
Abstract
Demand for mental health care from U.K. ambulance services is increasing, yet paramedics report feeling underprepared to manage these presentations. This study aimed to identify knowledge gaps, educational needs, and systemic factors shaping frontline paramedics’ ability to provide mental health care in England, examining: (1) mental health education and training at pre- and post-registration levels; and (2) paramedics’ experiences of managing mental health presentations. A two-phase mixed-methods design was employed across England. Phase 1 comprised a national review of pre-registration curricula across Higher Education Institutions and post-registration training provided by NHS ambulance services. Data were collected via surveys of programme and mental health leads, supplemented by publicly available curricula, synthesised descriptively. Phase 2 involved semi-structured interviews with 20 frontline paramedics. Case-based vignettes and a think-aloud approach were used to explore clinical reasoning. Data were analysed inductively using reflexive thematic analysis. Phase 1 identified substantial heterogeneity in the structure, content, and transparency of mental health education. Dedicated mental health modules, placements, and simulation were inconsistently provided, and post-registration training varied widely in duration, mandatory status, and topic coverage, with limited protected time for mental health learning. Phase 2 generated four interrelated themes. Paramedics described feeling underprepared for the complexity of mental health care, with reliance on experiential learning (“No one taught me any of this”). System constraints further complicated care (“Pitfalls and loopholes”). Managing risk, capacity, safety, and autonomy was described as ethically and emotionally demanding (“You have to deal with complexity”). Communication and relational skills were viewed as central yet insufficiently supported through formal education (“It's all about how you talk to them”). There is a clear misalignment between the realities of frontline paramedic practice and current mental health education and training. A more consistent, applied, and system-informed approach is required to strengthen clinical confidence and improve patient care.
Introduction
Mental health conditions represent a growing global public health challenge. Recent World Health Organization (WHO) estimates indicate that more than one billion people worldwide are living with a mental health condition, with disorders such as anxiety and depression contributing substantially to human suffering and economic burden. 1 In England, approximately one in five adults (20.2%) is estimated to be living with a common mental health problem, with the economic cost of poor mental health calculated at £300 billion per year. 2 Prevalence has increased among working-age adults (16–64 years), rising from 17.6% in 2007 to 22.6% in 2023/2024. 3
Socioeconomic inequalities are pronounced, with a higher prevalence of mental health issues in the most deprived areas of England (26.2%) compared with the least deprived (16%). 4 Individuals experiencing debt are double as likely to report a mental health problem compared to those without debt (39% vs. 18.4%), while rates among the unemployed (40%) are higher than those in employment (18.3%). 4 Alongside these structural inequalities, stigma and discrimination persist. Stigmatised attitudes towards mental illness are widely reported, with nearly half of the U.K. expressing feelings of shame associated with conditions such as depression and schizophrenia, and 48% of people with severe mental illness reporting discrimination from healthcare professionals. 2 Despite ongoing public awareness efforts, most people with mental health conditions report insufficient societal understanding, reluctance towards social integration and the use of negative labels. 2 These aspects compound the challenges faced by those living with mental health conditions and place increasing demands on frontline healthcare services.
According to the National Health Service (NHS), mental health services in England received 4.6 million referrals between April 2022 and March 2023, representing a significant increase (up 22% from 2019). 5 The growing demand for mental health support continues to exceed the capacity of available services, leaving approximately 1.2 million people on waiting lists for NHS community mental health treatment. 6 This unmet need places substantial strain on paramedics, who spend an estimated 1.8 million hours annually responding to mental health-related calls. 7 The increasing burden on ambulance services is reflected in the sharp rise in mental health-related 999 calls, which escalated from 524,485 in 2018–2019 to 652,720 in 2021–2022: a 24% increase in 3 years. 8
U.K. paramedics are frequently the first responders to patients with mental health care needs, including acute emergencies such as suicide attempts, as well as cases where pre-existing mental health conditions coexist with other medical issues that prompt ambulance calls (e.g., a suspected heart attack in an individual with anxiety or depression).9,10 While paramedics do not diagnose mental illness, they are responsible for responding to mental health-related calls within the ambulance triage system. 10
Despite the growing number of patients experiencing mental illness and requiring paramedic intervention, research indicates that paramedic students express a lack of willingness to interact with patients experiencing mental illness. 11 Paramedics report feeling inadequately prepared to manage such patients effectively,12,13 while often holding stigmatised views.13,14 A perceived lack of mental health education, support and training has been linked to frustration and uncertainty in providing patient care.13,15,16
Currently, there is no standardised educational requirement for paramedics regarding the care of individuals with mental health conditions, and several studies highlight the need for more comprehensive undergraduate and in-service training to enhance paramedics’ competence.17-19 A scoping review underscored that enhanced education and support are critical to improving paramedic experience when managing mental health-related cases. 7
Despite these findings, current mental health-related education provided to paramedic students and registered professionals has not been systematically examined. Evidence suggests that education aimed at enhancing paramedics’ mental health literacy,20,21 aided by the application of practical scenarios 22 and the inclusion of mental health placements as part of the undergraduate curriculum, 23 may be beneficial. However, there is limited understanding of the specific knowledge gaps that underlie paramedics’ concerns. Additionally, little of the existing research has focused on the context for paramedics in England, with most studies conducted in Australia.
Aim of the study
The aim of this mixed-methods study was to identify and assess knowledge gaps and educational needs related to the provision of mental health care among the frontline ambulance paramedic workforce in England.
