
Abstract
Approximately 6 million neonatal deaths occur globally, with approximately 99 percent of them occurring in developing countries. This study is an attempt to examine the prevalence and influence of non-biological factors on perinatal mortality in India. National Family Health Survey (2015-2016) data and bivariate and multivariate techniques have been used to fulfill the aforesaid objectives. Findings suggest that approximately 47 perinatal deaths occurred per 1,000 pregnancies lasting seven or more months during the last five years preceding the survey in Uttar Pradesh. Parental education, wealth status, variables related to pregnancy and delivery, mother's demographic factors, mother's height, and child characteristics have shown significant impact on perinatal mortality. For a policy point of view, more emphasis is needed on quality of care of National Health Mission (NHM) strategy at times of greater risk—that is, birth and the first few days of life—which could be the way forward for reducing high perinatal deaths.
The time after 28 weeks of gestation and the first week after termination of pregnancy (the perinatal period) is considered the most significant stage of life of a newborn.1,2 It reflects the general health and the various socio-biological features of mothers and newborns. Perinatal death provides a good indication of the degree of pregnancy wastage and the quality and quantity of health care available to the mother and the newborn. 3 Particularly, it is an important symbol of maternal health and nutritional status of the population and shows the excellence of obstetric and pediatric care availability in the community. 4 The survival of the newborn during the first week of life is mainly determined by stresses of intrauterine life and the birth process, as well as by adjustment to a new environment, nutrition, and infection. Therefore, the early neonatal period is the most hazardous period of life. Perinatal deaths result from complications of preterm birth, asphyxia or trauma during birth, infections, severe malformations, and other causes. Maternal health is essential for neonatal health, and maternal infections contribute to adverse pregnancy outcomes. 5
Approximately 8.2 million under-five child deaths occur per year. 6 A large number of these deaths occur (almost 3 million) occur within one week and approximately 2 million deaths occur within 24 hours of the newborn's life. 6 Furthermore, 3.3 million are stillbirths. A child has 15 percent more risk of dying in the first four weeks of their life than at any other time before their first birthday. Approximately 99 percent of neonatal deaths occur in developing and less developed countries. 6 India has been no exception to the above trends. A large number of neonatal deaths have occurred in African and South Asian countries that the slightest progress in reducing neonatal deaths has been made. 6
Overall, considerable improvement has been made in the direction of achieving the Sustainable Development Goals Target 3.2. Worldwide, the under-five mortality rate has declined by 61 percent since 1990, dropping from 93 to 37 deaths per 1,000 live births in 2020. However, the share of neonatal mortality in under-five mortality has been rising over time, from 40 percent in 1990 to 47 percent in 2020. 7 Although, this trend showing the sluggish decline in neonatal mortality than post-neonatal and childhood mortality throughout the last two decades in India. 8
Several risk factors have been associated with perinatal mortality. 9 These include low birth weight, maternal health and intrapartum complications, the gender of the child, poverty, and health care coverage—that is, skilled attendance at birth and proportion of births that take place at a health facility. 10 It is evident that during the early neonatal phase, non-biological factors play a prominent role in determining infant mortality, in addition to the so-called biological and health care factors. 11 Uttar Pradesh is one of the states with very high infant mortality rates. There is a significant amount of research into infant and child mortality. But fewer studies have covered perinatal mortality in Uttar Pradesh. Previous studies have been done on perinatal mortality, some of which are mainly based on hospital data that itself has many limitations, and very few studies have been based on secondary data.12–15 A significant number of studies have already been done on levels, trends, and determinants of infant mortality as a whole, but research focusing on the correlates of perinatal mortality is scarce in the Indian context, specifically for Uttar Pradesh due to lack of reliable data and the basic belief in the importance of biological and genetic factors in determining perinatal mortality.
