
Abstract
A primary goal of the New Rural Cooperative Medical Insurance (NRCMI) is to provide financial protection against health care costs and alleviate the financial burdens of rural residents in China. This article examines whether NRCMI participation impacted the incidence of catastrophic health expenditure (CHE) among middle-aged and older adults (45 years old and above). The analysis utilized data from the 2007 China Household Income Project survey in rural areas and an instrumental variable estimation method in Anhui and Sichuan provinces, which exhibited heterogeneity in the NRCMI implementation schedule. The results show that NRCMI participation was not associated with changes in the CHE incidence among families. The finding is consistent with the prior literature using quasi-experimental study designs. This study provides empirical evidence for policymakers, highlighting that the impact of NRCMI participation on financial protections is limited despite its extensive population coverage. The limited effects are probably due to the low reimbursement rate and increased utilization of expensive health care services.
The escalating costs of health care services have been a concern for many countries in the world. For example, 62 percent of bankruptcies in the United States were contributed by medical problems in 2007. 1 In Vietnam, 58 percent of low-income individuals with severe illnesses reported that they avoided or discontinued necessary treatments due to unaffordable medical bills. 2 More than 40 percent of total health expenditure was paid out-of-pocket in many developing countries such as Mexico, Columbia, and Thailand. 3
In China, medical expenditures could account for as much as 65 percent of per capita income in some low gross domestic product counties in 2011. 4 Medical poverty could negatively affect people in many ways in the short and long term. In the short term, it could prevent individuals from seeking timely diagnoses or treatment, 5 increase households’ inter-family labor substitution, 6 and lead them to fall into poverty traps, either by selling assets or borrowing money at excessive interest rates from loan sharks. 7 In the long term, those with limited financial resources to cope with medical bills may become trapped in a vicious cycle of worsening health and deepening poverty. 8
Since the founding of the People's Republic of China, residents in both urban and rural areas had health coverage, receiving health care services for free or at very low prices. This system eventually collapsed, primarily due to the significant financial burden on the central government, in the 1980s. 9 After the late 1970s, most of the rural residents and approximately half of the urban residents lost their health insurance coverage. In 1998, China formally launched the Urban Employee Basic Medical Insurance, a reformed national health insurance program. This program aimed to provide comprehensive health insurance coverage for the majority of urban employees, requiring premium payments from both the employers and employees. During 1998–2006, there was a substantial urban-rural health insurance coverage gap. Starting in 2006, rural residents began to gain health insurance coverage when China formally launched the New Rural Cooperative Medical Insurance (NRCMI) nationwide. The NRCMI was initiated in some villages in 2006 and gradually expanded to cover the remaining villages in 2007 and 2008.
The primary goal of the NRCMI, like other health insurance, is to provide financial protection to the insured. The central government guided the overall NRCMI implementation, while provincial governments decided the implementation schedule for each county. Once implemented at the county level, county and village leaders determined the participation schedule for each village. NRCMI covers 740 million rural residents, the majority of whom are more economically vulnerable and had a fragmented coverage of health insurance since the mid-1980s. As of the end of 2006, the enrollment rate of NRCMI has reached 95 percent, and 54 percent of the national population obtained health insurance in only three years. 10
Even though the NRCMI covers the majority of rural residents in China, its reimbursement rates for both inpatient and outpatient services are considerably lower compared to beneficiaries of the Urban Employee Basic Medical Insurance. The NRCMI participants may receive reimbursements as low as 20 percent for outpatient services if using top-tiered hospitals in urban areas and 60 percent for inpatient services if using village clinics. In contrast, the average reimbursement rate of the Urban Employee Basic Medical Insurance for inpatient services is 80 percent, with the ratio for outpatient services ranging between 50 percent (in top-tier hospitals) and 80 percent (in community clinics). 11
Given the significance of the NRCMI as a major health policy breakthrough following China's economic reforms in the 1970s and its coverage of much of the rural population, its impacts on financial protection warrant rigorous evaluation. Using the gradual rollout schedule of the NRCMI at the village level, which facilitates the use of the instrumental variable methodology, this article examines whether participating in NRCMI changes the likelihood of experiencing catastrophic health expenditure (CHE) among middle-aged and older adults in rural China.
Literature Review
Effects of the New Rural Cooperative Medical Insurance on Health Outcomes and Health Utilization
A large body of literature has examined the effects of the NRCMI on health outcomes, psychological wellbeing, doctor visits, and inpatient service utilization.12–16 Overall, the findings of the effects of NRCMI participation on health outcomes and health utilizations are mixed.
Some studies have identified positive effects of the NRCMI, particularly on inpatient service utilizations.12–14 For example, using primary data from five provinces between 2005 and 2008 and the method of difference-in-differences, Babiarz and colleagues 12 found that the NRCMI implementation improved the finances of township health centers, and the NRCMI participants increased their inpatient service utilization significantly. Li and Wang 13 analyzed the China Health and Retirement Longitudinal Study 2011 data using a multilevel regression approach and found that the NRCMI participation was associated with increased utilization of inpatient and outpatient health care services. Additionally, Ma and collegues 14 used the China Health and Nutrition Survey 2004 and 2006 data and the method of propensity score matching and difference-in-differences to investigate the effect of NRCMI participation on food consumption, finding improved intakes of protein, carbohydrates, and fats among beneficiaries.
However, other studies found no significant effects of NRCMI on health outcomes, well-being, and service utilization. For instance, in contrast to the findings of Babiarz and colleagues 12 and Li and Wang, 13 Yu and colleagues 15 used primary data from Ningxia and Shandong provinces in 2006 and reported no significant association between NRCMI enrollment and inpatient service utilization for middle- and low-income families. Using data from the China Longitudinal Healthy Longevity 2005 and 2008 Survey and a combined method of propensity score matching and difference-in-differences, Cheng and colleagues 16 concluded that NRCMI did not enhance enrollees’ self-perceived health status or mortality rates. Similarly, Huo and Chen 17 found no impact of NRCMI participation on recipients’ happiness using data from both the China Family Panel Study and the China Health and Nutrition Survey.
