
Abstract
Background:
Despite its critical importance, there has been no comprehensive quantitative synthesis focused specifically on clinical inertia in upper-middle-income countries. Without pooled prevalence estimates, identification of common predictors, and contextual insights into consequences, policymakers and clinicians in these settings are limited in their capacity to design targeted interventions.
Objective:
This study aimed to estimate the pooled estimate of clinical inertia among adults with type 2 diabetes mellitus in upper-middle-income countries.
Design:
This study was conducted as a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources and methods:
A comprehensive search was conducted using electronic databases such as PubMed, Science Direct, African Journals Online, and Google Scholar. All retrieved records were imported into EndNote reference manager, and duplicates were removed. The methodological quality of included observational cross-sectional studies was assessed using the Modified Newcastle-Ottawa Scale adapted for cross-sectional and cohort studies. Data were extracted from all studies that met the inclusion criteria using the Joanna Briggs Institute standardized data extraction form in Microsoft Excel. Quantitative data were analyzed using STATA software version 17. Heterogeneity between studies was assessed using the Cochran’s Q test and quantified with the Higgins (I2) statistic.
Results:
Ultimately, 13 studies met the eligibility criteria and were included in the final review. In this study, the pooled effect size using the random-effects model was estimated to be 45.56% (95% CI: 32.87–58.25). The pooled prevalence should be interpreted as a summary measure reflecting the overall body of evidence, as substantial between-study heterogeneity was observed (I2 = 99.8%). Diabetes complications and comorbidities were significantly associated with clinical inertia.
Conclusion:
The findings highlight considerable variability in the reported prevalence of clinical inertia across upper-middle-income countries, suggesting important contextual and methodological differences between studies. This meta-analysis demonstrates that diabetes complications and comorbidities are significantly associated with clinical inertia. Overall, these findings highlight that clinical inertia remains a pervasive barrier to optimal chronic disease management. Health systems should prioritize patients with diabetes complications and multiple comorbidities for timely monitoring and treatment adjustments.
Trial registration:
CRD420251231712.
Plain language summary
This study looked at why doctors sometimes delay changing or intensifying treatment for people with type 2 diabetes in upper-middle-income countries. Delays in treatment, also called clinical inertia, can lead to higher blood sugar levels and increase the risk of complications such as heart disease, kidney problems, and vision loss. We reviewed and combined results from multiple studies to better understand how common clinical inertia is and what factors contribute to it. Our findings show that both patient-related factors (like not following advice or missing appointments) and healthcare-related factors (like limited resources, lack of guidelines, or busy clinics) can lead to delays in treatment. Understanding these reasons is important because it can help improve diabetes care, reduce complications, and help patients live healthier lives.
Background
Type 2 diabetes mellitus (T2DM) represents one of the most challenging and rapidly expanding non-communicable diseases globally.1,2 A study based on Global Burden of Disease data found that the burden of type 2 diabetes (mortality and DALYs) increased most rapidly in upper-middle-income countries (UMICs), showing the sharpest rise in these countries. 3 Indeed, nearly 80% of people living with diabetes are in UMICs, where substantial portions remain undiagnosed or inadequately treated. 4 The growing prevalence of diabetes, coupled with limited health system resources, highlights the critical need to address deficiencies across the entire care continuum, from early detection to sustained glycemic management.5–7
Achieving and maintaining glycemic targets in T2DM is critical to preventing both micro-vascular and macro-vascular complications. 8 Studies have demonstrated that rigorous glycemic management substantially reduces the risk of micro-vascular complications like retinopathy and nephropathy, as well as cardiovascular events.9–11 Yet despite well-established evidence and clinical practice guidelines, many patients in real-world settings do not achieve recommended targets. One of the key barriers is clinical inertia, defined as the failure of healthcare providers to initiate or intensify therapy when indicated by clinical guidelines.12–14
Clinical inertia is part of a broader phenomenon known as therapeutic inertia, encompassing not only failure to intensify therapy but also lack of switching among therapies, inadequate dose adjustment (titration), and even reluctance to de-escalate when appropriate.15,16 In type 2 diabetes, this implies that even when patients consistently show elevated HbA1c levels, clinicians postpone treatment intensification, delay starting insulin, or neglect to adjust medication doses despite inadequate glycemic control.17–19
The prevalence and impact of inertia have been well documented in high-income countries.12,20 A systematic review of 25 studies, including over 575,000 people with T2DM, found that more than half of patients experienced clinical inertia. The rates varied widely by country, ranging from 35.4% to 85.8% in the United States and 22.1% to 69.1% in the United Kingdom. 12 However, data from UMICs remain much more limited. This lack of evidence is particularly problematic, given that UMICs face unique structural, economic, and health system challenges that may amplify inertia.21–23
Several studies in UMICs have highlighted the presence and magnitude of clinical inertia. In Malaysia, a 5-year retrospective cohort study using data from the National Diabetes Registry found that only 45.4% of patients with HbA1c ⩾7% experienced therapy intensification within the study period. 24 In UMICs, 65.8% of insulin-treated patients exhibited clinical inertia, with very limited change in insulin dosing even over a two-year follow-up period and persistently elevated HbA1c levels. 25 Moreover, a recent cross-sectional study in Ethiopia reported that 31.4% of patients at a public hospital showed clinical inertia. 26 In Colombia, retrospective cohort data from newly diagnosed T2DM patients revealed an overall clinical inertia rate of 93.5%, with higher inertia in subsidized versus contributory health insurance regimens. 27 These findings suggest that in UMICs settings, inertia may be particularly entrenched and related to social, economic, and health system inequities. 28