Data Source and Methodology
Data
Data for the present study was used from the fourth round of National Family Health Survey (NFHS-4), conducted during 2015-2016. The NFHS-4 is the Indian version of the Demographic and Health Survey conducted by the International Institute for Population Studies, Mumbai, under the stewardship of Ministry of Health and Family Welfare, Government of India. It is nationally representative data that provides estimates on health issues at the district level across places of residence. NFHS-4 adopted a two-stage stratified sampling design to reach the ultimate sampling unit. The 2011 census served as the sampling frame for the selection of Primary Sampling Units (PSUs). PSUs were villages in rural areas and Census Enumeration Blocks (CEBs) in urban areas. Within each rural stratum, villages were selected from the sampling frame with probability proportional to size. In urban areas, CEBs were sorted according to the percentage of the Scheduled Castes and Tribes (SC/ST) population in each CEB, and sample CEBs were selected with probability-proportional-to-size sampling.
In NFHS-4, for Uttar Pradesh, information was collected from 76,233 households for a response rate of 97.5 percent. Of these households, 97,661 women aged 15-49 were interviewed, with a response rate of 97.2 percent. For the present study, the pregnancy history of women has been used to fulfill the study objective. NFHS collects information on those mothers and their children who were born (or stillbirths) within the five years preceding the survey years. For the present analysis, we considered information of 42,563 such pregnancies reaching seven months of gestation.
Exposure Variable
The perinatal death is the outcome variable in the study. It is defined as “any death that occurred after 28 weeks of gestation period (late stillbirth) and infant death within first week of birth.” Perinatal death is recoded as a binary variable in this study, where “0” indicates that the child survived for more than seven days and “1” indicates otherwise (i.e., late stillbirth and death of the newborn within seven days).
Independent Variables
All possible socioeconomic and demographic variables are included in the study. The independent variables consist of women's age (<20 years, 20-29 years, 30-39 years, and 40-49 years); place of residence (urban vs. rural); women's education level (no education, primary education, secondary education, and higher education); birth order (1 order, 2 order, 3 order, and 4+); caste (SC/ST – Scheduled Castes/Scheduled Tribes, OBC – Other Backward Classes and General); religion (Hindu, Muslim, and Others); sex of the child (male vs. female); consanguinity among couple (no vs. yes); consuming tobacco (no vs. yes); women height (<145 cm vs ≥145 cm); media exposure (no vs. any exposure); and region (Bundelkhand, Avadh, Braj, and Purvanchal).
Statistical Methods
The present study employed univariate, bivariate, and multivariate statistical techniques for data analysis. Bivariate analysis has been used to examine the level and differentials of the perinatal mortality in Uttar Pradesh. In multivariate analysis, binary logistic regression has been used to show the effect of non-biological factors on perinatal mortality.
Concentration Index. Income-related inequality in perinatal mortality was quantified by the concentration index (CCI) and the concentration curve (CC), using the household wealth score (continuous) as the socioeconomic indicator and binary outcome as perinatal. The CC is obtained by plotting the cumulative proportion of perinatal mortality against the cumulative share of perinatal mortality ranked by the socioeconomic indicator.16,17 The CCI can be written as follows:
If the curve lies above the line of equality, the CCI takes a negative value, indicating a disproportionate concentration of inequality among the poor (pro-rich). Conversely, if the curve lies below the line of equality, the CCI takes a positive value, indicating a disproportional concentration of inequality among the rich (pro-poor). In the absence of socioeconomic-related inequality, the CCI is zero.
Decomposition of the Concentration Index. The study used Wagstaff decomposition analysis to decompose the CCI. Wagstaff's decomposition demonstrated that the CCI could be decomposed into the contributions of each factor to the income-related inequalities.