The examination of NRCMI's effects on health outcomes and health service utilization often concerns the issue of self-selection-based endogeneity bias. 18 To address these issues, Lei and Lin 19 used longitudinal data from the China Health and Nutrition Survey and the county-level NRCMI implementation year as the instrumental variable. They found that participating in NRCMI at the individual level had no effect on formal health service utilization or health conditions. The instrument was argued to be valid as individual participation is highly correlated with county-level implementation because individuals can only participate in NRCMI when their county implements the NRCMI plan. Additionally, the county-level implementation of NRCMI is exogenous to the individual's health use and health conditions, as the variation in the timing of implementing NRCMI mainly followed the guidance of central and provincial governments.
Effects of New Rural Cooperative Medical Insurance on Health Expenditures and Poverty
Another set of studies investigated the role of NRCMI implementation in alleviating poverty by relieving the health expenditure burdens on families. Xu and colleagues 20 compared the incidence rates of health payment-induced poverty before and after the implementation of NRCMI. They found decreased rates in all five counties in Guangdong province. Similarly, Chen and colleagues 21 found a 25.79 percent and 19.2 percent reduction in the poverty gap among the NRCMI trial counties in Hubei province in 2003. Sun and colleagues, 22 using primary data collected in Shandong province in 2014, concluded that NRCMI reimbursement reduced health payment-induced poverty by one percentage point.
Though informative, the results obtained from these descriptive studies may be biased. It remains unclear whether the occurrence rates or intensity of poverty are comparable before and after NRCMI implementations. Furthermore, the trial counties in the studies by Chen and colleagues 21 and Sun and colleagues 22 were not randomly selected. The participants and nonparticipants of NRCMI were different in many ways, including socioeconomic status, access to health care services, and reception of other local welfare programs.
Similar to the work of Lei and Lin, 19 Cheung and Padieu 23 also used combined methods of fixed effects and instrumental variable estimation to address the issues of self-selection bias and reverse causality. Differently, Cheung and Padieu 23 instrumented the household enrollment rates of NRCMI in communities to investigate its impact on household savings. The authors stated that the instrumental variable is exogenous, as participation rates of NRCMI within communities correlate with efforts by the central and provincial governments but are not directly associated with household saving and consumption behaviors.
Large-scale surveys typically measure the economic burden of health care payments using either absolute amounts of expenses or relative burdens. CHE measures the relative impact of health care payment on the basic standard of living of a household, defined as a ratio of medical costs to disposable income, varying from 5–40 percent across countries.3,24 However, neither outcome measured in the two studies mentioned above reflects the relative financial burdens of NRCMI.
Effects of New Rural Cooperative Medical Insurance on Catastrophic Health Expenditure
Seven existing studies have examined the effects of NRCMI on CHE. Similar to the findings on health service utilization and health outcomes, the impact of NRCMI on the incidence or prevalence of CHE obtained in prior studies is mixed.
Five of the seven studies used either linear or logistic regressions to simply compare the incidence or intensity of CHE before and after the implementation of NRCMI. Among these, two studies showed that the NRCMI was effective in reducing the prevalence and intensity of CHE. Gong and colleagues 25 found that the implementation of NRCMI significantly reduced the prevalence of CHE in 2006 and 2008 in Shandong and Ningxia provinces. Zhang and colleagues 26 observed that NRCMI reimbursement helped reduce the intensity of CHE, particularly among people with lower incomes using inpatient services. However, two other studies found that NRCMI was not effective. Jiang and colleagues 27 discovered that increasing reimbursement benefits of NRCMI did not reduce the incidence of CHE among families with chronic patients. Li and colleagues 28 found that NRCMI participation was not significantly associated with lower CHE nationally in 2008. Sun and colleagues, 29 on the other hand, found that NRCMI reimbursement did not reduce the prevalence of CHE but lessened its intensity in Shandong province in 2004. These five studies may involve endogeneity issues, where enrollees who chose to participate in NRCMI might be significantly different from non-enrollees. In addition, the likelihood of experiencing CHE and participation in NRCMI could affect each other bidirectionally.
The other two studies, using quasi-experimental designs, found no effect of NRCMI participation in reducing the incidence of CHE. Specifically, Wagstaff and colleagues 30 used the combined method of propensity score matching and difference-in-differences and two primary datasets collected in 12 trial provinces between 2003 and 2005. Their findings indicated that NRCMI participation did not significantly change the incidence of CHE, which used 10 percent, 20 percent, and 40 percent as cutoffs, respectively. The other study employed similar methodologies and the primary data collected in 17 trial provinces in 2003 and 2005. 31 They concluded that NRCMI participation had no effect on the incidence of CHE. However, it is noteworthy that neither of these two quasi-experimental studies examined the effects of NRCMI in the later stage of its expansion after 2006.
Other Factors Influencing Health-Related Financial Burdens
Prior studies also explored three clusters of leading factors contributing to health payment-related impoverishment: socioeconomic position before health care, chronic or severe illnesses, and certain demographic and behavioral factors. These studies have concluded that higher socioeconomic position groups in developing countries and countries in transition are more likely to obtain health care when needed, with their medical expenditure proportion being significantly lower than those in lower socioeconomic positions. 32 Health-induced poverty is also more prevalent in families with members suffering from chronic diseases, 33 injuries or other health shocks, 34 multiple morbidities, 35 and serious illnesses. 36 Additionally, a higher heath payment-induced burden is associated with older age 37 and broader social networks, enabling patients to get access to more health care services. 38
No existing study has examined the effects of NRCMI on CHE using instrumental variable estimation, a rigorous quasi-experimental design that is suitable when policy rollout is gradual. Building on the existing literature, this article will: (a) assess the impact of NRCMI on relative financial burden using the ratio of health-induced expenditure to disposable income, instead of an absolute poverty line, to determine poverty status; (b) use instrumental variables to address the endogeneity issues, caused by selection bias and reverse causality, and measurement error, which were noted limitations in prior studies; (c) examine the effects of NRCMI participation on enrollees’ financial burdens in the later stage of its expansion.
