
Abstract
Introduction
Drug shortages in Latin America represent a widespread and persistent challenge, with a high proportion of hospitals reporting frequent supply disruptions that affect treatment continuity and quality of care.
Methodology
A cross-sectional study was conducted using a structured survey applied in 144 hospitals across eight Latin American countries between January and April 2025. A non-probabilistic snowball sampling strategy was used to recruit pharmaceutical professionals and personnel responsible for drug procurement. The questionnaire was developed by the research team and reviewed by a panel of hospital pharmacists to ensure content validity. Data were collected anonymously and are based on self-reported perceptions from professionals representing their institutions. Descriptive analyses and exploratory chi-square tests were performed.
Results
75.0% of the responses came from South America, 20.8% from Mexico and 4.2% from Costa Rica. 75.7% of hospitals reported shortages as a serious problem, with a daily frequency in 30.6% and weekly frequency in 27.8% of cases. The most affected categories were antimicrobial, cardiovascular and oncological. Among the most relevant causes were inefficient procurement processes (84.3% in Argentina; 66.7% in Uruguay and Costa Rica), high prices, supply chain disruptions and global shortages of active ingredients. 53.7% of the hospitals had contingency plans, the presence of which was significantly associated with a lower frequency of shortages (p=0.025). The most commonly used strategies were therapeutic substitution (85–90%), inter-institutional collaboration, and the development of alternative formulations (95.5% in Colombia and 75% in Brazil).
Conclusions
Shortage of drugs in the region are a multifactorial phenomenon with a relevant clinical and organizational impact. The implementation of contingency plans and inter-institutional cooperation strategies is associated with improved response capacity, understood as a reduced frequency and better management of shortage events. These findings highlight the need to strengthen contingency planning and promote coordinated regional policies based on the observed variability in causes and mitigation strategies.
Plain language summary
Medicine shortages are a growing problem that affects many hospitals in Latin America. When essential medicines are not available, patients’ treatments can be delayed or interrupted, leading to health complications and stress for both patients and healthcare workers. This study collected information from 144 hospitals in eight Latin American countries, where pharmacists and hospital managers answered a survey about how often medicine shortages occur, what causes them, and what strategies are used to manage them. Most hospitals (about three out of four) reported that shortages are a serious problem. In many cases, the lack of medicines happens every day or every week. The most affected drugs include antibiotics, cardiovascular medicines, and cancer treatments. The main causes of shortages are inefficient purchasing processes, high prices, problems in the global supply chain, and difficulties obtaining active ingredients used to make medicines. More than half of the hospitals have created contingency plans to deal with shortages, and these plans were linked to fewer problems of medicine supply. The most common actions include using therapeutic alternatives, sharing medicines between hospitals, and preparing customized formulations when needed. These results show that medicine shortages are a complex issue with serious consequences for patient care. However, hospitals that plan ahead and cooperate with others can reduce the impact. Stronger regional policies and better coordination between countries are needed to ensure that patients across Latin America always have access to the medicines they need.
Introduction
Drug shortages are a global and persistent problem, with hundreds of active shortages reported annually in several countries, affecting both high- and low-resource health systems. Medicines are a fundamental pillar in medical care, being essential for the management of chronic diseases, emergency care, infection control and the provision of basic health services. When certain drugs are no longer available in health centers, the consequences can be serious, compromising the continuity of treatments, increasing the incidence of therapeutic errors due to the inappropriate use of alternatives and putting the health of thousands of people at risk.1,2
Despite policy initiatives and limited supply-chain improvement (stronger inventory controls and regional procurement pilots), shortages remain a recurring problem affecting both developed countries and those with more limited economies. Latin America is no exception. The region faces challenges due to factors such as dependence on imports, supply chain problems, economic crises and heterogeneous regulations among different countries. In addition, the financial impact is substantial. In low- and middle-income countries, medicines may account for a large share of total health spending. Shortages add further costs, either from purchasing at higher prices or from treating complications due to lack of access.1,3
The interruption of drug supply affects both the availability and affordability of essential and high-cost drugs and worsens outcomes in patients with specific conditions such as autoimmune diseases, mainly due to limited access to biosimilars and significant variability in prices. In countries such as Venezuela, the socioeconomic crisis has generated a drastic decrease in the availability of medicines, supplies and vaccines, affecting health indicators and access to basic treatments.4,5
Frequent antiretroviral shortages compromise treatment continuity in HIV patients, increasing disease progression and transmission risks. Similarly, the increase in maternal and infant mortality, as well as the resurgence of vaccine-preventable diseases, such as measles and diphtheria in Venezuela, show that the shortage of essential medicines and biologics not only compromises individual care, but also generates serious setbacks in public health indicators and in the achievements made in the control of communicable diseases in the region. 6
While there are numerous reports of drug shortages in high-income countries, such as the United States, evidence from hospital-based studies in these settings shows that shortages remain recurrent and operationally demanding. For example, longitudinal analyses in tertiary hospitals have reported repeated shortages over several years, with peaks during the COVID-19 pandemic and significant time and resource requirements for their management. However, information on this problem in low- and middle-income nations remains limited. 2
The present study aims to descriptively assess the perception, impact, and management strategies of drug shortages in selected Latin American countries. It explores the perception and experience of drug shortages in these countries, the mechanisms that have been implemented to manage crises, and the prevention strategies that could be adopted to mitigate its impact. Understanding the situation in Latin America helps make the problem visible but can also identify areas for improvement in the management of the supply of medicines and contribute to the formulation of more effective public policies to guarantee equitable access to essential treatments.
Methodology
This study was based on a cross-sectional and descriptive survey aimed at pharmaceutical professionals and personnel in charge of drug purchases in hospitals in Latin America, with the aim of evaluating the perception of drug shortages, their impact, and mitigation strategies in the region.
The information for this study was obtained from 144 participating hospitals located in eight Latin American countries: Argentina, Brazil, Chile, Colombia, Uruguay, Venezuela, Mexico and Costa Rica. The selection of participants was not direct, but the survey was initially sent via email to contacts in several countries in the region, who then shared the form within their respective professional networks. Selection criteria included (1) active professional role in hospital pharmacy or drug procurement, (2) institutional affiliation with a participating hospital, and (3) voluntary willingness to participate.
Given the exploratory nature of the study and the absence of a complete sampling frame of hospitals and pharmaceutical professionals in Latin America, a formal statistical sample size calculation was not performed. The survey included all participants who responded voluntarily, resulting in a total of 144 hospitals across eight countries. Due to the snowball sampling strategy and indirect distribution of the survey, it was not possible to determine the response rate. This approach is consistent with exploratory surveys, where the primary objective is to obtain diverse perspectives and generate preliminary insights rather than achieve statistical representativeness.
Participants answered the survey voluntarily and anonymously.
Data collection instrument
A structured questionnaire was designed in Microsoft Forms in Spanish, composed of closed and multiple-choice questions, and was available online from January to April 2025. The survey remained continuously open during this period, and periodic reminders were sent through professional networks to increase participation. The questionnaire was specifically developed for this study based on a review of the relevant literature and the research objectives, aiming to capture key aspects related to drug shortages and pharmaceutical supply management in the Latin American context.
