
Abstract
In an attempt to avoid the inequitable outcome of the COVID-19 pandemic whereby High-Income Countries received the overwhelming majority of vaccine doses after they became available, the World Health Organization initiated negotiations in December 2021 on a legally binding Pandemic Agreement. This paper uses a variety of documents and personal experience to examine how the Canadian government communicated with its domestic stakeholders about the stances that Canada was taking during the negotiations and to illustrate what positions Canada was advancing at the negotiations table in Geneva. This article argues that the government lacked transparency in its communications and gave no indication that it was listening to the feedback it was receiving. During the negotiations, aside from advancing a progressive position of gender equality, the government pushed to weaken the obligations of countries and the commercial sector to ensure that vaccines, treatments and technology would be available on an equitable basis globally in any future pandemic. Now that the Pandemic Agreement has been adopted by the World Health Assembly, there is still the task of agreeing on an annex on pathogen access and benefit sharing. Past experience suggests that during these negotiations Canada will favor commercial over public health interests.
Keywords
Introduction
In an attempt to avoid the inequitable outcome of the COVID-19 pandemic whereby High-Income Countries (HIC) received the overwhelming majority of vaccine doses after they became available, 1 the World Health Organization (WHO) initiated negotiations in December 2021 on a legally binding Pandemic Agreement. 2 (In various documents the Agreement is also referred to as an instrument, treaty, convention or accord. For the purpose of this article it will uniformly be called an Agreement.) The overarching objective of the Agreement is to help the world “prevent, prepare for and respond to pandemics.”
Primary documentation on the Canadian government's negotiation positions was not publicly available 3 and the negotiating text of drafts of the Agreement on the WHO website 4 was only unmarked up versions so the amendments proposed by the different parties were not available. (Two different versions of the negotiating text with proposed changes were leaked and available on web sites.5,6)
This article uses a combination of media reports and articles, reports and commentaries from civil society organizations, journal articles, government documents and reports and my participation in some events. Journal articles came from a PubMed search using the terms “Pandemic Agreement” and “Canada” and the same terms were used to search the Canadian Newsstream Collection for media reports and articles. If the same issue was mentioned in articles from both sources and there was a difference in content, then the academic source was prioritized. Government documents were accessed from a Canadian government website. 3 Commentaries and reports from civil society organizations such as Médecins Sans Frontières were obtained by directly contacting the organization. My personal participation in events organized by the Canadian government was used to supplement what was contained in the government material.
This combination of material was used to analyze Canada's actions with domestic stakeholders, its positions in the negotiation process during the recently concluded Agreement and what Canada's position is likely to be in the upcoming further negotiations on the annex to the Agreement. Particularly, it looks at the discrepancies between Canada's formal position on the Agreement which was that the government aimed to “improve global cooperation, strengthen collective action and accountability and address gaps in pandemic prevention, preparedness and response” 3 and its support for the interests of the private sector, primarily the pharmaceutical and biotechnology industries.
Public Consultation on Canada's Position in Negotiations
The Canadian government convened a two-day meeting in March 2023 of about 100 representatives of Canadian provinces and territories, Indigenous peoples, youth, civil society, private sector, and academia (and another 100 participants virtually) to “help inform the development of Canada's priorities and objectives in the creation of a pandemic instrument”. 7 But while the meeting was a good first step it was also flawed. There was no evidence in the formal document that summarized the consultation that Health Canada's Office of International Affairs consulted ahead of the two-day event with any of the stakeholders about what issues they wanted to provide feedback on. 8 The questions posed to the attendees, while interesting, seemed to reflect issues that the Office wanted feedback on, rather than issues that the attendees wanted to discuss. The background document only mentioned positive actions that the Canadian government undertook during the pandemic and did not deal with any of the criticisms about the government's actions and inactions. The document also cited a statement made by the International Federation of Pharmaceutical Manufacturers and Associations (IFPMA) about the increase in manufacturing capacity for vaccines without acknowledging the conflict of interest that the IFPMA had in its role as a lobbyist for the international pharmaceutical industry and in discussing the volume of vaccine production. It is also worth noting that it took over 5 months between when the meeting was held (March 21–22, 2023) until when the report was released (August 24, 2023). During that time, the meeting attendees and any other interested members of the public were in the dark about the potential impact of the meeting. 9
