
Abstract
In government-controlled media, serving governments’ economic, political, or ideological interests often diverts media health policies from their primary target of promoting public health, making them ineffective. Understanding the growth of this diversion in countries’ political and social contexts over a long period demands a multi-layer historical analysis. Thus, to explore the roots of this diversion in government-controlled media, we examined the development process of health policy making in Iranian mass media. We conducted and analyzed interviews with 21 media experts and health policy makers through causal layered analysis, including litany, system, discourse, and metaphor layers. Results indicate that the “absence of stable management” and “health programs’ low quality” undermined achievements of health policy making, including establishing the Health Policy Council and two health channels. We identified “lack of comprehensive strategy,” “policymakers’ inadequate knowledge,” “insufficient financing,” and “extensive government intervention” as underlying social causes of ineffective health programs. In addition, the Islamic ideological approach to health issues has been revealed as the dominant discourse. Interview data imply that conflicts between modern medicine and Iran's traditional medical knowledge make it difficult for media health policy makers to achieve their strategic aims. This study provides insights into the challenges of health policy making in government-controlled mass media.
Sociocultural and political–economic circumstances affect both media health policies and health outcomes. These effects are, to a large extent, a function of the governance system in any country, including power structure, political control, and influence of various actors.1,2 Being controlled by the government is an important determinant of policymaking in mass media production. 3 The political–ideological motives of those who control or influence mass media often intersect with their interests.4,5 For instance, while mass media are the primary sources of health information and are frequently targeted by policymakers, their health programs are not mainly focused on promoting public health. The diversion toward programs in the interest of owners, especially in government-controlled media, makes mass media health policies ineffective in shaping public opinion toward better health. 6
To explore the roots of this diversion in health policy making, in this study, we investigate the Iranian mass media system as an example of government-controlled mass media. Iranian mass media (national radio and television) has been reformed based on the Islamic Republic's Constitution, which assigned direct control of them to the government. The Islamic Republic of Iran Broadcasting (IRIB), in charge of all television and radio programs, has become the country's most dominant media institution. As shown in Figure 1, 57.7 percent of Iranian people 7 cited IRIB as their main source of information on the country's daily news.
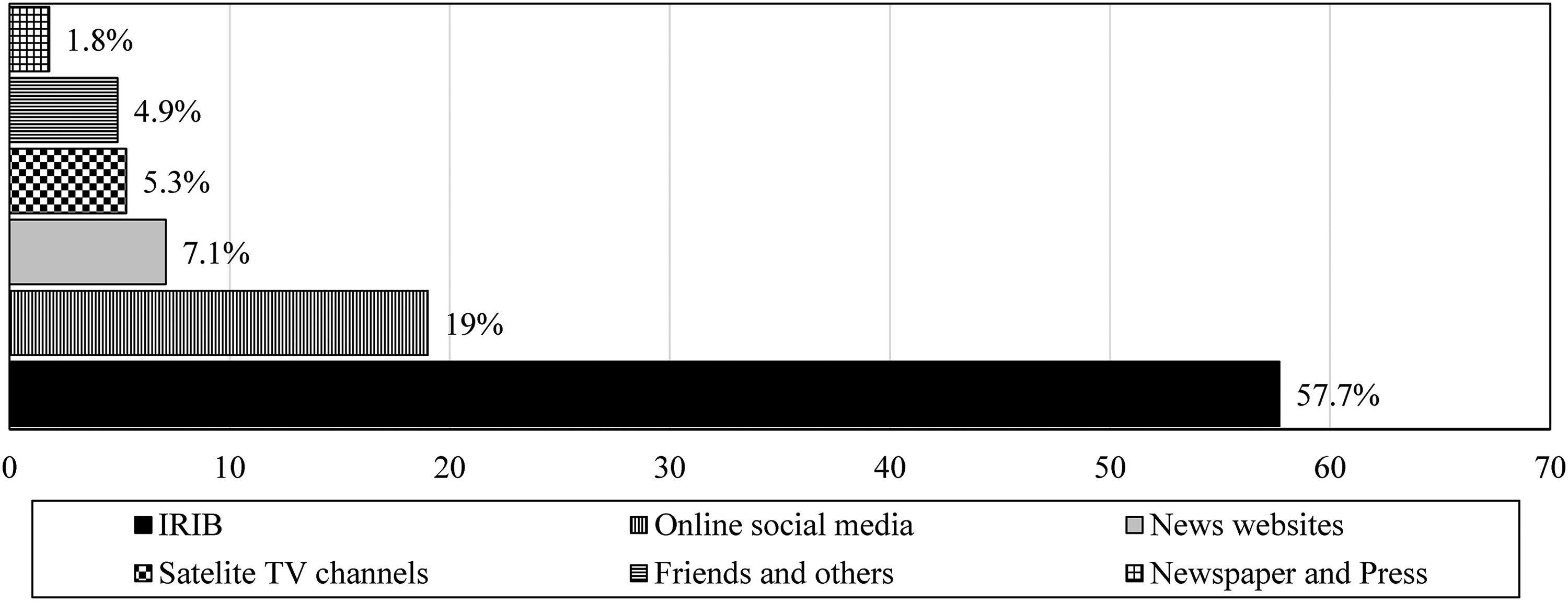
Type of media used by iranians for Daily News. 7
Iranian Government Approach to Media Health Policy
Two general views are discernible in the literature in connection with media policy. One readily accepts the need for media policy 8 and thus the role of government intervention in such policymaking. 9 McQuail 2 favors the means to ensure a level of control over media markets by the government. This line of thinking thus places media policy squarely in the realm of public policy. Iranian media system follows an extreme version of the McQuail approach. The second perspective emphasizes the importance of unofficial processes associated with media policy. This view embarks on devising policies together with laws and regulations to ensure their control over the media, although the extent of this control is country-dependent. 