17
Based on the linear regression relationship between the outcome variable
Here, C is the outcome of two components: first, the determinants or “explained” factors. The explained factors indicate that the proportion of inequalities in the perinatal mortality is explained by the selected explanatory factors, that is, xk. Second, a residual or “unexplained” factor
Results
The socioeconomic and bio-demographic characteristics of the respondents are summarized in Table 1. A higher proportion of women belonged to the 20- to 29-year-old age group (73%), resided in rural areas (79.5%), and belonged to the Hindu religion (79%). Approximately 43 percent of women had no formal education; one-fourth of women had birth order 4+ and belonged to the SC/ST caste group (27%). Approximately 14 percent of respondents had consanguineous marriage and 8 percent consumed tobacco. Approximately half of the respondents (48.4%) had exposure to media, and 16 percent had height less than 145 centimeters. Regional variation in the sample distribution was also observed.
Sample Distribution of Women Who Had Experience Perinatal Mortality in Last Five Years Preceding the Survey in Uttar Pradesh, 2015-2016.
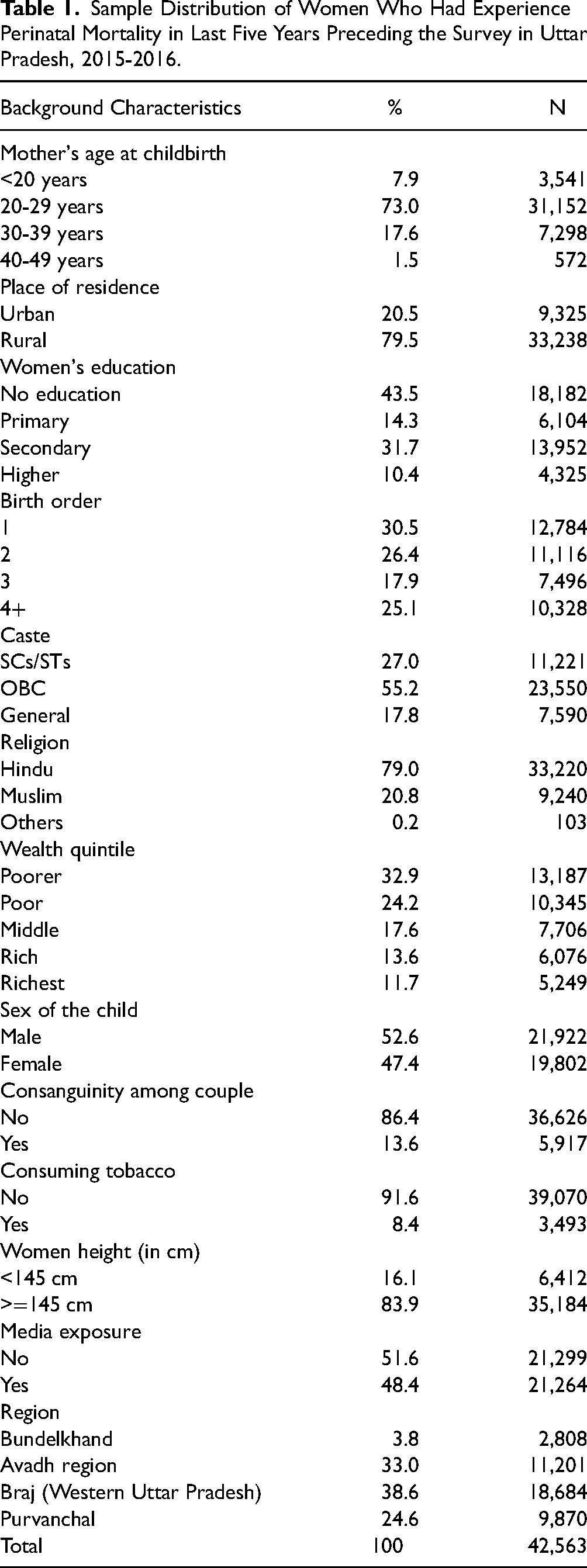
Table 2 shows bivariate and multivariate association between perinatal mortality and selected background characteristics. Overall, 5.6 percent of the respondents experienced perinatal mortality in last five years preceding the survey. Perinatal mortality was significantly higher among younger and older age women than other age groups. It was also more prevalent in rural areas (5.9%) compared to urban counterparts. Additionally, women's education has a significant negative association with perinatal mortality. The prevalence of perinatal mortality was higher among women with first birth order (4.3%) and those who had 4+ birth order (4.2%). The likelihood of perinatal mortality was lower among female children than male counterparts [OR: 0.80; CI: 0.72-0.89]. Women who had consanguineous marriage were 26 percent more likely to have perinatal mortality compared to those who did not [OR: 1.26; CI: 1.09-1.45]. Similarly, women who consumed tobacco had a 34 percent higher likelihood of perinatal mortality than those who did not consume tobacco [OR: 1.34; CI: 1.12-1.59]. Moreover, the likelihood of perinatal mortality was 34 percent less likely among women with a height more than or equal to 145 centimeters (cm) than those who had less than 145 cm height [OR: 0.66; CI: 0.58-0.76].
