
Abstract
Introduction
In Canada, paramedics and hospital emergency department (ED) nurses utilize the Canadian Triage and Acuity Scale (CTAS) to assign acuity. This study examined concordance of assessment between paramedics and emergency department triage nurses. We also assessed operational factors to provide confidence that paramedic triage scores were not being influenced by non-patient-related factors such as workload, delays in handover or destination type.
Methods
We conducted a retrospective cohort study of all paramedic-transported patients to hospitals from 1 January 2018 to 31 December 2022. All records of patients transported by paramedics to in-region EDs or urgent care centres (UCCs) where CTAS was recorded at two different points by paramedics (at time of transport) and triage nurses (at time of ED triage) were reviewed. We analyzed concordance using crude percentages, inter-rater agreement using a weighted kappa (kW) analysis, and computed an adjusted multilevel binomial regression model to determine independent associations between agreement and operational and clinical factors using odds ratios (OR) with 95% confidence intervals (CIs).
Results
Inter-rater reliability analysis showed ‘substantial’ agreement for the most critical patients (CTAS 1: 78.8%, κW = 0.66) and ‘fair’ agreement for the least urgent patients (CTAS 4: 32.8%, κW = 0.30; CTAS 5: 25.9%, κW = 0.34). Discordance increased with patient complexity (i.e. higher numbers of medical conditions [OR 0.98, 95% CI 0.97–0.98], patients aged ≥18, primary problems of mental health or soft tissue injury/pain presentations). Concordance increased with patient age and paramedic certification level. No operational factors examined demonstrated an independent association with CTAS agreement.
Conclusions
Patient acuity agreement declined with lower acuity scores. Operational influences were not detected as significant predictors of CTAS disagreement. Several clinical factors were found to potentially affect agreement, particularly with increasing patient complexity. The implications for paramedic practice, paramedic education and EMS response priority planning warrant further investigation.
Introduction
The accurate assessment and recognition of patient acuity by health-care professionals in the emergency setting is crucial for delivering care in accordance with medical necessity and has important implications for patient safety and resource allocation. Various classification instruments such as the Australasian Triage Scale, the Manchester Triage Scale and the Emergency Severity Index have been employed in emergency departments (EDs) and in the prehospital environment to triage patients based on objective factors such as patient concern, history and vital signs. 1 Among these ordinal instruments is the five-level Canadian Triage and Acuity Scale (CTAS), which is based on the Australasian Triage Scale and has demonstrated predictive ability similar to that of the Emergency Severity Index.2–4 CTAS is utilized in all EDs and paramedic services in Ontario, Canada, providing a comparative opportunity for analysis. Previous research demonstrates evidence of CTAS inter- and intra- rater reliability among ED triage nurses and physicians,5,6 and moderate inter-rater reliability between paramedics and ED triage nurses 7 when using CTAS in the prehospital setting.
Accurate paramedic CTAS scores not only serve as a universally understood indicator of acuity for receiving hospital staff but also as a guide for paramedic clinical decisions. Such decisions include determination of the appropriate medical directives to implement, the receiving medical facility, and whether lights and sirens [which can pose risks if utilized unnecessarily 8 ] should be utilized during transport. Additionally, assessments of paramedic-assigned acuity are gaining increasing importance in more advanced methods of emergency medical services (EMS) system response planning. 9 While the complex interplay of clinical, interpersonal and operational factors in the application of CTAS by ED nurses has been studied and shown to influence its application, 1 there is a gap in understanding the impact of clinical and non-clinical factors on paramedics who employ CTAS as a standardized acuity measure in the prehospital setting.
Our primary objective was to determine and examine agreement of patient triage scores between paramedics in the prehospital setting and hospital nurses upon triage. Our secondary objective was to examine clinical and non-clinical factors associated with triage agreement between paramedics and hospital nurses, to understand whether contextual operational factors might influence paramedics’ application of CTAS as has been evidenced with nurses in ED settings.
Methods
Study design
We conducted a retrospective cohort study of routinely collected administrative data at Niagara Emergency Medical Services (Niagara EMS), one of Ontario's largest EMS providers. We reported results according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline. 10
Population and setting
All cases transported to a Niagara Region hospital ED or urgent care centre (UCC) by Niagara EMS paramedics between 1 January 2018 and 31 December 2022 were eligible for inclusion. Niagara Region is an ‘upper tier municipality’ in Ontario, Canada with an urban and rural population of 477,901 residents, of which 51.3% are female, and 23.3% are greater than 65 years of age. 11 Niagara EMS (NEMS) is a municipal paramedic service providing 24/7 response as the sole EMS provider. At the time of this study, NEMS deploys up to 35 transport-capable ambulances at peak staffing, staffed with primary care (PCP, 60%) and advanced care (ACP, 40%) paramedics, with an annual call volume of approximately 70,000 responses/year. This is supplemented with a number of non-transporting ‘mobile integrated health’ units staffed by ACP or PCP and, in some cases, other health-care professionals such as nurses or occupational therapists.
NEMS paramedics transport patients to hospital systems within the Niagara 99.2% of the time, with a small percentage (0.8%) being transported out of region based on proximity or field trauma triage guidelines. At the time of this study, patients in Niagara could be transported to UCC rather than ED if the patient was a CTAS 3 or lower, and the UCC was closer than the ED.
Niagara Region was chosen for this study due to the availability of both paramedic and triage nurse CTAS scores within a single database. Cases were excluded if paramedic transport was not a result of a 9-1-1 call, was a transfer between health-care facilities, no patient was transported (i.e. refused transport, resuscitation terminated on scene), the patient was transported to a hospital outside of Niagara Region, or where CTAS scores were missing. The study timeframe represents the most recent five-year period for which full-year data were available at the time of study initiation.
Data source
Data for this study were extracted from the NEMS internal data repository, a patient incidence database that securely collects and stores all electronic patient care reports (ePCRs). The ePCR is a health-care record completed by paramedics in the prehospital setting following each patient interaction using iMedic™ software.
Variables and measurement
All patient and clinical characteristics included in this study were measured and recorded at two different points: the time of paramedic transport and upon assessment by the receiving hospital triage nurse. CTAS missing values represented approximately 2.8% of hospital cases, and zero missing EMS cases, as CTAS was required to complete the ePCR used by paramedics. Missing CTAS did not demonstrate clustering in descriptive review; however, formal analysis was not performed. We selected characteristics based on prior literature, clinical judgement and data availability. Characteristics include age, sex, paramedic triage acuity (CTAS assigned by the paramedics at time of transport), nurse triage acuity (CTAS assigned by triage nurse), 9-1-1 call priority, date, pick-up municipality, paramedic care level (primary or advanced care), presenting concern, final problem, hospital destination (ED or UCC), number of ambulances awaiting offload in ED at the time of transport and duration of offload delay (offload time exceeding 30 min) in minutes within the hour of transport.