10 In the case of Iranian mass media, Namakdoost Tehrani 11 argues that the Iranian government's interventions in the mass media are often aimed at protecting its interests at the expense of violating people's rights. In this regard, Mohsenian Rad 12 highlights inattention to Iranian society's need for free media in the post-revolutionary period and argues that we should privatize radio and television in Iran.
Although television is the leading media in terms of access to health-related information in Iran,13–15 its dominance has been declining due to increased use of social media, improved health literacy of Iranian audiences, non-attractive educational formats, and limited broadcast schedule.16,17 Furthermore, ideological restrictions imposed by the Iranian government have limited health-related programs about culturally sensitive social issues such as high-risk sexual behaviors to warning messages or clinical advice without discussing preventive measures.18–20 For example, radio and television programs do not discuss the causes of substance abuse.13,21,22 In fact, they provide messages that criminalize addiction while disregarding preventive measures. 23 Likewise, despite the tremendous potential of mass media in addressing HIV/AIDS, the effectiveness of IRIB activities on HIV/AIDS has been questioned.24,25 However, the Iranian government recently issued the General Policies on Health that underscore an urgent need to develop prevention programs. These policies emphasize the role of media, cultural, and educational organizations in raising public awareness, responsiveness, empowerment, and participation in national health objectives. 26
To explore the dimensions of government control on mass media and its impacts on health policy making, in this study, we aim to identify achievements, barriers, underlying social causes, dominant discourses, and metaphors in the health policy making of Iranian mass media, including national radio and TV. To do so, we conducted semi-structured, in-depth interviews with experts in mass media and health policy making in Iran and analyzed interview results through causal layered analysis. Results revealed that program barriers such as low quality hinder the benefits of establishing health channels in Iranian media. Moreover, we identified social causes (e.g., non-scientific strategies, inadequate funding, and extensive government intervention) that could negatively affect the success of media health programs.
Methods
Given the multi-layered nature of health policy making for mass media, this study has relied on the causal layered analysis (CLA) to investigate media health policy in Iran. First adopted by Inayatullah, 26 CLA attempts to deconstruct social issues and events to achieve a deeper understanding. This method provides a more profound knowledge of past and present problems, enabling the development of alternatives for the future. 27 CLA can be adapted to probe a variety of subjects 27 and has been used in health-related studies.28–30
In this study, four layers are treated in CLA. The first layer, dubbed “litany,” poses and addresses superficial questions targeting official and accepted views of reality as well as quantitative trends on the general approaches of the Iranian mass media toward community health. The second layer investigates social causes and systematic perspectives associated with the prevailing situation. The third layer concerns dominant discourses and meanings constructed by the media for health and disease. Finally, the fourth layer analyzes the policies’ myths and metaphors (see Figure 2).
