
Abstract
The COVID-19 pandemic was a global public health crisis that demanded a “whole-of-society” response. In many countries, coordinating efforts across public and private health care sectors proved challenging. Yet South Korea maintained one of the world's lowest excess mortality rates despite having a predominantly privatized health care system, with 90.3% of hospital beds privately owned. This outcome was enabled in part by the government's strategy of disproportionately mobilizing and repurposing public hospitals as dedicated COVID-19 treatment facilities. These hospitals, historically few in number, chronically under-resourced, and marginalized as safety nets for vulnerable populations, became the backbone of Korea's health care system response. This qualitative study examines how this process unfolded and its consequences for public hospitals and marginalized populations they serve, drawing on in-depth interviews with public hospital staff and community activists, complemented by publicly available government reports and administrative data. Our findings reveal that the repurposing of public hospitals was carried out through a highly centralized, top-down process with minimal coordination, inadequate legal safeguards, and no institutional protection. This approach generated short-term gains but ultimately led to reduced patient trust, financial instability, and a staffing exodus that compromised the long-term capacity of the public health sector.
The COVID-19 pandemic was a global public health crisis that necessitated a “whole-of-government” or “whole-of-society” approach, as advocated by the World Health Organization (WHO). 1 Within the context of national health care systems, this requires the swift mobilization of resources and capacities from both the public and private health care sectors to effectively curb the spread and mitigate the impact of COVID-19. However, engaging private medical institutions in national pandemic responses has been a significant challenge worldwide, in both high-income country (HIC) and low- and middle-income country (LMIC) contexts.
Research in Greece found that despite government efforts to encourage private sector participation, these measures were largely unsuccessful. 2 Instead, private hospitals experienced revenue growth and record profits during the pandemic, raising concerns about profiteering. 2 Similarly, a United Kingdom-based study revealed that even with substantial government funding, private hospitals contracted by the National Health Service (NHS) prioritized private patients over NHS patients. 3 In Italy, declining public funding for the NHS between 2010 and 2017, coupled with increasing privatization, resulted in staff reductions, hospital closures, and a weakening of essential emergency services. As a result, both the public and private health sectors were ill-prepared for the COVID-19 pandemic; despite being contracted to support the NHS, the private health sector remained limited as it lacked expertise in delivering complex and costly emergency care. 4 Similarly, in LMICs, including Bangladesh, Ghana, Nepal and Nigeria, private medical institutions have reduced services or refused COVID-19 patients due to financial risks and safety concerns, directly affecting access to care for vulnerable populations. 5 Williams and colleagues 6 argue that the multiple crises faced by the private health sector in LMICs during the COVID-19 pandemic were rooted in pre-existing market failures in their privatized health care systems, underscoring the limitations of market-driven health care delivery, especially during a global health emergency.
Existing literature suggests that heavily privatized health care systems face significant limitations, as the profit-driven nature of the private sector often conflict with the need for a coordinated and equitable response in times of crisis. However, South Korea (hereinafter “Korea”) appears to diverge from this pattern in terms of outcomes. According to previous studies, Korea was among the countries with the lowest levels of excess mortality during 2020–2021, despite having a predominantly privatized health care system, with 90.3% of hospital beds in the private sector. 7 This success was accomplished without overwhelming the health care system or resorting to draconian lockdowns. While Korea's low excess mortality has been widely attributed to timely governmental response, widespread testing, extensive use of information and communication technologies for contact tracing and quarantine enforcement, and strong public cooperation, 8 less attention has been paid to how the medical care sector was organized and governed. In particular, it is important to understand how COVID-19 patient care was delivered in a predominantly privatized health care system with limited public hospital capacity.
In this study, we analyze Korea's health care system response, which we define as the institutional configuration and state coordination of medical care delivery across both public and private sectors. As widely documented in policy and media reports, this response was implemented largely through the disproportionate mobilization of the country's historically under-resourced and marginalized public hospitals. This strategy involved evacuating and repurposing public hospitals into dedicated COVID-19 facilities, effectively creating “COVID-free zones” in the private health sector. Taking this policy approach as our analytical point of departure, we aim to investigate how this strategy was operationalized in practice and to analyze its short- and long-term consequences for public hospitals and the vulnerable populations they serve.
While international literature has highlighted the limited engagement or resistance of private medical institutions in pandemic response efforts, the implications for the public health sector remain largely underexplored. This gap is understandable in contexts where public medical institutions constitute the backbone of service delivery, as in many HICs. For instance, in 2020, public hospitals accounted for 66.3% of total hospital beds in Greece, 100% in the United Kingdom, and 63.7% in Italy. 9 In contrast, countries like Korea present a markedly different institutional landscape, with 90.3% of hospital beds located in the private sector. In such settings, the government's failure to effectively mobilize private providers during the pandemic may carry significant long-term consequences for the public health sector. In Korea, this placed a disproportionate burden on public hospitals, which have been already under-resourced safety nets for vulnerable populations, exposing deep structural inequities and raising urgent ethical questions. It is this underexamined dynamic that our study investigates.
We aim to address a critical gap in the literature by examining the process and impact of the disproportionate mobilization of public hospitals in Korea during the COVID-19 pandemic. By tracing how this strategy unfolded and what consequences it generated, our analysis contributes to broader debates on health system resilience and reform, particularly in contexts characterized by high levels of privatization.
The Privatized Health Care System of Korea
Since 1989, when mandatory health insurance was expanded to cover the entire population in Korea, the National Health Insurance Service (NHIS) has functioned as a single-payer system, requiring the participation of all health care providers, both public and private.10,11 However, health care services are predominantly delivered by private institutions, with publicly owned hospitals accounting for only 6% of the approximately 4100 hospitals nationwide as of 2022. These include 231 institutions, ranging from general hospitals like those affiliated with national universities, municipal medical centers, Red Cross hospitals, and the National Medical Center, to specialized hospitals serving specific medical conditions or patient groups, such as psychiatric hospitals and veterans’ hospitals. Among these, only 41 public hospitals, including 35 municipal medical centers and six Red Cross hospitals, function as crucial “community hub hospitals,” providing essential health care services to their local populations.
The current dominance of the private sector in Korea's health care system can be traced to the state's response to the increased demand for medical services following the implementation of universal health coverage. Instead of investing in the capacity and quality of public hospitals, the Korean government facilitated the rapid expansion of private medical institutions by offering financial incentives, providing loans, and easing regulations on hospital bed distribution across regions.12,13 Consequently, as of 2020, Korea had the highest number of hospital beds among the Organisation for Economic Co-operation and Development (OECD) countries, with 12.65 beds per 1000 people, yet the lowest proportion of those beds in public hospitals, at only 9.7% (see Figure 1).