Age was categorized into groups (0–17, 18–39, 40–64, ≥65 years) to reflect clinically and operationally meaningful distinctions in emergency care populations. Individuals aged 0–17 years are managed within distinct paediatric modifiers within CTAS. 12 Adults aged 18–39 years were considered a younger adult group, generally characterized by lower comorbidity burden and different patterns of acute illness and injury. The threshold at 40 years was selected to reflect a transition to midlife, during which the prevalence and clustering of cardiovascular and metabolic risk factors become clinically meaningful. Population-based studies demonstrate that by age 40, a substantial proportion of individuals exhibit one or more cardiovascular risk factors, and risk prediction frameworks commonly initiate assessment at this age.13,14 These changes are associated with evolving patterns of disease presentation that may influence acuity assessment in emergency care settings. Patients aged ≥65 years were categorized as older adults, consistent with widely used definitions in emergency medicine and prehospital research. Older adults are known to have increased frailty, multimorbidity and atypical presentations, all of which may affect triage accuracy and inter-rater agreement.15,16 These categories were selected a priori to balance clinical interpretability with sufficient sample size within each group.
Since there were 61 distinct primary problem codes, we reported the nine most frequent categories individually and grouped all remaining codes into an ‘other’ category for interpretability and to avoid sparse cell counts. Additionally, we included patient comorbidities, pickup location type, trauma codes (trauma type/location), recorded interventions, ambulance shift duration/proximity to end of shift and ‘special transport codes’ (indicating the need for specialized care centre transport, such as a trauma centre or stroke centre). The operational variables (number of ambulances waiting in ED, duration of offload time, end of shift) were included as proxy measures for perceived ‘busyness’, in keeping with findings of Reay et al. 1 regarding operational influences on nurse CTAS in the ED setting. This information is available to NEMS paramedics through smartphone or mobile data terminal (MDT) applications. ‘Departure scene time proximity to paramedic end of shift’ was included because time pressure and sustained cognitive workload during long shifts have been linked to decision fatigue in clinical settings, particularly nursing.17,18 Decision fatigue can lead to diminished cognitive resources and changes in decision patterns as shifts progress, providing a theoretical basis for examining temporal proximity to shift end as a contextual factor in prehospital triage scoring decisions.
The outcome measured was agreement between CTAS applied at two points: paramedic acuity score (the recorded CTAS on scene departure) and hospital nurse acuity score (CTAS assigned on hospital arrival). Median scene-to-hospital transport time for the period of the study was 632 s (10.5 min), with a 90th percentile of 1349 s (22.5 min). Agreement was represented as a dichotomous variable, categorized as either ‘agreement’ (same scores) or ‘disagreement’ (differing scores). Paramedics document CTAS at three intervals: upon arrival at patient before intervention, upon departure from scene and upon arrival at hospital. The depart-scene CTAS score was selected for this study as this score is unalterable by paramedics in the paramedic ePCR. This is communicated to the ambulance dispatch centre via MDT immediately upon departing the scene and automatically uploaded into the ePCR. This logic permitted guaranteed observation independence and mitigated the potential influence of nurse triage assessment. Nurses in the hospital facilities of this study used electronic software to compute the CTAS score following input into the triage record, a valid tool used in hospitals for triage.19,20 Paramedics do not have access to any software tools in the prehospital setting to assign acuity and must rely on CTAS training, clinical training and experience.
Statistical analysis
Descriptive statistics are reported using measures of central tendency (frequencies, proportions). We reported differences in patient characteristics using chi-squared tests with statistical significance with a p-value of ≤0.05. Missing data were reported directly and handled using complete case analysis, a pragmatic statistical approach when datasets are large, and the percentage of missing data is low.
Descriptive statistics were also used to summarize annual mean CTAS scores assigned by paramedics and ED nurses across the five-year study period (Figure 1). These analyses were exploratory and intended to provide context only. Formal longitudinal modelling of temporal trends and interaction effects between year and professional group was not performed. Future studies using individual-level longitudinal data could further evaluate temporal changes in CTAS assignment using mixed-effects regression approaches.
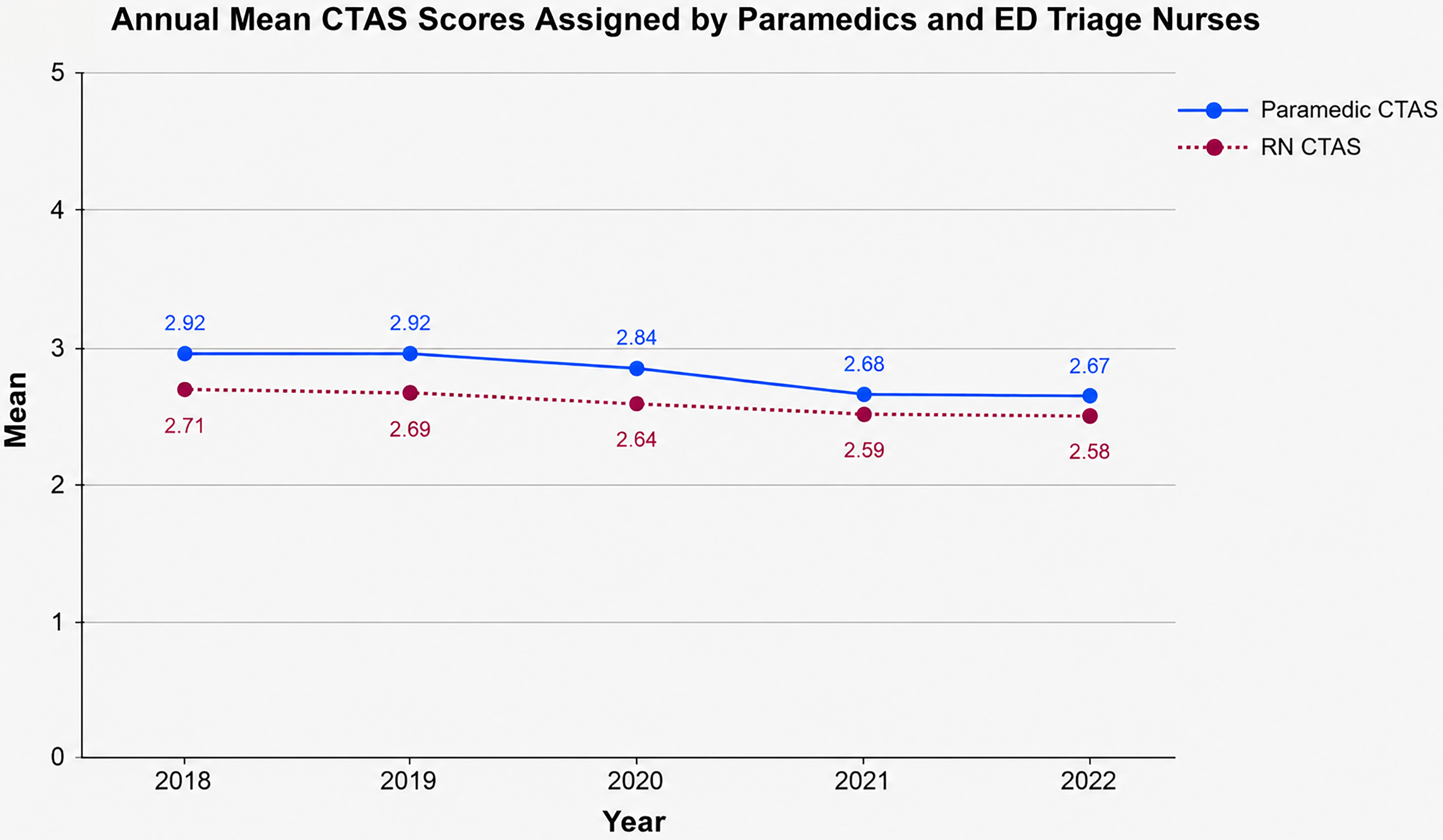
Year-over-year changes to paramedic and nurse CTAS mean. Values are presented descriptively; no formal statistical testing of temporal trends was performed.