When I emailed the Pandemic Instrument Engagement Team and asked directly about the inclusion of the IFPMA statement in a background document, the response did not directly address the question and just said that these documents “were intended to describe the scope of the issues being discussed.” In response to another question about how participants for the consultation were chosen, the response was vague and non-informative. “The event was designed in consultation with departments across the Government of Canada, who have been regularly interacting with partners and stakeholders throughout the COVID-19 pandemic. We also held a number of virtual calls and technical briefings with partners and stakeholders, which helped inform the topics selected for the Forum” (Personal communication, April 5, 2023, Supplementary File 1)
A second in-person series of consultations in various cities across Canada and on-line (one in English and one in French) was held in January-February 2024. This time, the attendees were given more latitude about the topics that were discussed. With the help of an external facilitator, the attendees identified the articles in the Agreement of the greatest relevance to their organizations and for which they most wanted to provide information to Canada's negotiating team. 10 While the range of topics discussed was more flexible than in the first consultation, one analysis of the summary of the consultations concluded that there were subtle differences from the 2023 report on the initial consultation with a bias in favor of comments from representatives of the pharmaceutical industry. 11
Only 4% of the 116 people attending the second consultation in-person and virtually identified as coming from the private sector 10 and it is quite likely that not all of them came from either the pharmaceutical or biotechnology sectors. Despite the low representation from those industries, three articles in the draft Agreement prominently featured industry-friendly comments. For example, in Article 9: Research and Development the report noted that “Public disclosure requirements may discourage private sector research and delay the development of vaccines and therapies.” In Article 11: Technology Transfer and Know-How, the report said that “The weakening of intellectual property rights could have negative impacts on the participation of the private sector.” The summary of the discussion of Article 12: Access and Benefit Sharing said “Between pandemics, we must drive innovation through the retention of IP, but clarity is needed on how far the protection of IP goes.” According to de Beer and De Koker this change to a more industry friendly tone was possibly because the current version of the proposed Agreement text was more industry friendly, because the report was reflective of the positions that the Canadian government was already taking in the negotiations or some combination of these factors. 11
What wasn’t in the two summaries was probably more significant than what was. There was no indication of how Canada used or planned to use the feedback it received in communicating with its stakeholders and in developing its negotiating positions. In many instances, Canada's actions were in direct contradiction to what the majority of the stakeholders advocated. One of the Key Takeaways from the first consultation was that “Transparent processes and decision-making are key to building trust and ensuring equity. Stakeholder input must be represented in the document and acted on in its implementation”. 8 But as the next section shows, this Takeaway was observed mostly in the breach. In many instances what Canada was saying at the negotiating table was directly opposed to what it heard from its stakeholders.
Another main recommendation from the first stakeholder engagement was that “The instrument must promote the sharing of information, data, best practices, expertise and resources”. 8 But during negotiations, Canada, along with other HICs, opposed the original draft text about technology transfer that said “The Parties shall strengthen existing and develop innovative multilateral mechanisms that promote and incentivize relevant transfer of technology and know-how for production of pandemic-related products on mutually agreed terms particularly in developing countries”. 5 Canada's priority was to ensure that any transfer of technology was done on a voluntary basis, ie, that there was no obligation on countries to share knowledge or products.