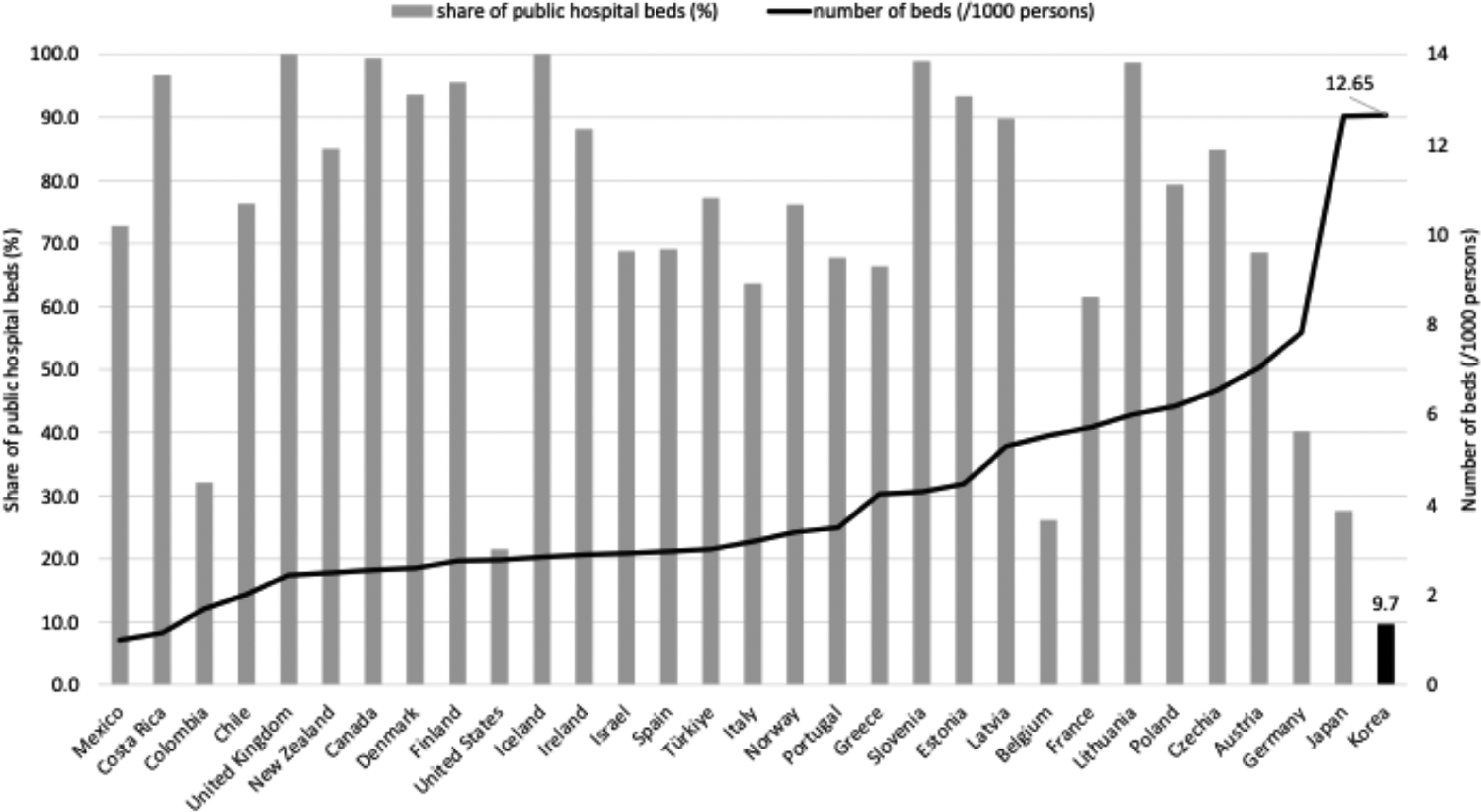
Hospital beds per 1000 population and public sector share in OECD countries, 2020. Data source: OECD Data Explorer, Hospital beds by sector, accessed on February 17, 2024.
Korea's Health Care System Response to the COVID-19 Pandemic
Unlike many countries that adopted early at-home care policies for COVID-19 patients, Korea relied primarily on facility-based care until October 2021. COVID-19 patients were hospitalized or accommodated in community treatment centers specifically established for mild or asymptomatic cases. Consequently, Korea initially saw an extremely high hospitalization rate for COVID-19, exceeding 90%. While this rate steadily decreased, it remained notably higher than in other countries. As of November 2021, Korea's hospitalization rate was 20.2%, significantly surpassing rates in the United Kingdom (4.6%), Singapore (7.0%), and Japan (13.8%). 14
Korea's facility-based strategy involved repurposing entire hospitals or wards into dedicated infectious disease facilities, effectively segregating COVID-19 patients. This required transferring non-COVID-19 patients to other facilities or discharging them early to accommodate the influx of COVID-19 cases. Although public hospitals accounted for less than 10% of the country's total hospital bed capacity, they absorbed a disproportionately large share of the national COVID-19 caseload in the early stages of the pandemic. Figure 2 presents the percentage of all COVID-19 beds nationwide that were designated to public hospitals and the percentage that were occupied in public hospitals each year from 2020 to 2022. In 2020 alone, public hospitals were responsible for 87.5% of all designated COVID-19 beds and 89.0% of beds actually occupied, underscoring the extent to which the burden was concentrated within Korea's limited public hospital capacity. 15
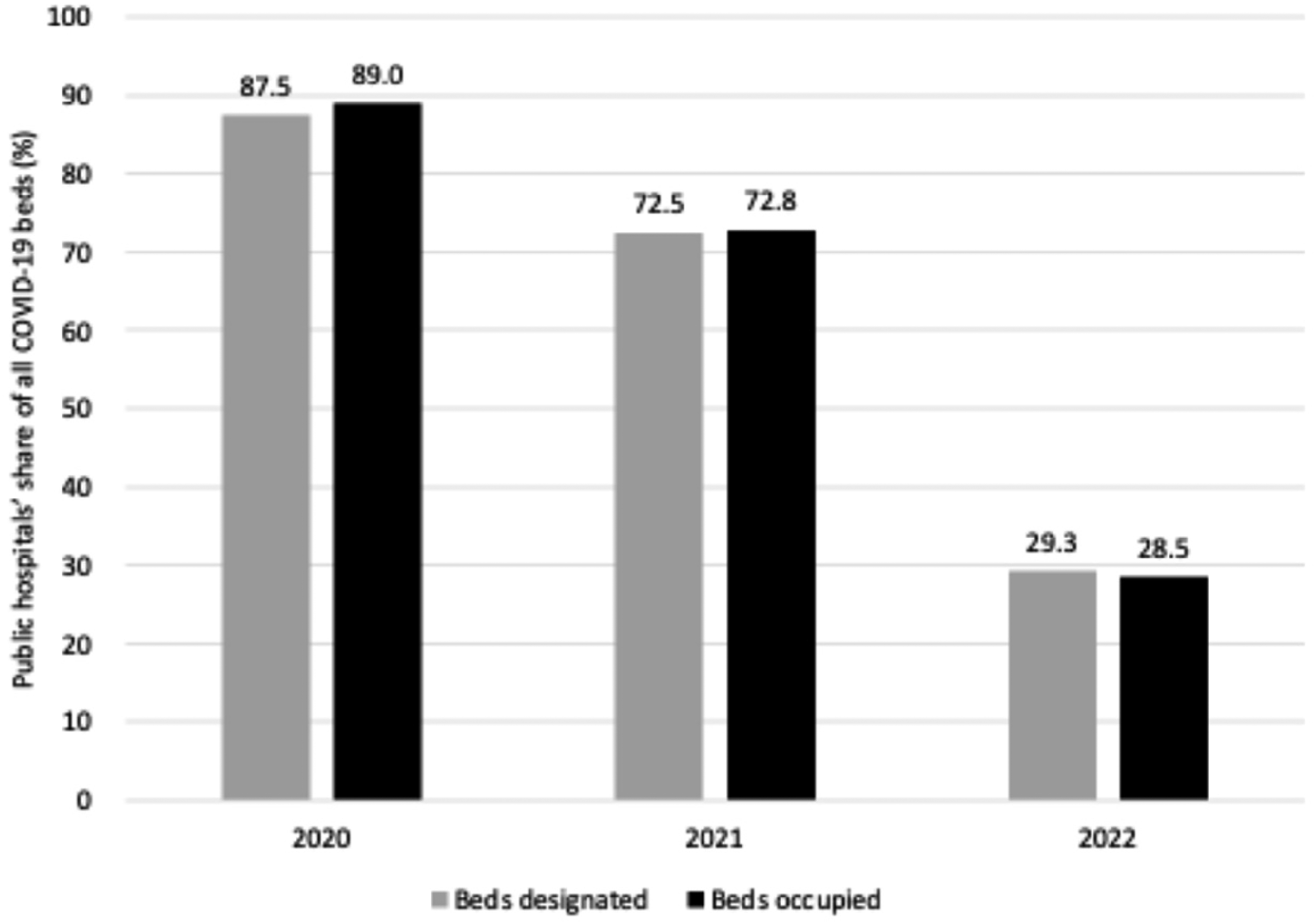
Public hospitals’ share of all COVID-19 beds designated and occupied in Korea, 2020–2022. Note. Adapted from “Chapter 6. Medical Response to the COVID-19,” by M. H. Kim, in S. I. Cho (Ed.), Evaluation on COVID-19 Response Part 2 (p. 294), 2024, Ministry of Health and Welfare and Seoul National University. Data from Central Disaster Management Headquarters. Adapted with permission.