Methodology
Study design
This study employed a sequential exploratory mixed-methods design to: investigate mental health education provision for paramedics in England; and explore paramedics’ knowledge when managing patients experiencing mental health issues. Figure 1 depicts a methods flow diagram for the study. Phase 1 comprised a national review of mental health education and training provided to paramedics at pre-registration (university-level) and post-registration (in-service) stages. Phase 2 involved qualitative interviews with frontline paramedics using case-based vignettes. Preliminary analysis of phase 1 findings was undertaken prior to commencement of phase 2 interviews. Early findings from Higher Education Institution (HEI) curricula, programme lead (PL) survey responses, and ambulance service mental health lead survey responses informed the initial development of the interview guide and prompts used in phase 2, as well as the vignettes. The interview guide was refined iteratively during ongoing phase 1 data collection, primarily through modification of prompts and areas of emphasis. Integration occurred during study design, interpretation of findings, and synthesis within the Discussion. We adhered to the Good Reporting of a Mixed Methods Study (GRAMMS) 24 (Supplement A) and to the Reflexive Thematic Analysis Reporting Guidelines (RTARG). 25
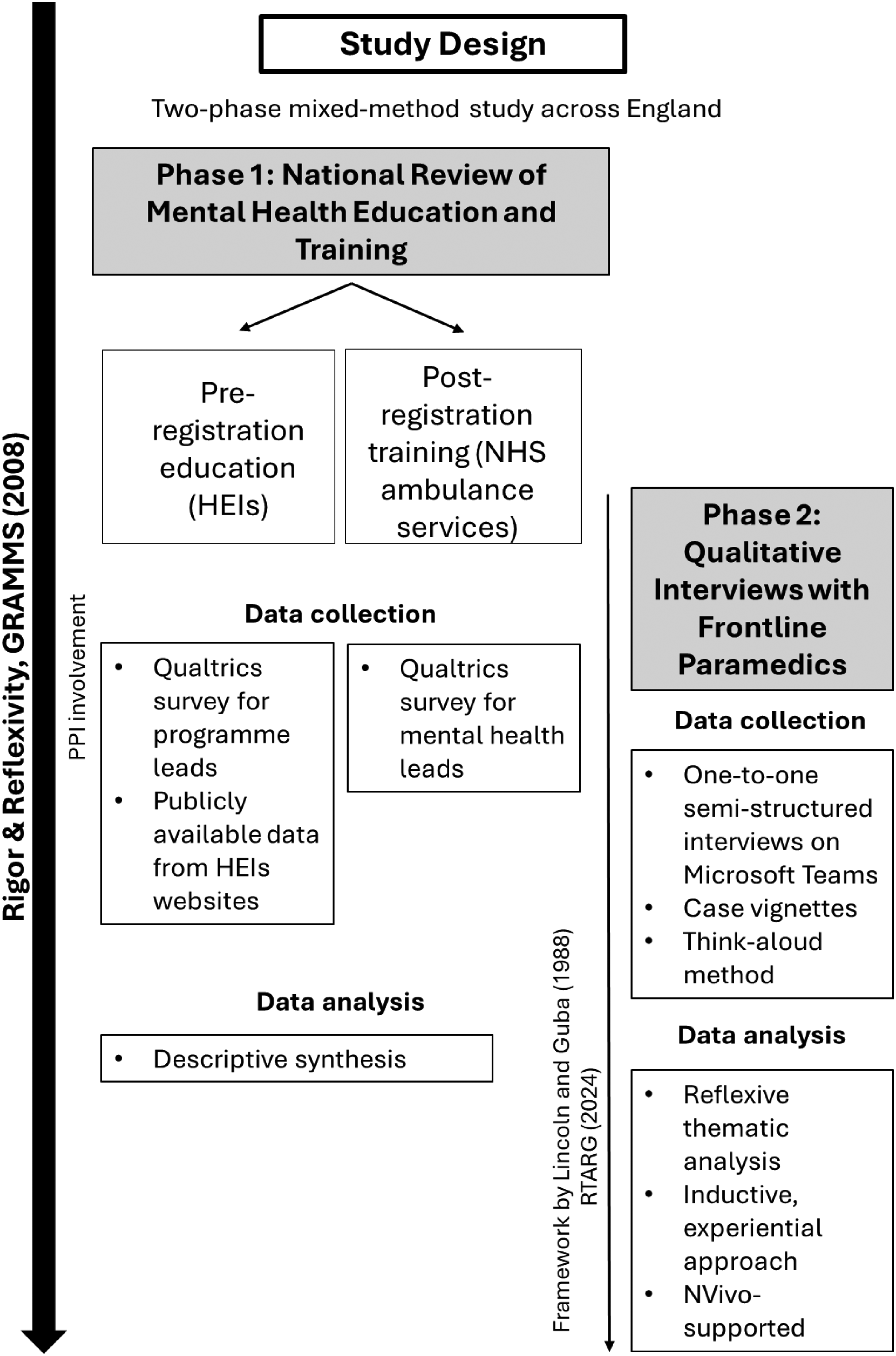
Methods flow diagram.
Phase 1: review of mental health education and training
Phase 1 involved a structured review of mental health education provision within pre-registration undergraduate paramedic programmes delivered by Higher Education Institutions (HEIs) across England, alongside post-registration mental health training provided by NHS ambulance services.
Data collection
Information on pre-registration education was collected from PLs responsible for all identified paramedic science degrees at English HEIs using a brief online survey on Qualtrics (see Supplement B), which remained open from April 2025 to January 2026. This was supplemented by publicly available data from institutional websites, including programme specifications and module descriptors. Publicly available curriculum information was systematically identified from HEI websites and programme specifications using predefined search terms including “mental”, “psych”, and “dementia”. The review was conducted in June 2025 and reflects provision for the 2025–2026 academic year.
Information on post-registration education was obtained via the National Ambulance Mental Health Group, which comprises mental health leads from NHS ambulance services in England (see Supplement C). Mental Health Leads were asked to complete a brief survey on Qualtrics, which remained open from April to December 2025. This ensured comprehensive national coverage of in-service mental health training provision.
PLs and mental health leads were sent regular reminders to complete the Qualtrics survey throughout the recruitment window.
The two brief Qualtrics surveys were developed by the research team based on the study aims, relevant literature, and discussions with the PPI advisory group. They were designed for descriptive mapping purposes and no formal psychometric validation was undertaken; however, survey items were reviewed for clarity and relevance by the research team prior to distribution.
Data analysis
Data extracted from website materials and Qualtrics survey responses were organised into structured comparison tables to facilitate descriptive synthesis across institutions and ambulance services. Analysis focused on identifying similarities and differences in the structure, visibility, depth, and delivery of mental health education and training provision. These findings were then narratively synthesised to identify areas of heterogeneity and potential educational gaps relevant to the study aims.
Phase 2: qualitative interviews
Participants and sampling
Eligible participants were HCPC-registered paramedics working as frontline clinicians within NHS ambulance services in England. Non-registered ambulance clinicians (e.g., technicians) and other healthcare professionals were excluded, as paramedics typically act as the primary clinical decision-makers at scene.
Initial recruitment aimed for 15–20 participants. However, recruitment was guided by the principle of information power, 26 whereby sample adequacy depends on study aim, sample specificity, quality of dialogue, and analytic strategy. Recruitment continued until the research team determined that sufficient rich data had been generated to address the research questions.
Purposive sampling 27 was used to ensure variation in geographical location, ambulance service, role seniority, length of experience, and educational background. Recruitment took place between July and November 2025.
Recruitment and data collection
Ethical approval was granted by the University of Southampton Faculty of Environmental and Life Sciences Ethics Committee (ERGO ID: 103415). Participants were recruited via professional and social media platforms, including the Royal College of Paramedics research page, X, LinkedIn, Bluesky, and Facebook. Interested paramedics accessed a participant information sheet and completed eligibility screening, including provision of their HCPC registration number to confirm eligibility.
Participants took part in a one-to-one semi-structured interview with F.Z. via Microsoft Teams to maximise accessibility and geographical reach. Interviews were video-recorded, lasted between 37 and 68 min (mean 49 min), and were transcribed verbatim.
Emerging findings from Phase 1 informed development of the Phase 2 indicative interview guide and prompts used during the qualitative interview. Specifically, variability in mental health teaching, resources and support available, exposure to applied mental health scenarios, time allocated to mental health-related content and modality of delivery shaped interview prompts exploring confidence, communication, risk assessment, decision-making, needs and perceptions of training. The indicative interview guide (Supplement D) was refined collaboratively with a dedicated patient and public involvement (PPI) advisory group (n = 6), who contributed throughout study design, data collection, and dissemination. PPI involvement is reported using the short form of the Guidance for Reporting Involvement of Patients and the Public Checklist 2 (GRIPP2) 28 (Supplement E).
To explore clinical judgement, interviews incorporated real-world case vignettes reflecting common mental health presentations in pre-hospital care.29,30 The three vignettes (Supplement D) were initially developed by the research team based on common pre-hospital mental health presentations identified from clinical experience and the literature, and subsequently refined with feedback from the PPI advisory group. Vignette methodology was chosen as it encourages openness, minimises idealised responses, and allows decision-making processes and knowledge gaps to be investigated. 30 A think-aloud method was used alongside the vignettes to elicit participants’ cognitive processes and decision-making in real time.31-33 Demographic information was collected at interview completion. Participants received a gift voucher in recognition of their time.