The primary objective was to examine the inter-rater agreement between paramedics in the prehospital setting and triage nurses in the hospital setting. Agreement was measured overall, at each individual CTAS level (1–5), and as blocks of emergent (CTAS 1, 2), urgent and less-emergent (CTAS 4, 5) acuities using a weighted Kohen's kappa (κW) statistic with 95% confidence intervals (CIs). Because CTAS level 0 (witnessed cardiac arrest) is an EMS-only level, cases assigned CTAS 0 by paramedics (n-22) were excluded from agreement analysis to ensure comparable ordinal categories (CTAS 1–5) across raters. Weighted kappa was selected to account for the ordinal nature of CTAS categories, recognizing that disagreement between adjacent acuity levels (e.g. CTAS 2 vs CTAS 3) is less clinically substantial than disagreement across more distant acuity levels (e.g. CTAS 1 vs CTAS 5). Agreement was calculated overall, for each CTAS acuity level, and for grouped categories (CTAS 1–2 and CTAS 4–5). Ninety-five percent confidence intervals (CIs) were calculated using standard large-sample approximation methods. Agreement was analyzed annually to understand trends amongst the study years. The kW was categorized based on previously published literature of: ≤0 = poor, 0.01–0.20 = slight, 0.21–0.40 = fair, 0.41–0.60 = moderate, 0.61–0.80 = substantial and 0.81–1 = almost perfect. 21
For the secondary objective, a multivariable binary logistic regression model was constructed with agreement (yes/no) as the dependent variable. Predictor variables were selected a priori based on data availability, theoretical plausibility and prior literature examining contextual and operational influences on triage decision-making. The following covariates were entered simultaneously (forced-entry method): number of documented patient medical conditions, number of paramedic interventions administered, number of ambulances at the receiving healthcare centre at time of decision, offload delay duration (in minutes), healthcare destination type (ED vs UCC), and time interval between paramedic triage assignment and end of shift.
Demographic variables (e.g. age, sex) were examined in descriptive analysis but were not included in the multivariable model, as the objective was not to construct a fully adjusted predictive model but to evaluate the independent contribution of clinically and operationally relevant factors related to the decision-making environment at the time of triage. While demographic factors may influence patient presentation, they were not expected to substantially confound the relationships between these variables and agreement. This approach prioritizes interpretability of clinically meaningful factors over development of a fully adjusted predictive model. However, the potential for residual confounding is acknowledged.
We reported results as adjusted odds ratios (ORs) to show independent associations of each characteristic, with 95% CIs. The Omnibus test of coefficients was utilized to test the model's overall performance with corresponding 95% CIs. We managed and analyzed all data using IBM SPSS Statistics (version 29).
Ethics approval
This study received ethics approval from the Hamilton Integrated Research and Ethics Board (HiREB), review number 16921. Local study approval was also received by the Niagara Region Public Health Research and Ethics Review Committee (RERC), review number 2023–05.
Results
Over the five-year study period, 188,222 records of patient transport were included as they had both the paramedic and nurse CTAS scores recorded (Table 1). There were 5388 records excluded due to a missing CTAS score. Overall, the majority of patients were female (55%) and over the age of 65 years (56%), aligning with the typical paramedic case mix in this region (Table 2). From 2018 to 2022, agreement increased steadily. Disagreement was highest in the age demographic of 0 to 17 years, and the highest agreement in the age demographic 65 years or older (p < 0.01). Documented ‘primary problem’ codes for behaviour/psychiatric, soft tissue injuries and trauma/pain/oedema demonstrate a trend towards disagreement (p < 0.01). Conversely, ‘dyspnoea’ was associated with greater agreement (p < 0.01). Agreement has an inversely proportional relationship to CTAS level, with the highest acuity (CTAS 1) showing the highest agreement and the lowest acuity (CTAS 5) the lowest (p < 0.01). Higher levels of paramedic care certification were positively correlated with agreement (p < 0.01).
Case selection process.