The instrument was reviewed by a panel of 4 experts with experience in pharmaceutical services and drug supply management. The experts were selected based on their professional background and evaluated the questionnaire in terms of clarity, relevance, and content adequacy. Feedback was incorporated through an iterative process until consensus was reached, ensuring content validity.
A formal pilot test was not conducted prior to the study, and no formal reliability assessment (e.g., Cronbach’s alpha or test–retest analysis) was performed. This decision was based on the exploratory nature of the study and the absence of a previously validated, standardized instrument specifically designed to assess drug shortages and mitigation strategies in the Latin American hospital context.
The questionnaire was developed de novo by the research team, guided by the study objectives and informed by a review of the available literature on drug shortages. Given the heterogeneity of healthcare systems and supply chain structures across Latin America, existing instruments from other regions were not directly applicable without substantial adaptation.
Instead of formal psychometric validation, content validity was prioritized through expert review by a panel of hospital pharmacists with experience in pharmaceutical services and drug supply management. The iterative consensus process ensured clarity, relevance, and contextual appropriateness of the questions.
While consistent with the exploratory design, the absence of pilot testing and reliability assessment may limit the formal evaluation of internal consistency and reproducibility.
Furthermore, the questionnaire was not designed as a psychometric scale intended to measure a single latent construct, but rather as a descriptive instrument covering multiple independent domains related to drug shortages. Consequently, internal consistency measures such as Cronbach’s alpha were not considered appropriate, as the items were not expected to be internally correlated. Test–retest reliability was also not feasible within the study design, as the survey was administered only once and participants were not re-contacted following data collection.
The questionnaire was originally developed and administered in Spanish, as it was the primary language of the target population. Therefore, no translation was required during data collection. For manuscript preparation, selected responses were translated into English by bilingual professionals, ensuring semantic accuracy and preservation of the original meaning.
The survey covered the following aspects: demographic and employment characteristics, perception of the frequency and severity of drug shortages, impact on medical care and clinical outcomes, existence and effectiveness of institutional protocols, mitigation strategies, and evaluation of national shortage notification systems.
Data analysis
Descriptive statistics, including frequencies and percentages, were calculated. An exploratory chi-square test was performed to assess the association between the presence of contingency plans and the frequency of drug shortages. A significance level of p < 0.05 was established. This inferential analysis was exploratory in nature and was not intended to establish causal relationships.
Although Microsoft Excel has limitations for advanced statistical procedures, it was considered appropriate for the scope of this study, which primarily involved descriptive analyses and a limited number of inferential tests (chi-square), without complex modeling or multivariate analysis.
Ethical consideration
This study was considered exempt from formal ethical review as it involved an anonymous, voluntary survey of healthcare professionals and did not collect patient data or identifiable personal information. This approach is consistent with international ethical standards for research involving human participants. Participation was voluntary, and all responses were collected anonymously.
Results
Geographical distribution of the responses obtained in the survey.
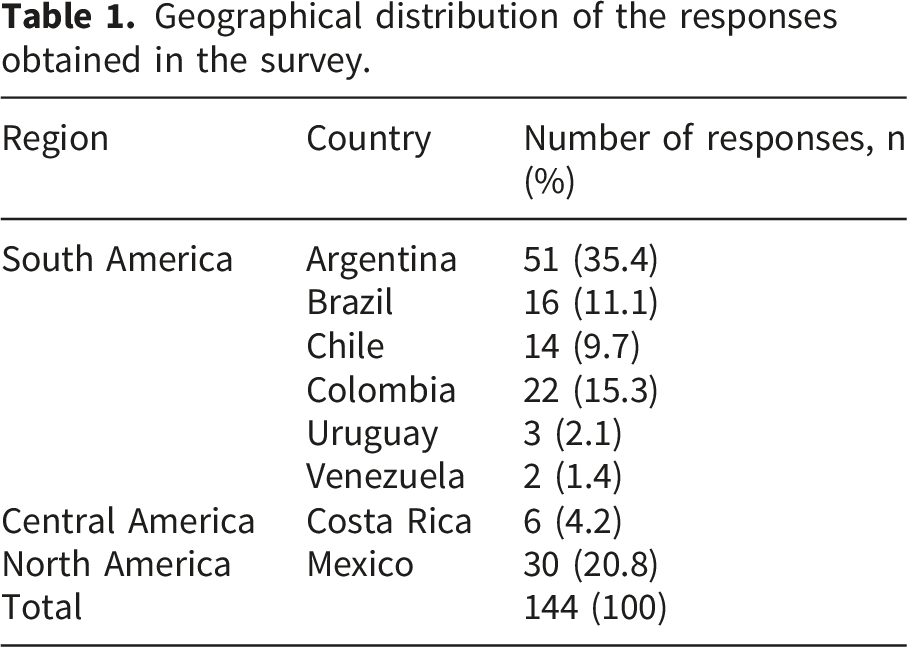
To better understand the variability in drug shortage and the strategies used for its management, a country analysis of the hospitals participating in the study was carried out through the surveyed professionals. This analysis examined key aspects such as how often shortages occur, the implementation of contingency plans, and the strategies adopted to mitigate its impact. In addition, the main causes reported by hospitals were identified based on their geographical location.
Since the structure and organization of hospitals can influence the way they manage drug shortages, a comparative analysis between public and private hospitals was carried out. Aspects such as the drug procurement process, the implementation of contingency plans, the existence of shortage registration systems, and the availability of critical drug lists were evaluated. In addition, the strategies used to mitigate shortages in both types of institutions were analyzed.
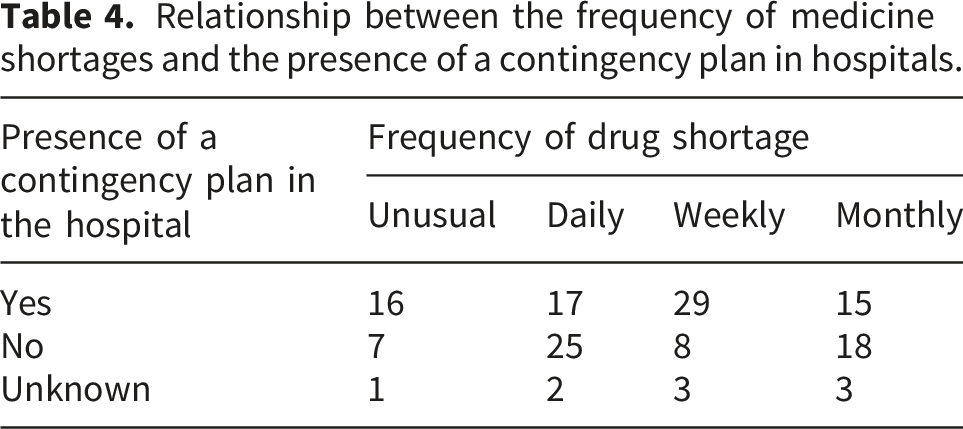
The presence of a contingency plan in hospitals can influence how often they experience shortages of medicines. To evaluate this relationship, the frequency of shortages reported in hospitals that have a contingency plan was compared with those that do not have one or whose implementation is unknown. The results allow us to identify potential benefits of having structured strategies to manage drug shortage.
The statistical analysis shows a significant relationship (p = 0.025) between the presence of a contingency plan and the frequency of drug shortages in the hospitals participating in the study. It is observed that hospitals without a contingency plan report daily and monthly shortages more frequently, while those with a plan have more cases of weekly or unusual shortages.