Data analysis
Qualitative data were analysed using reflexive thematic analysis (RTA) following Braun and Clarke's six-phase approach.34,35 An inductive, data-driven strategy was adopted. Analysis was supported by NVivo (version 14, Lumivero). RTA is theoretically flexible, with no fixed epistemological or ontological framework. 35 Given our goal of understanding paramedics’ experiences and needs when managing patients with mental health conditions, we adopted an experiential qualitative approach, which focuses on how people make sense of their realities, their worldviews, and frames of reference. 35 Our study was grounded in a critical realist ontological perspective, which acknowledges both the existence of an objective reality (realism) and how human experiences and practices shape our understanding of it (relativism).35,36 Our phenomenological epistemological stance further emphasises first-person lived experience, treating the subjective experiences of our participants as valid and meaningful in understanding reality. 35
For the duration of the research process, the authors actively engaged in reflexivity, critically examining how their own experiences, values, and identities shaped the study. Reflexive team discussions, ongoing PPI engagement, and reflexive diaries were maintained throughout the project (Supplement F).
Rigour was ensured through attention to credibility, dependability, confirmability, and transferability, consistent with the framework outlined by Lincoln and Guba 37 and adherence to the RTARG. 25
Results
Phase 1
Review of mental health education in pre-registration paramedic curricula
Thirty-five HEIs in England were identified as offering an undergraduate B.Sc. (Hons) pre-registration programme in Paramedic Science.
Twelve PLs provided information regarding mental health education delivered within their programmes. Responses indicated substantial heterogeneity in the structure, intensity, and approach to mental health education across pre-registration paramedic programmes (Table 1).
Mental health education delivered within paramedic programmes in England, reported by PLs.
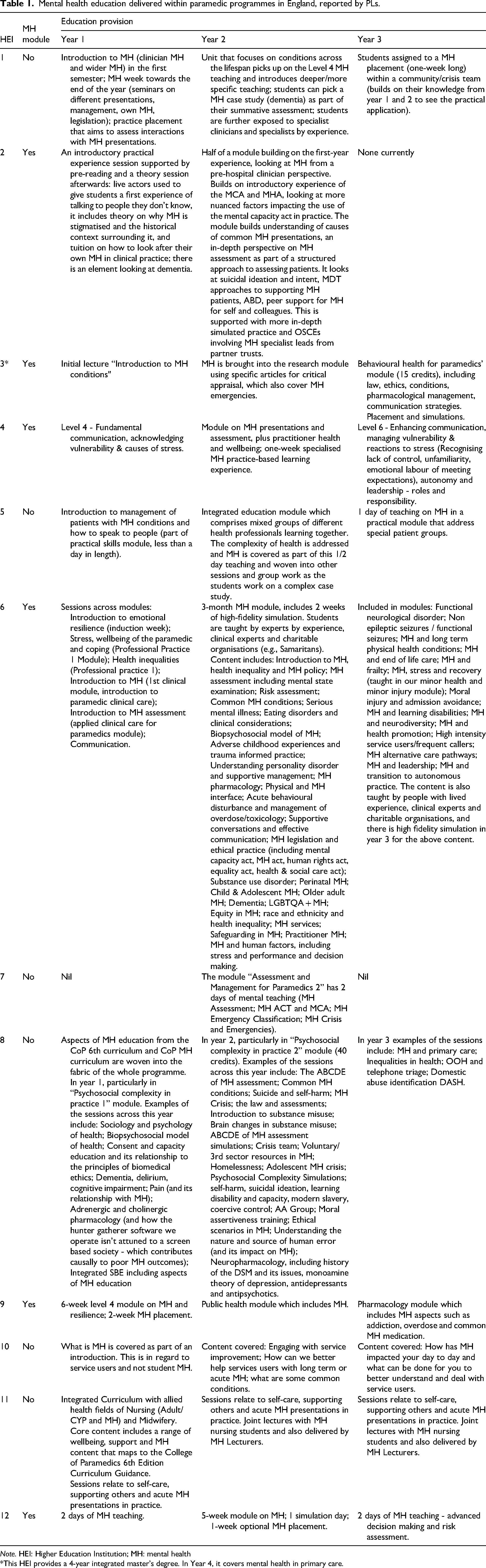
Note. HEI: Higher Education Institution; MH: mental health
*This HEI provides a 4-year integrated master's degree. In Year 4, it covers mental health in primary care.
Of the 12 PLs who completed the study form, half (6/12) reported delivering a dedicated mental health module. Where present, these modules varied in length and level, ranging from short introductory modules in early years to larger credit-bearing modules later in the programme. Some PLs reported the absence of a standalone mental health module, instead describing mental health as intentionally embedded across multiple modules and years of study. Experiential learning formed a core component of mental health education in several programmes. PLs reported the use of high-fidelity simulation, objective structured clinical examinations (OSCEs), scenario-based learning, and teaching delivered by people with specialist and lived experience. A smaller number of programmes offered dedicated short mental health placements, while others noted opportunities for optional placements or mental health within broader practice-based learning.
The level of publicly available information relating to mental health education varied considerably across HEIs. Of the 35 institutions, 13 provided a full programme specification online. Several HEIs listed core modules accompanied by summaries of content, while others provided only module titles with no further description. As a result, the extent and depth of mental health education could not be consistently determined from website information alone. Where detail was available, mental health content was described as being integrated within broader modules addressing clinical assessment, professional practice, psychosocial complexity, or public health, rather than delivered as a discrete, standalone mental health module. In some instances, there was explicit reference to mental health placements or simulations. In eight programmes, there was no mention of mental health or psychology-related content in any of the publicly available programme information. A full summary of website-derived data is provided in Supplement G.
Review of post-registration mental health training provided by ambulance services
Mental Health Ambulance Leads from nine of the 11 ambulance services in England provided information on post-registration mental health training for frontline paramedics (one service did not have a mental health lead in post at the time of data collection, and one service did not respond).
Training content varied across services. Legislation-related training (including the Mental Health Act (MHA) and Mental Capacity Act (MCA)) was the most consistently reported topic, alongside mental health conditions, self-harm/suicide, and staff wellbeing. Fewer services reported training content specifically addressing older adults’ mental health, children and young people's mental health, LGBTQIA + topics, or additional “other” areas (see Figure 2).