Methodology
Data
This article uses the China Household Income Project (CHIP) 2007 data. The CHIP data have been the only national representative data with information on both NRCMI implementation at the village level and NRCMI participation at the individual level in 2007. In addition, the CHIP data explicitly collected information on incomes and expenditures at both the individual and household levels, which helps in obtaining the incidence of CHE more accurately.
The CHIP data have three questionnaires that cover three targeted populations, respectively: urban residents, rural residents, and the migrant population. This study uses the rural dataset. A total of 8,000 households were randomly selected from 800 villages in nine provinces, which were also randomly chosen to represent the three regions: east, central, and west China. Among the 8,000 households, all family members aged 16 and older were interviewed face-to-face if they lived in the same household for more than six months in the prior year to the survey.
This study used individual-, household-, and village-level characteristics. The individual information was collected from each family member. The household-level data were obtained from the household head, such as the information on social networks, family events/shocks, the welfare reception by the household, etc. The village-level information was also used in the analysis, which was collected from the village leaders. As a result, each respondent had three levels of information in the analytical data. Given that the samples were not selected through probability-proportional-to-size sampling, multiple weights were adopted in the analysis in this study.
In the CHIP 2007 dataset, four out of the nine provinces had all villages implement the NRCMI in 2007, and three other provinces had above 98 percent of the villages implement NRCMI by 2007. Therefore, this study excluded these seven provinces and focused on the two remaining provinces, Anhui and Sichuan provinces, which had village implementation rates in 2007 of 72.5 percent and 91.8 percent, 1 respectively. This study also excluded the sample who did not report their health-related costs. 2 The final analytical sample size was 3,583 individuals in 1,980 households in 197 villages. The unit of analysis in this study was the individual, which was consistent with the work of Lei and Lin. 19 Even though theoretically the enrollment of NRCMI is at the household level, practically some members may opt out from the enrollment. The participation information collected in the CHIP survey also reflected that not all of the households had all their members participate in NRCMI in 2007.
Measurement
The key dependent variable, CHE, was defined as the occurrence (Yes/1, No/0) if the ratio the health-related costs to disposable income exceeded 40 percent. A uniformly accepted threshold for measuring CHE has not been reached. The thresholds range from 5–40 percent, varying based on the denominators, numerators, and study population.39–42 Typically, higher thresholds (i.e., 40% or 30%) were adopted in developing countries or when the denominator was the ability to pay or disposable income (household income minus other dead-end need expenses like food). Conversely, lower thresholds (i.e., 5%, 10%, or 20%) were adopted in developed countries or when the denominator was annual household income or consumption.
In this study, the health-related costs (the numerator of CHE) included payments for health care services after reimbursement, medical assistance, health insurance premiums paid out-of-pocket, and other accommodation costs, such as transportation associated with receiving health care services. The household income (the denominator of CHE) included salary income, net business income, intra- and inter-family transfers, and other government transfers. Considering China's status as a middle-income country in terms of the real gross domestic product per capita, and following the work of Xu and colleagues, 43 I chose a higher threshold of 40 percent in the analysis. To test the robustness of the results, this study also used 20 percent and 10 percent as alternative CHE thresholds 44 in the sensitivity analysis.
As a comparison, this study examined medical expenses as another dependent variable to assess the effect of NRCMI participation on absolute expense amounts alongside the relative financial burden measured by CHE. Medical spending refers to the total out-of-pocket amount paid by an individual, excluding reimbursements and reduced amounts, for insurance premiums, medications, treatment, facilities, and other health-related services in 2007.
The key independent variable was the individual's NRCMI enrollment status in the survey year, dummy coded as one for enrolled and zero for not enrolled. The analysis included two instrumental variables. One was the year of NRCMI implementation at the village level, coded from 2002 to 2007, or as 9999 if not yet implemented. The second was the NRCMI participation rates in the survey year at the village level, treated as a continuous variable and coded as zero if not yet implemented. Both were reported in the village survey questionnaires by the leaders of the villages. To examine if the results persist, this study also considered the NRCMI participation rate and roll-out time at the county level in the sensitivity analysis. Details about the implementation of NRCMI and the validity of these instrumental variables are provided in the empirical strategy section.
The control variables included individual demographic characteristics and health status. The demographic characteristics included age, marital status (coded as one for married or remarried, and zero for cohabiting, divorced, widowed, or never married), educational attainment (coded as one for no schooling, two for completed elementary school, three for completed junior middle school, and four for completed high school or above), the quintile of annual income, and the province dummy variable. The control variables of health status included self-perceived health status (ranging from 1–5, where a higher value indicated worse health status), disability status, and disease history in the last three months (coded as one if the respondent reported a disability and disease history, and zero otherwise).
Empirical Strategies
To address the issues of selection bias and reverse causality, this study used the instrumental variable method. 45 Specifically, it utilized two instrumental variables—the time of NRCMI implementation in villages and the NRCMI participation rates in these villages. Individual NRCMI enrollment status was instrumented using these village-level variables—NRCMI implementation and the percentage of enrolled households. Both the instrumental variables have been conceptually and statistically validated as effective in multiple studies.17,19,23 To reduce the overidentification problem, this study used these two instrumental variables both jointly in the first set of analyses and separately in subsequent analyses. 46
As outlined in the background section, the year of macro-level NRCMI implementations—the first instrumental variable in the analysis—was determined by the central government and provincial governments. Once the NRCMI was implemented at the county level, leaders at both county and village levels decided which village would participate in which year. Lei and Lin 19 used the county-level NRCMI implementation as the instrumental variable to examine the effects of NRCMI enrollment on health service utilization and health conditions. Similarly, I posited that the village-level implementation of NRCMI is exogenous to an individual's health expenditure, following the rationale of the implementation procedure.