The determinants of clinical inertia in T2DM are multifactorial and operate at multiple levels. At the provider level, common barriers include limited guideline knowledge, risk aversion (particularly concerns about hypoglycemia or weight gain), insufficient time during consultations, therapeutic nihilism, and lack of decision support.12,18,29,30 At the patient level, factors may include low adherence, fear of side effects, cost constraints, low health literacy, and competing comorbidities. In resource-limited settings, system-level issues are also crucial: drug unavailability, limited formularies, fragmented follow-up mechanisms, and high out-of-pocket costs are all pervasive.31–33
In UMICs, these system-level challenges may exacerbate inertia more than in high-income settings. Beyond prevalence and determinants, clinical inertia has serious clinical implications. Delays in treatment intensification mean prolonged periods of uncontrolled glycaemia, exposing patients to cumulative risk of complications.29,34 Systematic reviews indicate that median delays in intensification often exceed 1 year, and in some settings, much longer. In inertia-affected populations, suboptimal control due to delayed therapy changes translates into greater morbidity, increased healthcare utilization, and higher long-term costs.12,18,34,35 Despite its critical importance, there has been no comprehensive quantitative synthesis focused specifically on clinical inertia in UMICs. 21 Without pooled prevalence estimates, identification of common predictors, and contextual insights into consequences, policymakers and clinicians in these settings are limited in their capacity to design targeted interventions. 28
Therefore, this study aims to fill this gap by conducting a systematic review and meta-analysis of clinical inertia among adults with T2DM in UMICs. Specifically, the study will (1) estimate the pooled prevalence of clinical inertia in these settings; (2) identify the determinants associated with inertia. The goal of the study is to provide robust, contextually grounded evidence that informs future strategies such as task sharing, decision-support integration, formulary reform, and training to reduce inertia and improve diabetes outcomes in resource-constrained environments.
Methods
Study design
This study was conducted as a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-2020) guidelines. 36 A meta-analysis was conducted to provide a broad quantitative summary of clinical inertia across studies sharing a core conceptual definition, while acknowledging underlying methodological and contextual variability.
The protocol was registered with the Prospective Register of Systematic Reviews https://www.crd.york.ac.uk/PROSPERO/view/CRD420251231712 for transparency and to minimize bias. The result of the study was also reported based on the updated Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA-2020) checklists (Supplemental File 1).
Eligibility criteria
Inclusion criteria: The review has the following inclusion criteria;
Observational studies (cross-sectional, cohort, case-control) and interventional studies reporting clinical inertia among adults (⩾18 years) with T2DM.
Studies conducted in UMICs (as classified by the World Bank). 37
Studies reporting prevalence, determinants/predictors of clinical inertia.
Articles published in English.
Exclusion criteria: The review has the following exclusion criteria;
Studies including only type 1 diabetes or gestational diabetes patients.
Case reports, reviews, editorials, conference abstracts without full-text, and studies with insufficient data.
Selection criteria (PICO framework)
The eligibility of studies was defined using the Population, Intervention/Exposure, Comparison, and Outcomes (PICO) framework as follows:
P – Population
Adults aged ⩾18 years diagnosed with T2DM.
Participants receiving diabetes care in UMICs as defined by the World Bank classification.
Studies including mixed populations were included only if data for T2DM patients could be separately extracted.
I – Intervention/Exposure
Clinical inertia (therapeutic inertia), which can be defined as: Failure by healthcare providers to initiate or intensify therapy when glycemic targets remain unmet.
Exposure may include inertia related to oral hypoglycemic agents, insulin initiation/intensification, or other guideline-recommended treatments.
C – Comparison
Studies comparing: ○ Patients who experienced clinical inertia versus those who received timely treatment intensification. ○ Different health care settings, treatment modalities, clinician characteristics, or patient profiles.
O – Outcomes
Primary outcomes:
Prevalence of clinical/therapeutic inertia among T2DM patients.
Secondary outcomes:
Predictors/determinants of clinical inertia (e.g., age, disease duration, and healthcare system barriers).
Information sources and search strategy
A comprehensive search was conducted using electronic databases such as PubMed/MEDLINE, Science Direct, African Journals Online (AJOL), and Google Scholar (for gray literature). The search covered publications from January 1 2015 to November 20, 2025. Keywords and MeSH terms were used in combination with Boolean operators. Reference lists of included studies (Snowball technique) were also screened to identify additional relevant articles (Supplemental File 2).
Clinical inertia measurement
Clinical inertia in the included studies was defined and measured using varying criteria, reflecting differences in study design and clinical context. Measurement approaches included:
Failure to intensify therapy within a defined timeframe after identifying unmet glycemic targets (e.g., 3 months).
Failure to adjust medication at the next clinic visit despite persistently elevated HbA1c levels.
Lack of treatment intensification despite physician documentation indicating clinical decision-making considerations, such as patient readiness, comorbidities, or potential contraindications.
These differences in operational definitions were carefully recorded and considered in the analysis. To account for variability across studies, we employed a random-effects meta-analysis for prevalence estimates and performed subgroup analyses where possible, acknowledging that heterogeneity in measurement could influence pooled estimates.
Study selection
All retrieved records were imported into EndNote reference manager, and duplicates were removed. Two reviewers (D.G.H. and H.F.H.) independently screened titles and abstracts for eligibility. Full-text articles were then assessed independently against the inclusion criteria. Discrepancies were resolved through discussion or consultation with a third author (W.C.T.).
Methodological quality assessment
The methodological quality of included observational cross-sectional studies was assessed using the Modified Newcastle-Ottawa Scale (NOS) adapted for cross-sectional and cohort studies. The NOS uses a star system to rate studies based on three broad domains: Selection (up to 5 stars), Comparability (up to 2 stars), Outcome (for cohort studies), or Exposure (up to 3 stars). The maximum score a study can achieve is 10 stars. Finally, studies with 7–10 stars indicate high quality, 4–6 stars (moderate quality), and 0–3 stars (low quality) 38 (Supplemental File 3). Two authors (D.G.H. and H.F.H.) independently assessed the methodological quality of each study. Disagreements in the assessment and scoring were solved through discussion and consensus.