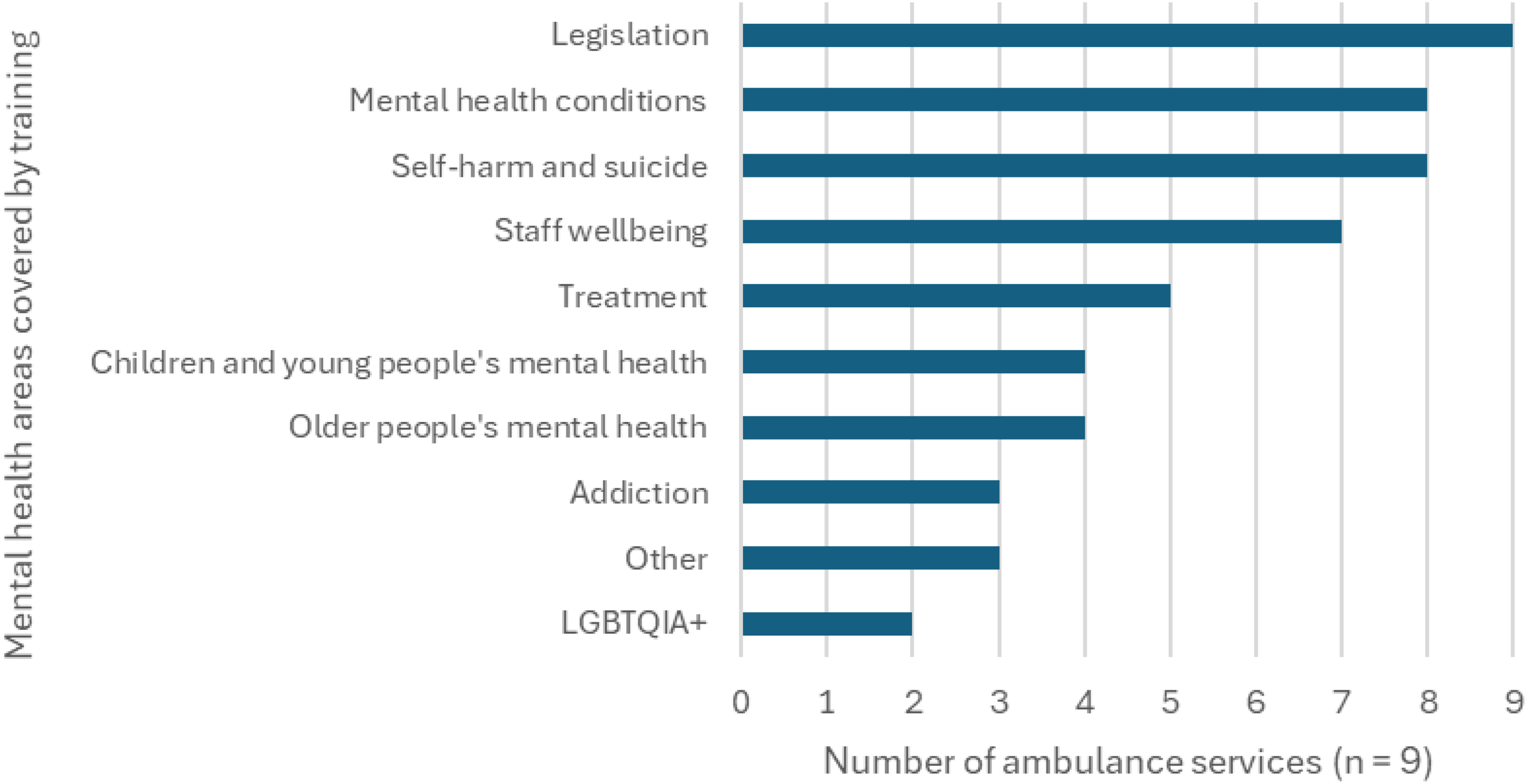
Mental health areas included in post-registration paramedic training (n = 9 ambulance services).
Reported time spent on mental health education varied, and not all services were able to provide numeric estimates for training hours. Among services providing numeric data, estimated annual hours ranged widely across services and delivery modes, and mandatory mental health training accounted for a variable proportion of overall education time (Table 2). The approach to provision also differed: some services described provision that was not delivered annually, and some reported that structured provision was primarily limited to new starters through induction, with additional continuing professional development (CPD) available but not mandated for all staff.
Reported annual mental health training hours provided by ambulance services in England (n = 9).
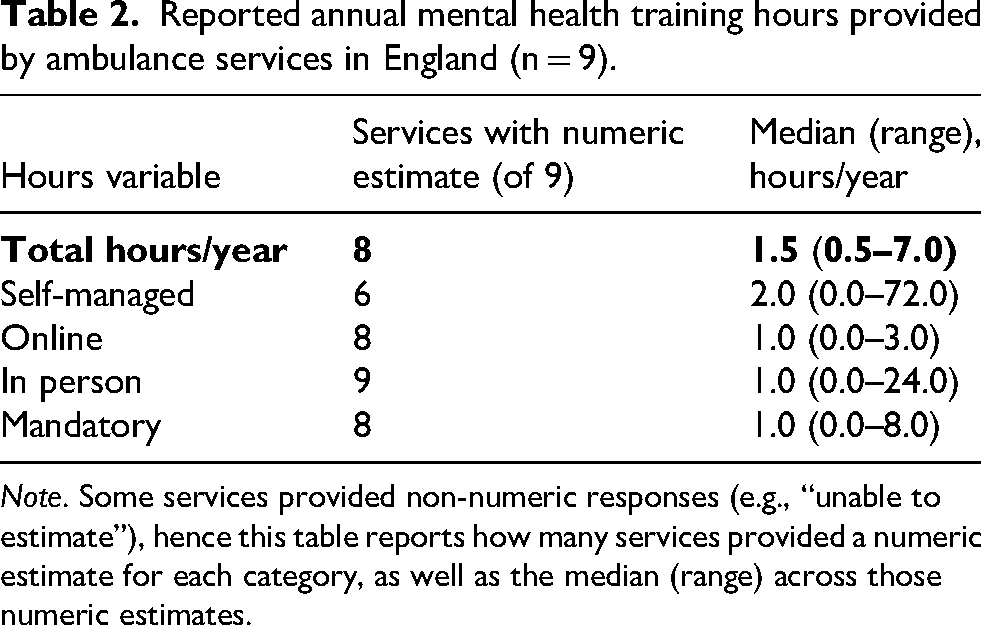
Note. Some services provided non-numeric responses (e.g., “unable to estimate”), hence this table reports how many services provided a numeric estimate for each category, as well as the median (range) across those numeric estimates.
Most services described plans to maintain and/or develop mental health training provision, including updating training content (e.g., in response to policy or legal changes), ongoing review of training materials, and, in some cases, training needs analysis or investment in CPD pathways. A minority of leads highlighted implementation constraints, including limited education capacity, competing organisational priorities, and a reliance on voluntary training in their own time, which in some cases restricted the ability to expand provision or mandate additional training.