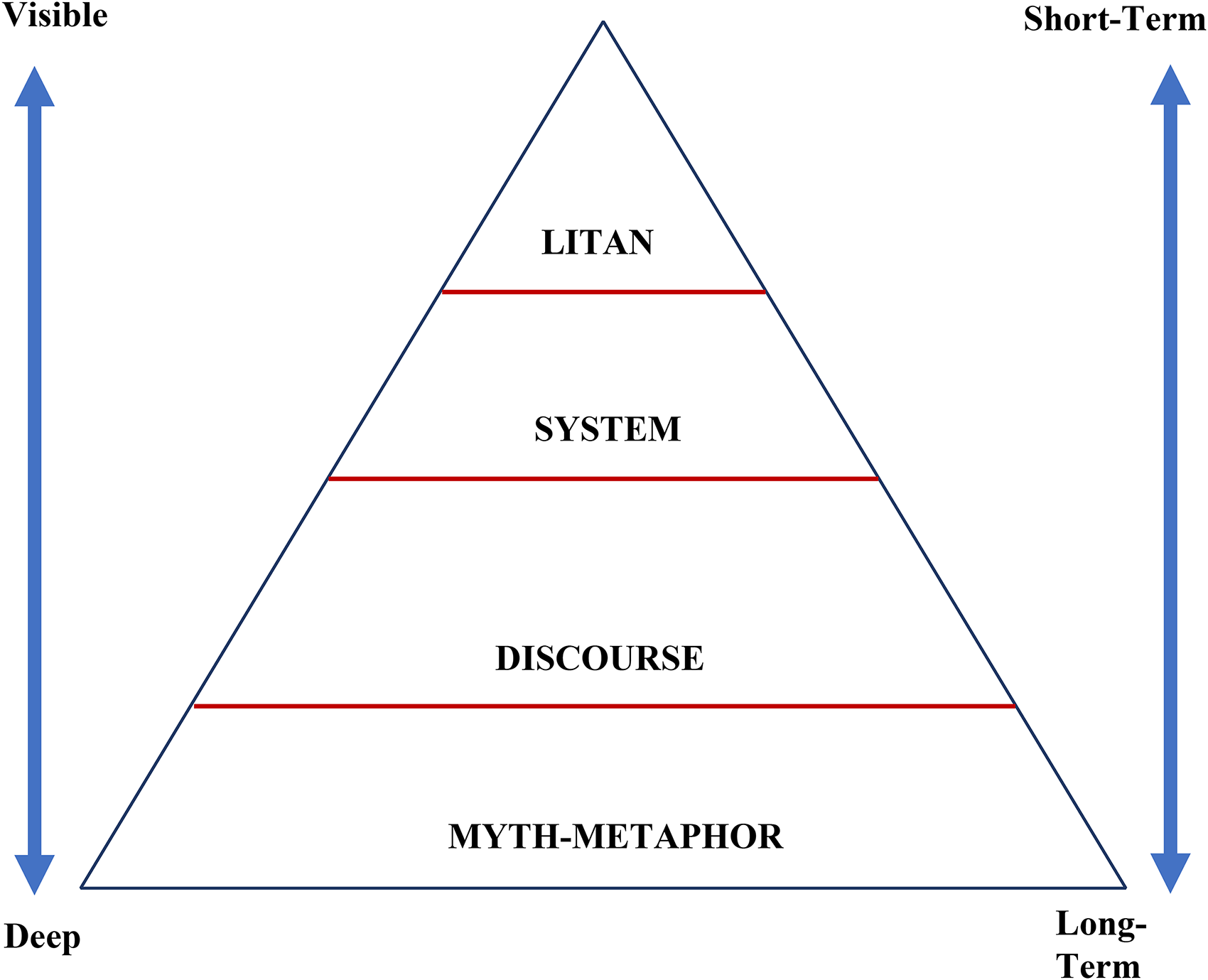
Four layers of analysis in the CLA method. 26
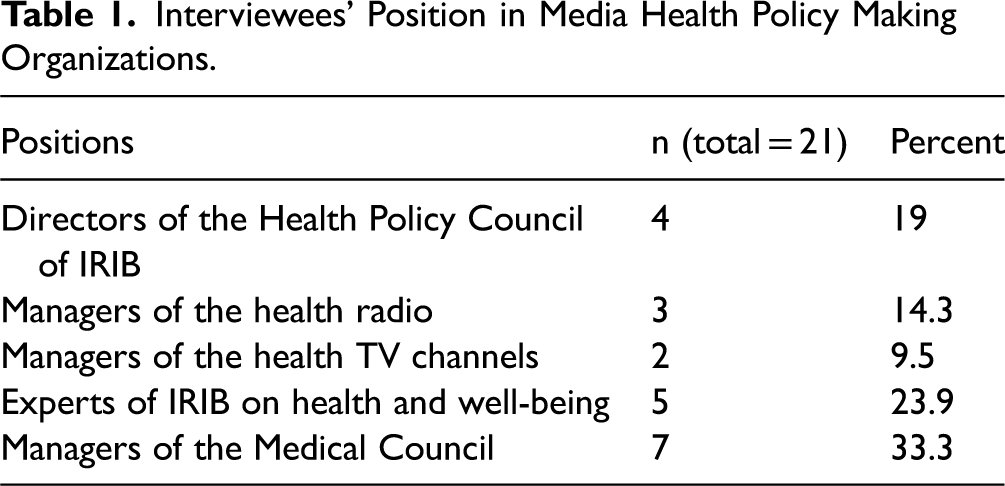
In total, 21 participants were recruited through purposive sampling from health communication experts, members of the medical council of Iran, and managers of health media channels. Before conducting interviews, the objectives and a brief explanation of the study were explained by phone calls or face-to-face conversations with participants, and informed consent was given verbally. The study protocol was approved by the University of Tehran ethics committee. Data collection was performed until we reached data saturation, confirmed by two researchers. Information saturation was achieved when the last three interviews did not provide any new code or additional information. Therefore, the total sample of 21 in this study was considered sufficient as we reached saturation and the sample size was larger than the minimum sample size 12 suggested for qualitative studies.31,32 The semi-structured, in-depth interviews were held between January 2020 and February 2021. The interviews lasted 90 min on average Table 1.