Regarding the type of health establishment, the distribution of the hospitals participating in the study shows a slight inclination towards public hospitals, which represent 80 of the 144 respondents (55.6%), compared to the 64 private hospitals that responded to the survey, equivalent to 45.14% of the total. Likewise, of the 144 hospitals in Latin America, 73 (50.7%) indicated that they had a system that allows recording and quantifying the drug shortage, including the number of affected stock keeping units (SKUs), while 71 hospitals (49.3%) indicated that they did not have a system of this type. Future studies should compare these perceptions with official health statistics to validate whether reported shortages align with national indicators.
Of the 144 survey responses, 118 (81.9%) reported having a variety of brands for the same active ingredient and pharmaceutical form, which allows them to mitigate the shortage of certain products and offer therapeutic alternatives to doctors to adjust prescriptions and ensure continuity of treatment. This likely reflects stock diversification policies to mitigate shortage risks rather than routine access to lower prices. However, 75.7% of the results (109 hospitals) consider that the lack of medicines currently represents a serious problem in their health centers. In contrast, 22.9% (33 hospitals) indicated that they do not perceive this situation as a significant problem, while the remaining 1.4% (2 hospitals) could not define whether the shortage constitutes a problem in their institution.
Regarding the frequency with which drug shortages occur, 44 hospitals (30.6%) reported that they face this problem daily in their health centers, while 40 hospitals (27.8%) indicated that it occurs weekly. On the other hand, 36 hospitals (25%) indicated that shortages occur monthly, and the remaining 24 hospitals (16.7%) mentioned that this problem is rare in their institutions. Table 5 details the pharmacological categories with the highest incidence of shortages in the health centers participating in the study.