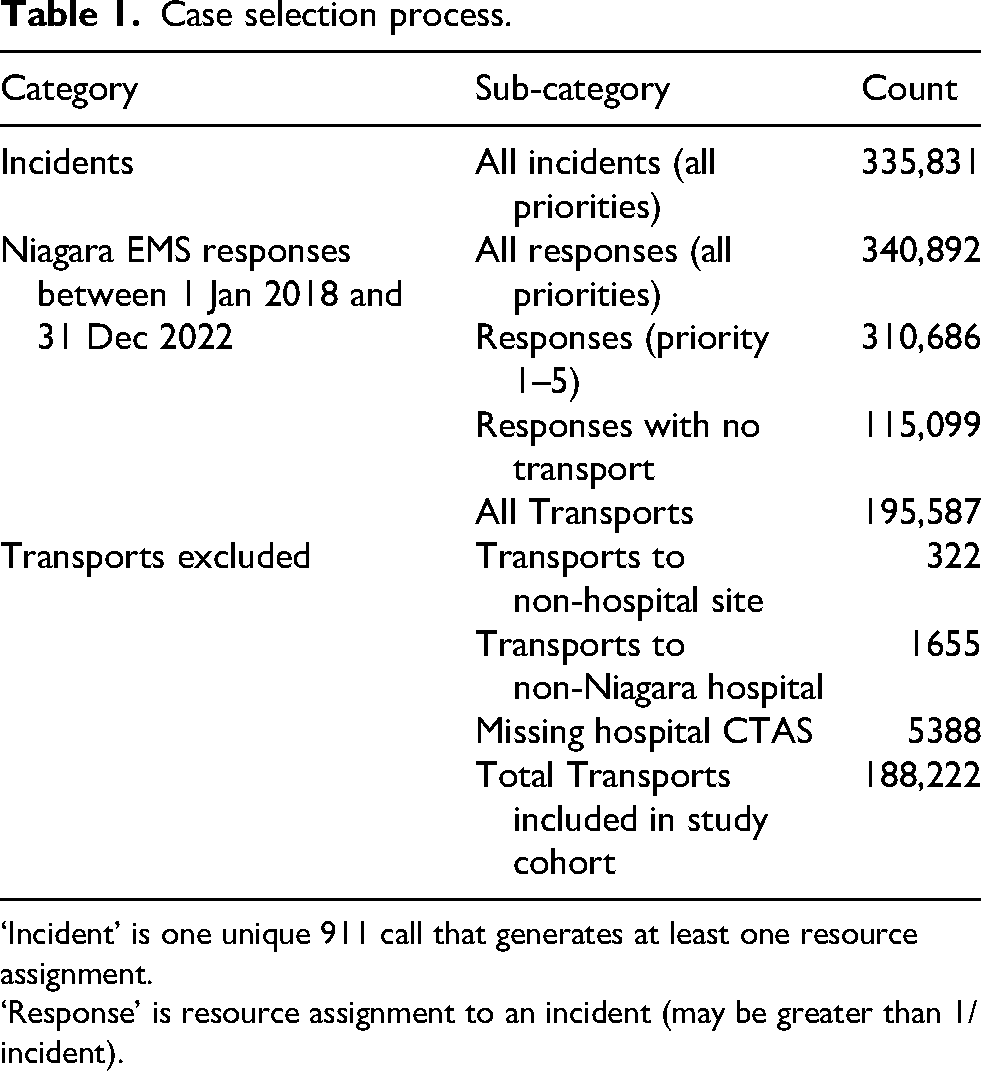
‘Incident’ is one unique 911 call that generates at least one resource assignment.
‘Response’ is resource assignment to an incident (may be greater than 1/incident).
Descriptive statistics.
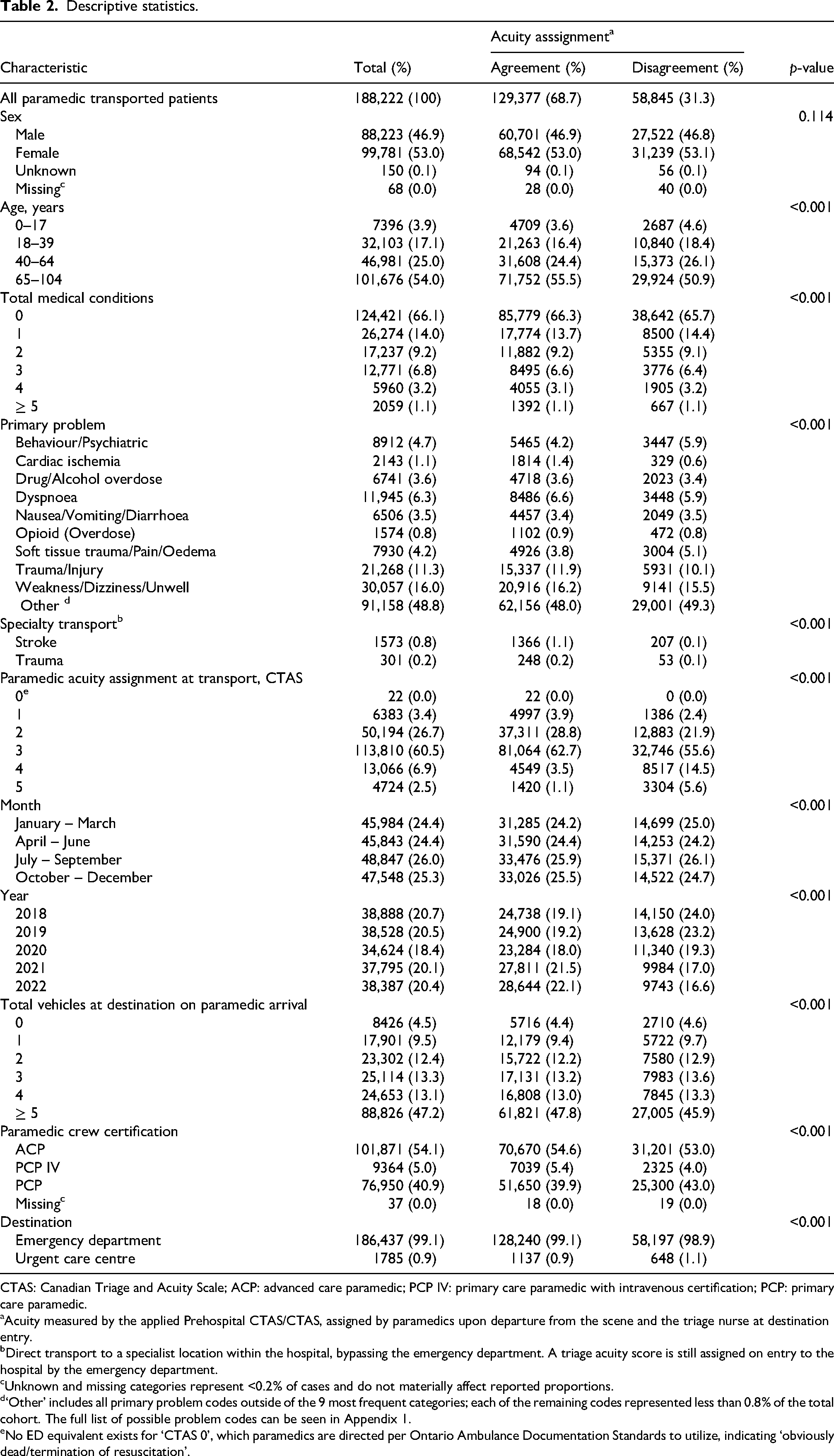
CTAS: Canadian Triage and Acuity Scale; ACP: advanced care paramedic; PCP IV: primary care paramedic with intravenous certification; PCP: primary care paramedic.