Interviewees’ Position in Media Health Policy Making Organizations.
The inductive approach for the thematic analysis was applied to both interview transcripts and documents.33,34 MAXQDA software version 2021 was used to analyze the interview transcripts. First, the transcripts were reviewed multiple times for accuracy, 35 and emergent themes (open coding) were identified. 36 Then, subthemes were categorized into four main levels (axial coding). In this thematic analysis, initial codes were discussed with the research team to be categorized into the four layers of CLA. We addressed the validity of our findings in three ways. First, the principal researcher worked with a second senior researcher to develop and check a coding framework. Second, interim results were presented to the participants to enhance reflexivity and ensure that presumptions, experiences, and personal bias were considered. Third, all research activities were rigorously documented to permit a critical appraisal of the methods.
Results
First Layer (Litany): Achievements and Barriers
Analyzing the interviews showed that political inclinations in Iran regularly affect the health policy making process. Health policy making in Iran started with the macro transformations in the early 1990s, when there was a change in government leadership. Furthermore, massive social changes following the Iranian–Iraqi War demanded new cultural needs, which IRIB tried to address. Thus, IRIB management attempted to launch new TV channels, which until then had been only two with limited hours of broadcast. One of the interviewees said that “new radio and television channels, with longer hours of broadcast, were launched, with health-related programs being among the most popular shows. However, due to the priority given to political and religious programs, the responsibilities assigned to the IRIB regarding health-related issues had been mostly overlooked.”
Interviewees highlighted the increase in the number of health programs as an achievement. However, they demonstrated the low quality of these health programs as a significant barrier to success. One participant said, “the increase in the hours of TV programs and audiences’ growing interest in health-related shows gradually led to the production of more of these programs. However, no improvement was made in the quality of these programs.” The interviewees also pointed out issues such as “presence of unqualified people in the field of health,” “uninformed selection of experts by TV and radio program producers,” “arguments between producers and health experts,” and “personal preferences” as the roots of the programs’ low quality. One of the former managers of IRIB stated that, “There were times when a producer liked a doctor and invited him to a program. Or they might have been friends or shared some interests. And some doctors were always present on TV and radio programs.”
To enhance the quality of the programs, media policymakers and managers decided to establish a Health Policy Council to supervise and coordinate various production units in the organization. With a high authority, the new Health Policy Council was made up of physicians familiar with media issues. This committee was responsible for assessing the qualifications of experts invited to health-related TV programs and supervising the content of these programs.
The instructions of the Health Policy Council included a list of dos and don'ts for producing TV and radio programs. According to interview results, the committee gradually gained control of commercials and limited some commercials advertising unhealthy food products, regardless of the high money turnover for these commercials. Supplemental Table 1 presents one of the Health Policy Council's instructions for TV programs revealing such programs’ limitations. The Health Policy Council has frequently changed management, members, duties, and authority. Health media activities have also experienced significant volatility over the years, so the council's performance has often been below expectations.