Prevalence of Perinatal Mortality and Logistic Regression Estimates by Background Characteristics in Uttar Pradesh, 2015-2016.
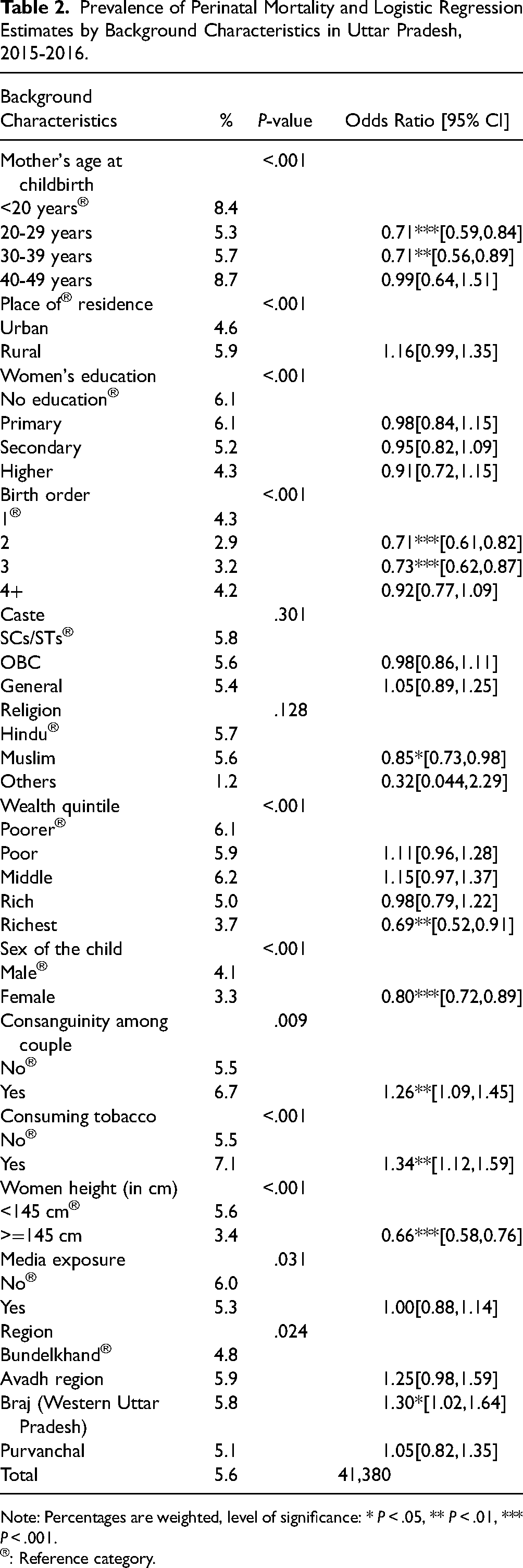
Note: Percentages are weighted, level of significance: * P < .05, ** P < .01, *** P < .001.
®: Reference category.