aAcuity measured by the applied Prehospital CTAS/CTAS, assigned by paramedics upon departure from the scene and the triage nurse at destination entry.
bDirect transport to a specialist location within the hospital, bypassing the emergency department. A triage acuity score is still assigned on entry to the hospital by the emergency department.
cUnknown and missing categories represent <0.2% of cases and do not materially affect reported proportions.
d‘Other’ includes all primary problem codes outside of the 9 most frequent categories; each of the remaining codes represented less than 0.8% of the total cohort. The full list of possible problem codes can be seen in Appendix 1.
eNo ED equivalent exists for ‘CTAS 0’, which paramedics are directed per Ontario Ambulance Documentation Standards to utilize, indicating ‘obviously dead/termination of resuscitation’.
Analyses of agreement are shown in Table 3, and the interplay of CTAS scores is illustrated in Figures 1 and 2. Overall, paramedics and nurses agreed on 68.7% of all transported patients, demonstrating an overall moderate agreement (κW = 0.53, 95% CI 0.53–0.53; p < 0.01). There was a negative gradient between CTAS level and interrater agreement, ranging from ‘substantial’ agreement [κW = 0.66 (p < 0.01, 95% CI 0.65–0.67)] on CTAS 1 patients to ‘moderate’ for CTAS 2 [κW = 0.50 (p < 0.01, 95% CI 0.50–0.51)] and CTAS 3 [κW = 0.48 (p < 0.01, 95% CI 0.44–0.45)], down to ‘fair’ for CTAS 4 [κW = 0.30 (p < 0.01, 95% CI 0.29–0.31)] and CTAS 5 [κW = 0.34 (p < 0.01, 95% CI 0.33–0.35)] patients. Combined emergency acuities (CTAS 1 and 2) showed ‘moderate’ agreement [κW = 0.57 (p < 0.01, 95% CI 0.56–0.57)], while combined nonemergent acuities (CTAS 4 and 5) showed only ‘fair’ agreement [κW = 0.40 (p < 0.01, 95% CI 0.40–0.41)]. Over the five-year course of the study period, the mean CTAS for both paramedics and nurses are presented descriptively in Figure 1, while overall agreement between paramedic and hospital CTAS scores is illustrated in Figure 2. Most cases demonstrated concordance, with the largest flows observed along the diagonal of the Sankey diagram. In this diagram, thicker flows represent larger patient volumes, whereas thinner flows represent smaller volumes. Among cases in which paramedic and hospital CTAS scores differed, ED triage nurses more frequently assigned higher acuity (i.e. lower CTAS scores) than paramedics. Specifically, higher acuity was assigned at hospital triage in approximately 75% of discordant cases (36,129 of 48,219; 95% CI 74.5%–75.3%), compared with 25% in which lower acuity was assigned. This asymmetry was statistically significant (binomial test, p < 0.001).
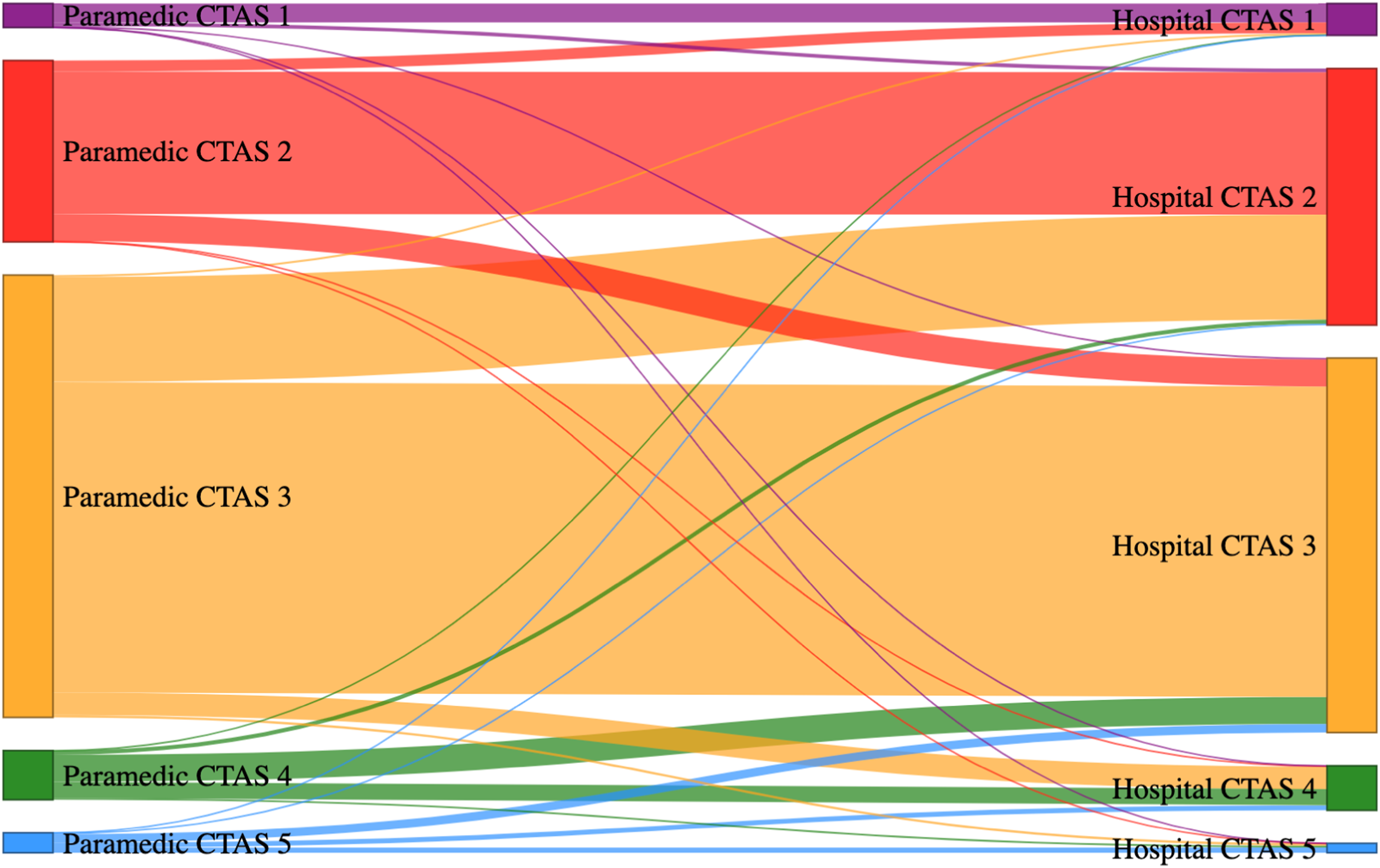
Sankey plot of triage acuity scores between paramedics and hospital nurses. Flows represent the number of patients transitioning from paramedic-assigned CTAS at departure scene (left) to ED nurse-assigned CTAS at ED triage (right). The width of each flow is proportional to the number of patients represented. Agreement is recognized by flows that remain in the same horizontal category, whereas branching flows indicate disagreement between assessments. Lower CTAS scores indicate higher acuity. Flows moving toward lower CTAS categories reflect higher acuity assignment by emergency department nurses. Colours are used to distinguish CTAS categories only.