Data extraction
First, studies were assessed through title and abstract review by two independent authors. Disagreements were solved by consensus; a third author was invited in case of persistent contradiction. Second, potentially-eligible studies undergo full-text review to determine if they satisfy the criteria set for inclusion. Data were extracted from all studies that met the inclusion criteria using the Joanna Briggs Institute standardized data extraction form in Microsoft Excel. The two authors (D.G.H. and G.W.A.) independently extract all relevant information. Extracted information included study characteristics (first author, year of publication, country, study setting, and design), participant characteristics (sample size and duration of diabetes), and key measures related to clinical inertia. In addition, we extracted the definition or method of assessment of clinical inertia, prevalence estimates, and identified determinants. Any discrepancies between reviewers were resolved through discussion. For studies reporting incomplete or unclear data, attempts were made to contact the corresponding authors to obtain the necessary information.
Statistical analyses
Quantitative data were analyzed using STATA software version 17 (StataCorp LLC, College Station, TX, USA). The prevalence of clinical inertia was pooled across studies using a random-effects meta-analysis (DerSimonian and Laird method) to account for anticipated between-study heterogeneity. Heterogeneity between studies was assessed using the Cochran’s Q test (p < 0.10 considered significant) and quantified with the Higgins (I2 statistics), with values of 25%, 50%, and 75% indicating low, moderate, and high heterogeneity, respectively. 39 Forest plots were generated to visualize pooled estimates and study-level variability.
Subgroup analyses were conducted to explore potential sources of heterogeneity. Meta-regression analyses were performed to examine the effect of study-level covariates such as mean age, diabetes duration, and sample size on prevalence estimates. To assess the robustness and reliability of the pooled estimates, a leave-one-out Jackknife sensitivity analysis was conducted.
Publication bias was detected by the visual inspection of the funnel plot and the statistical Egger’s test.40,41 A p-value less than 0.05 from Egger’s test indicated notable publication bias, implying that studies with larger effects (either positive or negative) are more likely to be published. 42 A trim and fill analysis was performed to address this publication bias. 43
Results
Article search results
A total of 3125 records were identified from database searches, including 840 from PubMed, 1164 from African Journals Online, 317 from HINARI (Research4Life), 50 from Science Direct, and 754 from Google Scholar. An additional 12 records were identified from websites, and 6 records through citation searching. Before screening, 845 duplicate records and 624 records removed for other reasons were excluded. The remaining 1656 records were screened by title and abstract, and 1463 records were excluded at this stage. Full texts of 193 articles were retrieved for detailed assessment. Of these, 56 were excluded due to target population differences, 119 because of unclear or insufficient information, and 7 because of poor methodological quality. Ultimately, 11 studies, along with 2 additional reports, met the eligibility criteria and were included in the final review. These studies were conducted in Ethiopia, Malaysia, Colombia, Bosnia, Serbia, Thailand, Brazil, South Africa, Cameroon, and India (Figure 1).

Flow diagram for the selection of studies included in clinical inertia among patients with type 2 diabetes mellitus in UMICs (n = 13).
Overview of included studies
This systematic review and meta-analysis included 13 studies conducted across 10 countries. The studies, published between 2017 and 2025, involved a total of 28,441 participants, with individual study sample sizes ranging from 111 to 7646. The studies were carried out in Ethiopia, 26 Malaysia (2 studies),24,44 Colombia (2 studies),27,45 Bosnia, 46 Serbia, 47 Thailand (2 studies),48,49 Brazil, 25 South Africa, 50 Cameroon, 51 and India. 52 Five studies employed an institutional-based cross-sectional (IBCS) design, while the remaining eight used a retrospective approach. The reported prevalence of clinical inertia varied widely, ranging from 12.6% to 93.5%. All articles were published in peer-reviewed journals (Table 1).
Overview of included studies in clinical inertia among patients with type 2 diabetes mellitus in UMICs (n = 13).

UMICs: upper-middle-income countries; IBCS: institutional-based cross-sectional.
Pooled prevalence of clinical inertia
In this study, the pooled effect size (ES) using the DerSimonian and Laird random-effects model was estimated to be 45.56% (95% CI: 32.87–58.25). Although the pooled prevalence of clinical inertia was estimated at 45.56%, the extremely high heterogeneity (I2 = 99.8%) indicates substantial variability across studies and limits the interpretation of this value as a precise epidemiological estimate. The between-study variance (Tau 2 ) was estimated at 540.16. The overall ES was statistically significant (z = 7.04, p < 0.001). The pooled prevalence should be interpreted in light of substantial heterogeneity observed across studies with differing settings and operational definitions (Figure 2).