Method: Qualitative Data Collection and Analysis
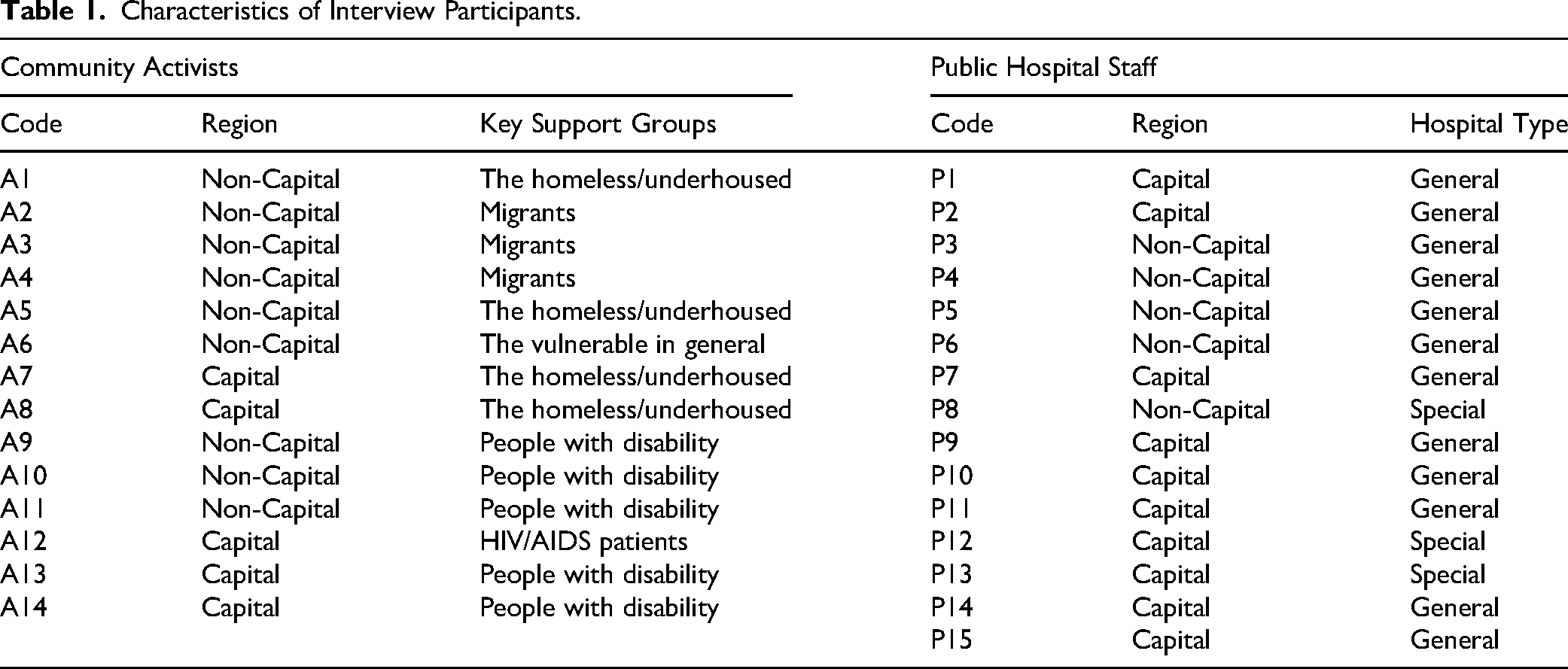
This study is part of a broader qualitative research project examining Korea's health care system response to the COVID-19 pandemic, with particular attention to how the response affected both public hospitals and the socioeconomically marginalized populations, for whom these institutions often served as the sole source of accessible care. Between June and September 2021, we conducted semi-structured interviews with 14 community activists and 15 staff members from 11 public hospitals that had been designated as dedicated COVID-19 facilities (see Table 1). The interview guide used to facilitate these interviews is included in the Supplemental materials.
Characteristics of Interview Participants.
While the broader project draws on perspectives from both community and institutional actors, this article focuses specifically on the interviews with public hospital staff. Insights from interviews with community activists have been analyzed and published elsewhere, in a separate article examining how the evacuation of public hospitals affected access to care for vulnerable populations. 16 In this article, we analyze how the disproportionate mobilization of public hospitals was operationalized during the pandemic and explore its consequences for public hospitals and the patients they serve.
Participants were recruited from both the greater Seoul area and other regions to ensure diverse perspectives. Public hospital staff included directors, care coordination and quality managers, and frontline clinical personnel with extensive experience in pandemic response and supporting vulnerable populations. The corresponding author of this study leveraged professional networks to identify potential participants and expanded the sample through referrals, using a snowball sampling method. Recruitment ceased once data saturation was reached, meaning that interviews began to yield recurring themes and no new insights emerged. All interviews were transcribed and analyzed using a reflexive thematic approach, guided by iterative coding and interpretive engagement with the data.17–19 To contextualize our analysis and support the interpretation of interview data, we drew on publicly available policy documents and descriptive statistics. These materials were used not as standalone data for analysis, but as supplementary references to enrich our understanding of the broader policy environment and inform our interpretation of the interview narratives. Ethical approval was obtained from the National Medical Center Research Ethics Committee (approval no. NMC-2021-06-078) on June 25, 2021.
Results
The Fragile Foundation: Public Hospitals in the Pre-Pandemic Era
Participants’ accounts of the pre-pandemic roles of public hospitals provide critical insight into how these institutions were positioned within Korea's health care system. These accounts help explain why the government disproportionately repurposed public rather than private hospitals as COVID-19 facilities, and why this decision had such far-reaching implications for both public institutions and the marginalized populations they primarily serve.