The first Key Takeaway from the March 2023 consultation was to “Embed Equity in the Process.” “Participants felt strongly that equity must be a primary consideration underpinning all aspects of the Pandemic Instrument and be central to its development process.” Again, Canada seemed to completely ignore that Takeaway, and according to MSF, 12 was the key mover in inserting restrictions on technology transfer in Article 4, the article that defined equity as one of the treaty's guiding principles.5,9
Transparency in Canada's Communications
According to the Canadian government, its engagement with stakeholders about the Pandemic Agreement negotiations “aim[ed] to promote transparency and facilitate meaningful and inclusive engagement”. 13 However, based on my experience and the newsletters circulated by the Pandemic Instrument Engagement Team that was not an entirely accurate description of how the government acted. Over the course of the consultations there were 7 newsletters issued between Winter 2023 and March 2025. These newsletters outlined in broad terms the state of the negotiations on various articles in the Agreement and indicated areas where Canada was active, but they did not explain what positions Canada was taking nor whether the feedback that Canada was receiving affected its positions. When I emailed the Pandemic Instrument Team in April 2024 to ask about Canada's position on a particular item the response that I received back a week later said that “Canada does not traditionally comment on positions on active negotiations” (Personal communication, April 22, 2024, Supplementary File 1). Canada's position was in marked contrast to that of the European Union which proactively published its proposals on technology transfer and other articles in the Zero Draft of the Pandemic Agreement. 14
Ahead of the initial consultation in March 2023, the Director General of the Office of International Affairs for the Health Portfolio promised to “continue to engage with a diverse range of partners and stakeholders throughout the development of the pandemic instrument”. 8 However, although the Pandemic Instrument Team continued to issue the newsletters referred to above and asked readers to provide feedback on issues being negotiated, the newsletters never said how the feedback was received or whether it affected the positions that Canada took in the negotiations. Finally, the January-February 2024 consultation was the last in-person event held by the Pandemic Instrument Team, before Agreement negotiations concluded in mid-April 2025, although there was a virtual event in January 2025.
Canada's Position on Text in the Agreement
According to bodies such as the United Nations Framework Convention on Climate Change, one of the core principles that should underwrite any Agreement is the acceptance of “common but differentiated responsibilities” (CBDR). 15 The principle holds that those with greater culpability, capability, and less vulnerability must step up and take the responsibility in addressing any future pandemic. Habibi and Wenham noted that “while some entities see CBDR as the key to achieving health equity among the world's nations, others, including Canada, view it as a divisive and unworkable concept in global health law”. 15
Medecins sans Frontieres (MSF, Doctors Without Borders) analyzed Canadian amendments to an early draft of the Agreement.
5
(Table 1 shows the proposed changes Canada made to different drafts of the negotiating text.) According to MSF, Canada seem[ed] more insistent than any other country—except possibly the U.S.—that any tech transfer under the pandemic treaty take place on voluntary and/or mutually agreed terms. In other words, even in a pandemic, the maker of a life-saving vaccine or drug would have had no obligation to help [other countries access its vaccine].