Many health centres have a list of medicines considered “critical”, the availability of which must be always guaranteed. In this study, 91 hospitals (63.2%) reported having one of these lists, while 37 (25.7%) indicated that they did not have one. In addition, 16 hospitals responded to the survey (11.8%) stated that they did not know if their institution had a list of critical medicines.
In relation to the drug procurement process, most of the hospitals participating in the study are not dependent on a centralized system at the national level but rather use a decentralized or mixed system. The details of this process are presented in Figure 1. Distribution of the type of drug procurement process in the hospitals participating in the study.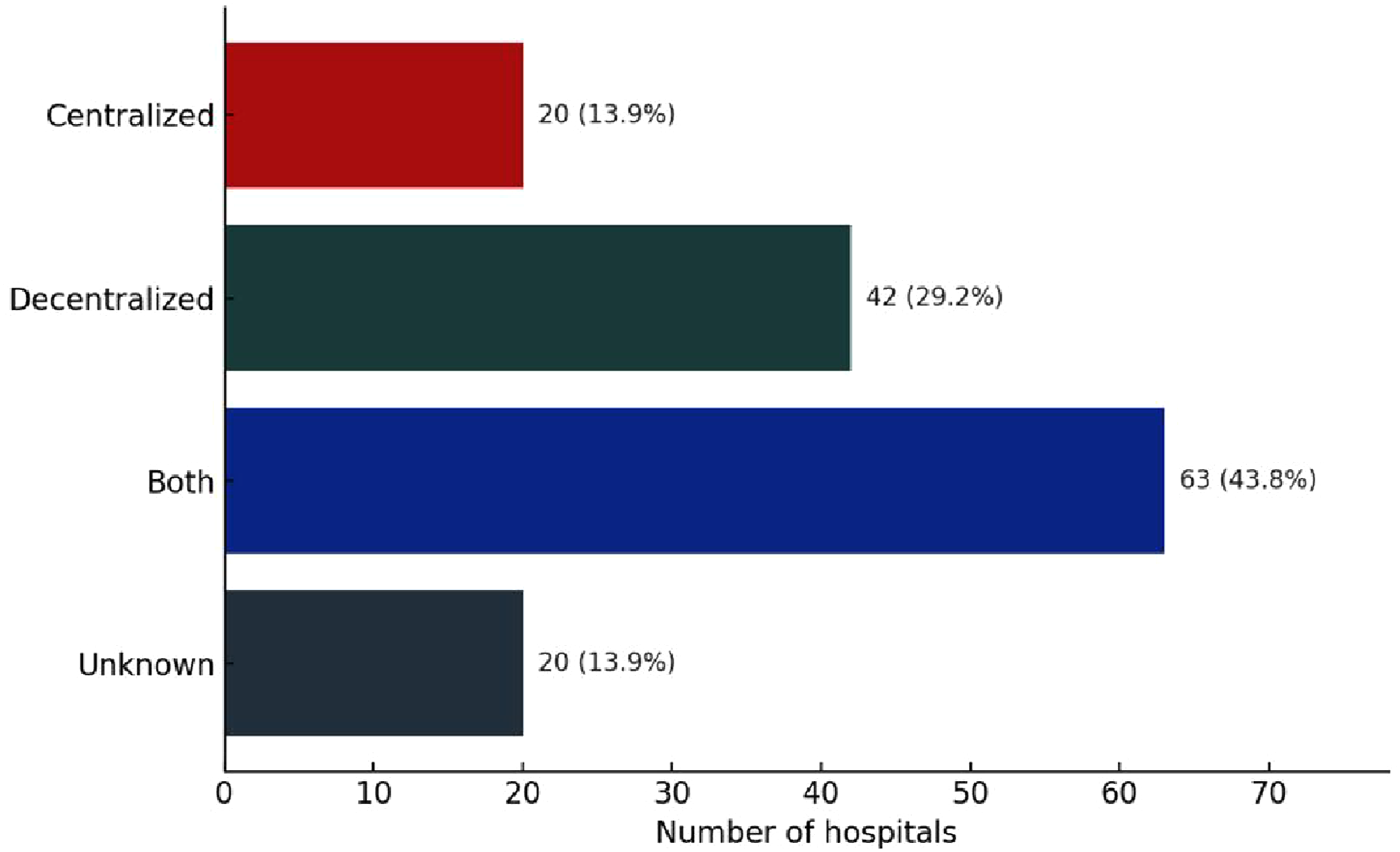
Health professionals have identified various problems associated with the shortage of drugs in the hospitals where they work. The main impact reported is the delay in the therapy or treatment of patients, followed by their dissatisfaction with not being able to access the necessary medicines in health centers. Figure 2 presents in detail the main effects of the drug shortage in the region. Main impacts of drug shortages in hospitals participating in the Latin American study.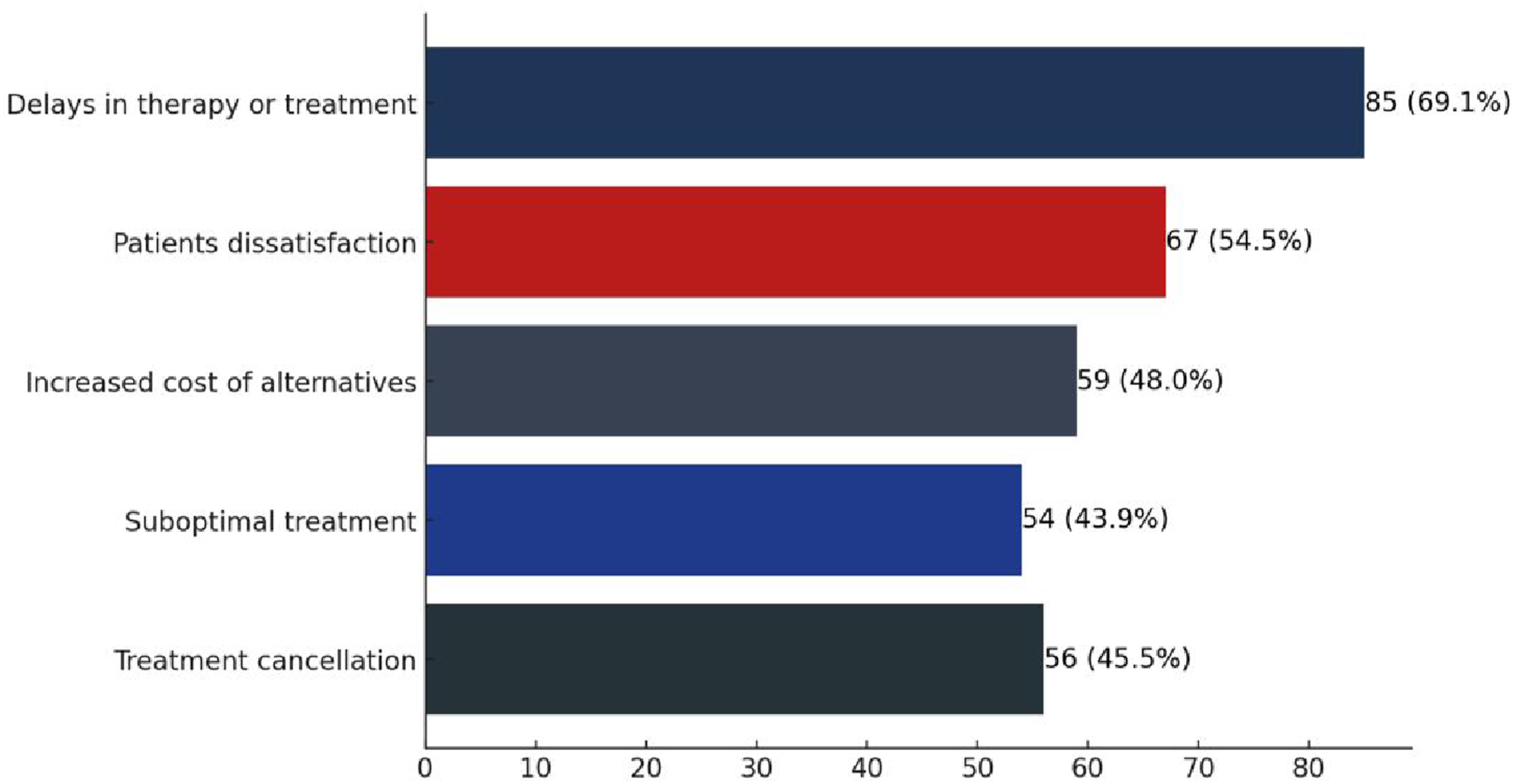
Overall, 77 of 144 hospitals (53.5%) reported having a contingency plan to manage shortages. Hospitals having contingency plans to mitigate drug shortages commonly employ therapeutic substitution and cross-institutional collaboration (Figure 3). However, despite these measures, 43.1% of hospitals have reported significant clinical consequences derived from this problem. Among the main effects are the aggravation of patients’ conditions and an increase in the rate of hospital readmissions. In addition, difficulties in accessing treatments have compromised the continuity of medical care, prolonging recovery times and generating a greater care burden for health centers. Strategies implemented by hospitals to mitigate drug shortages.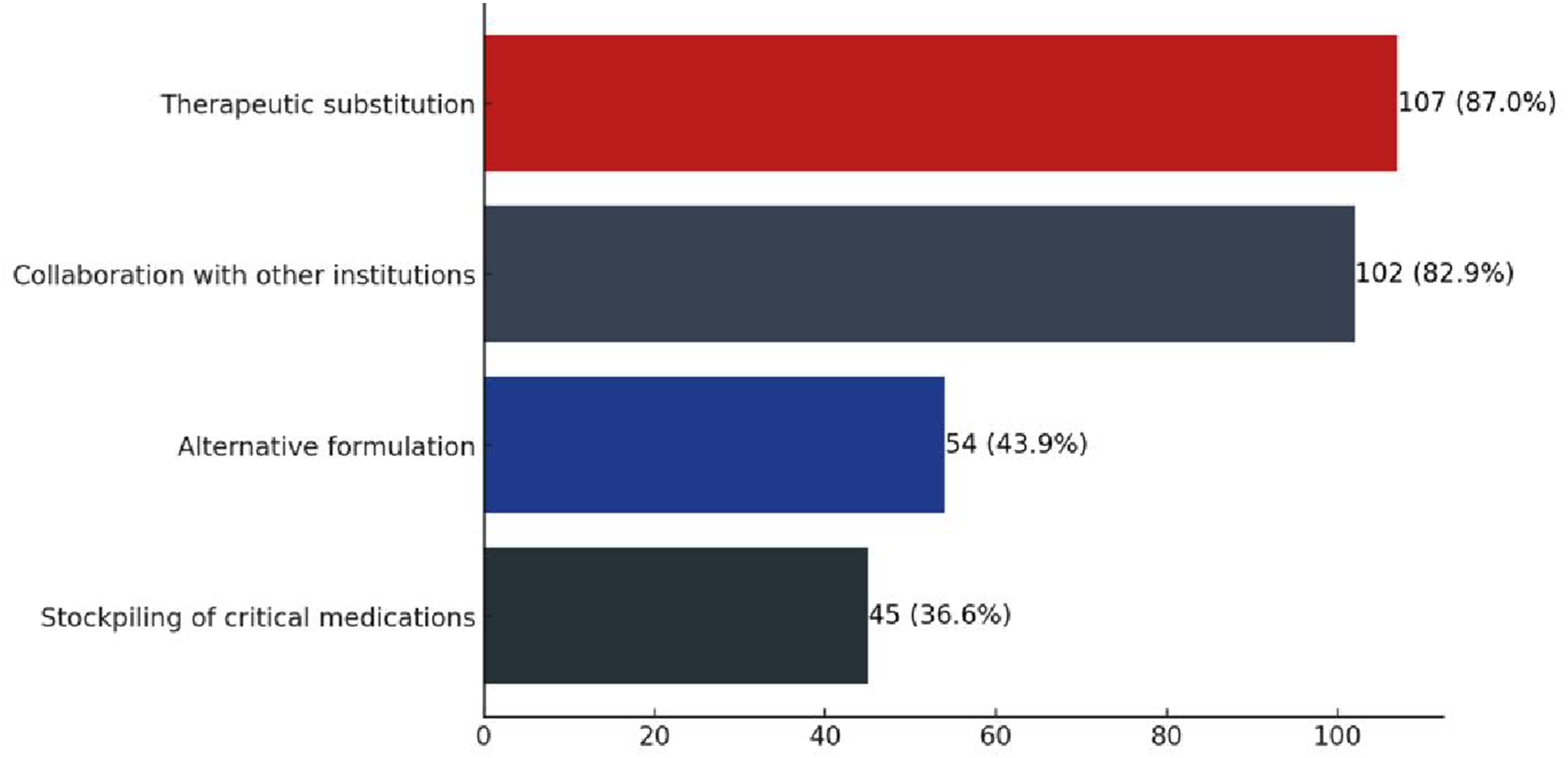
One of the communication strategies within the health center is to inform the rest of the members of the health team about the shortage of a medication, either through internal meetings or via institutional email. The details of the means of communication used by each of the hospitals that participated in the study can be found in Table A2 in the annexes section.