Participants emphasized that public hospitals, though often underappreciated, play a vital role in their communities. They described these institutions as providing essential care and prioritizing appropriate treatment over profit, setting a standard for responsible and ethical health care. 20 Public hospitals also function as a safety net for vulnerable populations and underserved communities, as one public hospital director (P1) explains: “In public health care, one of our longstanding, core roles has been to care for vulnerable patients—the very individuals often turned away by private hospitals. From the past to the present, this role has been universally recognized and firmly established, without any debate or controversy.”
According to participants, the concentration of vulnerable populations within public hospitals reflects a complex interplay of policy, systemic, and cultural factors. For instance, individuals experiencing homelessness often rely on “Homeless Tier 1” benefits, which severely restrict their access to designated medical facilities. These facilities are predominantly public hospitals, leading to situations described by one public hospital director (P7): “When a homeless person is found, they almost always end up here. Whether it's 911 picking them up or someone finding them collapsed in front of a private hospital, we get the call, and they’re brought here to us.” This concentration creates a hospital environment where certain populations become the norm, fostering a sense of belonging and acceptance. As one public hospital director (P1) explains, “There are plenty of people just like them here, so they feel at ease right away.”
However, participants emphasized that the concentration of marginalized groups in public hospitals reflects not only patterns of access but also deeper systemic failures, particularly the lack of adequate community-based care. Interviews revealed that public hospitals have long been burdened with filling a “social care” gap, often accommodating individuals with complex social needs who might be better served by nonmedical, community-based resources. According to participants, many of these patients are not hospitalized for acute medical conditions, but they return repeatedly due to unmet social needs such as housing insecurity or lack of caregiving support, or the absence of stable social networks. Participants pointed to broader systemic issues, particularly chronic underinvestment in community-based care and the erosion of informal family support, as key structural factors that have pushed social responsibility onto already resource-strained public hospitals.
While participants emphasized that public hospitals were overburdened by having to fill persistent social care gaps, they also described these vulnerable patients as paradoxically serving as a crucial source of stable occupancy in otherwise underutilized and underfunded facilities. Even prior to the pandemic, participants described their institutions as grappling with chronic financial strain. Several directors pointed to a decade of operating deficits (P1) and recurring wage arrears (P7) as clear indicators of systemic underfunding. One director (P6) captured the dilemma vividly: “This public hospital is tasked with caring for socioeconomically vulnerable groups, yet we’re also expected to compete with [private hospitals]. Just because we serve the underserved doesn’t mean the government fully funds us. We’re left to fend for ourselves.” These accounts reflect the structural tension between the social mandate of public hospitals and the financial constraints they operate under. Participants attributed these pressures not only to inadequate public funding but also to structural disadvantages such as remote locations and low patient volumes, which limited revenue opportunities and weakened their capacity to provide a comprehensive range of medical services. In this context, repeated admissions of patients with unmet social needs, though not medically necessary, became one of the few consistent sources of patient volume and revenue. As one director (P2) put it, “We rely on vulnerable individuals to maintain occupancy; without them, our beds would remain empty.”
Taken together, participants’ accounts reveal a paradox at the heart of Korea's health care system: the very public hospitals that were chronically underfunded and structurally disadvantaged were also those the government turned to first when the pandemic struct, not despite their weakness but partly because their lack of power and resources made them easier to mobilize. This fragile pre-pandemic foundation, marked by resource scarcity, systemic neglect, and a reliance on marginalized populations for financial survival, predisposed these hospitals to carry an unequal share of the pandemic burden. The section that follows examines how this burden unfolded in practice, as public hospitals were rapidly evacuated and repurposed with minimal support or coordination.
Evacuating Public Hospitals to Meet the Initial Surge
Top-Down Order: Public Hospitals Evacuated Within One Week. During the first two years of the pandemic, Korea adopted a facility-based care strategy, heavily reliant on repurposing existing public hospitals, often already strained, into dedicated COVID-19 treatment centers. The government enforced the evacuation of these hospitals with minimal consultation, leaving them to grapple with the challenges of adaptation on their own. One public hospital director (P1) described the abrupt process, stating, “We received a sudden call from the Ministry of Health and Welfare, gathered as instructed, and signed a memorandum giving us one week to clear all our hospital beds.” This top-down directive forced public hospitals to transfer or prematurely discharge non-COVID-19 patients to accommodate the influx of COVID-19 cases.
The core problem is not the mobilization of public hospitals during a public health emergency, but rather the unequal burden placed on already strained public hospitals, particularly municipal medical centers and Red Cross hospitals functioning as community hub hospitals. Many public hospitals were confronted with a challenging “all-or-nothing” decision due to outdated infrastructure that made it impossible to safely isolate COVID-19 patients from other patients (P8, P15). The inability to simultaneously treat both COVID-19 and non-COVID-19 cases forced them to prioritize one group, leaving the other underserved.
In contrast, private hospitals, which held the majority of the nation's hospital beds, resisted treating COVID-19 patients. This reluctance to share the burden frustrated public hospitals: “We kept telling the government that other hospitals needed to start opening beds [for COVID-19 patients]. But it wasn’t until the situation had deteriorated so badly—until we were absolutely overwhelmed with patients—that the government finally took action to open beds in other hospitals. Honestly, if the patient numbers hadn’t surged the way they did, if things hadn’t reached that crisis point, they probably wouldn’t have opened them at all” (P4). “By this point, we’ve learned a lot about COVID-19. Now that we understand it's more like a cold or the flu, I really believe other [private] hospitals should also be taking in COVID-19 patients” (P5).
Multiple participants described the government's eventual mandate for private hospital participation as coming far too late, only after public hospitals had been pushed to the brink. Participants interpreted this delay as a reflection of the state's reluctance to interfere with private hospital autonomy. This view is consistent with the government's actual timeline: five executive orders were issued in the final two months of 2021 to mobilize private hospital beds, narrowly averting repeated system collapse. 21 These accounts underscore the difficulties of coordinating an effective health care system response in a system dominated by private institutions. As Figure 3 illustrates, because government compensation was tied to hospitals’ pre-pandemic revenue, engaging private hospitals during the pandemic required significantly greater financial outlays than was required for public hospitals. 22 This fact underscores a critical governance dilemma: in a health care system dominated by private ownership, mobilizing private institutions in a public health emergency demands enormous public spending. Without substantial financial incentives, the state struggles to align private sector priorities with collective public health needs.