Second Layer: System
In the second layer, we deal with social, economic, cultural, political, and historical causes. Upon its establishment, the Health Policy Council's main objective was to address the low health-literacy levels prevalent among the Iranian population. Increasing the number of radio and television programs on medical and health issues was their first solution to tackle the problem. According to interview results, part of the airtime for a radio channel was dedicated to health issues in 2002. However, it was run by IRIB managers, who were nonetheless familiar with health issues, rather than health specialists. Later, the Health Radio channel started, with its dedicated frequency accessible to many areas in Iran, and is now accessible through digital receivers. Health received its specialized television channel later.
According to the interview data, the council failed to develop a comprehensive and transparent strategy concerning information dissemination, public education, and coherent representation of health messages. The interviewees explained that the health channels’ programs had been mostly in the form of roundtable discussions, which are unlikely to be attractive to many audiences. This failure also reflects the policymakers’ inadequate knowledge about the characteristics of potential audiences, such as their ages, genders, cultural backgrounds, and social classes.
Another challenge was the complete obedience of health channels’ management to IRIB's centralized policies, which has tied their hands by preventing them from treating certain health-related issues. For instance, some of the participants asserted that “constraints on other channels regarding sex education have also been imposed on the health networks.” Furthermore, health channels have largely relied on programs obtained from other networks or institutions, rather than in-house production. The channels have also suffered from self-censorship. This self-censorship is partly a reflection of risk aversion and the low level of creativity among IRIB managers and policymakers. They have opted to avoid initiating any health media campaign or challenging the health care authorities. Producers of health messages may have also lacked adequate maneuvering skills to include sensitive content in their programs or have focused more on securing the largest number of audiences. It is noteworthy that part of the censorship is imposed from outside.
The health channels on radio and television have also suffered from insufficient financing. While IRIB receives direct funding from the public budget, it augments this source with income from commercials and infomercials as well as joint projects carried out with outside entities. One of the participants explained, “This has stopped them from dealing with the social and psychological roots of issues and made them merely focus on the personal and therapeutic aspects of problems, which has made criticizing the status quo and the performance of the government impossible.” These circumstances have relegated the health-related needs of the audiences in favor of those associated with the financial source. Health policy in IRIB was also affected by a more significant challenge, the absence of macro policies in health, which has made the IRIB unable to develop effective media plans. Additionally, we identified the extensive intervention of the government as a cause of failure in media health policy making.
Third Layer: Worldview and Discourse
In the third layer, discourses and worldviews are discussed with the legitimizing structures that commonly remain hidden. Health policy making is influenced and directed by the values and interests of political, ideological, economic, or even social power sources. In fact, disease is a social construct whose meaning is reconstructed by the source of power. 37 Discourses, as systems of knowledge, determine what is right or wrong. 38 At the discourse level, media policymaking for health faces two important challenges. First, the values and ideology governing the IRIB were designed to strengthen the values and ideology of the Islamic Republic of Iran, which set limitations on the production and broadcast of radio and television programs. For example, programs and shows that may cause moral corruption or be considered an insult to society cannot be broadcasted on radio or television. Interpretations of this policy have resulted in limitations for health-related programs, such as programs about sex education.
The second challenge is the never-ending conflict between traditional and modern medicine discourses in Iranian society. 39 While the policymakers and managers of the IRIB seem to believe in using modern medicine, they mostly have traditional perspectives. For example, one of the interviewees, who was a top manager in the IRIB, mentioned, “I’ve always told the producers that they should think about a situation where, for example, their sister is sitting in a taxi alone with the driver, listening to the radio. They should present their ideas, so the taxi driver and their sister feel safe and face no harm.”
Many challenges have arisen when media health policy makers try to convey messages that might be in contrast with people's traditional values or the rules of IRIB. For example, in Iranian society, people do not talk openly about sexual issues because Islam prohibits extramarital relationships and use of the word “condom” is not accepted by IRIB rules. Thus, informing people about prevention methods for HIV or sexually transmitted diseases is very challenging. As a result, in some recent TV programs, although the manager of IRIB tried to adopt an educational approach and show sympathy toward HIV-positive people, the ideological stigma was reproduced. 40 Another example is the restriction on discussing child abuse in order to increase parents’ awareness. One of the participants, who was among the top health policy makers in IRIB, stated, “We used traffic light metaphors when talking about child abuse. For example, we told the families that a child should not sleep in somebody else's house, even in their grandfather's, when they’re under seven. This is the red light.”
With the outbreak of COVID-19, the conflict between traditional and modern medicine emerged again. In the early weeks following the pandemic, when no medications were prescribed yet, some traditional groups asked for the application of traditional medicine. Advocates of traditional medicine even appeared on some TV programs and encouraged people to use salt instead of wearing masks, which led to harsh criticism by many physicians. Then, Iranian radio and television channels focused more on informing people about this crisis, and doctors and managers in charge of the modern scientific sectors were given more time in the media. However, the traditional groups could still promote their ideas by relying on their institutional power.
