thereby non-conveyance decisions. Here, we explicate how those cultural elements may influence the extent to which ambulance clinicians enable patients’ self-determination, potentially constraining autonomy when conveyance is treated as the safer option.
As mentioned above, autonomy in our context refers to a person's ability, right and opportunity to make informed decisions about their care and life, which presupposes decision-making capacity.66,67 Assessment of a patient's capacity typically accompanies a clinical evaluation. 68 In our data, respondents did not refer to the four core abilities of capacity: understand, reason, appreciate relevant information, and communicate a choice.66,67 Instead, assessments of capacity appeared to rely on whether patients were perceived to have sufficient insight into what was considered to be in their best interests, with references to confusion, reduced awareness, or dementia serving as indicators of incapacity. Furthermore, respondents reported difficulties with making judgments regarding decision-making capacity, consistent with other studies that documented limited tools, templates and training to support these complex assessments.25,69–72 When clinicians encounter patients in high-risk situations who refuse the help offered by ACs (e.g. self-harm or suicidal behaviour), legal frameworks allow interventions when imminent danger exists, and in Norway, clinicians must act in the patient's best interest when there is imminent risk of harm. 73 Applying Schein's levels (artefacts, espoused values and basic underlying assumptions) and retroduction from our empirical observations, we interpret practices such as persuasion, lies, tricks and coercion to ensure conveyance7,65 as, at least in part, stemming from interacting cultural and organisational mechanisms. Their experience of leadership priorities, weak managerial support, scarce training and limited referral pathways shape how clinicians interpret risk and what counts as acceptable actions in response. Barghout et al. (2025) ‘Elements of Guidance for Emergency Medical Services Clinicians’ shows that managing patients’ refusal of conveyance involves many practical steps beyond capacity assessment. It involves risk evaluation, persuasive communication, escalation to medical oversight, and meticulous documentation, underscoring that autonomy in the field is negotiated through multiple, context-dependent practises. The medicolegal landscape also matters. The risk of liability is generally low for using reasonable force to convey a patient out of genuine concern, but substantially higher if a patient left on-scene later experiences an adverse outcome. 74
Taken together, these findings indicate that organisational culture plays a significant role in shaping clinicians’ everyday practices around refusal and conveyance, with important ethical implications. Without managerial attention to the cultural and structural supports for autonomy, patients’ self-determination may be unduly compromised even when legal criteria for intervention are not met.
Implications
Our findings indicate that organisational generative mechanisms that produce current conveyance practices must be addressed to improve how services respond in mental health crises, not only at the level of individual clinicians. Using Schein and Schein's three levels, interventions should address artefacts (training, tools, referral pathways), espoused values (management priorities and performance metrics), and the underlying basic assumptions that drive the practice of conveyance as a default measure, for example, the fear of not getting managerial support in case of an adverse outcome after non-conveyance. Strengthening education and training in mental healthcare and in assessing decision-making capacity may help clinicians manage complex situations more confidently and reduce reliance on default conveyance. While several studies highlight a lack of knowledge and confidence among ACs,10,14,41,42 there is limited research on what specific competencies should be prioritised or how such training should be delivered. 75 Addressing this gap is important to ensure that educational efforts are both evidence-based and adapted to the prehospital context.
We suggest that explicitly integrating ambulance services in mental-health policy could strengthen collaboration between ambulance services, primary healthcare, and community-based resources and ensure coordinated access to established alternative referral pathways where those exist – an approach with high feasibility and low cost that leverages existing structures. For example, this could include establishing direct consultation and referral pathways with local resources such as assertive community treatment teams and municipal psychosocial support services, accessible to ambulance clinicians for patients already under the care of such services and, in future, those not currently engaged with them.
Management within ambulance services plays a crucial role in shaping practice and is accountable for securing this collaboration and embedding existing alternative referral pathways through clear policies, training, and interagency agreements. By fostering a supportive, person-centred culture and clarifying professional and legal responsibilities, management can help reduce defensive practices and promote care that respects and supports patient autonomy.