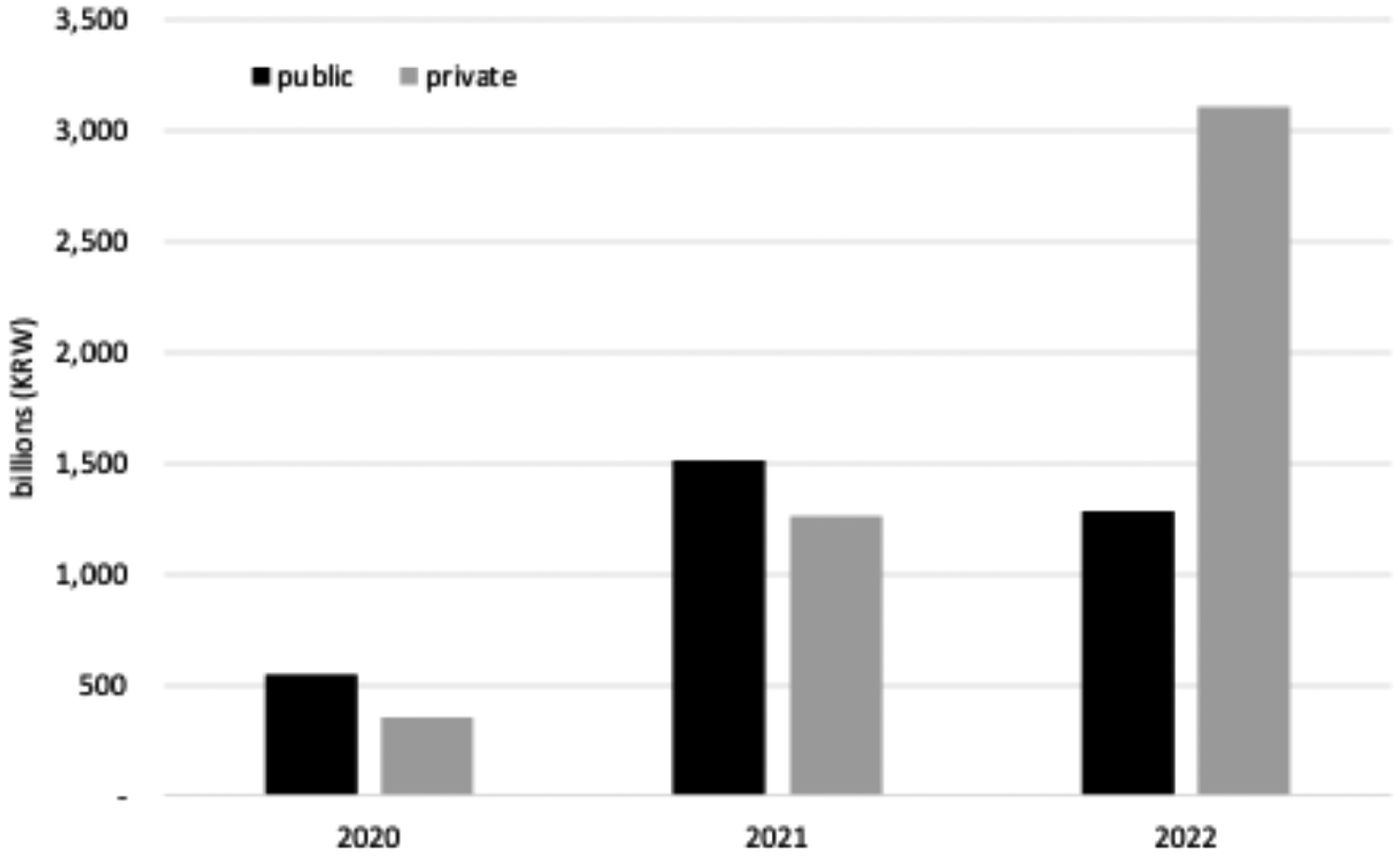
Government compensation for hospital losses during the pandemic. Note. Adapted from “Chapter 6. Medical Response to the COVID-19,” by M. H. Kim, in S. I. Cho (Ed.), Evaluation on COVID-19 Response Part 2 (p. 294), 2024, Ministry of Health and Welfare and Seoul National University. Data from Central Disaster Management Headquarters. Adapted with permission.
Left in the Lurch: No Protection, No Coordination. In addition, public hospitals faced considerable legal risks as they hastily discharged and transferred patients to comply with government directives, without any legal safeguards in place. A notable example is a lawsuit filed by a patient discharged prematurely without adequate postoperative care, leading to alleged health complications (P4). In another instance, the closure of a public hospital's emergency room resulted in a patient's death after being transferred elsewhere, prompting a lawsuit from their family (P9). Furthermore, hospitals received complaints about patients being discharged “without guardian consent,” a particularly concerning issue when guardians of vulnerable, isolated patients could not be reached on short notice (P11).
The government's lack of coordination in patient evacuations from public hospitals led to widespread chaos and complications. Hospitals were left to grapple with the challenges independently, with staff relying on informal networks to secure patient transfers to neighboring facilities. One public hospital physician (P9) expressed frustration, stating that, “the government should have mandated other [private] hospitals to accept transfers unconditionally, rather than leaving us to plead for cooperation.” This statement highlights the absence of effective governmental coordination and support, which placed an unfair burden on already under-resourced public hospitals.
Struggles to Transfer Vulnerable Patients. The urgent discharge or transfer of existing inpatients from public hospitals during crises exposed a stark contrast in experiences. While patients with mild conditions and no socioeconomic disadvantages faced only logistical challenges, socioeconomically vulnerable populations—often deemed unprofitable by private hospitals—faced immense hurdles finding alternative care, leaving them stranded in public hospitals until the last possible moment. These individuals included those living in poverty, undocumented migrants, those battling stigmatized diseases, or those with complex medical conditions requiring specialized care. Public hospital officials recounted the struggles involved in transferring such patients, citing examples like: a migrant with tuberculosis (P3), a bedridden patient following a suicide attempt whose medical bills were not covered by insurance and who lacked a guardian to assist with payment (P11), a bedridden patient with pressure sores requiring a feeding tube (P15), and a migrant patient hospitalized for over 100 days after being abandoned by their family who returned to their home country (P14).
Moreover, patients were often reluctant to transfer to private hospitals due to concerns about increased out-of-pocket costs. While public hospitals offered financial assistance programs for medical and nursing fees, these benefits were not transferable between institutions, creating a significant barrier for patients needing to relocate. Many opted for premature self-discharge, stating they “could not afford the additional financial burden” (P10). Paradoxically, public hospitals faced administrative challenges due to the non-portability of their financial assistance programs, leaving them unable to fully utilize their allocated budgets while the needs of vulnerable populations remained unmet. To further explore how this situation affected health care access for vulnerable populations, see the authors’ related study. 16
Becoming Dedicated COVID-19 Hospitals: Process and Consequences
Participants described how their hospitals were designated as dedicated COVID-19 facilities for extended periods throughout the pandemic. As context, by March 2022, 40 of 41 community hub hospitals had received this designation at least once, with an average duration of 628 days. 23 This prolonged designation fundamentally reshaped hospital operations, management priorities, and patient demographics. Participants reflected on how these changes affected their work, their institutions, and the vulnerable populations who depended on them.
Short-Term Gains, Long-Term Losses for Public Hospitals. Participants noted that being repurposed during the pandemic temporarily boosted the image and visibility of public hospitals. Several observed that support for publicly funded health care grew during the pandemic. Survey data confirmed this sentiment, revealing greater public endorsement of public health care and increased calls for expanding public hospitals.24,25 Some participants acknowledged the temporary financial reprieve from government compensation. One director even stated, “the COVID-19 pandemic saved financially struggling public hospitals” (P7), which was attributed to the government's compensation policy that initially calculated payments based on national average revenue per occupied bed for general hospitals. As a result, some public hospitals received a substantial financial boost, offering a temporary respite.