Phase 2
Participant characteristics
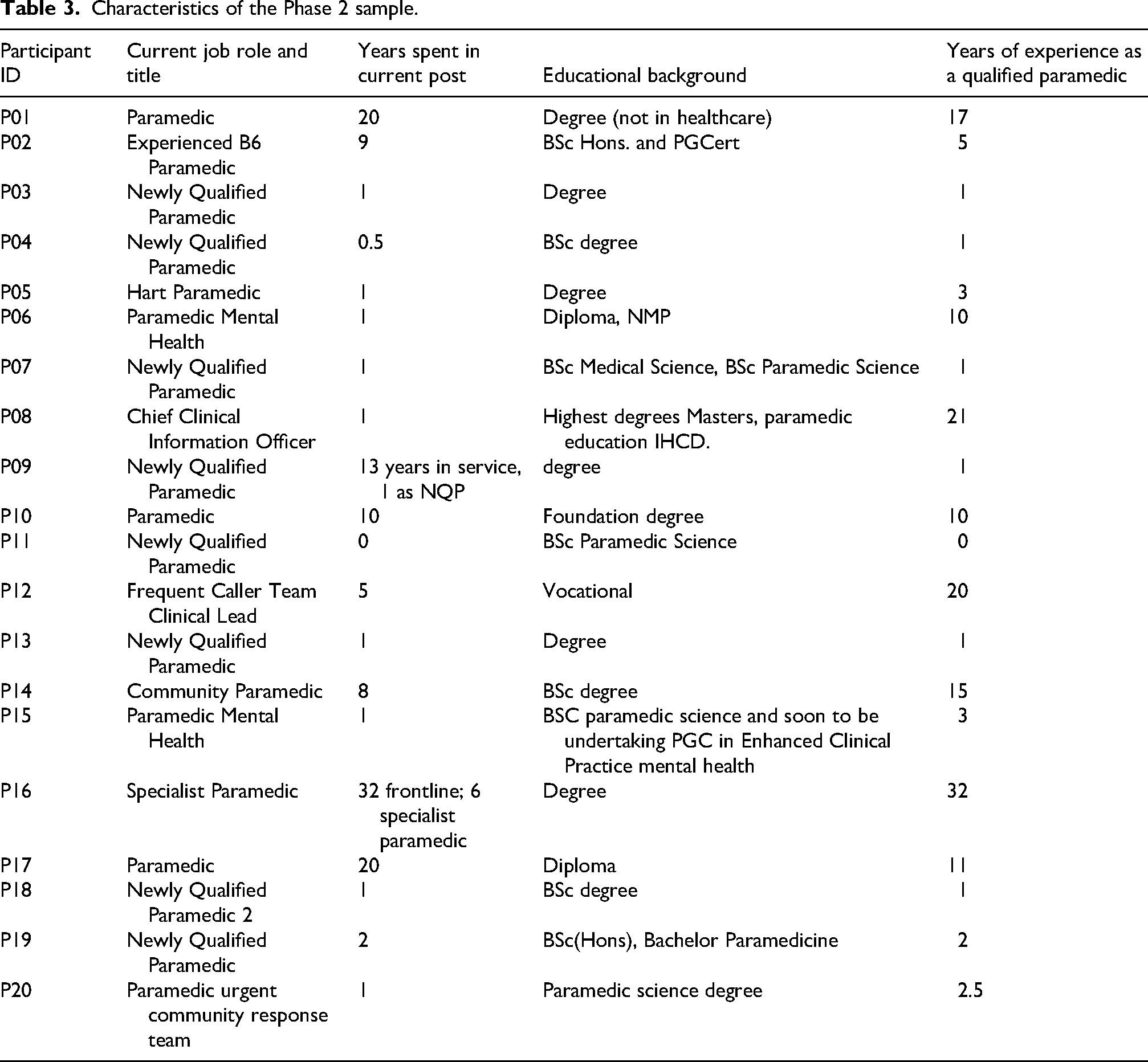
Forty-one participants completed the online screening and consent form. Of these, n = 8 were deemed ineligible as they provided an invalid HCPC number, and n = 5 did not respond to the researcher to arrange the interview. A further n = 8 were eligible but were not interviewed as the research team, guided by the concept of information power, determined that sufficient high-quality data had been collected and that these additional participants would not enhance the demographic diversity of the sample. This resulted in a final dataset of n = 20 participants (n = 11 males, n = 9 females). Participants were drawn from eight ambulance services in England: London Ambulance Service NHS Trust (n = 4), Yorkshire Ambulance Service NHS Trust (n = 4), South East Coast Ambulance Service NHS Foundation Trust (n = 3), South Western Ambulance Service NHS Foundation Trust (n = 3), East Midlands Ambulance Service NHS Trust (n = 2), North East Ambulance Service NHS Foundation Trust (n = 2), South Central Ambulance Service NHS Foundation Trust (n = 1), and North West Ambulance Service NHS Trust (n = 1). Participant characteristics are summarised in Table 3.
Characteristics of the Phase 2 sample.
Themes
A thematic map of results is shown in Figure 3. Analysis generated four interrelated themes describing how paramedics experience, understand, and manage mental health presentations in practice. Across themes, participants emphasised the growing prevalence and complexity of mental health calls and described a persistent mismatch between the realities of contemporary paramedic work and the education, training, and system-level support currently available. Overall, paramedics reported managing mental health presentations with limited preparation, high emotional load, and reliance on communication skills.
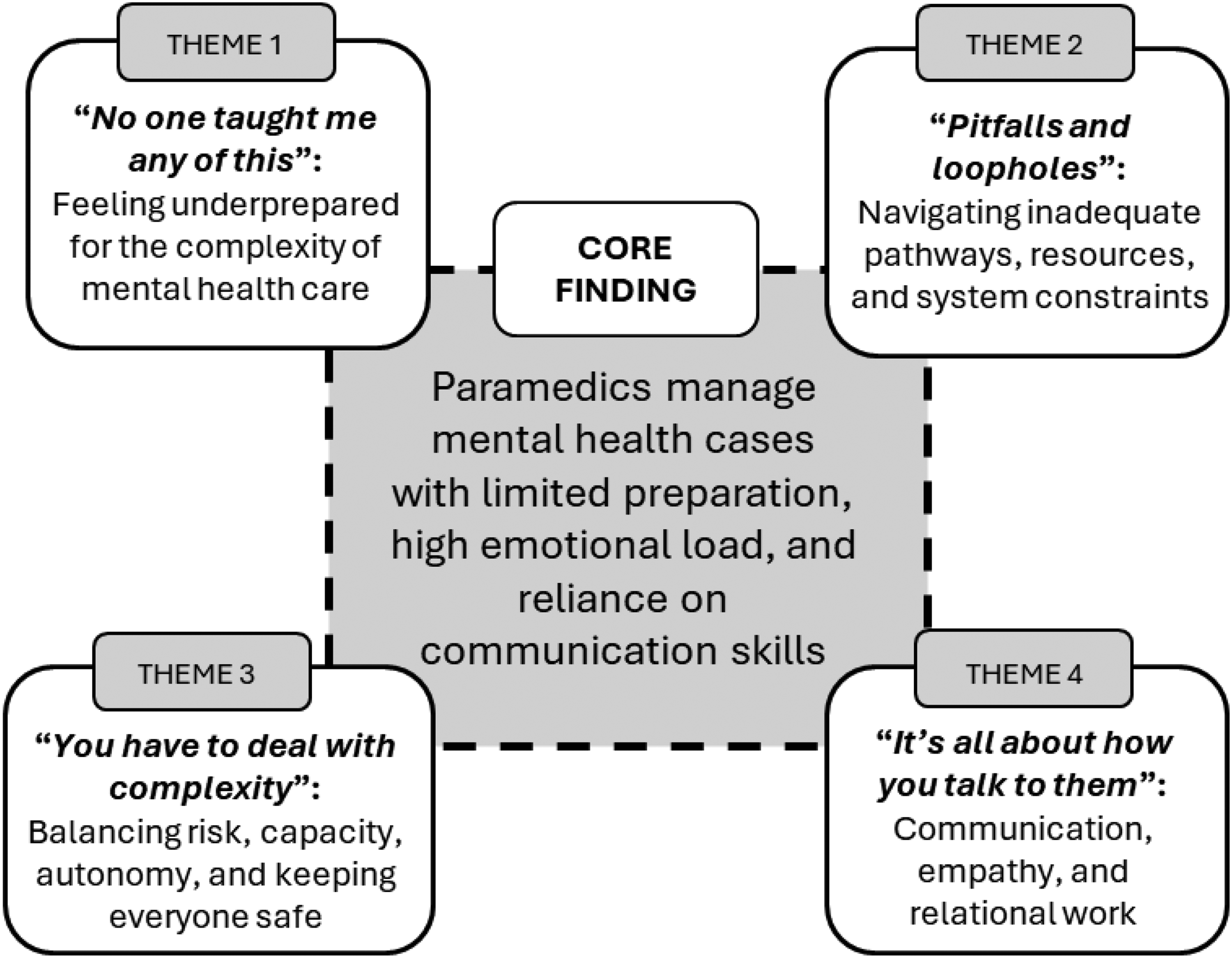
Thematic map.