Strengths and limitations
This study has several strengths, including the inclusion of participants from three of the four Regional Health Trusts in Norway, representing both urban and rural areas. Participants were drawn from 8 of the 18 ambulance services, providing insights into organisational practices across a range of contexts. The qualitative design enabled an in-depth exploration of key challenges faced by ACs in managing people in mental health crisis within the current healthcare system. We consider it a strength that the first author holds clinical experience from the ambulance service, which added valuable context from an insider perspective. The outsider and user perspectives from the co-authors and advisory board members have challenged preconceived perceptions and sparked deeper reflection, aligning with the RTA methodology. However, the study also has limitations. A strategic sample means some regional and organisational variability, and the underlying contextual and cultural mechanisms influencing practice may not have been fully captured, especially given the potential for cultural differences both between and within individual ambulance stations. Additionally, while the interviews focused on mental health cases, participants did not always clearly distinguish these from general patient cases. This may reflect how mental health presentations are embedded in everyday ambulance practice, but it may also have affected the specificity of the findings. The findings presented here are those showing the most salient patterns inferred from the data, acknowledging that they are partial representations rather than exhaustive accounts. We opted not to elaborate on legal capacity and best-interest judgements to remain focused on organisational culture's influence on ACs’ conveyance practices and, by extension, patients’ autonomy, because this will be elaborated in a later publication.
Conclusion
This study offers an account of key challenges faced by ACs in managing mental health crises. Insufficient organisational support when patients refuse assessment or conveyance, combined with the substantial responsibility placed on individual clinicians and fears of adverse outcomes and regulatory scrutiny, appears to trigger mechanisms that shift practise away from person-centred care toward defensive, self-protective decision making. Organisational culture and leadership further shape attitudes and practices, including decisions about non-conveyance and the extent to which patients are enabled to exercise their right to self-determination. Addressing these challenges requires a system-wide approach targeting both structural conditions and cultural influences, including enhanced mental health training, stronger and accessible referral pathways, clear inter-agency agreements and a supportive organisational culture that empowers clinicians to provide autonomy-respecting, person-oriented care.
Supplemental Material
sj-docx-1-pam-10.1177_27536386261457283 - Supplemental material for Non-conveyance and autonomy: How organisational contexts influence ambulance clinicians’ practice in mental health crises – A qualitative study
Supplemental material, sj-docx-1-pam-10.1177_27536386261457283 for Non-conveyance and autonomy: How organisational contexts influence ambulance clinicians’ practice in mental health crises – A qualitative study by Nina Øye Thorvaldsen, Anne Kristine Bergem, Jorun Rugkåsa and Kristin Häikiö in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386261457283 - Supplemental material for Non-conveyance and autonomy: How organisational contexts influence ambulance clinicians’ practice in mental health crises – A qualitative study
Supplemental material, sj-docx-2-pam-10.1177_27536386261457283 for Non-conveyance and autonomy: How organisational contexts influence ambulance clinicians’ practice in mental health crises – A qualitative study by Nina Øye Thorvaldsen, Anne Kristine Bergem, Jorun Rugkåsa and Kristin Häikiö in Paramedicine
Footnotes
Acknowledgments
We are deeply grateful to all members of the Advisory Board: Eva-Brit Langva, Solveig Kjus, Ole Petter Gjerdrum, Fredrik Sundby, Øyvind Holst, Jacob Jorem, Magnus Hjortdahl, Trine Møgster Jørgensen, Lin Ulvøy and Hege Helene Bakke for their guidance and for their insightful input and fruitful discussions. We are equally grateful to everyone who assisted with the recruitment and organisation of the interviews for their dedicated assistance, and to all participants for their time, openness, and invaluable insights, which greatly enriched this study.
Ethical approval and informed consent statements
The Regional Committees for Medical and Health Research Ethics (reference 516477/REK South-East) deemed that the study was outside the scope of the Health Research Act. The Norwegian Centre for Research Data (reference 903381), the Data Protection Officer at each local health trust, and the management of each ambulance service granted their approval of the study. Additionally, all respondents provided signed informed consent declarations.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by OsloMet - Oslo Metropolitan University, Faculty of Health Science, which provided financial support for the doctoral fellowship under which this research was conducted. The funder had no role in data collection, interpretation, or reporting.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The interview/focus-group data underlying this study cannot be made publicly available because participants could be indirectly identifiable. Sharing such data would violate the permissions granted by the Norwegian Centre for Research Data (NSD) and the ethical guidelines for research. However, de-identified extracts sufficient to support the findings are included in the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.