Discussion
The drug shortage in Latin America profoundly impacts regional public health, affecting patients directly and health systems through delays, interruptions, or omissions in treatments. This can translate into worsening of diseases, increased morbidity and mortality, and the occurrence of adverse events when therapeutic alternatives that may be less effective are used (Figure 2).7–9
According to Oldfield et al. (2025), 10 originator brand medicines in the private sector display high median price ratios relative to international reference prices (≈16.5–52.9), while the lowest-priced generics range from ≈3.0 to 11.5. These figures refer to private-sector patient prices and may differ from institutional procurement prices.
Parameters measured in the survey according to participating country.

Note. Percentages were calculated based on the total number of responses per country (shown in the first row), unless otherwise specified.
Pharmaceutical professionals also pointed to global shortages of active ingredients (APIs) and manufacturing problems as relevant causes, particularly in Brazil, Chile and Colombia, reflecting the region’s heavy dependence on global production chains concentrated in a few countries. This pattern shows a structural vulnerability: any international disruption has an immediate impact on local supply. Likewise, supply chain disruption was identified as a key factor in Colombia (63.6%) and Uruguay (100%), highlighting the logistical fragility and lack of resilience in distribution systems.
According to the results presented in Table 2, Chile (42.9%) and Colombia (45.4%) reported regulatory barriers as one of the main causes of shortages, reflecting the difficulty of regulatory systems in balancing health security with the need for timely access to medicines. In many cases, these restrictions delay the introduction of new drugs and, paradoxically, perpetuate dependence on external markets. 11 Our findings provide multicenter data from eight Latin American countries, which shows regional differences in causes and strategies. These results provide one of the few multicountry perspectives on drug shortages in Latin America, complementing previous studies mostly focused on high-income countries. Overall, these findings underscore the structural vulnerabilities of Latin American health systems and the urgent need for coordinated responses.
Another aspect identified was the increase in the demand for specific medicines, particularly in Costa Rica (83.3%), where particular epidemiological situations can overload health systems that already operate with limited supply margins. In contrast, parallel exports were reported less frequently, suggesting that shortages in Latin America are due more to domestic deficiencies than to external market pressures.
Studies carried out in the region show that the average availability of generic medicines ranges between 37.8% and 68.3% in the public sector and between 42.3% and 77.4% in the private sector, remaining below the World Health Organization (WHO) target of at least 80% in both cases. 10 This chronic under-availability contributes directly to recurrent drug shortages, as limited baseline stock levels leave health systems with little capacity to absorb supply disruptions. The situation is even more critical for innovative medicines: although many have been evaluated in clinical trials involving Latin American patients, they are often not registered or marketed in the region, and when available, their high prices, frequently exceeding the monthly minimum wage, further restrict access. Together, these factors create structural conditions that perpetuate medicine shortages and inequitable access to essential treatments. 12
Strategies used
Table 2 analyzes the strategies used by pharmaceutical professionals to deal with drug shortages in different Latin American countries, and Figure 3 shows which strategies are most used by all the participants in the study. In general terms, therapeutic substitution was the most reported measure, reaching figures above 80% in all countries, except for Venezuela, which reflects its role as the first option to guarantee the continuity of treatments. 81.9% of the respondents reported having a variety of brands of the same active ingredient and pharmaceutical form for this purpose. Collaboration with other institutions or providers was also highlighted as a widely used strategy, with percentages above 70% in most countries, suggesting that the articulation between actors in the health system is a key resource in the face of shortages.
The stockpiling of critical medicines, on the other hand, showed a much more heterogeneous adoption. While in Costa Rica (66.7%) it was indicated as a frequent practice, in countries with a higher number of participants such as Brazil (12.5%) and Mexico (22.7%) it was reported in a lower proportion, which may be associated with both differences in logistics capacity and inventory management policies implemented in each national context.
With regard to the Alternative formulations, including magisterial preparations, the results of Colombia (95.4%) and Brazil (75%) stand out, where this strategy was identified as fundamental to make up for the lack of industrial medicines. In countries such as Brazil, in fact, they have been systematically implemented to mitigate therapeutic gaps, particularly in pediatric populations and in the management of neglected diseases, although this practice requires investment and the development of standardized formulations. 13 However, it should be considered that the use of these formulations requires infrastructure and trained human resources, which limits their viability in other countries.
It is important to note that, in countries such as Uruguay (n=3) and Venezuela (n=2), the percentages should be interpreted with caution due to the small sample size, which restricts the generalizability of the findings. Even so, the recurrence of the same strategies in different contexts suggests common patterns in the region, although with variations determined by the technical, regulatory, and logistical capacities of each health system.
Comparison between public and private hospitals
Both private and public hospitals face the same structural problem of shortages, and their answers tend to differ depending on financial resources, administrative capacity, or degree of organizational flexibility. The lack of homogeneity in monitoring systems, the lack of standardization of contingency plans and the excessive reliance on palliative strategies (such as therapeutic substitution) highlight structural gaps that require urgent attention.14,15
Comparison of parameters related to the drug shortage according to type of hospital (private or public).