Weighted kappa for paramedic and nurse CTAS agreement by CTAS level (calculated excluding CTAS 0 (n = 22).
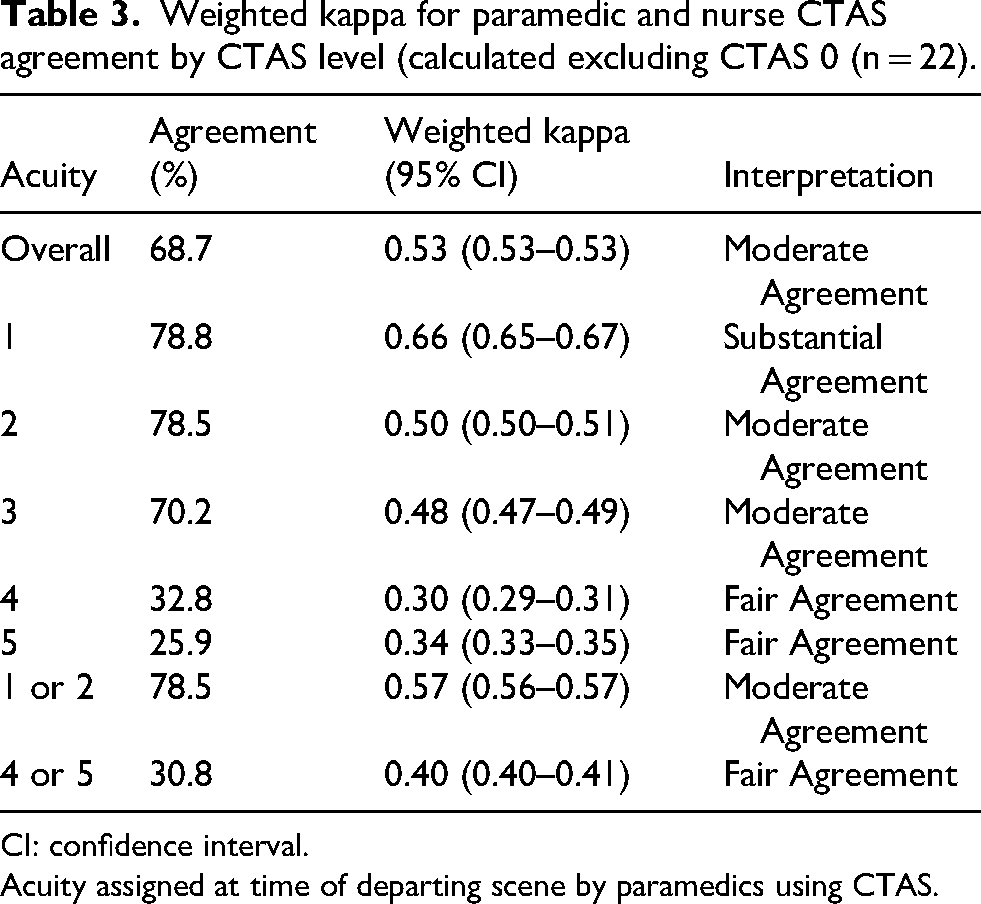
CI: confidence interval.
Acuity assigned at time of departing scene by paramedics using CTAS.
The results of the multivariable binary logistic regression are shown in Table 4. The number of documented patient medical conditions showed a statistically significant negative association on agreement (OR 0.98, 95% CI 0.97–0.98). An increase in the number of paramedic interventions performed had a positive influence on agreement (OR 1.03, 95% CI 1.03–1.04). Although offload delay reached statistical significance, the magnitude of the effect per minute was extremely small and unlikely to be clinically meaningful. No other characteristics showed statistically significant influence on agreement in the model.
Multivariable logistic regression analysis of clinical and operational factors associated with agreement in CTAS assignment between paramedics and emergency department nurses.