Yet many participants emphasized that these short-term financial gains came at the cost of long-term sustainability. Repeated evacuations, whether prompted by case surges or policy directives, strained hospital capacity and drove medical staff to seek more stable positions in private hospitals. Participants also noted that the constant threat of future evacuations undermined patient trust. Patients hesitated to return, fearing abrupt discharges during future outbreaks. This erosion of trust ultimately led to financial losses and a shrinking patient base. These concerns echoed hard-learned lessons from past epidemics. One hospital director (P9), reflecting on the 2015 MERS outbreak, recounted how their 400–450 bed facility had been emptied to accommodate just 10–20 MERS patients: “It took nearly two years to rebuild the patient base, and there was no compensation or recognition for the hospital's sacrifices.”
Interview data pointed to a widespread perception that COVID-related displacement had lasting consequences. This was corroborated by administrative data; by June 2023, the average bed occupancy rate in 35 municipal medical centers had fallen to 46.4%, compared to 80.5% in 2019. 26 Outpatient visits similarly declined, dropping 22% from 789.2 in 2019 to 613.5 in June 2023. 26 Financial indicators reflect the toll of this diminished patient volume. For instance, the National Medical Center's net deficit surged from KRW 34 billion in 2019 to KRW 72.7 billion in 2022. 27 Figure 4 illustrates the financial impact across 32 community hub hospitals, where average medical revenues fell from 35.9 billion KRW in 2019 to 25.1 billion KRW in 2020. While partial recovery occurred, revenue remained below pre-pandemic levels even as medical costs rose, deepening financial instability. Medical losses surged from 4 billion KRW in 2019 to 15.7 billion KRW in 2020, with little improvement since.
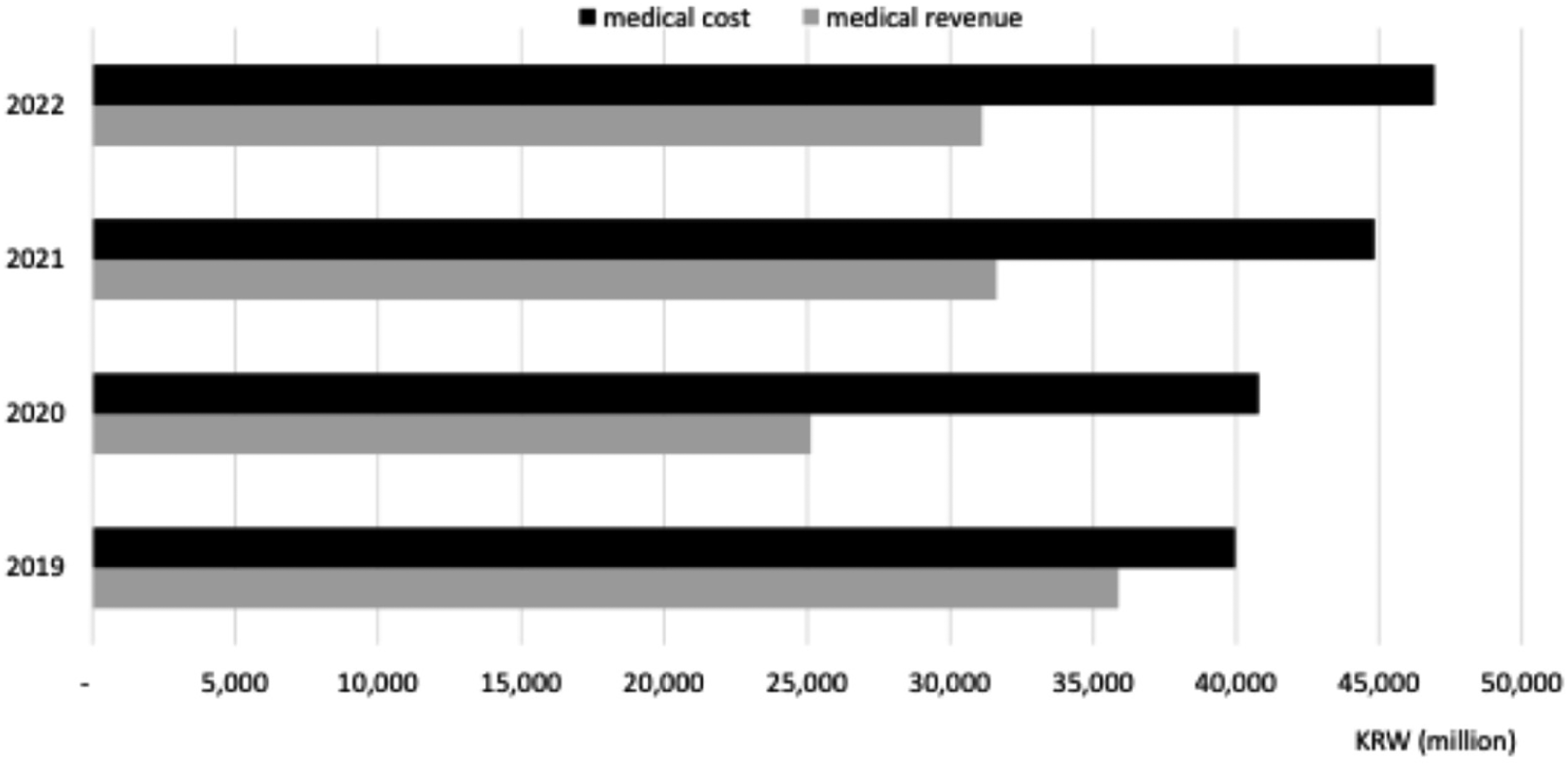
Annual average medical revenue and costs for 32 community hub hospitals, 2019–2022. Data source: Korea Health Industry Development Institute, Disclosure of Healthcare Institution Finances, accessed on August 13, 2024.