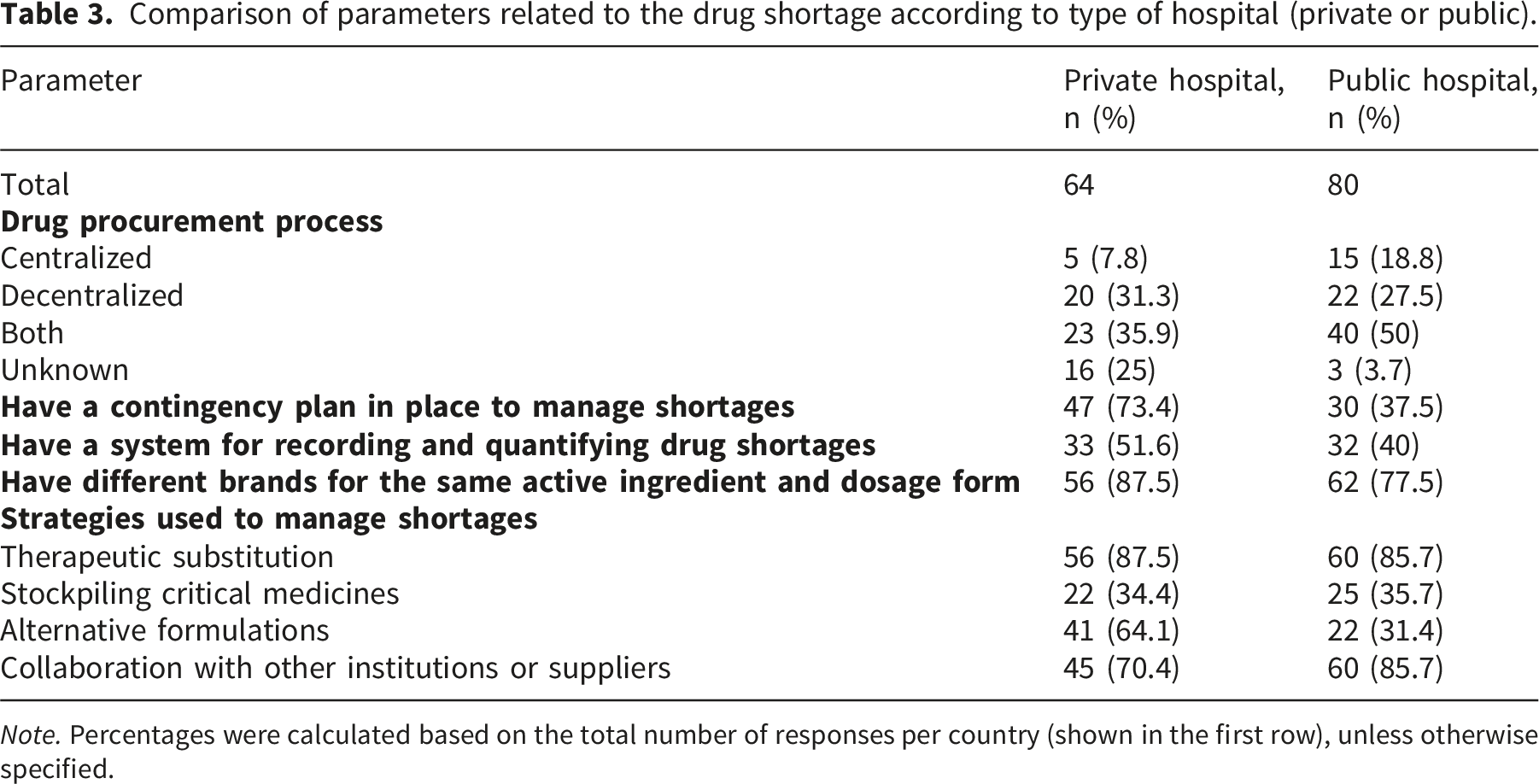
Note. Percentages were calculated based on the total number of responses per country (shown in the first row), unless otherwise specified.
Private hospitals rely more on decentralized (31.3%) or combined systems (35.9%). That gives them greater operational flexibility. The 25% of private respondents who do not know the procurement model suggests that purchasing is handled by non-clinical teams. These are specialized logistics or supply-chain units. They use standardized procedures, closer inventory monitoring, and more agile financing. This setup helps them anticipate and respond faster to drug shortages.
In the public sector, tighter budgets and rigid administrative layers slow risk detection and preventive actions. Figure 1 summarizes the overall distribution of procurement models.
Relationship between the frequency of medicine shortages and the presence of a contingency plan in hospitals.
Hospitals often prepare for possible drug shortages by applying strategies that reduce their impact on patient care. These actions do not prevent shortages but help manage their consequences. The most frequent measures include therapeutic substitution, keeping critical medicines in permanent stock, developing alternative formulations, and cooperating with other hospitals or suppliers to share available resources.
According to the results of the survey, both public and private hospitals mainly resort to therapeutic substitution (85.7% and 87.5%, respectively) and collaboration with other institutions or providers (85.7% in public and 70.4% in private) as strategies to address shortages. Although these measures may be effective in the short term, they also carry clinical risks: substitution can compromise treatment efficacy or patient adherence, while reliance on external collaborative networks can lead to inequities in access to medicines.
Likewise, the use of alternative formulations, such as magisterial preparations, is considered both by public hospitals (31.4%) and to a greater extent by private hospitals (64.1%) as a viable alternative to deal with shortages. The availability of additional resources in the private sector may explain this observed difference, as it facilitates the implementation of more expensive and customized solutions. Finally, the stockpiling of critical medicines, a practice that requires robust inventory planning, with risks of expiry or waste if not properly managed, was observed in similar proportions in both sectors (34–35%).
One aspect in which similarities were observed between public and private hospitals was the presence of a system for recording and quantifying shortages, reported by 51.6% of private hospitals and 40% of public hospitals. The absence of these systems in a considerable proportion of hospitals limits the ability to adequately size the shortage and hinders strategic planning. Although studies with larger samples are required to confirm whether this trend is maintained at the regional level and to clarify whether it responds to structural limitations of health systems or to differences in hospital management, the truth is that the lack of reliable and standardized data prevents the implementation of effective inventory management policies and makes it difficult to generate early warnings that allow anticipating shortages. Prioritizing the distribution of critical medicines and designing evidence-based mitigation strategies.15,16
Main medicines reported with shortages
Pharmacological categories with the highest incidence of drug shortage in the health centers surveyed.
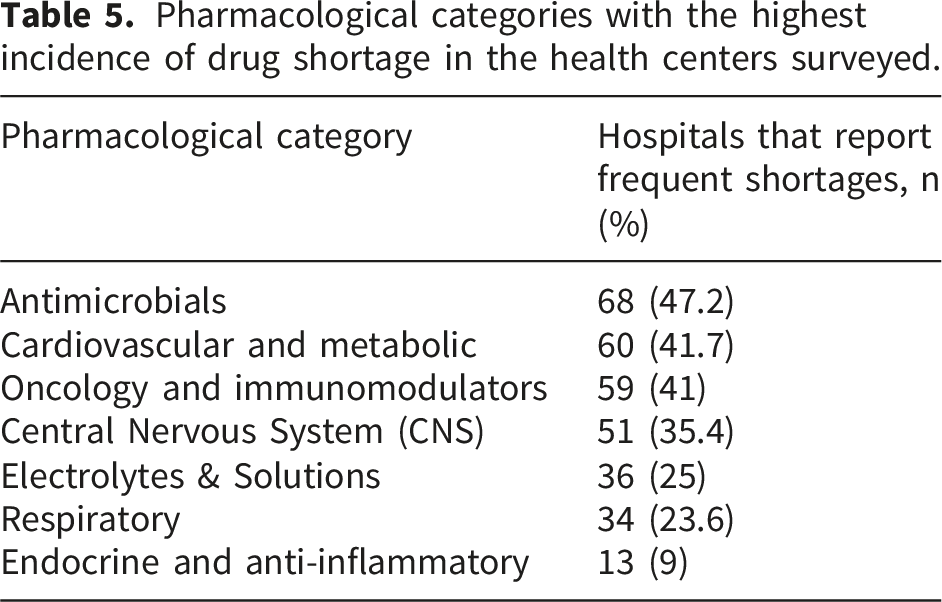
Antimicrobial shortages are currently a persistent and growing global problem. Antibiotics are among the pharmacological classes most affected by supply disruptions (Table A1), with significant clinical and public health consequences.17–19
Manufacturing and quality issues, as well as reliance on active ingredients from single sources, regulatory difficulties, unexpected production disruptions by suppliers, and increased demand are the main reasons for the shortage of this group of drugs. 19
The clinical implications are serious. Delayed administration of appropriate treatments, forced use of broader-spectrum alternatives that increases the risk of antimicrobial resistance, the risk of toxicity and has hampered antimicrobial stewardship programs. 20
However, the shortage of oncology drugs represents a critical and persistent problem, with a direct impact on clinical care and patient safety. Recent studies carried out in the United States document that more than half of cancer centers have experienced shortages in recent months, affecting essential chemotherapy drugs as well as support drugs. This leads to the need to modify therapeutic schemes, the use of alternatives that may be less effective or more toxic, and an increase in medication errors. In addition, stockouts have generated ethical dilemmas in the prioritization of patients and have complicated inclusion and continuity in clinical trials, with implications for equity and quality of treatment.21–23
In the case of cardiovascular drugs, drug shortage is a long-standing phenomenon that does not only affect Latin American countries. The lack of therapeutic alternatives for many cardiovascular agents aggravates the clinical impact, forcing complex and potentially risky adjustments in treatment regimens, which increases the burden of care and the risk of errors, in addition to generating anxiety and stress in both patients and health professionals.24,25
Limitations of the study
This study has several limitations that should be considered when interpreting its findings. First, it is based on a cross-sectional survey with self-reported responses from pharmaceutical professionals and purchasing personnel, which can introduce perception and memory biases. The use of a non-probabilistic snowball sampling approach may introduce selection bias, as participants are more likely to be connected through professional networks. The information obtained is restricted to the perception of health professionals without including objective data from inventories or national registries, which could underestimate or overestimate the true magnitude of the shortage. Furthermore, the absence of pilot testing and formal reliability assessment may affect the robustness and reproducibility of the survey instrument. In particular, while participants were asked to identify causes of drug shortages, they do not work directly in pharmaceutical manufacturing or global supply chains, so their responses reflect perceptions rather than first-hand evidence. These opinions may be influenced by information from suppliers, media, literature, or informal sources, and may not accurately represent the actual dynamics of shortages. In addition, although 144 hospitals from eight countries participated, the distribution was not uniform, with a greater representation of Argentina and a lower representation of countries such as Uruguay and Venezuela, which limits the generalization of the results to the entire region. The design of the study also does not allow establishing causal relationships between the factors identified and the frequency of drug shortage, but only statistical associations. In addition, the analysis did not account for potential confounding variables such as country-specific differences, institutional characteristics, or professional experience. On the other hand, Caribbean countries were not included, nor was the sample stratified according to levels of hospital complexity. Future studies employing randomized and stratified sampling designs are needed to enhance generalizability.