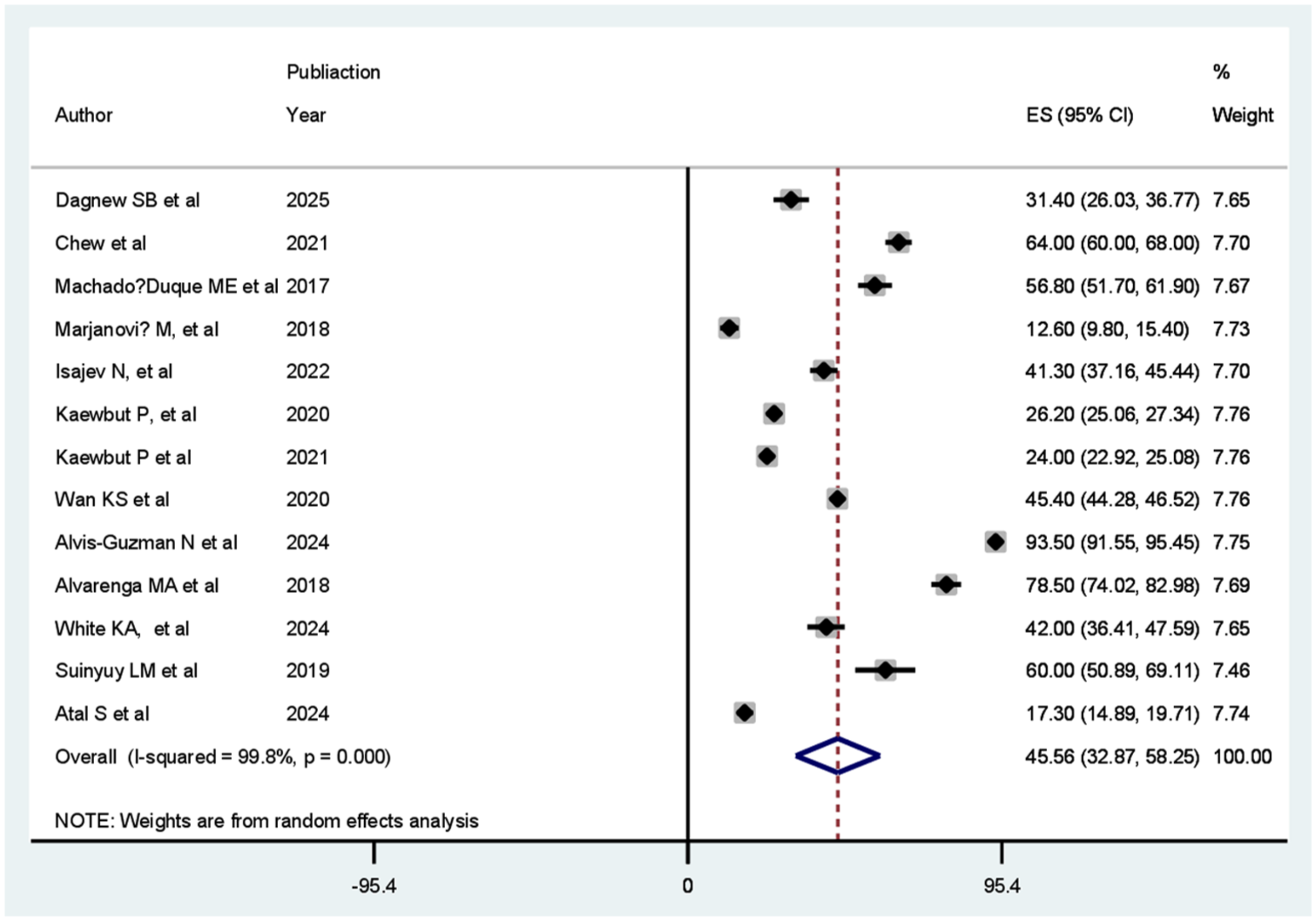
Forest plot for the pooled prevalence of clinical inertia among patients with type 2 diabetes mellitus in UMICs (n = 13).
Subgroup analysis
Subgroup analysis based on study design revealed that the pooled prevalence of clinical inertia varied between IBCS and retrospective studies. Among the IBCS studies, the pooled prevalence was 47.08% (95% CI: 34.90–59.26, I2 = 94.9%, p < 0.001), with individual study estimates ranging from 31.40% to 60.00%. For retrospective studies, the pooled prevalence was 44.80% (95% CI: 29.19–60.41, I2 = 99.9%, p < 0.001), with individual study estimates ranging from 12.60% to 93.50%. The effect sizes were statistically significant for both subgroups and overall (IBCS: z = 7.58, p < 0.001; retrospective: z = 5.63, p < 0.001; overall: z = 7.04, p < 0.001) (Figure 3).

Forest plot for subgroup analyses based on study design on the pooled prevalence of clinical inertia among patients with type 2 diabetes mellitus in UMICs (n = 13).
Publication bias
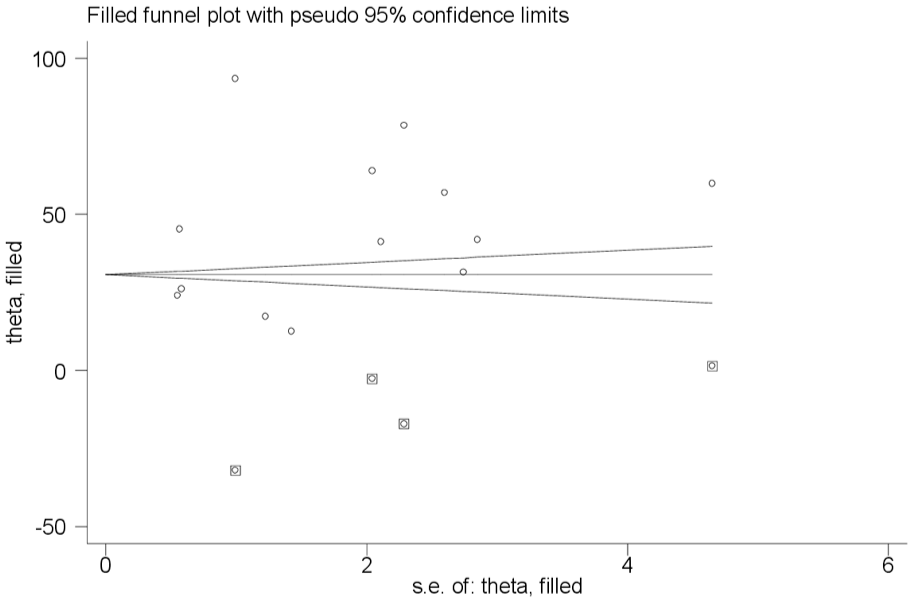
Publication bias was assessed using both Begg’s and Egger’s tests. Begg’s test showed no significant evidence of publication bias (adjusted Kendall’s score z = 0.73, p = 0.464; continuity corrected z = 0.67, p = 0.502). In contrast, Egger’s test indicated potential small-study effects, with a statistically significant slope coefficient (slope = 29.25, p = 0.019), although the bias intercept was not significant (bias = 9.50, p = 0.386). These results suggest that while Begg’s test did not detect bias, Egger’s test highlighted a possible asymmetry among the included studies. The discrepancy between Begg’s and Egger’s test results may reflect differences in their statistical power and sensitivity to small-study effects; therefore, findings were interpreted cautiously. In addition, the trim-and-fill analysis suggested potential publication bias; however, the adjusted estimates did not substantially alter the overall results, indicating that the main findings remain relatively robust. The funnel plot also showed an asymmetrical distribution of studies, indicating potential publication bias (Figure 4).