Proposed Canadian Changes to Negotiating Drafts.
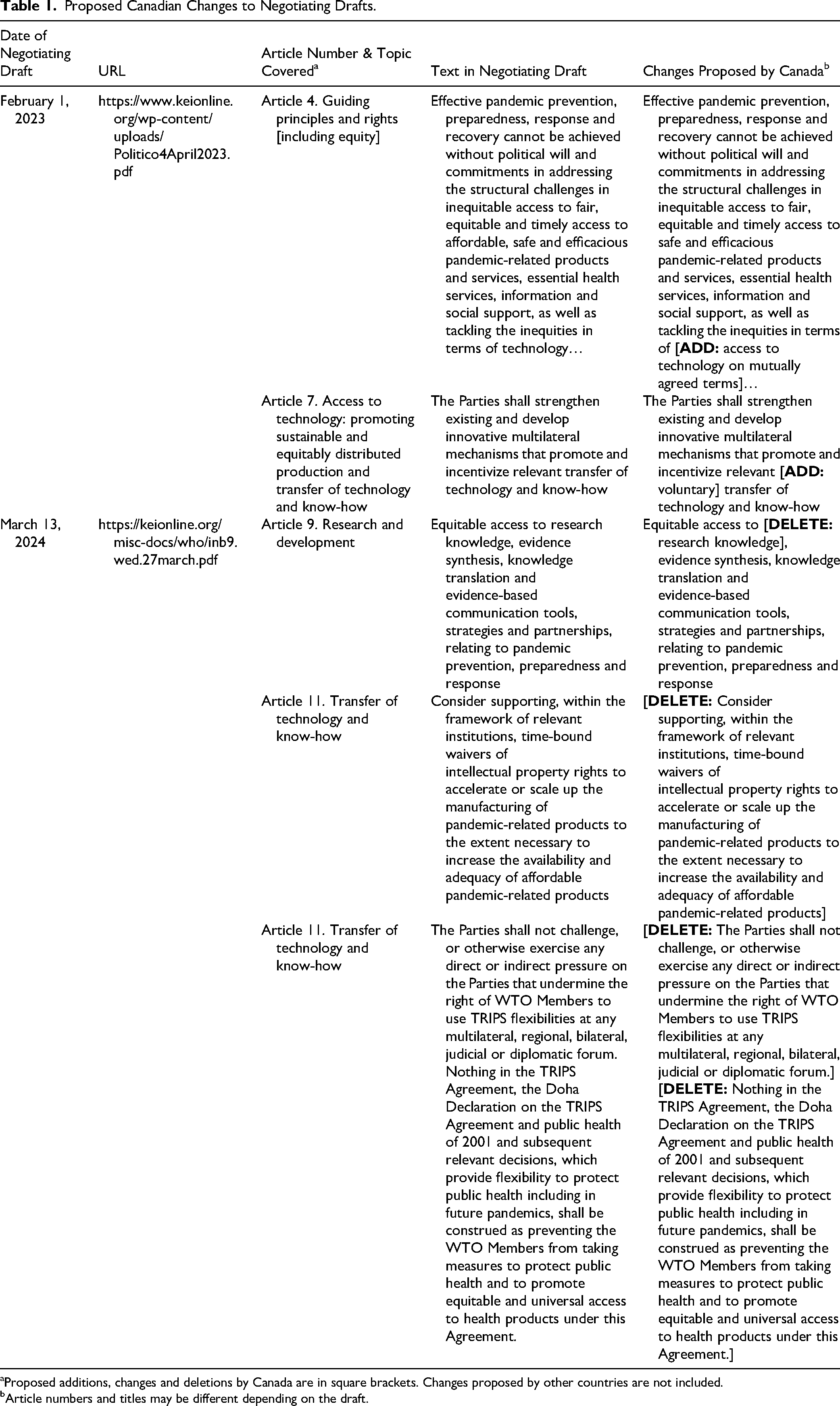
Proposed additions, changes and deletions by Canada are in square brackets. Changes proposed by other countries are not included.
Article numbers and titles may be different depending on the draft.
Klein and Schouten analyzed Canada's position on simultaneously weakening the TRIPS Agreement flexibilities (flexibilities in the Trade Related Aspects of Intellectual Property Agreement agreed to by all members of the World Trade Organization) and strengthening support for intellectual property (IP). (TRIPS flexibilities allow countries to implement their intellectual property obligations in a way that supports their own public policies and economic development.) Canada made repeated amendments to remove and limit references to IP waivers including deleting critical provisions aimed at ensuring adequate implementation and full use of TRIPS flexibilities. “Canada also removed language that would have required parties to amend domestic legislation to fully implement TRIPS…[and] it deleted language that would have prevented ‘[p]arties [from] exercis[ing] any direct or indirect pressures on the Parties that undermine the right of WTO Members to use TRIPS flexibilities’”
18
(page 5) (Table 1)
In the ninth round of negotiations in March 2024, Canada proposed deleting “reference to parties promoting ‘equitable access to research knowledge’…On sustainable production, Canada proposed adding a reference to ‘as needed’ and ‘to the extent possible’” 11 (page 8). Canada also sought to cap the provision on time-bound waivers on intellectual property by only requiring parties to merely ‘consider supporting’ time-bound waivers and recommended deleting “reference to the purpose of the provision to ‘accelerate or scale up the manufacturing of pandemic-related products to the extent necessary to increase the availability and adequacy of affordable pandemic-related products’” 11 (page 8) (Table 1). In effect, what all these measures that Canada advocated for meant was that instead of minimizing any barriers to the transfer of technology and research knowledge Canada sought to enhance them.
Canada's proposal about equitable access to research knowledge mirrored its rejection of a similar recommendation in a Canadian parliamentary committee report on vaccine equity and the pandemic. The report recommended that the Canadian government should ensure that its agreements to provide research and development funding include clauses that allow intellectual property resulting from that funding—including vaccines, therapeutics, and diagnostics—to be easily licensed to manufacturers serving low- and middle-income countries.
20
This recommendation echoed one from the House of Commons Standing Committee on Health in 2018 that called for the Canadian Institutes of Health Research to “include in its existing research and development programs support for the development of open science models of drug discovery”
21
(page 21). Instead, the government reinforced its position that Public benefit is maximized when IP terms and conditions are tailored to address the specific context and objective of each funding opportunity on voluntary, mutually agreed terms. One size fits all solutions can put the desired public benefit at risk. Where it is appropriate to consider possible licensing and access commitments, officials will do so on a contextualized basis.