In addition, the questionnaire used in this study was not subjected to formal psychometric validation procedures, such as pilot testing or reliability assessment (e.g., Cronbach’s alpha or test–retest analysis). While content validity was addressed through expert review, the lack of these additional validation steps may limit the formal assessment of reproducibility and internal consistency of the instrument. This limitation is particularly relevant given that the questionnaire was developed specifically for this study and was not adapted from a previously validated tool.
Conclusions
This study showed that drug shortages in Latin America are a frequent problem with significant clinical and organizational impact, reported as serious by three out of four participating hospitals and occurring daily in nearly one-third of them. The most affected categories include antimicrobials, cardiovascular, and oncology drugs, posing substantial risks to treatment continuity and patient safety. The results highlight that inefficient procurement processes, high prices, global shortages of active ingredients, and supply chain disruptions are key drivers of stock-outs.
Given that more than half of hospitals reported having contingency plans and that their presence was associated with a lower frequency of shortage episodes, strengthening the implementation and standardization of these protocols should be prioritized as a key management strategy. Similarly, considering that a considerable proportion of hospitals lack systems for recording and quantifying shortages, the development of national monitoring systems is essential to enable early detection and more efficient allocation of critical medicines.
The widespread use of therapeutic substitution and inter-institutional collaboration as mitigation strategies reflects both the adaptability of healthcare facilities and the reliance on reactive approaches. This underscores the need to complement hospital-level responses with more proactive and coordinated strategies. In this context, drug shortages in Latin America require a comprehensive approach that integrates institutional measures with coordinated regional policies aimed at reducing structural vulnerabilities and ensuring equitable and continuous access to essential treatments. Addressing this challenge will require not only strengthening hospital-level capacities but also advancing regulatory, supply chain, and coordination mechanisms at the system level to improve long-term resilience.
Footnotes
ORCID iDs
Author contributions
E.M-V. made substantial contributions to data interpretation, intellectual content revision, drafting of the manuscript, and final approval of the version to be published. D.A-M., A.M-G., V-T., J.M-V., S.D-N. and C.S-S. contributed to the intellectual content revision and gave final approval of the version to be published. E.Z-M., A.V-M, S.A-C. and R-M. made substantial contributions to the conception, analysis, interpretation, drafting, reviewing, and final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data generated are available in the body of the article.
Appendix