Although overall health care utilization declined during the early pandemic, municipal medical centers experienced a more sustained and pronounced decline than comparable private hospitals. Figure 5 highlights the disproportionate drop in hospitalizations at public hospitals, particularly beyond the spring of 2020. 28
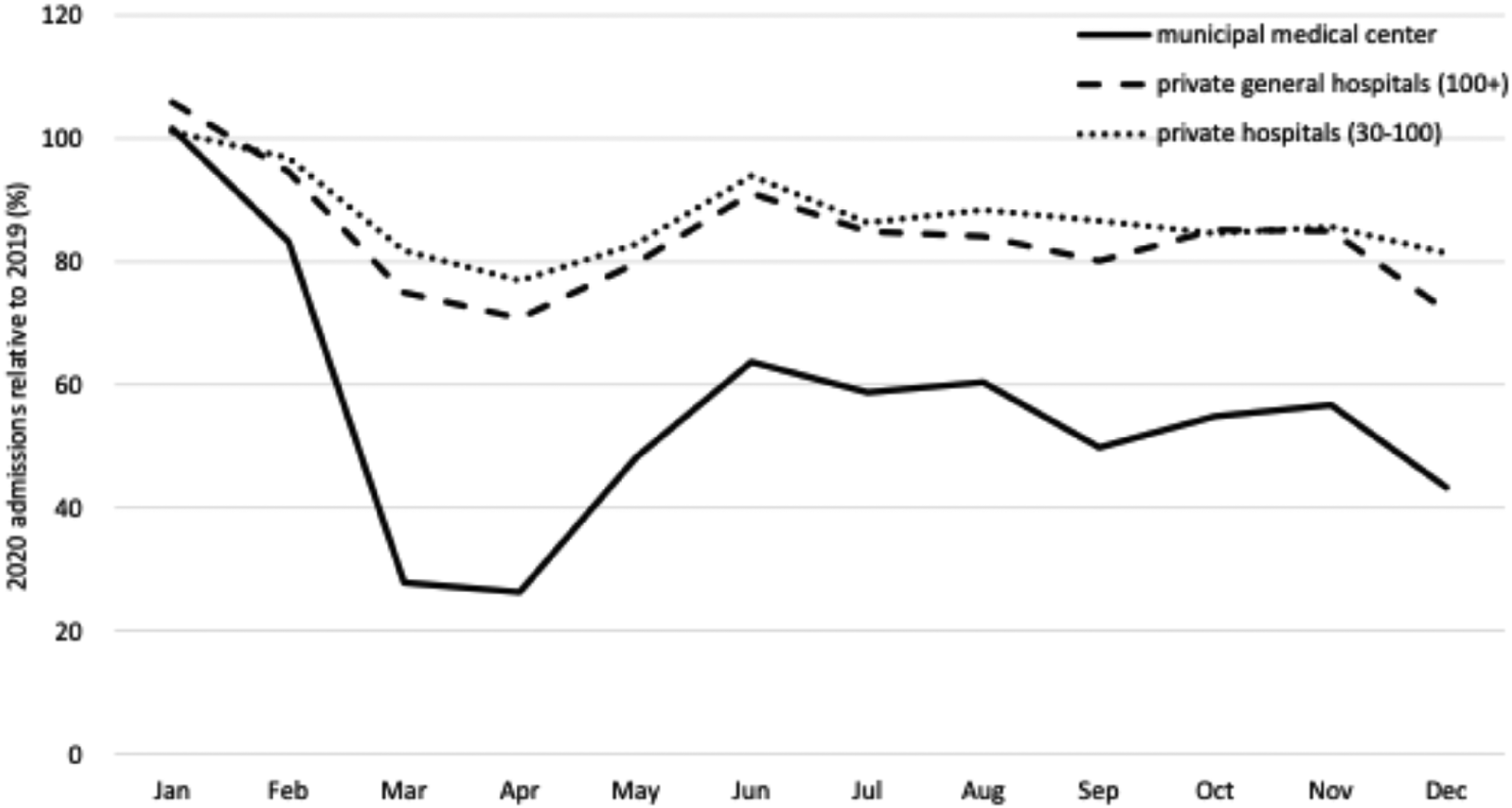
Comparison of 2020 hospital admissions to 2019 baseline, by hospital ownership and bed size. Note. Adapted from Figure 10 (p. 247) in Unmet Medical Needs among Vulnerable Populations during the COVID-19 Pandemic and Development of Policy Alternatives, by the authors of this article, 2022, National Medical Center. Data source: National Health Insurance Database. Private general hospitals exclude teaching hospitals affiliated with medical schools.
Quality of Care Compromised During the Pandemic. Participants emphasized that even when public hospitals continued offering outpatient services alongside COVID-19 care, it was difficult to maintain service quality. Directors described how traditional compensation systems, which combined seniority-based salaries with performance metrics linked to patient volume, created internal tensions. As outpatient visits declined, physicians expressed concern that their performance evaluations and income would be negatively affected. In response, directors implemented staff rotations between COVID-19 wards and outpatient clinics to distribute workload and preserve physicians’ compensation eligibility. However, these frequent rotations disrupted continuity of care and reduced physicians’ sense of responsibility for individual patients. One director (P2) noted, “Patients had to see different doctors at each visit.” Participants reported that this fragmentation sometimes led to superficial encounters, such as prescription refills being issued without proper patient assessments, which contributed to patient dissatisfaction and reduced return visits.
Staff Exodus from Public to Private Hospitals. The prolonged designation of public hospitals as dedicated COVID-19 facilities has impacted staffing levels. Data from 32 municipal medical centers and four Red Cross hospitals showed that hospitals designated as dedicated COVID-19 facilities for over 400 days suffered significant declines in both physician retention and recruitment. 23 Between 2019 and 2021, larger hospitals (250 + beds) saw a 7.4% drop in total physician numbers and a 28.8% decline in new physician appointments. Smaller hospitals experienced a 2.9% drop in physician staffing and a stark 53.2% decline in new physician appointments.
These numbers align with the perspectives shared by hospital directors, who cited dissatisfaction, skill deterioration, and reduced professional fulfillment as key drivers of attrition. One director (P1) lamented the loss of hard-to-recruit specialists, stating, “The urologist, orthopedic surgeon, and dental specialist all left” (P1). Another public hospital physician (P11) explained: “When there's nothing meaningful to do, how can any doctor find purpose or satisfaction here? These aren’t even my own patients . . . . It's not even my area of expertise. Just sitting there—I can’t magically become a pulmonology expert overnight. And for surgeons, if they go years without stepping into an operating room, why would they stick around? Medicine moves fast . . . . Take a few years off, and you’re left behind.”
This inability to practice their specialties or maintain clinical competence further diminished physicians’ motivation to remain in public hospitals.
Discussion
This study examined how public hospitals in South Korea were mobilized as dedicated COVID-19 treatment facilities and the consequences of this strategy. Our findings highlight three interrelated themes. First, public hospitals entered the pandemic from a position of structural disadvantage. Interviews revealed that these institutions were chronically underfunded, financially precarious, and relied on marginalized populations to sustain patient volumes. Public hospitals routinely filled social care gaps created by insufficient community-based services, reinforcing their role as de facto safety nets. Second, public hospitals were disproportionately and abruptly repurposed during the pandemic, often under top-down directives with little coordination or support. This led to the displacement of existing patients, particularly those with complex social or medical needs, and placed legal and logistical burdens on public hospital staff. The private sector's delayed and limited participation further intensified pressure on public institutions. Administrative data corroborated participants’ accounts, showing lasting declines in patient volume and institutional revenue. Third, while some participants noted short-term gains, such as improved public visibility, temporary financial relief, and greater public support, these gains were offset by long-term losses. Public hospitals struggled to maintain service quality due to staff rotations and experienced sustained erosion of patient trust and physician retention. Hospitals designated as COVID-19 facilities for extended periods reported declining physician numbers and difficulties recruiting new staff. Taken together, these findings reveal how Korea's pandemic response both exposed and intensified existing structural weaknesses in Korea's health care system, particularly the challenges that arise when under-resourced public hospitals are expected to shoulder a disproportionate share of critical public health functions in a system dominated by private providers.
These findings challenge the prevailing narrative of Korea's COVID-19 response as an unqualified success, revealing the hidden costs and complexities that lie beneath the surface of the country's relatively low death toll. While previous studies in other HICs have primarily focused on private-sector noncooperation,2–4 our study highlights both the immediate and potential long-term consequences faced by the public health sector in Korea. In contrast to countries with a dominant public health sector, Korea's public hospitals are very small in number and limited in capacity. We situate Korea's unique pandemic response within the context of its preexisting national health care system, critically examining the rationale, implementation, and far-reaching consequences of the strategy that predominantly, if not almost exclusively, mobilized its already constrained public hospitals. The mobilization of public hospitals was characterized by an authoritarian approach, justified in the name of health security, where shared decision making was absent and unilateral compliance with central government directives was enforced.