22
Although the stakeholder meetings that Canada organized expressed strong support for the priorities of Indigenous partners in the Pandemic Agreement through addressing systemic racism and the social determinants of health, promoting Indigenous rights, providing culturally competent care and building community-level capacity 8 there is no record of Canada actively pushing these issues in the negotiations, except for the one mention in passing referred to in the next paragraph. There was only a single mention of Indigenous Rights in the final text of the Pandemic Agreement. Article 15 calls on Parties to the Agreement to “promote and facilitate the effective and meaningful engagement of Indigenous Peoples…in planning, decision-making, implementation, monitoring and evaluation of policies, strategies and measures”. 23
The only area in the negotiations where it appears that Canada took a consistent and progressive stance was on gender equality. Canada requested “the following provision be added: ‘it recognises that pandemics have a disproportionate impact on women and girls, Indigenous peoples and all marginalised groups or people in vulnerable situations’” 11 (page 6). It also pushed for gender-inclusive language by recommending that “Article 16 on International Collaboration and Cooperation include specific mention of women in a provision that calls for equitable representation of decision makers” 11 (page 8). Klein and Schouten, however, note the disjuncture between Canada using equity-focused rhetoric around gender equality while resisting IP measures to promote global health equity. 18 This difference was glossed over in an on-line presentation about the state of the negotiations that took place in January 2025. The Public Health Agency of Canada emphasized that “Canada is continuing to work with like-minded to secure [gender equality] in the principles and/or preambular section of the text” whereas when it came to global equity for pandemic-related health products all that was said was that “articles related to technology transfer, supply chain and logistics, procurement, distribution, and access and benefit sharing, remain unresolved”. 24 Brisbois and colleagues argue that “Canada's obstruction of global COVID-19 vaccine equity is a logical and deliberate extension of dominant neoliberal economic policy models” (page 1) as expressed by the prioritization of protecting IP at the expense of equity. 25
The Pandemic Agreement and Next Steps
The final version of the Pandemic Agreement, passed at the May 2025 meeting of the World Health Assembly (WHA),
23
is a mixed bag of successes, partial successes and failures
26
in terms of achieving the initial objectives laid out by an international panel of experts. The panel recommended that the Agreement ensure “sufficient financing for biomedical research and development (R&D), creates conditions for licensing government-funded R&D, mandates technology transfer, shares intellectual property, data and knowledge needed for the production and supply of products, and streamlines regulatory standards and procedures to market medical countermeasures…[and] that a pandemic treaty ensures greater transparency and inclusive governance of these systems”
27
(page 1).
The purpose here is not a detailed analysis of the final version of the Agreement, nor is it to claim that Canada was a major player in the shaping of the Agreement. The federal government maintained that “Canada supported the development of the Agreement to: improve global cooperation, strengthen collective action and accountability and address gaps in pandemic prevention, preparedness and response”. 28 However, in practice that is not what happened. Although it is difficult to determine how much the Canadian position influenced the final wording of the Agreement, in many respects, its text reflects Canadian concerns that private industry and governments of HICs should not be required to participate in any meaningful actions to increase equity. In particular, when it comes to sharing technology, instead of obligations, the final draft says that technology will be shared where “mutually agreed upon,” leaving it to the goodwill of companies and countries. The article on research sharing, even when the research is publicly funded, is also weak, only saying that Parties shall “develop and implement national and/or regional policies, adapted to its domestic circumstances”. 23 While the obligation to develop policies is placed on Parties, there are no requirements about what those policies should contain. On-the-other hand, Canada was not successful in embedding the concept of gender equality in the Agreement. The only places the term occurs are passing mentions in Article 3 on Principles and Approaches and Article 7 on Health and Care Workforce.
The approval of the Pandemic Agreement is not the final step in the process, as there are a number of steps still to be completed, most importantly an annex on pathogen access and benefit sharing (PABS). The objective of the annex is to: facilitate rapid and timely access to pathogens that have the potential to become a pandemic and to support rapid and equitable access to benefits, including vaccines, diagnostics and therapeutics. Until this annex is finalized, the overall Pandemic Agreement will not be open to signing and ratification. “Conditioning the signature of the Pandemic Agreement on a PABS Annex…reflects the geopolitical fault lines that overshadowed the negotiations. Bridging the chasm between countries with strong health sectors and health product research and manufacturing capacity and those that depend on the charity of such countries “is not simply a question of redistribution, but one of restructuring and acknowledging long histories of exploitation and extraction” 29 (page 4).