Theme 1: “No one taught me any of this”: feeling underprepared for the complexity of mental health care
Participants consistently described mental health presentations as common (“mental health is such a crisis these days, we see it all the time”, P19) and time-consuming yet felt insufficiently prepared to manage them (“we go… but we’re very ill-equipped to go”, P06).
This sense of under-preparedness spanned foundational clinical knowledge (e.g., recognising and differentiating mental health presentations, understanding specific conditions such as bipolar disorder, and interpreting physical symptoms linked to anxiety or distress), as well as skills to manage mental health conditions and symptoms.
Participants described mental health calls as unpredictable and highly individualised, lacking clear algorithms and procedural pathways that typically guide physical health emergencies. As a result, cases were consistently framed as complex and challenging. It's difficult… not one size fits all, does it? The cardiac arrest you know you follow on algorithm whereas with mental health, it's really difficult to follow an algorithm because everybody's different, and everybody's mental health affects them differently (P09).
Overall, paramedics recognised mental health care as a central part of their workload, yet experienced their education and training as lagging behind service realities. Knowledge gaps were not framed as isolated technical deficits but as broader, systemic under-preparedness, leaving practitioners reliant on informal learning, observation, and trial-and-error approaches. No one's taught me this by the way, this is what I’ve observed, being able to live with uncertainty, create frameworks and boundaries to be able to describe a complex pattern… kind of emotional responses and relationships which maybe overlaid or underlaid by some kind of pathological diagnosis (P08).
Mental health calls were also described as emotionally demanding. Participants reported feelings of responsibility, guilt, frustration, and doubt, sometimes persisting long after the call. The emotional burden was heightened by limited resources, unclear pathways, and restricted authority, leaving paramedics feeling accountable for outcomes they could not fully control. We’re first there, first to attend… so, we carry the weight of everything really and, I think, a lot of people expect us to not necessarily make the right decision (P17).
Theme 2: “Pitfalls and loopholes”: navigating inadequate pathways, resources, and system constraints
Participants described significant challenges arising from the systems surrounding mental health care. Even when paramedics felt able to assess and support patients, they often encountered limited referral options, inconsistent pathways across regions, and poor access to mental health services, particularly out-of-hours.
Structural barriers included difficulty contacting crisis teams and communicating with other professionals, long waiting times, lack of community alternatives, no access to patient medical records, and challenges managing cases involving alcohol or other substances. There are some massive loopholes within the mental health services and, I think, it's a domino effect. I don’t know what the best way forward is in regards to these kind of things, but I do know that… I’m sure they’re doing their best with the resources that they’ve got as we all do, but there's definitely some massive pitfalls and loopholes within the services… (P17)
Participants highlighted a disconnect between police and ambulance services, mainly linked to the “right care, right person” (RCRP) approach,
38
with police seen as difficult to involve in mental health calls. I would say there is a disjoint between the police Right Care, Right Person and ambulance about how you manage these cases. There is complete disharmony at times between the two and you end up being in limbo about who should be managing and the best way to manage this cohort of patients because the police work very differently to ambulance. Very differently. And even though I can understand why they brought it in and, I think, it's absolutely right, there is a disjoint between the two (P12). Sometimes there's nowhere for them to go but A&E, if that makes sense, and A&E isn’t always the right place for somebody to go when they’re in crisis (P09).
Theme 3: “You have to deal with complexity”: balancing risk, capacity, autonomy, and keeping everyone safe
Managing mental health presentations was described as a constant balancing act. Participants highlighted the complexity of assessing risk, determining capacity, safeguarding patients and others, and respecting autonomy within legal and ethical boundaries.
Capacity assessments were repeatedly described as “subjective” (P02) and context-dependent, particularly in cases involving distress, alcohol, drugs, or fluctuating presentations. Additionally, managing cases where patients were deemed to lack capacity was also seen as complex (“If she wasn’t really cooperative and not communicating with us and I had reason to believe that she was sort of not of sound mind and not meeting that threshold for mental capacity, then that's usually where our job gets quite difficult”, P11 discussing vignette 1).
Safety, of the patients as well as of the crew, was often reported as “paramount” and participants described risk assessment and safeguarding as among the most stressful and knowledge-dependent aspects of practice. Decisions often involved negotiating patient wishes, anticipating escalation, and ensuring safety in the absence of clear thresholds or consistent guidance.
Decision-making was described as iterative and situational, often involving parallel physical and mental health assessments, negotiation with patients and families, and frequent reassessment. The social context was reported as particularly important, with care plans shaped by living circumstances, available support networks, and the involvement of family members, friends, or housemates. Across accounts, “recognising the level of urgency” (P16) and collecting information to “build a complete picture” (P01, P14) were described as central to decision-making. Moreover, de-escalation and conflict resolution were viewed as essential skills, yet ones that, for many, required further training and support.
Participants described varying approaches to involving patients in decision-making. While some emphasised respecting patients’ wishes and avoiding any sense of coercion, others described using persuasion, rapport-building, or “befriending” strategies to guide patients toward what they perceived as the safest or most appropriate option. Many recognised the ethical difficulty of determining where support ends, and coercion begins, particularly when refusal, distress, and ongoing risk intersected.
Areas of discrepancy and inconsistency emerged, particularly regarding decisions to convey patients to hospital and the involvement of police. These decisions were influenced by patient preferences, trust protocols, clinical judgement, and differing levels of confidence. While some participants described pre-emptively involving police, others were hesitant, expressing concern that police presence could escalate situations. Many reported uncertainties about when police involvement was necessary (It's difficult to know when to call police sometimes because it's either obvious that they need to be there, and sometimes it's very much borderline, P02).
Participants often described seeking support to manage complex mental health cases, including contacting healthcare professionals, mental health services, senior clinicians, or crisis teams, although access varied by service and depended on resources available. I would just ask for help because I wouldn’t really know what to do (P19, discussing vignette 3). We’ve got a really, really good mental health crisis service down where I am and ninety-nine percent of the patients I go to who present with mental health, I will speak to for background information that I can’t see on their GP records, any previous engagements, sort of reaching out crisis, and then just sort of some shared sort of decision-making in regards to what's best (P03).