Our study contributes to scholarship on health care system responses to global health crises by highlighting how Korea's predominantly privatized health care system managed COVID-19 patient care during the pandemic. While existing narratives have praised Korea's overall pandemic response, especially the swift implementation of testing, tracing, and treatment (3 T) strategies,29–33 these accounts often overlook how treatment responsibilities were distributed within the health care system. We draw attention to a critical yet underexamined dimension: the government's heavy reliance on public hospitals, which, despite being underfunded and structurally disadvantaged, were disproportionately repurposed as dedicated COVID-19 facilities. This reliance came at a significant cost to both the institutions and the vulnerable populations they serve. While some scholars have pointed to private sector involvement, such as private clinics providing tests and vaccinations, as evidence of successful public-private collaboration, 34 this framing obscures the limited role private hospitals played in COVID-19 patient care. By centering the experiences of public hospital staff, our study offers a more nuanced understanding of Korea's pandemic response and calls into question the long-term sustainability of relying on a small public sector to carry the burden of emergency care in a privatized health care system.
This study is not without limitations. It is based on qualitative interviews conducted between June and September 2021, primarily capturing experiences from the early phases of the pandemic. As such, the findings may reflect the initial contours of public hospital mobilization rather than the full trajectory of Korea's pandemic response. However, to address this limitation and demonstrate that the repurposing of public hospitals was not confined to the early phase, we drew on a range of administrative data sources to contextualize and interpret participants’ accounts. These data help illustrate the continued and prolonged use of public hospitals as dedicated COVID-19 facilities, as well as the evolving consequences of this strategy over time.
Our findings align with the argument of Williams and colleagues 6 that the challenges faced by LMICs with heavily privatized health care systems during the pandemic were not unforeseen results of the crisis itself. Rather, they were predictable outcomes of inherent market and redistributive failures within mixed public–private models. Korea's pandemic response exemplifies this pattern, reflecting a path deeply rooted in the historical development of its privatized health care system and the complex interplay of actors within it. 35 The state's actions were constrained by the market-driven structure of the health care system, its relationship with private providers, and prevailing ideologies. These factors limited the government's strategic options during crises like COVID-19, effectively confining its actions to mobilizing public hospitals. The prevailing belief that states cannot infringe upon private property precluded the direct mobilization of private resources, necessitating substantial financial incentives to involve private hospitals.
Our study challenges the prevailing literature on successful pandemic responses, which often emphasizes government capacity and political legitimacy. For instance, Christensen and Lægreid 36 argue that both government competency and citizens’ trust in government are critical factors in Norway's successful pandemic response. Similarly, Asthana and colleagues 37 suggest that Singapore's centralized administration and efforts to gain public trust enabled an agile government response. However, our analysis of the Korean case reveals a potential conflict between the pursuit of public trust and the protection of vulnerable populations during public health crises. While the Korean government endeavored to cultivate public trust to facilitate agile decision-making during crises, this approach led to the marginalization of society's most vulnerable populations. This raises a pivotal question: When discussing public trust, who precisely constitutes “the public,” and whose trust are we truly prioritizing?
The Korean government's exertion of authoritarian control over public hospitals, juxtaposed with its historical underinvestment in them, highlights a persistent legacy of the developmental state that characterized Korea from the 1960s to the 1980s.38–40 While the developmental state facilitated rapid industrialization and economic growth, it also prioritized such growth over robust social welfare provisions. 41 This prioritization led to inequalities and underinvestment in social programs, including public health care, leaving these sectors vulnerable in times of crisis. This legacy manifested during the pandemic as the state leveraged its strong capacity for policy implementation to mobilize a swift response, but did so through a top-down approach that disproportionately burdened public hospitals, without addressing their historical underfunding. This authoritarian approach, favoring efficiency and control, left public hospitals and the marginalized communities they serve particularly vulnerable.
A troubling ethical dimension of Korea's pandemic response was its utilitarian orientation, which prioritized population-level health outcomes even at the cost of disproportionately burdening vulnerable populations. This logic was evident in how public hospitals were repurposed as dedicated COVID-19 facilities with little regard for the consequences for existing patients and staff. For example, patients with complex social or medical needs were hastily discharged or left with nowhere to go, while public hospital staff were stretched thin and exposed to burnout and faced professional stagnation as their usual clinical work was suspended. In contrast, private hospitals, which account for the majority of beds in Korea, remained largely insulated from these disruptions. They were slow to participate in COVID-19 patient care and appear to have benefited more from government compensation. This dualized strategy appeared to ensure access to safe health care for the general population during the crisis, reinforcing public trust in the government's pandemic response. By concentrating the burden on already under-resourced public hospitals, the state avoided resistance from powerful actors in the private health sector and a broader legitimation crisis. 42
While this strategy may have been effective in averting system-wide collapse, it obscures serious equity and justice concerns. The long-term consequences for public hospitals, such as loss of patient trust, declining service quality, financial strain, and physician attrition, raise critical questions about whether this approach is ethically and operationally sustainable. Existing ethical debates about pandemic response have largely focused on the tension between restrictive public health measures, such as lockdowns and mask mandates, and individual rights and freedoms.43,44 However, the findings from this study point to the need to also consider issues of distributive justice in resource allocation, particularly in privatized health care systems where private profit motives may run counter to public health priorities. Expanding the ethical lens in this way highlights the importance of designing pandemic preparedness strategies that not only optimize population health outcomes but also ensure that the burdens and benefits of emergency responses are shared fairly across health care institutions and communities.
Conclusion
Our analysis reveals that Korea's success in managing the COVID-19 pandemic was not the result of an effective whole-health-system approach, but rather a reliance on the government's authoritarian control over public hospitals. While effective in containing the virus, this approach had significant long-term consequences, weakening the public health sector and exacerbating existing health inequalities. The decline in public hospital capacity not only represents a step backward from progress toward universal health coverage and the right to health but also threatens the ability to effectively respond to future public health emergencies.
The COVID-19 pandemic revealed significant limitations in health care systems that rely heavily on privatization. The profit-driven nature of the private health sector can clash with the need for a coordinated and equitable public health response during a crisis. It is imperative that the Korean government develop a comprehensive strategy to revitalize public hospitals and reform the national health care system to ensure equitable access to quality health care for all. This strategy must include a robust, health-system-wide approach to future public health emergencies, empowering public hospitals to lead while ensuring the entire health care system, including the private sector, works in concert.
Supplemental Material
sj-docx-1-joh-10.1177_27551938261449602 - Supplemental material for Privatized Health Care System in Times of Crisis: South Korea's Health Care System Response to the COVID-19 Pandemic
Supplemental material, sj-docx-1-joh-10.1177_27551938261449602 for Privatized Health Care System in Times of Crisis: South Korea's Health Care System Response to the COVID-19 Pandemic by Juyeon Lee, Jungwook Kim, Rora Oh, Rangkyung Ha and Myoung-Hee Kim in International Journal of Social Determinants of Health and Health Services
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the interview participants who generously shared their time and insights during this research. Their valuable contributions were instrumental in shaping the findings presented in this article.
Ethical Considerations
This study was approved by the National Medical Center Research Ethics Committee (approval no. NMC-2021-06-078) on June 25, 2021.
Consent to Participate
All participants provided written informed consent prior to participating. All participants provided written informed consent prior to participating.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Medical Center, Seoul, South Korea, (grant number NMC2021-General Research Program-09).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data from this study consist of qualitative interview transcripts and are not publicly available due to privacy and confidentiality restrictions.
Supplemental Material
Supplemental material for this article is available online.
Notes on contributors
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.