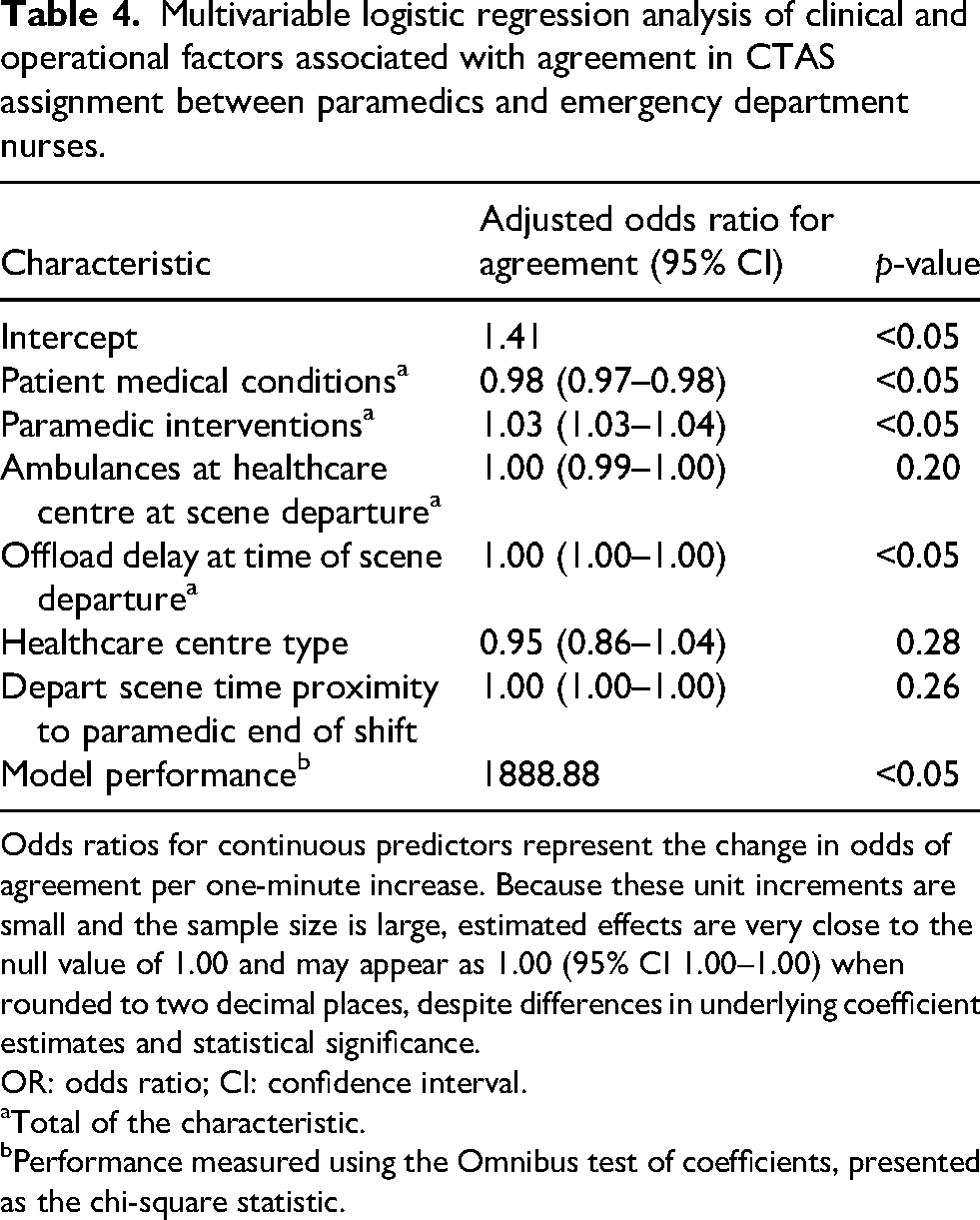
Odds ratios for continuous predictors represent the change in odds of agreement per one-minute increase. Because these unit increments are small and the sample size is large, estimated effects are very close to the null value of 1.00 and may appear as 1.00 (95% CI 1.00–1.00) when rounded to two decimal places, despite differences in underlying coefficient estimates and statistical significance.
OR: odds ratio; CI: confidence interval.
Total of the characteristic.
Performance measured using the Omnibus test of coefficients, presented as the chi-square statistic.
Discussion
Substantial agreement was detected between paramedics and nurses in their CTAS scores. Paramedics tended to assign a lower acuity level than nurses, a finding consistent with previous research where nurse and paramedic measures of acuity were compared.22–24 Notably, there was a tendency for paramedics and nurses to disagree more as acuity decreased, with paramedics assigning lower acuity scores overall. This finding contrasts with the research of Leeis et al., 7 who found paramedics tended to assign higher acuity scores compared to nurses in CTAS levels 4 and 5. In this dataset, measured proxy operational pressures were not significantly associated with triage agreement. These results diverge with findings from a study of nurses performing triage in an ED, which showed that operational and contextual factors (i.e. ED ‘busyness’, resource levels) did influence triage decision-making and CTAS assignment. 1
Disagreement increased when the number of patient medical conditions increased, suggesting that paramedic triage may be less reliable with more complex patients. This finding, combined with the results of previous research showing a higher number of hospital admissions for paramedic-assigned CTAS 4 and 5 patients than among nurses,7,25 indicates potential opportunities for enhanced training and oversight on application of CTAS and, if warranted, clinical assessment. Additionally, this result suggests the examination of possible potential benefit to the employment of an electronic CTAS decision-making tool (eCTAS) for paramedics, similar to those used in Canadian EDs.
In our research, we observed lower agreement with nonemergent acuity levels, paediatric patients, patients that have behaviour/psychiatric presentations, patients that have multiple co-morbidities, and where paramedics have a lower level of certification (i.e. scope of practice). This finding may be important for stakeholders of paramedic systems that organize and plan paramedic models of care and medical oversight. Particularly, systems reliant on forecasted paramedic-triaged acuity alone to determine acuity response and resource assignment to 911 calls may need further analysis. These findings suggest that when determining lower priority response levels, which may be deferred in favour of higher priority calls, acuity information may benefit from triangulation with other patient details to make an informed decision. Further modelling of these calls may be improved by incorporating linked patient outcome information, such as mortality rates, admission rates and other diagnostic information, to generate evidence when combined with acuity information to manage risk.
Inter-rater agreement between paramedics and nurses increased over the study period; however, the rationale for this change is uncertain. There were no changes to paramedic or nurse acuity protocols, and no additional CTAS education for paramedics that could explain the progression to higher agreement. Further examination is needed to identify the factor(s) driving this trend towards increasing agreement of patients presenting to paramedics. The rising rates of agreement observed with increasing paramedic certification (primary care paramedic, to primary care paramedic with intravenous autonomous, to advanced care paramedic) may suggest enhanced acuity proficiency and recognition, or higher experience level.
This is the first comprehensive study of inter-rater acuity agreement examining both potential clinical and operational influencers on paramedics’ application of acuity using CTAS. Since CTAS is widely used by both hospitals and paramedic services, these findings may be generalized to other areas where similar standardized measures of acuity are utilized for triage by paramedics and nurses, or by paramedics alone for the purposes of assigning acuity.
Limitations
This study was conducted using data from a single paramedic service in one Canadian municipality. There are slight variations expected between paramedic and nurse acuity assignment, particularly as hospitals have some assessment-based modifiers incorporated into the eCTAS program, which are not available to paramedics.
While transport times during this study period were relatively short, it is acknowledged that patient acuity may have changed from the time of paramedic scene departure to arrival at hospital based on condition progression, which may derive temporal and contextual differences. As this value was not available in the data set, the extent to which acuity might have changed is unknown. Despite attempts to ensure independence of rater assignment of acuity, there may be a small inherent degree of influence from paramedics on nurse acuity decision-making at the hospital.
Given the large sample size, statistically significant findings may reflect small differences that are unlikely to be clinically meaningful. Accordingly, results are interpreted with emphasis on the magnitude and clinical relevance of associations rather than statistical significance alone. Finally, individual paramedic experience level or years since initial paramedic training could not be accounted for, as these data are not available. The most recent acuity and CTAS training for all paramedics in this system occurred in 2018, or during new hire orientation for those employed since then.