Fourth Layer: Myth and Metaphor
In the fourth layer, a more in-depth analysis at the myth and metaphor level was conducted. At this level, we delved into society's collective unconscious and investigated social changes through history. The early scope of health issues handled by IRIB's health policy making, which was limited to medical problems and physical well-being, has gradually expanded over the past three decades. The changes in the title of the policymaking entity from Medical Council to Health Policy Council and the addition of psychological, social, and spiritual health reflect this evolution. One interviewee, an ex-director of the Health Policy Council, has explained this evolution: “I gradually shifted the scope of the Council from medicine to health. I saw the high number of deaths in the country that were related to medical issues in small ways.” Yet, other interviewees have described expanding the council's focus from physical health and medical issues to psychological and social dimensions of health as a reflection of global changes. Notably, including psychosocial dimensions in the definition of health converges with Iran's traditional medical knowledge and multi-dimensional approaches to health. 41
Discussion
In this study, the interview analysis across four layers showed that the formation of a specialized committee, the Health Policy Council, instituted health policy making in Iranian mass media. Increasing the frequency and duration of radio and television health programs was one of the first outcomes of media health policy making in Iran. However, establishing the two health channels, radio and TV, was considered the most significant outcome. Africa Health TV (Nigeria), Discovery Home & Health (Latin America, Asia, and United Kingdom), and Mindset Health (South Africa) are examples of health channels in other countries with content similar to that of Iranian health channels. 42
Similar to the outcomes of the Health Policy Council in Iran, which provides health messages and educational programs and applies some restrictions on non-healthy media content, developing media health policies in other countries for both independent (e.g., European countries) and government-controlled media (e.g., Sub-Saharan Africa) could lead to outcomes such as conveying health messages, 43 advocating in favor of vaccination, 44 and adopting health policies and interventions. 45 However, while some argue that traditional health channels have lost their share among the public due to increased use of new health information sources such as the internet and social media,46,47 recent studies suggest that traditional media's impact remains significant. As shown by Hwang and Shah, 48 parents who put more value on television rather than other sources of health information, such as social media, could better keep their children's vaccination schedules up to date. In another study, Piltch-Loeb and colleagues 49 showed that traditional channels such as national TV could increase the likelihood of COVID-19 vaccine acceptance more than social media. Similarly, the Iranian Health TV network has been able to play a significant role in conveying health messages after major public health issues such as COVID-19.50,51
Despite the establishment of a specialized committee and health channels in IRIB, we found that some barriers, such as lack of a systematic approach and instability in the top management of IRIB, itself a prominent feature of Iran's governance structure, have led to drawbacks in achieving strategic goals related to promoting public health through mass media. We also recognized the primary social causes of the current situation as the lack of a thorough strategy, inadequate knowledge of policymakers, insufficient funding, and extensive government intervention in health policy making. Likewise, Motamedi and colleagues 52 demonstrated a “lack of knowledge for policymakers” as a personal barrier to health policy making for sexual health programs in Iran. Interestingly, they also found “lack of a strategic goal,” “financial challenges,” and “uncoordinated and unstable management” as the structural barriers. The consistency between our findings and their results on non-media sexual health programs indicates that most barriers and social causes of ineffective health policy making are rooted in the power structure of a country. Thus, in government-controlled media, every weakness or challenge in the government structure can extend to policymaking for media and negatively impact the outcomes of health policies.