Funnel plot showing publication bias.
Trim-and-fill analysis
To adjust for potential publication bias, a trim-and-fill analysis was performed using a fixed-effects model. Across four iteration cycles, four studies were imputed, resulting in a total of 17 studies included in the filled meta-analysis. The pooled prevalence of clinical inertia after adjustment was 31.90% (95% CI: 17.52–46.27) using the random-effects model and 30.68% (95% CI: 30.15–31.20) using the fixed-effects model. Heterogeneity remained substantial (Q = 11,000, p < 0.001; moment-based between-study variance = 909.19). The imputed studies had effect estimates ranging from –32.15 to 1.35, while the original studies ranged from 12.60% to 93.50%, reflecting the wide variability in reported prevalence across studies. This adjustment helped to account for asymmetry and potential missing studies in the original analysis (Figure 5).
Trim-and-fill analysis for the asymmetrical distribution of the included studies.
Meta-regression
A random-effects meta-regression was conducted to investigate potential sources of heterogeneity across the 13 studies. The REML estimate of between-study variance (Tau 2 ) was 0, and the residual heterogeneity was negligible (I2(res) = 0.00%). The meta-regression model showed a reduction in residual heterogeneity (Tau 2 = 0; residual I2 = 0%), suggesting that the included covariates may explain a substantial proportion of the between-study variability. The model, including the number of participants, publication year, and sample size, did not significantly explain between-study variability (F(3, 9) = 0.92, p = 0.469, Knapp-Hartung adjustment). Individually, none of the covariates were statistically significant predictors of prevalence (participants: coef = –0.003, p = 0.839; publication year: coef = –0.086, p = 0.672; sample size: coef = 0.003, p = 0.849). These findings suggest that the observed heterogeneity was not attributable to these study-level characteristics. The apparent inconsistency between the high heterogeneity in the primary analysis and the low residual heterogeneity in the meta-regression may be due to the inclusion of study-level covariates that explained much of the between-study variability; however, these results should be interpreted with caution, given the limited number of studies. Covariates included in these meta-regression models were selected a priori based on their clinical relevance and evidence from previous literature, as well as data availability across studies, to explore potential sources of between-study heterogeneity. The meta-regression findings should be considered exploratory and hypothesis-generating rather than definitive evidence regarding the sources of heterogeneity.
Sensitivity analysis
A sensitivity analysis was performed to assess the impact of each individual study on the pooled prevalence of clinical inertia. The leave-one-out Jackknife analysis showed that omitting any single study resulted in pooled estimates ranging from 41.41% to 47.93%, with 95% confidence intervals overlapping the overall pooled prevalence of 45.56% (95% CI: 32.87–58.25). To further assess the robustness of the pooled estimates, we conducted sensitivity analyses by excluding studies with extreme prevalence values and compared the resulting estimates with the primary analysis. These results indicate that no individual study disproportionately influenced the overall estimate, confirming the robustness of the findings (Figure 6).
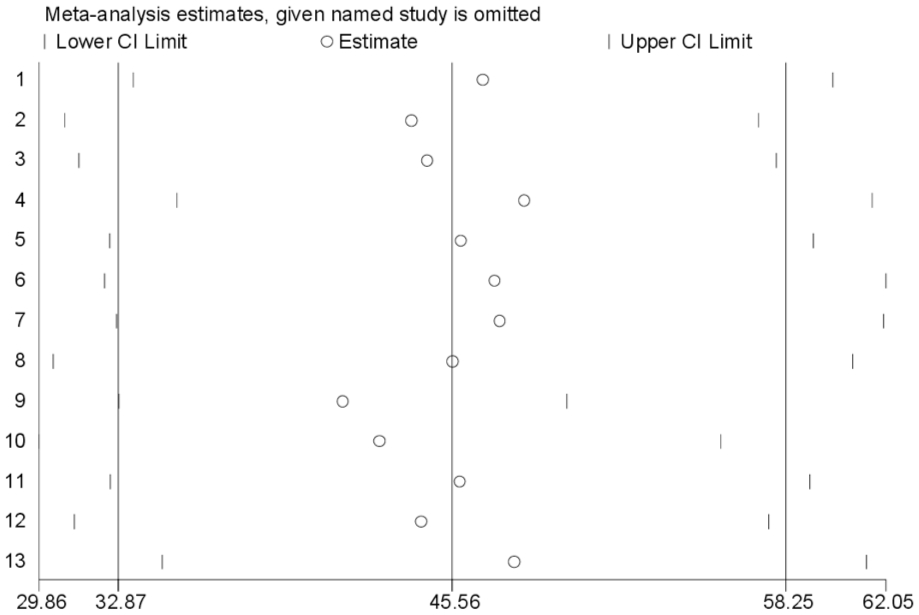
Result of sensitivity analyses.