Conclusions
Paramedics and nurses demonstrated agreement rates ranging from ‘fair’ to ‘substantial’ on patient acuity, showing an overall moderate agreement. There were higher rates of disagreement amongst lower acuity patients, patients with presentations of mental illness and soft tissue injury or pain and paediatric patients. Operational factors such as health system ‘busyness’, choice of destination type and time to shift end were not significantly associated with paramedic decision-making. These results suggest areas for further investigation, including whether decision-support tools or additional education may improve concordance. Further study is required to understand potential implications for paramedic practice and for EMS system design, where data on patient acuity may be used to inform response prioritization.
Footnotes
Acknowledgements
The authors thank Nadia Firdaus (Niagara EMS) for data collection. They also thank the Paramedics of Niagara EMS for their ongoing commitment to excellence.
Ethical considerations
This study received ethical approval from the Hamilton Integrated Research Ethics Board (approval #16921) on 9 February 2024.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant data are within this paper and its supporting materials. The minimum dataset cannot be shared publicly due to the legal health data restrictions in Ontario, Canada.
Appendix 1.
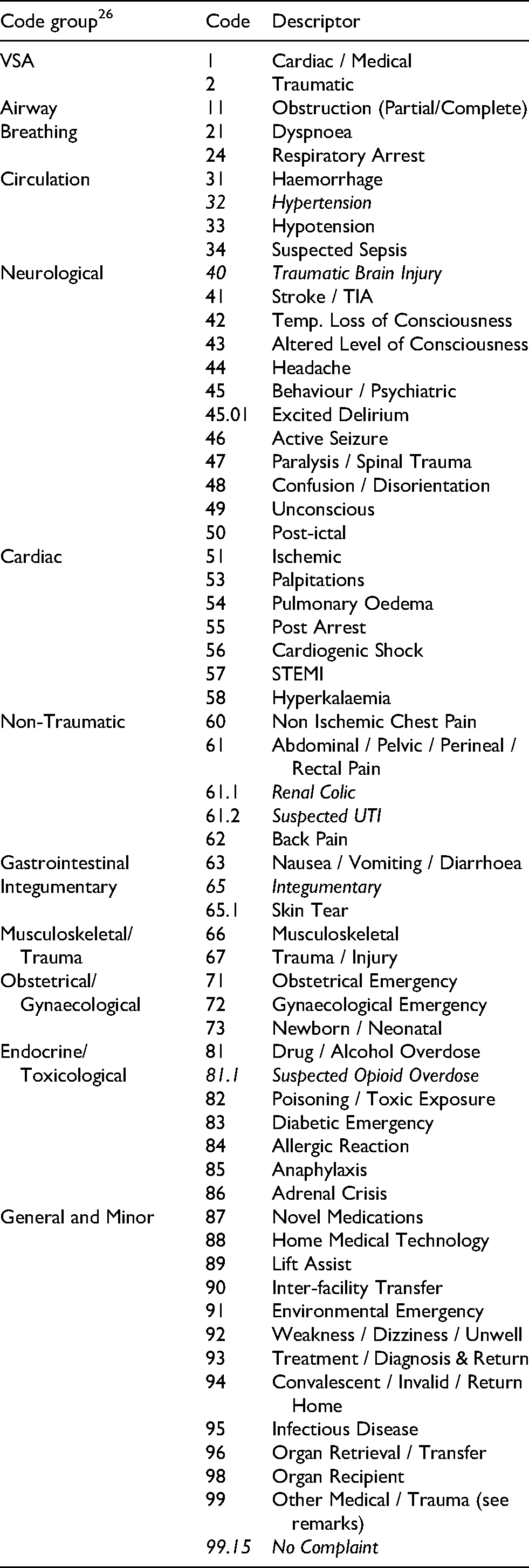
| Code group 26 | Code | Descriptor |
|---|---|---|
| VSA | 1 | Cardiac / Medical |
| 2 | Traumatic | |
| Airway | 11 | Obstruction (Partial/Complete) |
| Breathing | 21 | Dyspnoea |
| 24 | Respiratory Arrest | |
| Circulation | 31 | Haemorrhage |
| 32 | Hypertension | |
| 33 | Hypotension | |
| 34 | Suspected Sepsis | |
| Neurological | 40 | Traumatic Brain Injury |
| 41 | Stroke / TIA | |
| 42 | Temp. Loss of Consciousness | |
| 43 | Altered Level of Consciousness | |
| 44 | Headache | |
| 45 | Behaviour / Psychiatric | |
| 45.01 | Excited Delirium | |
| 46 | Active Seizure | |
| 47 | Paralysis / Spinal Trauma | |
| 48 | Confusion / Disorientation | |
| 49 | Unconscious | |
| 50 | Post-ictal | |
| Cardiac | 51 | Ischemic |
| 53 | Palpitations | |
| 54 | Pulmonary Oedema | |
| 55 | Post Arrest | |
| 56 | Cardiogenic Shock | |
| 57 | STEMI | |
| 58 | Hyperkalaemia | |
| Non-Traumatic | 60 | Non Ischemic Chest Pain |
| 61 | Abdominal / Pelvic / Perineal / Rectal Pain | |
| 61.1 | Renal Colic | |
| 61.2 | Suspected UTI | |
| 62 | Back Pain | |
| Gastrointestinal | 63 | Nausea / Vomiting / Diarrhoea |
| Integumentary | 65 | Integumentary |
| 65.1 | Skin Tear | |
| Musculoskeletal/Trauma | 66 | Musculoskeletal |
| 67 | Trauma / Injury | |
| Obstetrical/Gynaecological | 71 | Obstetrical Emergency |
| 72 | Gynaecological Emergency | |
| 73 | Newborn / Neonatal | |
| Endocrine/Toxicological | 81 | Drug / Alcohol Overdose |
| 81.1 | Suspected Opioid Overdose | |
| 82 | Poisoning / Toxic Exposure | |
| 83 | Diabetic Emergency | |
| 84 | Allergic Reaction | |
| 85 | Anaphylaxis | |
| 86 | Adrenal Crisis | |
| General and Minor | 87 | Novel Medications |
| 88 | Home Medical Technology | |
| 89 | Lift Assist | |
| 90 | Inter-facility Transfer | |
| 91 | Environmental Emergency | |
| 92 | Weakness / Dizziness / Unwell | |
| 93 | Treatment / Diagnosis & Return | |
| 94 | Convalescent / Invalid / Return Home | |
| 95 | Infectious Disease | |
| 96 | Organ Retrieval / Transfer | |
| 98 | Organ Recipient | |
| 99 | Other Medical / Trauma (see remarks) | |
| 99.15 | No Complaint |