This study's second instrumental variable—the participation rate of NRCMI in a village during the survey year—aligned with Cheung and Padieu's work, 23 which instrumented for NRCMI enrollment with the percentage of enrolled households in the community to examine the effect of NRCMI on household savings. Despite the nature of voluntary enrollment at the household level, the village-level participation rates are largely determined by macro-level efforts and incentives. During NRCMI implementation, central and provincial governments provided increased reimbursement rates and other benefits to boost the rural residents’ participation incentives. In addition, village leaders conducted home visits to transfer knowledge of NRCMI benefits and acknowledge the necessity of participations.47,48 Consequently, following Cheung and Padieu's assumption, 23 I considered the village-level NRCMI participation rates as exogenous to individual health expenditures.
The validity of the two instrumental variables was also statistically verified using three tests— the Kleibergen-Paap rank Lagrange-Multiplier (LM) test for under-identification, the Cragg-Donald Wald F statistics for weak identification, and the Sargan-Hansen test for overidentification. The under-identification test checks if the excluded instruments are correlated with the endogenous regressors. 49 A rejection of the null hypothesis with a Chi-squared p-value (< 0.05) in this test means the model is identified.
The weak identification test evaluates if the instruments are correlated with the endogenous regressors weakly. Both Cragg-Donald Wald F statistic and Kleibergen-Paap Rank Wald F statistic are compared against the 10 percent maximal IV size generated by Stock-Yogo weak ID test critical values, which was 19.93 in this analysis. F statistics exceeding the 10 percent maximal IV size suggest that the instruments are not even weakly correlated with the endogenous regressors. 49
The final validity test in this analysis was the overidentification test, which examined the exogeneity of all instruments. The null hypothesis of this test is that all the instruments are exogenous under the assumption that the valid instrument is no less than the endogenous regressors. A large Chi-squared p-value (> 0.05) indicates that the instruments are valid in the way that they are not correlated with the residuals and the instruments are excluded from the estimating model correctly. 49
Sensitivity Analysis
In the last step, this study conducted two sensitivity tests to verify the robustness of the results obtained from the IV analyses. The first test altered the threshold for CHE from 40 percent to 20 percent and 10 percent. Accordingly, if a respondent's health-related expenditure exceeded 20 percent or 10 percent of the annual household income, this respondent was categorized into the group who experienced CHE in the survey year.
The second sensitivity test used the NRCMI participation rate and implementation time at the county level as instrumental variables. Specifically, in line with the methodology in Lei and Lin's work, 19 counties with any of the villages implementing NRCMI in or before 2017 were considered to have NRCMI implementation. The NRCMI participation rate at the county level was calculated as the average participation rate of all villages in a county where NRCMI was implemented. Results using the two instruments, both jointly and separately, were reported, mirroring the approach of the primary IV analysis in this study.
Results
Descriptive Results