In our study, inadequate knowledge of policymakers was found as a critical factor in making media health programs unsuccessful. Political science scholars also highlighted the importance of policymakers’ knowledge in policy and decision-making. 53 One of the approaches to address this issue is evidence-informed health policy making (EIHP). As Sajadi and colleagues 54 discussed, EIHP is essential to achieving strategic goals regarding health policy making and improving public health. However, health research systems in the Eastern Mediterranean Region, including Iran, are not yet well-developed to create and use knowledge to inform health policy makers, leading to inadequate knowledge of policymakers in Iran. 54
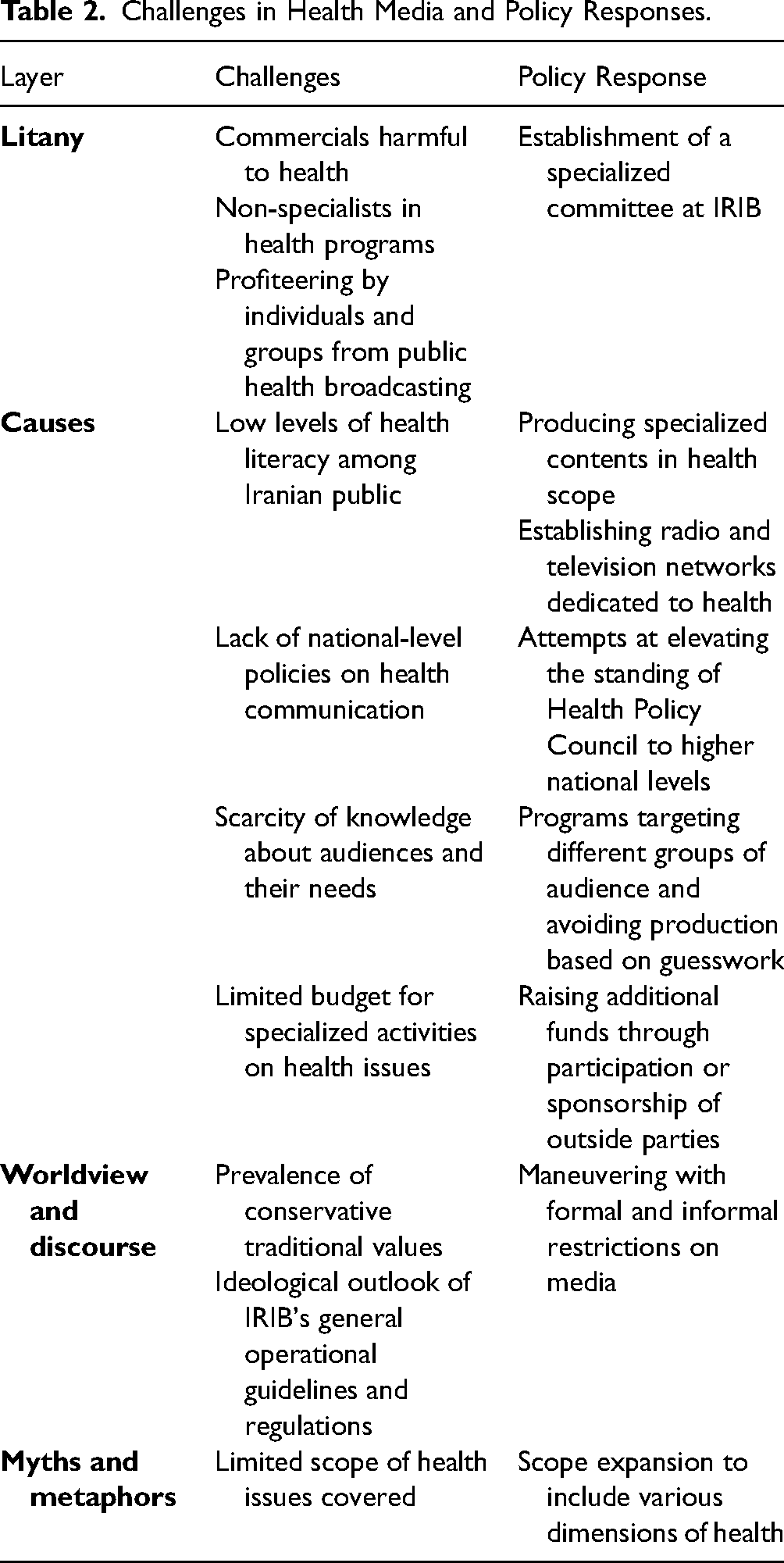
Table 2 summarizes the challenges in media health policy making targeted by policymakers and managers in IRIB and the solutions suggested by them. As shown in Table 2, at the discourse level, the prevalence of traditional conservative values was a significant challenge for health policy makers of mass media. While they suggested maneuvering with the restrictions as a solution, they asserted that its usefulness is limited to a few cases. The role of traditional beliefs in health policy making is not restricted to Iran. Other developing countries with government-controlled media, such as Kazakhstan, experience a similar issue. Recently, a World Health Organization report on the state of health policy making in Kazakhstan stated that a strong conservative attitude toward health in some regions of the country hindered the implementation of health policy decisions developed by evidence-informed policymaking. 55
Challenges in Health Media and Policy Responses.
Given the Islamic ideological approach of Iran's government in health policy making, many of these restrictions target issues such as HIV/AIDS, sexually transmitted diseases, unwanted pregnancy, and abortions. In this regard, some recent studies confirmed our findings and described traditional and religious beliefs, stigma, and non-scientific views of sexual health as challenges to policymaking for sexual health, 52 HIV/AIDS, 56 and reproductive health 57 in Iran.