Factors associated with clinical inertia
The findings demonstrate that diabetes complications and comorbidities are strong predictors of clinical inertia. Patients who have developed diabetes-related complications were substantially more likely to experience delays in treatment intensification. The pooled odds ratio (11.49; 95% CI: 2.92–45.20) indicates that these patients had more than 11 times higher odds of clinical inertia than those without complications. The very high heterogeneity (I2 = 93.3%) suggests that differences in study settings, patient characteristics, or definitions of complications may influence the magnitude of the effect. Similarly, comorbid conditions were also significantly associated with clinical inertia. The pooled OR of 3.36 (95% CI: 1.34–8.45) indicates that patients with additional comorbidities were more than three times more likely to experience inertia compared to those without comorbidity. Although the ES is smaller than that observed for complications, it still reflects a meaningful clinical burden. The substantial heterogeneity (I2 = 82.4%) suggests that variability across studies may arise from differences in the types or severity of comorbidities assessed (Figure 7).
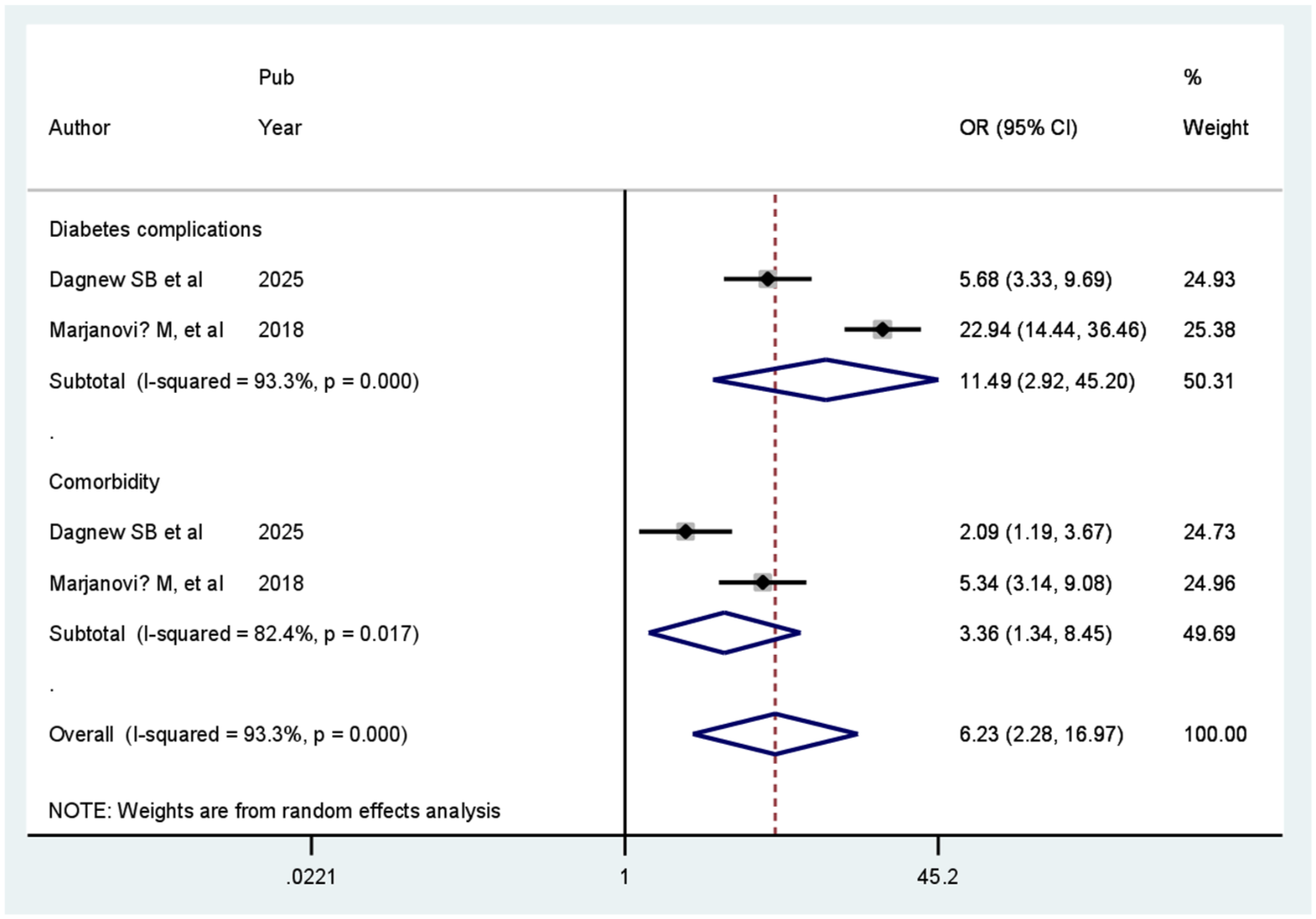
Factors associated with clinical inertia.
The meta-analysis of factors associated with clinical inertia should be interpreted with caution. The pooled odds ratios for diabetes complications and comorbidities were derived from only two studies each and should therefore be interpreted with caution. The wide confidence intervals observed in some pooled estimates indicate substantial uncertainty in the magnitude of the associations. Accordingly, this analysis is best considered exploratory and hypothesis-generating rather than confirmatory. While the findings are consistent with those reported in the primary studies, the quantitative synthesis provides a standardized summary of the direction and approximate magnitude of associations and makes the degree of uncertainty explicit. Importantly, it also highlights the limited and fragmented nature of the available evidence, underscoring the need for more robust and methodologically consistent studies to better understand these relationships.