The descriptive analysis results show the characteristics of villages, households, and individuals according to their NRCMI implementations or participation status in 2007. Specifically, at the village level, 68 villages in Anhui and 101 villages in Sichuan implemented NRCMI. The average household participation rates in these villages were 90.5 percent in Anhui and 91.6 percent in Sichuan. In general, compared to the villages that had NRCMI implemented in 2007, those with no NRCMI implementation had smaller populations, fewer households, and lower average household incomes. The travel time to the nearest county and clinic was consistent across both types of villages in both Anhui and Sichuan.
The second section in Table 1 presents the household characteristics. The numbers of NRCMI-participating households were 689 and 1,007 in Anhui and Sichuan, respectively, while 205 and 81 households did not participate in NRCMI in these provinces in 2007. Notably, the non-participating households differed in characteristics—they had fewer older adult members aged 60 and older, lower total household income, more extensive social networks, and slightly fewer major household events in both provinces.
Descriptive Results of the Village-, Household-, and Individual-Level Factors by NRCMI Implementation and Participation.
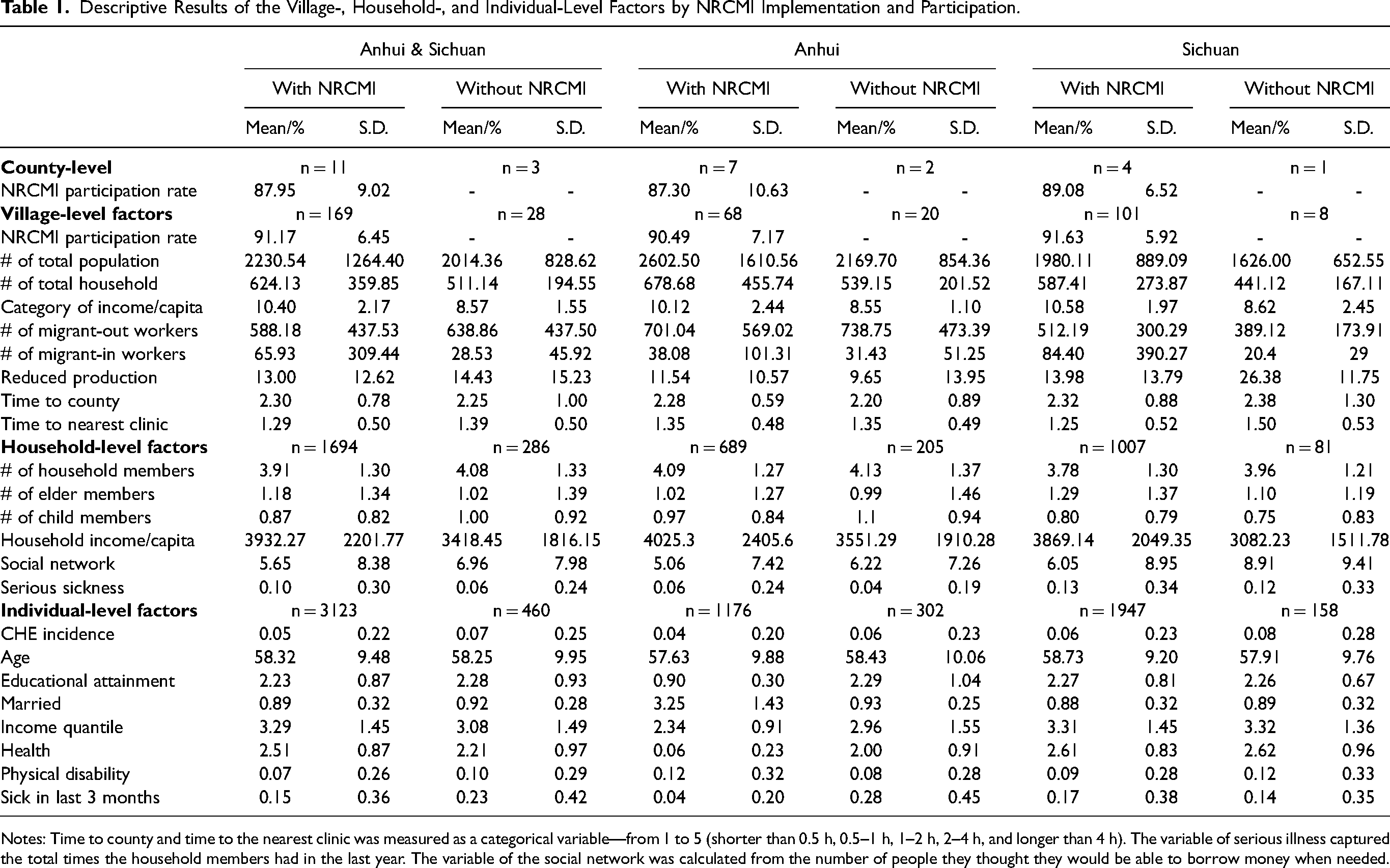
Notes: Time to county and time to the nearest clinic was measured as a categorical variable—from 1 to 5 (shorter than 0.5 h, 0.5–1 h, 1–2 h, 2–4 h, and longer than 4 h). The variable of serious illness captured the total times the household members had in the last year. The variable of the social network was calculated from the number of people they thought they would be able to borrow money when needed.
In terms of the individual characteristics of the analytical sample, the prevalence of CHE was higher among the individuals without NRCMI than those with NRCMI in 2007 in both Anhui and Sichuan provinces. In Anhui, the non-participating sample reported lower average annual incomes but better self-perceived health status compared to their participating peers. However, these characteristics did not vary between the groups in Sichuan. The attributes of average age, educational attainment, and marital status did not show significant differences between participating and non-participating individuals in both Anhui and Sichuan.
Instrumental Variable Estimation Results
Overall, individual participation in NRCMI was not significantly associated with the changes in the incidence of CHE. The results were consistent across the pooled sample (n = 3,424), as well as the sample from Anhui only (n = 1,385) and Sichuan only (n = 2,039), as shown in the first columns of Table 2, Table 3, and Table 4, respectively. As shown in the last few rows of these tables, the validity of the group instrumental variable, which combined village-level participation rate and roll-out time simultaneously, passed all over-, under-, and weak-identification tests.
Instrumental Variable Estimations of Effects of NRCMI Participation on CHE Incidence and Medical Expense Amount among Adults Aged 45 and Older in Anhui and Sichuan Provinces Using 40% as the Threshold of CHE.
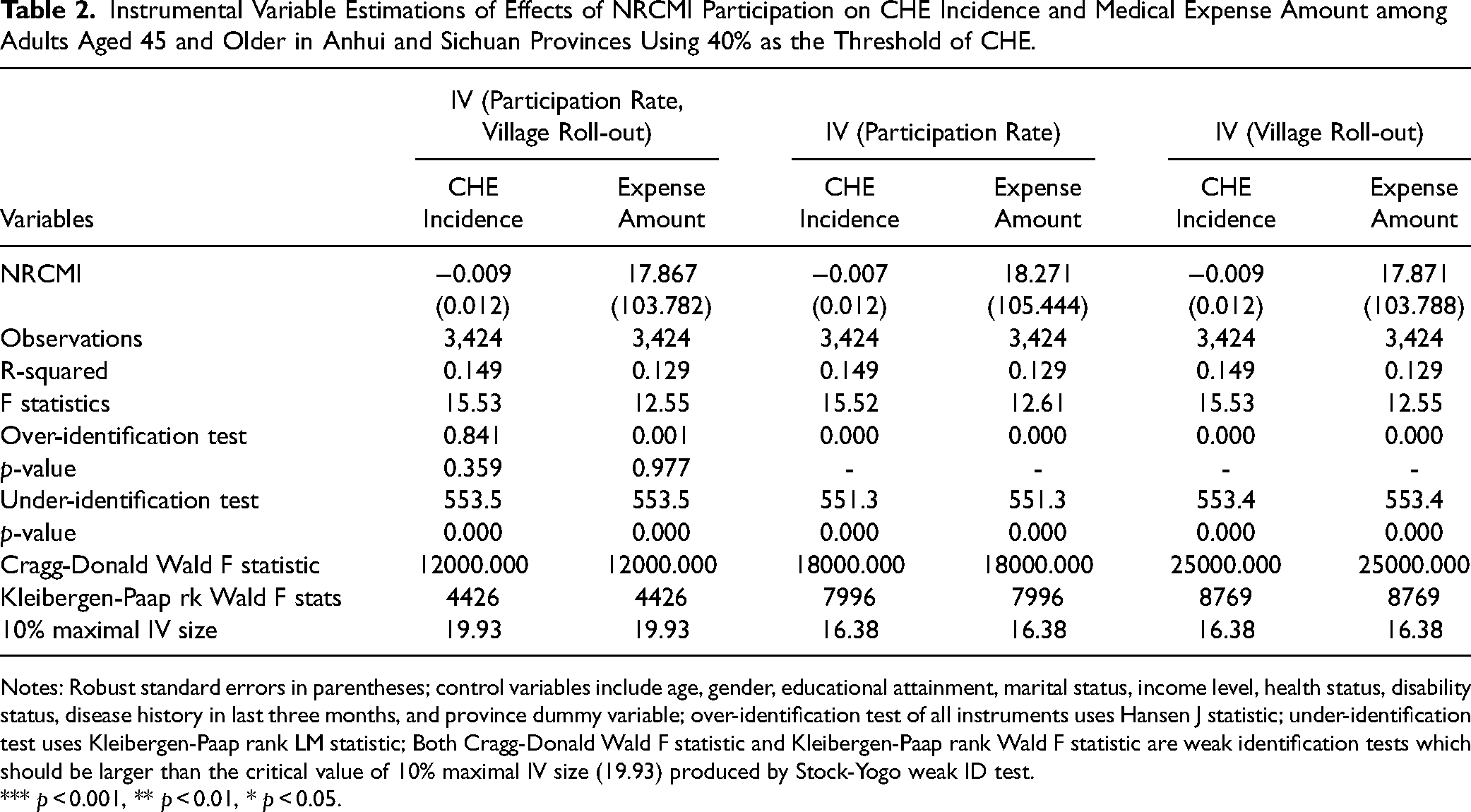
Notes: Robust standard errors in parentheses; control variables include age, gender, educational attainment, marital status, income level, health status, disability status, disease history in last three months, and province dummy variable; over-identification test of all instruments uses Hansen J statistic; under-identification test uses Kleibergen-Paap rank LM statistic; Both Cragg-Donald Wald F statistic and Kleibergen-Paap rank Wald F statistic are weak identification tests which should be larger than the critical value of 10% maximal IV size (19.93) produced by Stock-Yogo weak ID test.