The Canadian government is taking part in the negotiations on the annex and says that its engagement strategy aims to facilitate meaningful and inclusive engagement with partners and stakeholders. 28 However, it continually made the same hollow claims throughout the negotiating process for the Pandemic Agreement, so it is questionable what that engagement will look like and whose interests Canada will be representing in those negotiations. While there hasn’t been any research into lobbying by the pharmaceutical and biotechnology industries around the Pandemic Agreement, during the pandemic when India and South Africa proposed a waiver on IP connected to COVID-19 products and technology, the industry heavily lobbied the Liberal government not to support the proposed waiver. 30 The government, in turn, studiously avoided taking a position in support of the waiver. 25 It is almost certain that the industry will be making its case to the government about the annex and based on past experience the Liberals will be receptive to the messaging from industry. To date (September 21, 2025) Canada has not submitted any text proposals for the PABS Annex. 31
It is worth noting that even once the annex is finalized that Canada has not committed to signing the Agreement until it has examined the “implications for the federal government, provinces and territories and Indigenous partners”. 28 What “implications” the government will be looking at was not specified. Finally, if Canada eventually signs the Agreement, in order to comply with its provisions it will have to implement a policy that includes provisions in publicly funded research and development grants that promote timely and equitable access to pandemic-related health products. 23 However, given how resistant Canada has been to this type of policy in the past, it is highly likely that any new policy will be extremely weak.
Finally, there is the question of enforceability of the Pandemic Agreement. The only other treaty that the WHO has negotiated is the Framework Convention on Tobacco Control. There are no financial penalties or other kinds of sanctions for countries that fail to uphold the measures in that treaty. Instead, it primarily relies on a system of good faith. Like most international treaties, it operates with the expectation that once a country has signed onto the treaty it will enforce it.
32
Similarly, although the Pandemic Agreement and the still being negotiated PABS annex, is also legally binding, its ultimate enforcement rests with the actions of the WHO Member States. As Halabi and Gostin make clear The proposed WHO Pandemic Agreement COP [Conference of Parties] is charged with oversight functions but ultimately possesses no real authority to compel a government to take any action it does not wish to take. The text does not give the COP the ability to, for example, sanction a party that does not comply with either textual obligations or PABS provisions. In other words, there are no effective mechanisms in place to ensure compliance.
33
Conclusion
The BMJ commissioned a series of articles about Canada's performance in the COVID-19 pandemic and the editorial accompanying the articles was titled “The world expected more of Canada”. 34 The same sentiment applies to Canada's role in the creation of the Pandemic Agreement. While Canada formally professed support for strengthening global cooperation and collective action and went through the motions of public consultations, something that many countries didn’t undertake, ultimately it ignored what it heard during the negotiations. Instead of taking the opportunity to push for equity and prioritization of public health, it chose to continue its decades long policy of putting the rights of private interests first. 35
Supplemental Material
sj-docx-1-joh-10.1177_27551938261458695 - Supplemental material for The World Expected More of Canada: Canada and the Pandemic Agreement
Supplemental material, sj-docx-1-joh-10.1177_27551938261458695 for The World Expected More of Canada: Canada and the Pandemic Agreement by Joel Lexchin in International Journal of Social Determinants of Health and Health Services
Footnotes
Acknowledgements
Adam R. Houston and Roojin Habibi provided important information and pointed out issues that were initially not adequately covered.
Ethical Approval
Ethical approval was not necessary as all information was publicly available.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Between 2022–2025, Joel Lexchin received payments for writing a brief for a legal firm on the role of promotion in generating prescriptions, for being on a panel about pharmacare and for co-writing an article for a peer-reviewed medical journal. He is a member of the Boards of Canadian Doctors for Medicare and the Canadian Health Coalition. He receives royalties from University of Toronto Press and James Lorimer & Co. Ltd for books he has written. He has received funding from the Canadian Institutes of Health Research in the past.
Data Availability
No data was generated for this study.
Date of Submission
September 30, 2025
Supplemental Material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.