Based on our findings, there is still a lack of convergence between Iran's governmental and media health policies. For example, in the case of COVID-19, while the successful experience of South Korea in COVID-19 has been rooted in policy alignment, 58 the policy conflict between different executive systems in Iran was identified as the main barrier to controlling the coronavirus spread. 59 In this situation, Iranian national TV appears not to have established any significant interactions with other public health institutions to follow a common health policy.
Furthermore, the Health Policy Council and two health channels in Iran have made little effort to attract the participation of community-based institutions. Part of this argument has to do with the state of the monopoly in IRIB and its non-democratic structure that places it under the total control of the government. Given the importance of democratic media in enhancing citizens’ knowledge of the COVID-19 pandemic, 60 the lack of success of Iranian media in reconnecting Iranian citizens with health messages during the pandemic was predictable.
Given the potential of mass media in enhancing health access, targeting individuals with different backgrounds could be a strategy for policymakers. As shown by previous studies, having daily exposure to mass media could increase the frequency of receiving health care for various groups of people. 61 Mass media exposure could also positively affect women's reproductive health by providing them with more choices of facility delivery. 62 However, according to our findings, even though Iran's constitution calls for social justice in health, this discourse has not been adequately reflected in the IRIB programs regarding access to health care and health outcomes. For instance, while IRIB health programs could cover new developments in the prevention and treatment of HIV like other countries, 63 our previous study revealed that the main outcome of mass media in Iran for HIV/AIDS was reconstructing HIV-related stigma. 56
Another drawback of government-controlled mass media is their minimal efforts to create the grounds for two-way interaction with the audiences. In contrast, independent mass media focus on enhancing information-sharing, two-way interaction, co-production, and self-organization. 64 During COVID-19, while government-controlled mass media (e.g., Russian mass media) tended to mislead audiences by not reporting the actual positive rate of confirmed cases and the virus reproduction rate, 65 new technologies provided by independent media have facilitated communication for immediate response to the crisis. 66
Finally, the following suggestions might be of use in improving mass media health policy making, including increasing the participation of social groups and civil institutions, democratizing the mass media, interacting with audiences as active participants, improving audiences’ trust, and considering the cultural diversity of audiences in health-related education.
Limitations
Several limitations may impact our findings. First, due to limited access to documents and records of the Health Policy Council in Iran, our findings may not accurately represent all dimensions and challenges of health policy making in a government-controlled mass media. The second limitation may arise from conducting interviews with individuals associated with IRIB or Health Policy Council that may restrict them from explaining all defects and limitations of the IRIB system due to potential threats to their position. Including more health communication experts, health program producers, and critics not associated with IRIB could enhance the validity of the study findings. Third, differences among cultures, politics, and religions in countries with government-controlled mass media may limit the extension of our findings to other countries. Despite these limitations, we could capture the main barriers, achievements, social causes, discourse, and metaphors in health policy making for a government-controlled media by employing a multilevel approach that could inform health policy makers when designing an effective media health policy.
Conclusion
Previous studies have shown the significant impact of mass media policies on public health. 67 This impact includes all aspects of health care, from identification and prevention to treatment and evaluation.68,69 Through a causal layered analysis, this study has investigated the evolution of Iran's health media policy on Iranian national TV and radio (IRIB) as an example of government-controlled media. The results showed that despite achievements such as the launching of health radio and television channels, ideological approaches to media policy in health and lack of alignment between government policies and health media policies led to challenges that influence health-related media products. This study informs health policy makers about challenges in media health policy making for government-controlled mass media and can be used by designers of health promotion interventions to effectively use media for promoting public health.
Supplemental Material
sj-docx-1-joh-10.1177_27551938221143640 - Supplemental material for Government-Controlled Mass Media as an Obstacle to Health Policy Making: The Case of Iran
Supplemental material, sj-docx-1-joh-10.1177_27551938221143640 for Government-Controlled Mass Media as an Obstacle to Health Policy Making: The Case of Iran by Atefeh Aghaei and Mohammad Mahdi Mowlaei in International Journal of Social Determinants of Health and Health Services
Footnotes
Acknowledgements
The authors thank Iran's Health Policy Council members for their participation and valuable feedback.
Author's Note
Mohammad Mahdi Mowlaei is also affiliated with Faculty of communication sciences, Allameh Tabataba'i University, Tehran, Iran.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.