Pharmacological subcategories with the highest incidence of shortages in the health centers surveyed. *The drugs listed are representative examples of each category and are not an exhaustive list.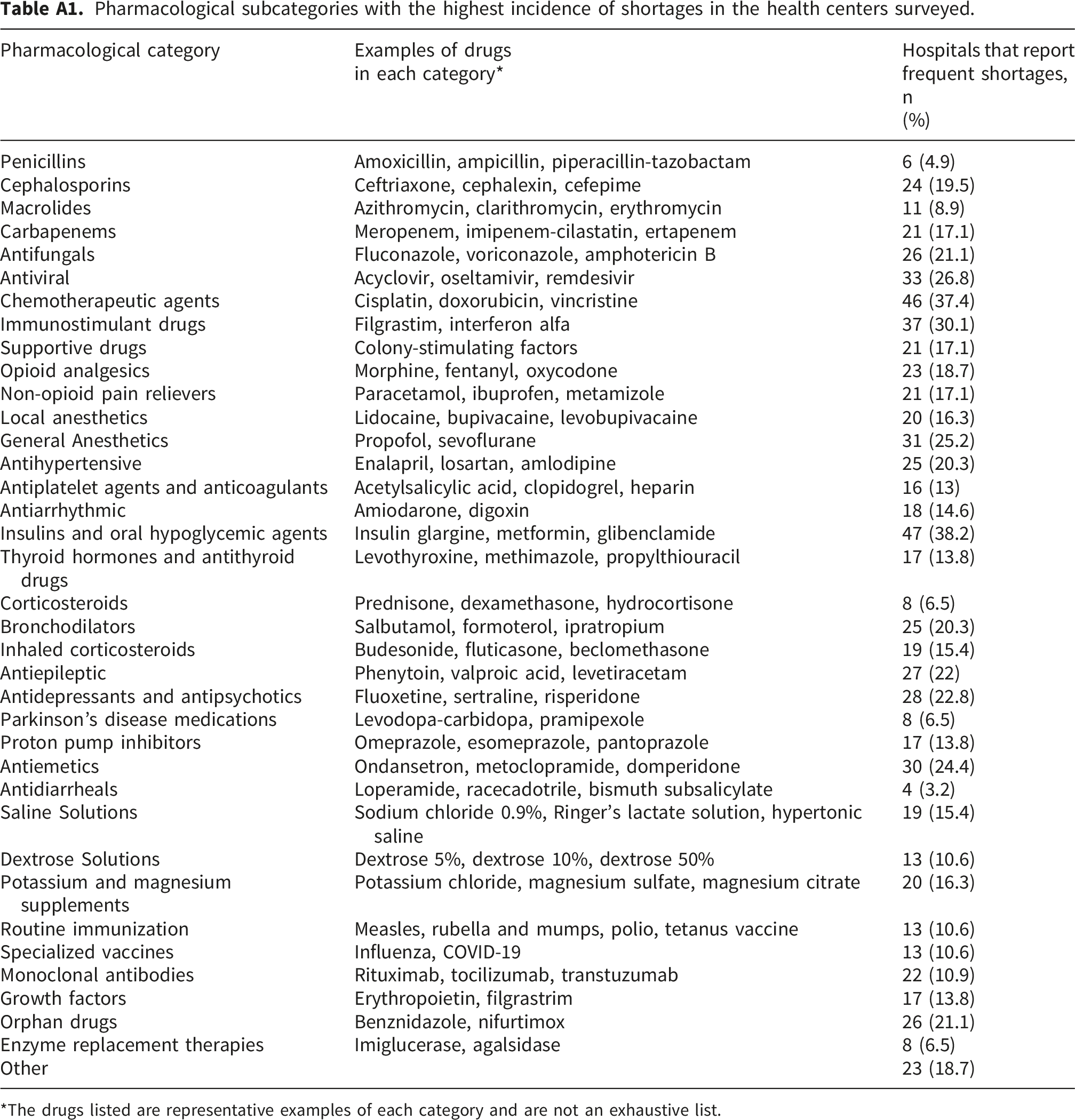
Pharmacological category
Examples of drugs in each category*
Hospitals that report frequent shortages, n (%)
Penicillins
Amoxicillin, ampicillin, piperacillin-tazobactam
6 (4.9)
Cephalosporins
Ceftriaxone, cephalexin, cefepime
24 (19.5)
Macrolides
Azithromycin, clarithromycin, erythromycin
11 (8.9)
Carbapenems
Meropenem, imipenem-cilastatin, ertapenem
21 (17.1)
Antifungals
Fluconazole, voriconazole, amphotericin B
26 (21.1)
Antiviral
Acyclovir, oseltamivir, remdesivir
33 (26.8)
Chemotherapeutic agents
Cisplatin, doxorubicin, vincristine
46 (37.4)
Immunostimulant drugs
Filgrastim, interferon alfa
37 (30.1)
Supportive drugs
Colony-stimulating factors
21 (17.1)
Opioid analgesics
Morphine, fentanyl, oxycodone
23 (18.7)
Non-opioid pain relievers
Paracetamol, ibuprofen, metamizole
21 (17.1)
Local anesthetics
Lidocaine, bupivacaine, levobupivacaine
20 (16.3)
General Anesthetics
Propofol, sevoflurane
31 (25.2)
Antihypertensive
Enalapril, losartan, amlodipine
25 (20.3)
Antiplatelet agents and anticoagulants
Acetylsalicylic acid, clopidogrel, heparin
16 (13)
Antiarrhythmic
Amiodarone, digoxin
18 (14.6)
Insulins and oral hypoglycemic agents
Insulin glargine, metformin, glibenclamide
47 (38.2)
Thyroid hormones and antithyroid drugs
Levothyroxine, methimazole, propylthiouracil
17 (13.8)
Corticosteroids
Prednisone, dexamethasone, hydrocortisone
8 (6.5)
Bronchodilators
Salbutamol, formoterol, ipratropium
25 (20.3)
Inhaled corticosteroids
Budesonide, fluticasone, beclomethasone
19 (15.4)
Antiepileptic
Phenytoin, valproic acid, levetiracetam
27 (22)
Antidepressants and antipsychotics
Fluoxetine, sertraline, risperidone
28 (22.8)
Parkinson’s disease medications
Levodopa-carbidopa, pramipexole
8 (6.5)
Proton pump inhibitors
Omeprazole, esomeprazole, pantoprazole
17 (13.8)
Antiemetics
Ondansetron, metoclopramide, domperidone
30 (24.4)
Antidiarrheals
Loperamide, racecadotrile, bismuth subsalicylate
4 (3.2)
Saline Solutions
Sodium chloride 0.9%, Ringer’s lactate solution, hypertonic saline
19 (15.4)
Dextrose Solutions
Dextrose 5%, dextrose 10%, dextrose 50%
13 (10.6)
Potassium and magnesium supplements
Potassium chloride, magnesium sulfate, magnesium citrate
20 (16.3)
Routine immunization
Measles, rubella and mumps, polio, tetanus vaccine
13 (10.6)
Specialized vaccines
Influenza, COVID-19
13 (10.6)
Monoclonal antibodies
Rituximab, tocilizumab, transtuzumab
22 (10.9)
Growth factors
Erythropoietin, filgrastrim
17 (13.8)
Orphan drugs
Benznidazole, nifurtimox
26 (21.1)
Enzyme replacement therapies
Imiglucerase, agalsidase
8 (6.5)
Other
23 (18.7)
Communication methods and channels used to report drug shortages in hospitals.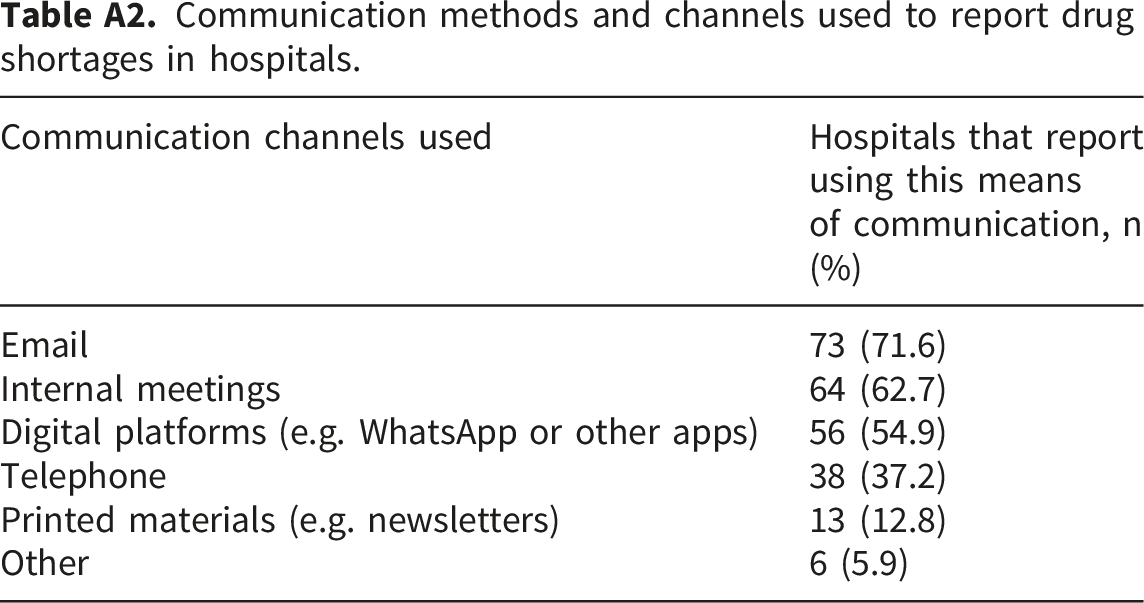
Communication channels used
Hospitals that report using this means of communication, n (%)
Email
73 (71.6)
Internal meetings
64 (62.7)
Digital platforms (e.g. WhatsApp or other apps)
56 (54.9)
Telephone
38 (37.2)
Printed materials (e.g. newsletters)
13 (12.8)
Other
6 (5.9)