Figure 1 depicts the CC and CCI for perinatal mortality across regions of Uttar Pradesh. The highest CCI was for Avadh region (−0.082), followed by the Bundelkhand region (−0.08) and Braj-Western region (−0.065) of Uttar Pradesh, while the lowest CCI was for the Purvanchal region (−0.060).
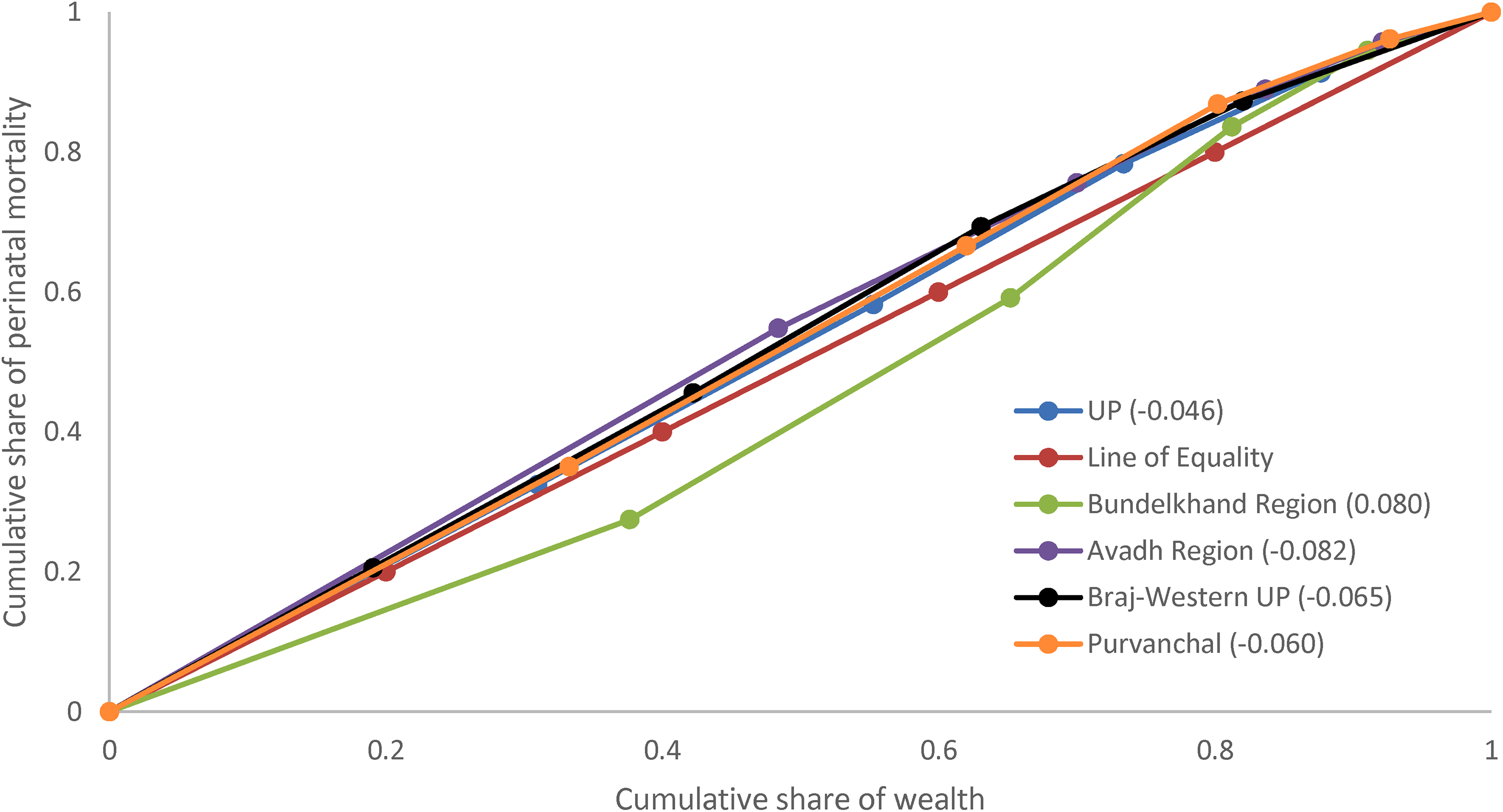
Concentration curve and index for perinatal mortality for Uttar Pradesh and its regions.