*** p < 0.001, ** p < 0.01, * p < 0.05.
Instrumental Variable Estimations of Effects of NRCMI Participation on CHE Incidence and Medical Expense Amount among Adults Aged 45 and Older in Anhui Province Using 40% as the Threshold of CHE.
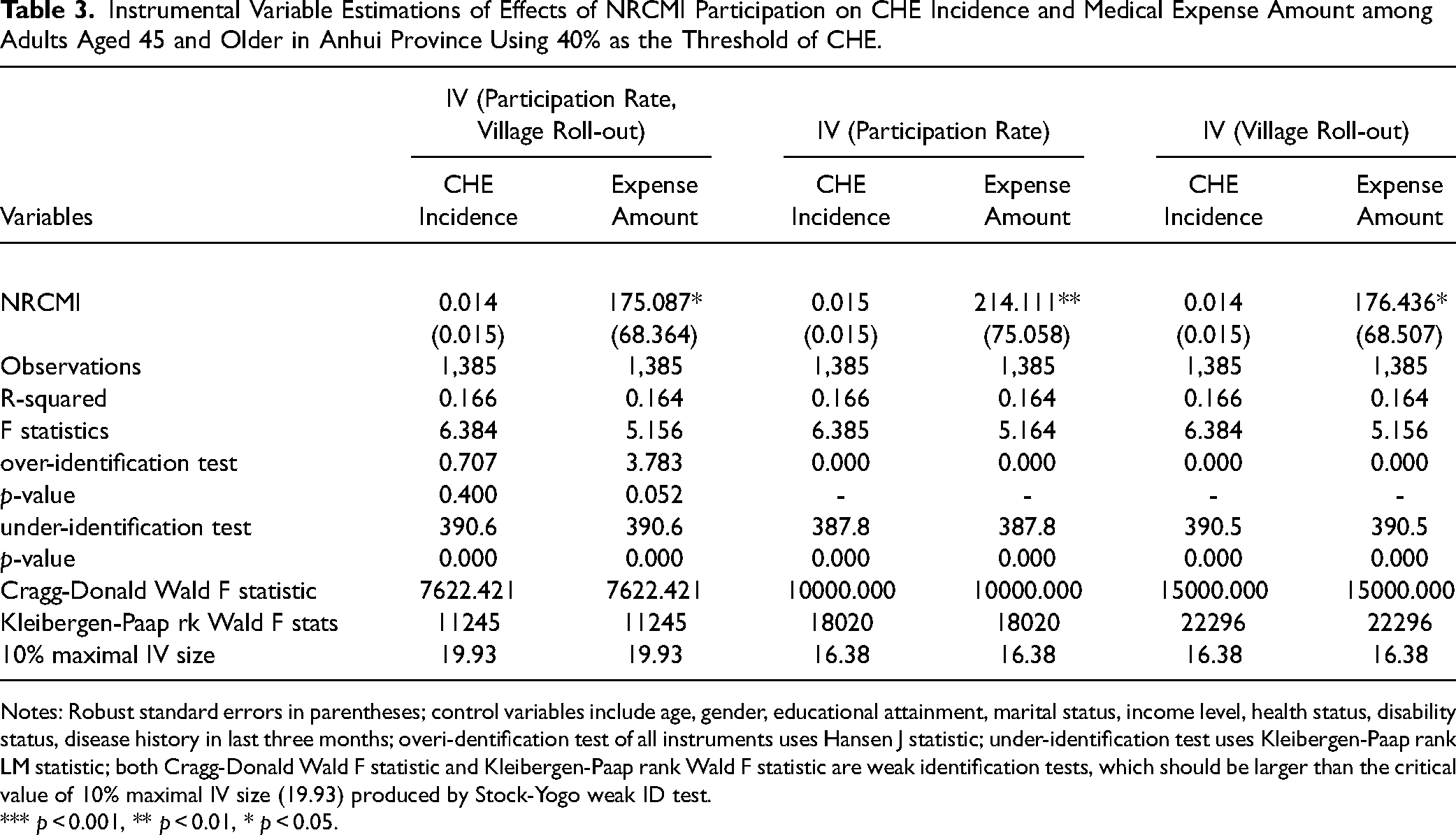
Notes: Robust standard errors in parentheses; control variables include age, gender, educational attainment, marital status, income level, health status, disability status, disease history in last three months; overi-dentification test of all instruments uses Hansen J statistic; under-identification test uses Kleibergen-Paap rank LM statistic; both Cragg-Donald Wald F statistic and Kleibergen-Paap rank Wald F statistic are weak identification tests, which should be larger than the critical value of 10% maximal IV size (19.93) produced by Stock-Yogo weak ID test.