Overall, paramedics reported having to consider and investigate a wide range of factors on scene, including physical health, medical history, previous service access, mental state, risk and protective factors, family dynamics, available services, and longer-term plans or outcomes. In the absence of structured frameworks, they emphasised the need to remain flexible, adapt rapidly to context, and “deal with complexity” (P08). However, approaches to the vignettes varied substantially, particularly in what participants prioritised and how they structured their assessment. Participants emphasised the importance of education that supports working with uncertainty, avoiding “jumping to conclusions” (P08), and taking a holistic view of presentations. Similarly, reflecting on the frequent overlap between physical and mental health presentations, it was also suggested that pre-registration education should integrate mental health content throughout the curriculum, rather than isolating it within a single module. I think, probably, thirty/forty percent of patients present either with a primary mental health presentation which is either underpinned or affected by physical diagnosis […] and I think therefore that the education should be something that isn’t centred around a module, and it becomes embedded into each of the areas of each of the modules (P08).
Theme 4: “It's all about how you talk to them”: communication, empathy, and relational work
Communication was consistently described as the primary tool by paramedics attending mental health calls. Participants emphasised empathy, kindness, reassurance, an understanding attitude, and rapport-building as central to effective case management, often more influential than clinical interventions and skills. You really have to be a really effective communicator in order to get the best out of that patient and be able to give them the best (P02).
Participants recognised that while some “people skills” develop through experience, structured education and training in communication, human factors, bias awareness, and trauma-informed approaches would be beneficial.
Intergenerational differences were noted, with newer paramedics sometimes perceived as lacking confidence or life experience, and more experienced staff sometimes described as dismissive or “old-school”. For the more old-school paramedics or the paramedics who came through as a tech who didn’t go to university, those questions might not have come as naturally because they haven’t experienced it themselves, and I put myself in this person's shoes whereas forty-year-old paramedics probably couldn’t because it was very different (P05, discussing vignette 2). How you approach anything makes a huge difference and I do think that sometimes, you know, I’ve had colleagues who don’t approach mental health jobs very positively, and they dread going in and, you know, they can be dismissive sometimes of behavioural mental health problems, and I just think that's unfair. I think, that's unfair to the patient and sometimes people can really escalate situations just by not really being very understanding and not listening (P02). At the end of the day, mental health is often something that's quite stigmatised as a job to go to. People, you know, they’re like: ‘urgh, here we go again’ (P04).
Discussion
This is the first study to examine the knowledge gaps, educational needs, and systemic factors shaping frontline ambulance paramedics’ ability to provide mental health care in England. By integrating a national review of pre- and post-registration mental health education and training with qualitative accounts of frontline practice, the study provides a comprehensive picture of how paramedics are prepared for, and experience, mental health work. Taken together, the findings point to a clear misalignment between the demands of frontline paramedic practice and the education, training, and organisational support currently in place. Although paramedics consistently recognised mental health care as a routine and legitimate part of their role, preparation for this work was uneven and poorly standardised across pre-registration and in-service contexts. As a result, mental health care was frequently delivered in conditions of uncertainty and emotional strain, with frontline paramedics relying on interpersonal skills and experiential learning rather than formalised training or evidence-based frameworks.
The review of pre-registration curricula highlighted substantial heterogeneity in how mental health education is structured, delivered, and documented across HEIs in England. While some programmes reported dedicated mental health modules, placements, and high-fidelity simulation, others described mental health content embedded across broader modules. Yet in most institutions, mental health content was difficult or impossible to identify from publicly available information. This limited reporting precludes assessment of the depth of preparation provided to student paramedics and, consequently, the identification of potential gaps and planning of improvements to existing curricula.
Similarly, post-registration training varied widely across ambulance services. Although legislation-related content was commonly reported, other areas, such as children and young people's mental health, older adults’ mental health, LGBTQIA + and addiction-related content were less commonly reported. Mental health training was frequently not mandatory, sometimes delivered only to new starters, or provided on a bi-annual or multi-year refresher cycle. These findings suggest that paramedics’ access to ongoing mental health education depends heavily on geographical location and organisational context, contributing to variability in confidence and practice, thus impacting patient experience.
The lack of a standardised approach to mental health education contrasts with the centrality of mental health work within paramedic practice. Participants’ accounts suggest this manifests as uncertainty, reliance on informal learning, and variability in decision-making. Experience on the job can be both essential and problematic: while experience can foster professional intuition and confidence, it can also reinforce unexamined assumptions or practices developed in the absence of formal guidance or feedback. 39
Across interviews, paramedics described feeling underprepared to manage the complexity of mental health presentations, echoing findings from previous U.K. and international studies, for example.7,13,15,40 The findings from this study add to the existing literature, providing explicit detail on the perceived knowledge gaps among paramedics. Rather than highlighting isolated gaps in factual knowledge, participants’ accounts illustrated limited confidence and a lack of structured frameworks to guide risk assessment and decision-making under pressure during mental health calls. Mental health calls were consistently framed as unpredictable, highly individualised, and lacking clear algorithms that often characterise physical health emergencies. This uncertainty generated fear, defensive practice, and reliance on hospital conveyance, even where participants felt this was not clinically optimal. Importantly, these experiences did not arise from a lack of motivation or interest among participants. Rather, there was widespread recognition that mental health constitutes a substantial proportion of paramedic workload, and a clear desire for improved preparation. The acknowledgement of knowledge gaps, alongside an expressed interest to address them, suggests a workforce that is receptive to change. However, findings from both phases suggest that current pre- and post-registration education does not equip paramedics with the skills required to meet these demands.
In response to the perceived knowledge gaps and needs, participants prioritised practice-relevant support which emphasised the importance of communication, de-escalation, empathy, and relational work, describing these skills as central to effective mental health care. While some viewed such skills as developing naturally through experience, many expressed a desire for structured education addressing communication, human factors, and bias awareness. Participants also highlighted the need for clearer frameworks to support structured assessment, risk assessment, referral decisions, and safety netting. Paramedics described wanting flexible frameworks that acknowledge complexity, uncertainty, and the interplay between physical and mental health. Education that explicitly supports working with uncertainty, avoiding premature conclusions, and taking a holistic biopsychosocial view of presentations was seen as particularly valuable. These findings align with often expressed critiques of paramedic education that emphasise a persistent privileging of biomedical, high-acuity scenarios over the “everyday” complexity of mental health and social care work. 41 As mental health calls and paramedicine continue to evolve,42,43 there is a need to reframe what counts as skilled, valued practice, recognising that managing mental health presentations effectively requires expertise underpinned by knowledge, not simply “people skills”.