Estimates of decomposition analysis for the contribution of various explanatory variables for perinatal mortality among women aged 15-49 years in Uttar Pradesh is presented in Table 3. The percentage contribution is the column to be interpreted for depicting the percentage contribution of factors for explaining socioeconomic status-related inequality for perinatal mortality. The negative and positive signs are to make the total contribution as 100 and dependents upon the sign elasticity and CCI of the table. Absolute contribution is the product of elasticity and CCI, whereas the percentage contribution is the proportion of absolute contribution multiplied by 100. Hence, the magnitude of the percentage contribution depends on the elasticity and CCI. In explaining socioeconomic inequality for perinatal mortality, place of residence (35.2%) was the most significant contributor in explaining the highest inequality, followed by women's height (25.3%), educational level (21.9%), and tobacco consumption (14.5%). Additionally, age at childbirth (3.5%) and birth order (2.8%) contributed in explaining socioeconomic inequality for perinatal mortality.
Estimates of Decomposition Analysis for the Contribution of various Explanatory Variables for Perinatal Mortality Among Women Aged 15-49 Years, Uttar Pradesh, 2015-2016.
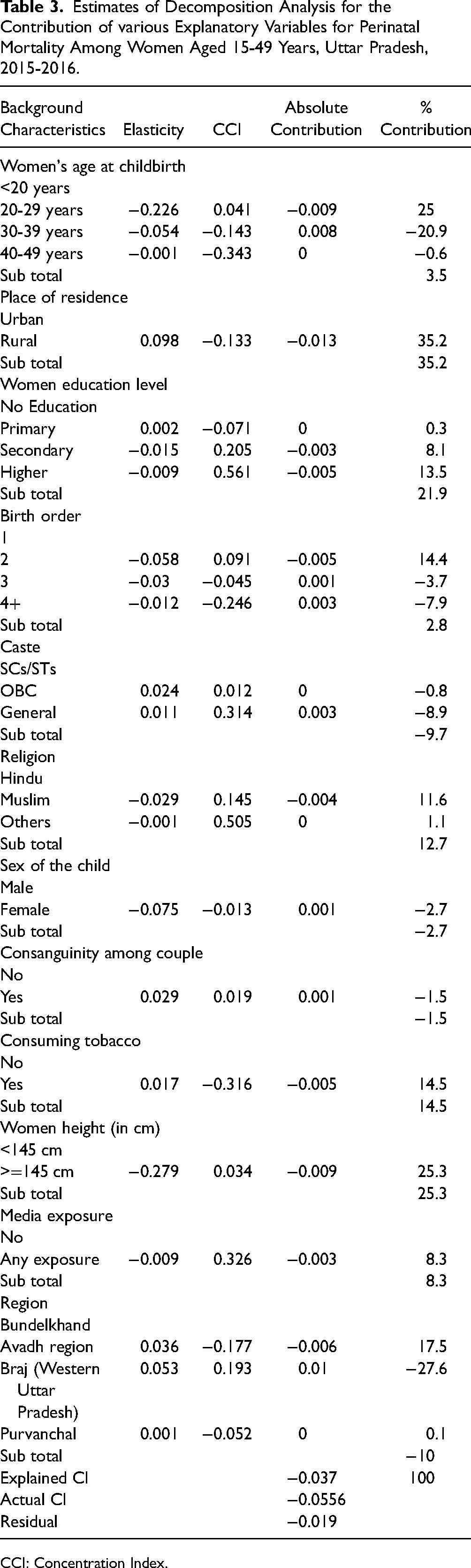
CCI: Concentration Index.