*** p < 0.001, ** p < 0.01, * p < 0.05.
Instrumental Variable Estimations of Effects of NRCMI Participation on CHE Incidence and Medical Expense Amount among Adults Aged 45 and Older in Sichuan Province Using 40% as the Threshold of CHE.
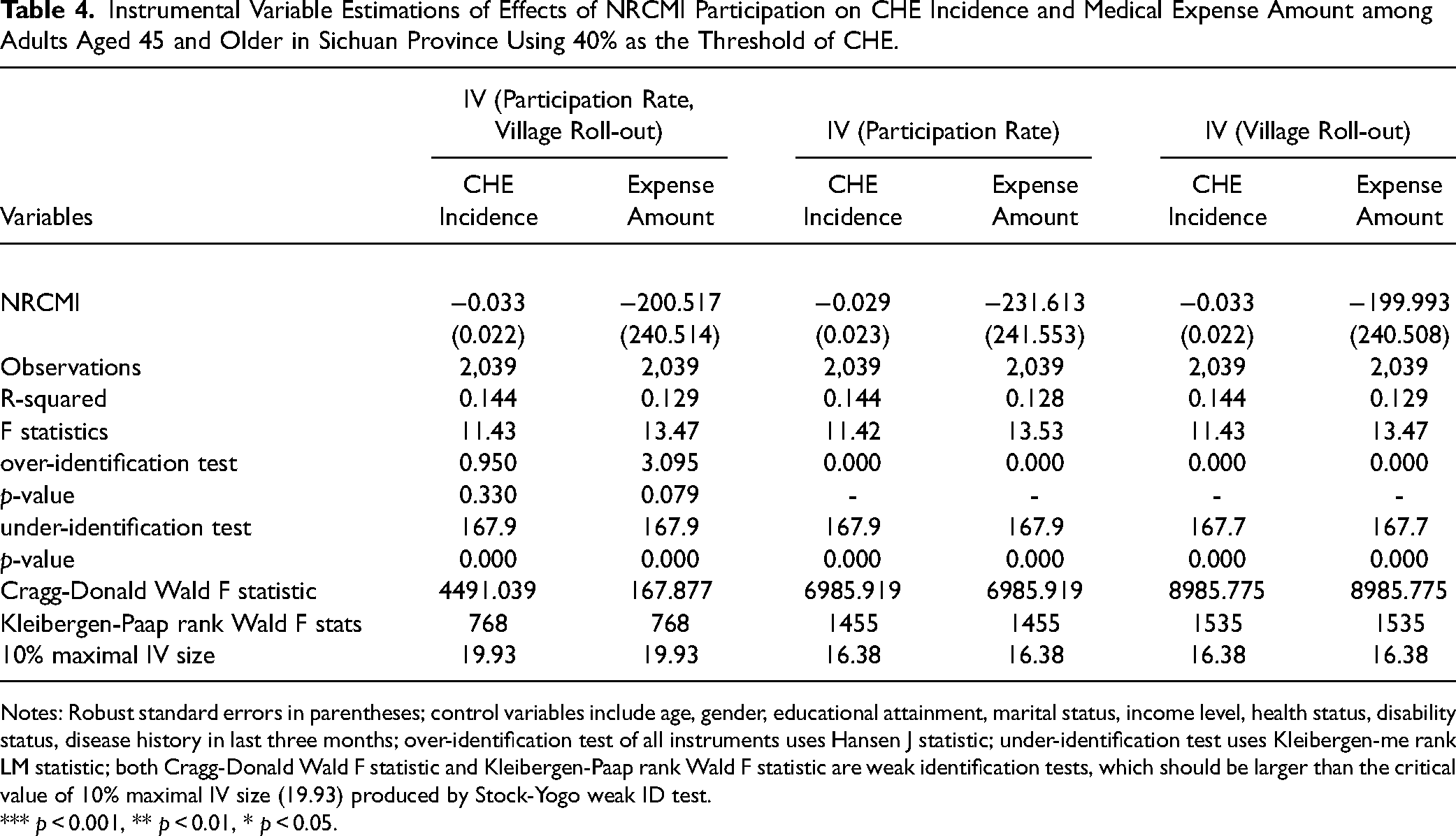
Notes: Robust standard errors in parentheses; control variables include age, gender, educational attainment, marital status, income level, health status, disability status, disease history in last three months; over-identification test of all instruments uses Hansen J statistic; under-identification test uses Kleibergen-me rank LM statistic; both Cragg-Donald Wald F statistic and Kleibergen-Paap rank Wald F statistic are weak identification tests, which should be larger than the critical value of 10% maximal IV size (19.93) produced by Stock-Yogo weak ID test.
*** p < 0.001, ** p < 0.01, * p < 0.05.
However, individual NRCMI participation was significantly associated with an increased amount of medical expenses in Anhui province. Specifically, NRCMI participants spent 175.1 more yuan on average on medications, treatments, facilities, and other health-related services in 2007 compared to non-participants (see Table 3). The significant association was not observed in the Sichuan sample or the pooled sample, (see Table 4), under the condition that the two instruments used in the analyses passed the three validity tests.
Similar results were obtained using the village-level NRCMI participation rate and NRCMI roll-out time, respectively, as the instrumental variables in the analyses; NRCMI participation had no significant impact on the changes in CHE in either Anhui or Sichuan but increased the actual amount of medical expenses in Anhui. However, it should be noted that the instruments did not pass the over-identification test because the equations using the two instrumental variables, respectively, were exactly identified with the p-values smaller than 0.05.