Discussion
While statistical heterogeneity was addressed using a random-effects model, the decision to conduct a meta-analysis was primarily based on an assessment of conceptual and methodological comparability across studies. A major finding of this review was the extremely high heterogeneity observed among the included studies, indicating that the prevalence of clinical inertia varies considerably across settings, populations, and healthcare systems. The observed heterogeneity may be explained by differences in healthcare infrastructure, clinical practice patterns, diagnostic criteria, treatment protocols, study populations, and methodological approaches across the included studies. Therefore, the pooled prevalence should primarily be interpreted as a summary indicator of the existing literature rather than a definitive estimate applicable to all UMICs.
Although clinical inertia is a complex and context-dependent construct, the majority of included studies share a common underlying definition—namely, the failure to initiate or intensify therapy when clinically indicated. We acknowledge that variations in operational definitions, healthcare settings, and patient populations introduce a degree of conceptual heterogeneity that cannot be fully resolved through statistical methods alone. However, given the presence of this core conceptual alignment, we considered quantitative synthesis to be appropriate while interpreting the pooled estimates with caution. Accordingly, the findings should be understood as a generalized summary across diverse contexts rather than a precise estimate applicable to any single setting. Given the substantial clinical and methodological heterogeneity across included studies, the findings have been primarily interpreted using a narrative synthesis, with meta-analytical results presented as exploratory and supportive.
In this meta-analysis, the pooled prevalence (ES) of clinical inertia among patients in UMICs was estimated at 45.56% (95% CI: 32.87–58.25), suggesting that nearly half of patients in UMICs settings may be subject to clinical inertia. Despite variability, the meta-analysis offers a useful benchmark by synthesizing fragmented evidence and highlighting the overall magnitude and variability of clinical inertia.
The finding of high prevalence aligns with prior literature: for instance, a recent systematic review of patients with T2DM reported that many included studies showed clinical inertia rates over 50% globally, including in high-income countries. 12
However, high between-study heterogeneity observed in our analysis (I2 = 99.8%) indicates substantial variability in clinical inertia prevalence across studies and contexts. This suggests that the pooled prevalence should be interpreted with caution, because the observed variation likely reflects real differences across settings rather than mere sampling error. Potential sources of heterogeneity include variation in healthcare system infrastructure, resource availability, access to care, patient populations (e.g., differences in comorbidity burden, socioeconomic status, and health literacy), disease conditions (e.g., diabetes, hypertension, and asthma), and differing definitions or measurement methods of “clinical inertia” (e.g., how treatment intensification is defined and when, follow-up duration, clinical threshold for action). Indeed, clinical inertia has been shown to vary substantially across countries and health systems. 12
The magnitude of clinical inertia in UMICs is particularly concerning, given the burden of chronic diseases in these settings. Chronic illnesses such as T2DM and hypertension are increasingly common in these countries, but resource constraints, lack of guideline-concordant care, limited access to diagnostic and therapeutic options, and workforce shortages may exacerbate delays in treatment intensification. 53 As recognized in literature, clinical inertia often arises from a complex interplay of provider, patient, and system-level factors. 54
The pooled prevalence of clinical inertia observed in UMICs indicates that nearly half of patients in these settings may not receive timely treatment intensification when indicated. The estimate is broadly consistent with prior literature on chronic disease management. For example, a systematic review of 25 studies comprising 575,067 patients with T2DM found that “most of the included studies showed clinical inertia rates over 50%.” In that review, country-level prevalence varied widely: in the United States, clinical inertia ranged from 35.4% to 85.8%, while in other settings (e.g., Canada, Brazil, and Thailand) it often exceeded 60%. 12
Another systematic review of clinical inertia in hyperglycemia management (covering 53 studies) reported that delays to treatment intensification were common, with the median time to intensification after detection of elevated HbA1c often exceeding 1 year, and in many cases substantially longer. These findings underscore that clinical inertia remains a major barrier to optimal glycemic control worldwide, a pattern that also appears in UMICs according to our data. 21
Taken together, these comparisons suggest that clinical inertia is a global phenomenon, affecting both high and low-/middle-income settings. However, the manifestation and magnitude of inertia may differ by context, likely influenced by health system factors, resource constraints, provider practices, patient characteristics, and how inertia is defined or measured. Given this variability, findings from high-income countries cannot be assumed to generalize to UMICs; tailored, context-sensitive strategies are needed to address inertia where resource limitations and systemic barriers are more pronounced.23,24
Although pooled analyses were conducted for selected determinants, the findings were based on a limited number of studies and therefore provide only preliminary evidence. The pooled analyses were retained because the included studies evaluated comparable determinants using similar outcome definitions, allowing a preliminary quantitative synthesis. However, these findings should be considered exploratory and hypothesis-generating rather than definitive evidence for clinical or policy decision-making. The analysis found that diabetes complications and comorbidities were significantly associated with clinical inertia. These strong associations highlight that patients with more complex disease burden are particularly vulnerable to delays or failures in therapy intensification. These findings are consistent with prior literature indicating that multimorbidity and complexity of health conditions contribute to clinical or therapeutic inertia in chronic disease management. In a large retrospective cohort of patients with T2DM treated with basal insulin, delays in intensification were significantly associated with a higher comorbidity index; patients with more comorbidities experienced longer delays until treatment escalation. 17 Similarly, in a more recent observational study of T2DM patients on oral therapy, a higher comorbidity burden was shown to significantly increase the risk of clinical inertia. 55
Moreover, systematic reviews of clinical inertia in diabetes management emphasize that complexity, including the presence of comorbidities or complications, is among the patient and system-level factors underlying non-intensification. One such review concluded that clinical inertia is a major barrier to achieving glycemic control even in specialized centers and that patient comorbidity burden contributes to physicians’ hesitation in intensifying therapy. 12
The clinical implications of our findings are considerable. Patients with diabetes complications often require more aggressive and timely therapy adjustments to prevent progression. However, the high odds of clinical inertia among this group suggest that many may remain under-treated or suboptimally managed, potentially increasing their risk for worsening complications and adverse outcomes. Indeed, modeling studies have suggested that even short delays in treatment intensification can substantially increase long-term incidence of micro-vascular complications such as nephropathy, retinopathy, and neuropathy. 56
Beyond individual patient risk, the results point to systemic challenges: clinicians may be reluctant to intensify treatment for patients with comorbidities or complications due to concerns over polypharmacy, drug–drug interactions, increased risk of side effects, or complexity of management. This is in line with narrative reviews arguing that clinical inertia results from a complex interplay of provider, patient, and system-level barriers, especially in patients with multiple conditions or complicated disease courses. 29
Limitations
Despite the strengths of this meta-analysis, several limitations should be considered when interpreting the findings. First, there was substantial heterogeneity among the included studies which may reflect differences in study design, population characteristics, measurement of clinical inertia, and healthcare settings. Such heterogeneity limits the generalizability of the pooled estimates across all included countries. Second, the included studies varied in their definitions of clinical inertia, with some focusing on delayed treatment intensification for hyperglycemia, others on blood pressure control, and some including broader measures of guideline non-adherence. This variability may have introduced measurement bias and affected the comparability of effect sizes.