Discussion
Infant and child mortality is generally used as a measure of the socioeconomic and health status of any society or any nation. It is an outcome rather than a cause, and hence, it directly measures the results of distribution and use of resources. Significantly higher neonates and infant mortality have shown the unequal distribution and use of resources by the socioeconomic group of the population of India. The study demonstrated that considerable high perinatal mortality differentials persist at socioeconomic factors related to mother and children. Mother's age was found to be significantly associated with the reduction in perinatal mortality. Older mothers not only possess better knowledge of pregnancy and childbirth but also enjoy greater autonomy compared to younger mothers, which helps them take care of their neonates in a better way in this period.18,19 Education also plays a significant role in reducing perinatal mortality. Smoking is an important determinant of premature birth and perinatal mortality. Smoking during pregnancy may lead to abnormal development of the placenta, premature birth, and delayed growth and may also be accountable for 15 percent of all premature births. 20 We found that female children had a lower risk of dying in the perinatal period compared to males. It has been suggested that male children are more prone to perinatal deaths than females for biological reasons. 21 By contrast, some studies have found a higher risk of perinatal deaths in females than males. However, these studies justified their findings by arguing that gender preference was practiced in their study populations.22,23
The “region” of state is also significantly associated with the risk of perinatal death. It was found that newborns from the Western Uttar Pradesh region were more likely to die in the perinatal period. Lower levels of socioeconomic development and poor functioning of the system could be some of the factors behind the poorer performance of Braj (Western Uttar Pradesh). Other regions, such as Avadh, are also characterized by comparatively poor socioeconomic and demographic indicators and dysfunctional government health care systems, which contributes to a concentration of perinatal mortality in the area.
Decomposition findings suggest that the observed perinatal mortality differential economic status of households in India is mainly a reflection of the wide rich-poor disparity in societal and community-level factors. Typically, nonpoor populations have better access to school and enjoy better education. Findings also suggest that maternal and child health care-related program factors played an important role in reducing the poor–nonpoor gap in perinatal mortality. 24 The inclusion of these factors is significant in the context of government policy and programs. The poor–nonpoor gap would have been much larger if perinatal were not as prevalent among the poor population of India. The inclusion of these factors is significant in the context of government policy and programs. The Janani Suraksha Yojana, a conditional cash transfer scheme, was initiated under the NRHM to encourage women to give birth in a health facility and had the prime objective of reducing maternal and neonatal deaths. The expansion of Janani Suraksha Yojana has led to substantial increases in the coverage of antenatal and intrapartum care and has probably contributed to the reduction in the numbers of perinatal and neonatal deaths. 25
The study, however, has some limitations, the first being the cross-sectional nature of the data. Studies based on national surveys are always subject to recall biases and limitations of a cross-sectional nature. Further, the analysis can be subject to potential heterogeneity due to the factors not considered in the study. The authors recommend that more large-scale studies be conducted in under-developed states of India.
Conclusion and Policy Implications
The study is a modest attempt to cater to the perinatal mortality scenario in Uttar Pradesh and has touched on various socioeconomic and demographic determinants. The results suggest that in addition to strengthening maternal health care programs, especially postnatal care within 48 hours, substantial efforts must also be made to improve household conditions (toilet facility, ventilation facilities) and female education (including literacy). It should be noted, however, that despite an overall health advantage, enormous differences exist between poor and better-off women in accessing maternal health care services. Community health worker support for mothers to manage their newborns can help in reducing risks. Specific training for the basic care of newborn can be feasible at community levels through routine home visits. Basic care information and awareness about protecting children from environmental stress, getting adequate nutrition, and preventing infections can help in reducing risks.
Footnotes
Acknowledgements
The authors are grateful to reviewers, who provided valuable comments for improvement of the manuscript.
Authors’ Contributions
All authors have contributed equally in each section of the study, read, and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.