Sensitivity Analysis Results
The first set of sensitivity test results, shown in Appendix Table 1, confirmed the robustness of the results stated earlier. In the first sensitivity test, using 20 percent and 10 percent as CHE thresholds, the analyses showed that NRCMI enrollment did not significantly alter the incidence of CHE among middle-aged and older adults in Anhui and Sichuan. These analyses passed all the validity tests in these analyses.
As shown in Appendix Table 2, using the county-level participation rate and roll-out time as instruments, the sensitivity analysis obtained consistent results with the analyses using the village-level participation rate and roll-out time as instruments, both for the incidence of CHE and the actual amount of medical expenses. The NRCMI participation did not change the incidence of CHE significantly or the amounts of medical spending in the pooled sample.
Conclusion and Discussions
Using the 2007 rural data from the CHIP and the instrumental variable method, this study investigated the effect of participating in NRCMI on the incidence of CHE and the actual amounts of medical expenses. The results show that NRCMI enrollment did not significantly impact the likelihood of experiencing CHE among middle-aged and older adults in Anhui and Sichuan. However, in Anhui in 2007, NRCMI participation increased the actual amount of medical expenses, a trend not observed in Sichuan. These results were confirmed by robustness tests which used the alternative CHE cutoffs and county-level instruments. These results suggest that NRCMI did not significantly alleviate the health-related financial burdens of rural beneficiaries. Policymakers could consider implementing cash subsidies or other relative welfare programs to reduce out-of-pocket payments on health care services among those who are more likely to experience CHE.
Prior studies have concluded mixed results in terms of the effects of NRCMI on the dollar value of health-related expenses and economic burdens induced by health services and medicines. Although none of the prior studies used instruments and village-fixed effects or took the endogeneity issue into account to investigate the impact of NRCMI on relative financial burden among the recipients, the results found in this study generally aligned with the prior research, particularly with those using quasi-experimental studies such as propensity-score matching and difference-in-differences analyses, which suggest that financial burdens did not impact significantly after participating in NRCMI. This study took a further step and examined both the relative financial burden, measured by CHE, and the absolute financial burden, measured by the actual amount of medical expenses.
There were two potential explanations for these findings. First, the reimbursement rates, which vary across regions and provinces, were generally low, particularly for outpatient services that were more commonly used as mentioned earlier. The average reimbursement rate in 2008 was 26.6 percent for inpatient service, 50 while for outpatient facilities and clinic visits, the reimbursement rates were even lower. 30 Additionally, due to the complexity of the reimbursement criteria and guidelines, beneficiaries had limited knowledge about eligible reimbursements and their amounts. Consequently, while the NRCMI beneficiaries increased their utilization of health services, this did not reduce health care costs.
Another possible explanation for these results could also be related to the changes in health service utilization behavior. The urban insured individuals in China were found to opt for more expensive treatments, services, and medicines after obtaining health insurance. 51 Although this trend has not yet been tested among rural beneficiaries, it is plausible that newly insured rural residents might seek health care from formal health care facilities, which are generally more costly than the services from village-based barefoot doctors. The annual household income might not have significant variations pre- and post-NRCMI enrollment; health care costs could rise substantially due to the usage of more expensive health care services and medicines. As a result, the relative financial burden for the new NRCMI recipients might have increased instead of decreasing or remaining stable.
This study had three contributions. First, it examined the effect of NRCMI on the relative financial burdens of beneficiaries, which had not been explored by using instrumental variables and village fixed effects, taking into account the endogeneity issues. Prior mixed findings were primarily due to the different empirical strategies each study used to deal with the selection bias, omitted variables, and bi-directional causality. Second, this study also went beyond measuring out-of-pocket health expenses in dollar terms, focusing on CHE, defined as a ratio of health-related costs to total household disposable income, to examine the relative financial burden of NRCMI beneficiaries. Third, this study added to research on the later-stage effect of NRCMI implementation. Most prior studies focusing on NRCMI's effects have used pilot counties or those that implemented NRCMI in its very early stage as the analytical sample. In contrast, this study considered counties that implemented NRCMI in the last two years before the implementation rates reached as high as 95 percent.
However, the results obtained from this study should also be interpreted cautiously, given that there were a few limitations in this study. Firstly, the two provinces analyzed were chosen because they had significant variations in NRCMI implementation at the village level and enrollment at the individual level. Consequently, the generalizability of the results of this study may be limited. Secondly, due to the data limitation, this study was not able to investigate what level of health care facilities the NRCMI beneficiaries used during the survey year. Given the considerable price differences across facility levels and the absence of data on service usage frequency in the CHIP surveys, it is untestable whether the increased health care costs were due to the more expensive health care services used or because health care services were more frequently used.
This study provides empirical evidence for policymakers, highlighting the limited impact of NRCMI participation on financial protections, while acknowledging the limitations of the studies. Future policy implementations could consider adopting additional strategies to enhance the effectiveness of NRCMI in reducing health-related financial burdens. Future studies could examine the longer-term effects of NRCMI on financial burdens by tracking changes in enrollment status and CHE over more years, particularly after the overall implementation rates reached 95 percent in 2008. Furthermore, comparative studies on the impacts of universal health care programs and means-test cash transfer programs in alleviating health payment-induced poverty in other countries would be beneficial. Such research could provide more evidence for the Chinese government to expedite the implementation of certain welfare programs, aiming to achieve the goal of eradicating poverty. 52
Supplemental Material
sj-docx-1-joh-10.1177_27551938241251747 - Supplemental material for Does Participating in New Rural Cooperative Medical Insurance Change Catastrophic Health Expenditure? Evidence from the China Household Income Project
Supplemental material, sj-docx-1-joh-10.1177_27551938241251747 for Does Participating in New Rural Cooperative Medical Insurance Change Catastrophic Health Expenditure? Evidence from the China Household Income Project by Yalu Zhang in International Journal of Social Determinants of Health and Health Services
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.