Third, the majority of studies were observational in nature, which increases the risk of confounding and limits causal inference. Unmeasured factors, such as healthcare provider characteristics, patient adherence, and healthcare system constraints, may have influenced both the exposure (complications or comorbidities) and the outcome (clinical inertia). Fourth, publication bias is present, as studies reporting significant associations are more likely to be published. Although attempts were made to include all relevant literature, some unpublished or non-English studies may have been missed, potentially affecting the pooled estimates. Some determinant meta-analyses were based on only two studies, limiting the robustness and reliability of the pooled estimates. Finally, data from certain regions or specific countries were limited, which may have underrepresented the variability in healthcare infrastructure, resource availability, and clinical practices across different countries. Future studies should aim to include more diverse settings to improve the representativeness of the findings.
Conclusion
This meta-analysis demonstrates that diabetes complications and comorbidities are significantly associated with clinical inertia. Overall, these findings highlight that clinical inertia remains a pervasive barrier to optimal chronic disease management, particularly among high-risk patients with complex clinical profiles.
Implication of the study
Targeted interventions for high-risk patients: Health systems should prioritize patients with diabetes complications and multiple comorbidities for timely monitoring and treatment adjustments.
Provider education and training: Clinicians should receive regular training on guideline-based care and strategies to manage complex patients safely, including polypharmacy and comorbidity considerations.
Clinical decision-support systems: Implementing electronic or structured tools to prompt timely treatment intensification can help reduce clinical inertia, especially in resource-limited settings.
Standardization of definitions and monitoring: Future research should use consistent criteria for clinical inertia to improve comparability and inform evidence-based policies.
Health system strengthening: UMICs should focus on improving access to medications, diagnostic services, and follow-up systems to support guideline-concordant care for patients with chronic disease.
Further research: Studies are needed to explore context-specific barriers and facilitators of treatment intensification, evaluate intervention effectiveness, and assess long-term outcomes of reducing clinical inertia. Further large-scale and methodologically consistent studies are needed to confirm these associations and improve the strength of the available evidence.
Supplemental Material
sj-docx-1-taj-10.1177_27558428261458915 – Supplemental material for Clinical inertia among patients with type 2 diabetes mellitus in upper-middle-income countries: A systematic review and meta-analysis
Supplemental material, sj-docx-1-taj-10.1177_27558428261458915 for Clinical inertia among patients with type 2 diabetes mellitus in upper-middle-income countries: A systematic review and meta-analysis by Worku Chekol Tassew, Dawit Gismie Hailemariam, Habiba Fenta Hussien, Getaw Wubie Assefa and Zemene Habtu Lakew in Sage Open Chronic Disease
Supplemental Material
sj-docx-2-taj-10.1177_27558428261458915 – Supplemental material for Clinical inertia among patients with type 2 diabetes mellitus in upper-middle-income countries: A systematic review and meta-analysis
Supplemental material, sj-docx-2-taj-10.1177_27558428261458915 for Clinical inertia among patients with type 2 diabetes mellitus in upper-middle-income countries: A systematic review and meta-analysis by Worku Chekol Tassew, Dawit Gismie Hailemariam, Habiba Fenta Hussien, Getaw Wubie Assefa and Zemene Habtu Lakew in Sage Open Chronic Disease
Supplemental Material
sj-docx-3-taj-10.1177_27558428261458915 – Supplemental material for Clinical inertia among patients with type 2 diabetes mellitus in upper-middle-income countries: A systematic review and meta-analysis
Supplemental material, sj-docx-3-taj-10.1177_27558428261458915 for Clinical inertia among patients with type 2 diabetes mellitus in upper-middle-income countries: A systematic review and meta-analysis by Worku Chekol Tassew, Dawit Gismie Hailemariam, Habiba Fenta Hussien, Getaw Wubie Assefa and Zemene Habtu Lakew in Sage Open Chronic Disease
Footnotes
Acknowledgements
The author would like to thank the authors of the included primary studies, which were used as sources of information to conduct this systematic review and meta-analysis.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author* upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.