Beyond education, the findings suggest that paramedics’ experiences of mental health care are shaped by broader issues of professional identity, organisational priorities, and system-level constraints. Contemporary paramedicine has undergone a significant transition from an occupation primarily associated with emergency transport and resuscitation towards a profession increasingly responsible for managing complex health, mental health, and social care needs in the community.44,45 However, professional identities, educational models, and organisational performance measures have not always evolved at the same pace. 45 Participants’ accounts reflected tensions between traditional conceptions of paramedic expertise, often associated with rapid assessment, urgent intervention, and protocol-driven decision-making, and the relational, time-intensive, and often uncertain nature of mental health care. Similar tensions have been described internationally, where paramedics report that organisational pressures, risk-averse cultures, performance targets, and limited access to alternative care pathways can constrain person-centred decision-making and reinforce conveyance to emergency departments even when this may not represent optimal care.46-48 From this perspective, the knowledge gaps identified in this study should not be viewed solely as individual educational deficits but as manifestations of wider structural and cultural factors that shape how mental health work is valued, supported, and enacted within ambulance services. Addressing these challenges will therefore require system-level responses that extend beyond curriculum reform to include organisational culture change, service redesign, and greater integration between ambulance services and mental health systems.46-48Stigma and bias emerged as additional issues. Participants described both personal and organisational attitudes that frame mental health calls as difficult, risky, or undesirable, sometimes associated with assumptions of violence or complexity. While many participants demonstrated reflexivity and awareness of these biases, their accounts suggest that stigma remains embedded within aspects of paramedic culture. This can be understood through broader sociological theories of stigma, professional culture, and symbolic value. Goffman's seminal work conceptualised stigma as a social process through which particular attributes become devalued, resulting in stereotyping, social distancing, and discriminatory responses. 49 Although participants frequently demonstrated awareness of the need for compassionate and person-centred care, their accounts also revealed enduring assumptions that mental health-related calls are inherently more difficult, risky, time-consuming, or less rewarding than physical health emergencies. Such perceptions may not simply reflect individual prejudice but can be understood as products of organisational and professional cultures. Drawing on Bourdieu's concepts of field, habitus, and symbolic capital, 50 paramedic practice can be viewed as a professional field in which certain forms of knowledge and expertise are afforded greater status than others. Historically, technical proficiency, rapid decision-making, and the management of acute physical illness and trauma have been highly valued within ambulance services, contributing to professional identities grounded in emergency intervention and rescue.45,51
In contrast, the relational, communicative, and often uncertain work associated with mental health care may possess less symbolic capital, despite representing a substantial and growing proportion of contemporary practice. Consequently, mental health work risks being positioned as peripheral to the “core” business of paramedicine, reinforcing negative attitudes and limiting opportunities for skill development. From this perspective, educational interventions alone are unlikely to eliminate stigma unless accompanied by broader cultural change that explicitly recognises mental health care as a legitimate domain of paramedic expertise and professional practice. Efforts to increase service-user involvement, reflective practice, and exposure to positive mental health care experiences may help challenge entrenched assumptions and reshape the professional values attached to mental health work.13,18,52
Strengths and limitations
This study integrates England wide review data with in-depth qualitative accounts, providing, for the first time, a comprehensive picture of mental health education and practice in paramedicine. In Phase 2, we ensured methodological quality following Braun and Clarke's 6-step process for data analysis, 35 reporting our research in accordance with the GRAMMS 24 and RTARG, 25 and adhering to the four criteria for trustworthiness outlined by Lincoln and Guba. 37 The use of case-based vignettes enabled exploration of real-world decision-making in case management, 30 while PPI involvement throughout the study enhanced relevance, sensitivity, and interpretive depth. 53
However, limitations should be acknowledged. Phase 1 was constrained by variable response rates from PLs and ambulance services, heterogeneity in publicly available curriculum data, and the absence of a mental health lead in one ambulance service. Phase 2 participants were geographically and professionally diverse but lacked ethnic diversity, reflecting broader workforce demographics. 54 Furthermore, not all ambulance services in England were represented in our sample. As with all qualitative research, findings are not intended to be statistically generalisable, though they offer transferable insights relevant to similar contexts. 35
Implications for education, practice, and policy
The variation identified in pre-registration and post-registration mental health education has important implications for professional standardisation and equity of care. As paramedics assume an increasingly central role in responding to mental health crises, variation in educational preparation risks creating inconsistencies in assessment, decision-making, referral practices, and patient experience across geographical regions and organisations. While professional regulation establishes broad standards of proficiency for paramedics, the findings suggest local variation in how mental health knowledge and skills are developed and maintained. 55 This raises questions regarding whether current educational and workforce structures adequately support a consistent national standard of mental health care. From a patient perspective, inequitable access to appropriately trained practitioners may contribute to variation in care quality, particularly for populations already experiencing health inequalities, including children and young people, older adults, LGBTQIA + individuals, and people with co-existing substance use or social vulnerabilities.56,57
Future policy and workforce development initiatives should therefore consider the establishment of more explicit national expectations for mental health education across the paramedic career continuum. Such approaches may include greater curriculum transparency, nationally agreed core mental health competencies, standardised CPD requirements, and strengthened collaboration between ambulance services, higher education institutions, mental health providers, and people with lived experience. Improving consistency in preparation has the potential not only to strengthen professional confidence and capability but also to reduce unwarranted variation in practice and promote more equitable, person-centred mental health care regardless of where patients access ambulance services.55-58Participants articulated practical suggestions for improvement. These included scenario-based training, joint working with mental health teams, access to specialist advice, and clearer referral pathways. These suggestions reflect a desire for support that enhances real-world decision-making rather than adding to cognitive or administrative burden. Further investment in specialist roles, such as mental health paramedics or dedicated mental health response vehicles, may also offer opportunities to support frontline staff and improve patient care, though further evaluation is needed.
Future directions
Future research should examine the impact of educational interventions on paramedic confidence and knowledge in managing mental health cases, decision-making, and patient outcomes, and explore how standardised mental health training could be implemented across diverse organisational contexts. Greater attention to cultural competence and the experiences of minoritised groups, both within the workforce and among patients, is also warranted. 54
Conclusion
Overall, the study demonstrates a profound gap between what paramedics are expected to manage and how they are prepared to do so. Mental health presentations are routine within contemporary ambulance work, yet education and training provision remains variable, fragmented, and insufficient to meet this. Consequently, paramedics are required to navigate complex mental health situations with limited formal preparation, substantial emotional burden, and heavy reliance on informal learning, personal experience, and communication skills rather than structured, system-supported approaches. Structural and system-level barriers need to be addressed and opportunities for further education and training in foundational clinical knowledge, decision-making skills, and system literacy, developed to strengthen paramedics’ confidence and capacity to provide best practice mental health care.
Supplemental Material
sj-docx-1-pam-10.1177_27536386261467717 - Supplemental material for Paramedics’ management of people experiencing mental health issues: An investigation of knowledge gaps and support needs in England
Supplemental material, sj-docx-1-pam-10.1177_27536386261467717 for Paramedics’ management of people experiencing mental health issues: An investigation of knowledge gaps and support needs in England by Francesca Zecchinato, Ursula Rolfe, Helen Sloan and Natasha Campling in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386261467717 - Supplemental material for Paramedics’ management of people experiencing mental health issues: An investigation of knowledge gaps and support needs in England
Supplemental material, sj-docx-2-pam-10.1177_27536386261467717 for Paramedics’ management of people experiencing mental health issues: An investigation of knowledge gaps and support needs in England by Francesca Zecchinato, Ursula Rolfe, Helen Sloan and Natasha Campling in Paramedicine
Footnotes
Acknowledgements
We would like to acknowledge the members of our Patient and Public Involvement and Engagement (PPIE) advisory group. We would also like to thank the study participants for their time and contribution.
Ethical considerations
Ethical approval was granted by the University of Southampton Faculty of Environmental and Life Sciences Ethics Committee (ERGO ID: 103415).
Consent to participate
Participants provided informed written consent before participating in this study.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration Wessex (ARC Wessex). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Study participants consented to the data being used for the sole purpose of this study and not to sharing for secondary analysis purposes. Data not available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.