
Abstract
Background:
The comparative effectiveness and safety of leflunomide and methotrexate in elderly rheumatoid arthritis (RA) patients remain understudied despite the growing prevalence of RA in this population.
Objective:
To compare the efficacy, drug survival, and safety of leflunomide and methotrexate in disease-modifying antirheumatic drugs (DMARD)-naive RA patients aged ⩾65 years.
Design:
Retrospective cohort study.
Methods:
Patients aged ⩾65 years with RA who were treated initially with either leflunomide or methotrexate were analyzed. Patients with DMARD-naive RA were selected according to the 2010 American College of Rheumatology/European League Against Rheumatism criteria. Patients received at least 6 months of treatment and were followed up for 24 weeks. Disease activity was assessed using the Disease Activity Score 28 (DAS28)-CRP (remission: DAS28-CRP < 2.6 and low disease activity (LDA): DAS28-CRP 2.6–3.2). Drug survival and adverse events were also recorded.
Results:
This study included 167 patients (80 on leflunomide and 87 on methotrexate). Methotrexate led to a greater reduction in DAS28-CRP (median reduction 1.9 vs 0.7, p < 0.001). By contrast, remission (37.9% vs 31.3%, p = 0.229) and LDA rates (82.8% vs 73.8%, p = 0.110) were not significantly different. In both groups, swollen joint count was associated with remission (p < 0.001). Drug survival rates were comparable in the unadjusted analysis (74.7% vs 66.3%, p = 0.152). After adjusting for baseline disease activity, methotrexate was associated with a 73% lower hazard of discontinuation (adjusted hazard ratio 0.27, 95% confidence interval [CI] 0.13–0.54, p < 0.001). The adverse event-related discontinuation rate was low and similar between the groups (10% for leflunomide vs 8% for methotrexate, p = 0.431).
Conclusion:
Both leflunomide and methotrexate are effective and safe in elderly RA patients. Methotrexate was associated with a greater reduction in disease activity and better adjusted drug survival. However, given the baseline differences in disease activity and the lack of statistically significant differences in remission and low disease activity rates at week 24, methotrexate remains a reasonable first-line option in the absence of contraindications for elderly RA patients. Leflunomide is a viable alternative when methotrexate is not tolerated.
Plain language summary
This study looked at two common medications (methotrexate and leflunomide) for rheumatoid arthritis (RA) in adults aged 65 and older. Commonly, doctors use methotrexate for treating RA initially. This is not always suitable for older patients who have other health problems. We investigated whether leflunomide is a suitable alternative in this age group by comparing the effectiveness and safety of the two drugs over 6 months. We reviewed the medical records of 167 patients aged 65 years with RA who were starting their first-ever RA medication. Eighty patients took leflunomide, and 87 took methotrexate. More patients on methotrexate saw their arthritis activity scores drop significantly. However, by the end of 6 months, there was no difference between patients taking methotrexate and those on leflunomide. The number of patients who reached a state of low disease activity or remission (where symptoms are minimal or gone) was similar in both groups. Additionally, the number of people who stopped their medication was similar for both drugs. However, when researchers accounted for the fact that patients starting methotrexate tended to have more severe arthritis at the beginning, patients were more likely to stay on methotrexate long-term. The results demonstrated that the chance of stopping leflunomide was almost four times higher than stopping methotrexate. Both medications were generally safe. The need to stop either medication due to adverse events was low (10 out of 100 patients on leflunomide and 8 out of 100 patients on methotrexate); some patients on methotrexate experienced nausea, while some patients on leflunomide experienced anemia. For older adults with RA, methotrexate remains the preferred first choice because it powerfully reduces disease activity, and patients are more likely to stay on it. However, leflunomide is a good alternative if methotrexate is not suitable because of other health conditions or side effects.
Introduction
Rheumatoid arthritis (RA) is the most common chronic inflammatory disorder. The prevalence is approximately 2% among individuals aged ⩾60 years in the United States. 1 This demographic comprises two distinct groups: patients with late-onset RA, defined as disease onset after the age of 60 years, and those with earlier-onset RA who have subsequently reached older age. 2 The population of elderly patients with RA is expanding, largely because of increased life expectancy and the rising incidence of late-onset RA.2,3
The efficacy of disease-modifying antirheumatic drugs (DMARDs) in treating RA has been demonstrated in several randomized controlled trials.4–6 However, elderly patients, who constitute a substantial proportion of the RA population, are poorly represented in clinical trials. In an observational study of 33,373 patients, less than one-third of the patients with late-onset RA used DMARD as their initial treatment. 7 Treatment options and treat-to-target strategies for older patients vary among countries and centers. In a study by Matsui et al., which tracked treatment trends longitudinally, the use of methotrexate gradually decreased, whereas that of biological/targeted synthetic DMARDs increased in patients with late-onset RA. 8 Managing RA in elderly patients is challenging. Comorbidities, polypharmacy, and a decreased glomerular filtration rate (GFR) influence treatment management strategies. Furthermore, a patient’s state of cognitive function may also guide treatment choice. Importantly, RA significantly impacts the patient’s quality of life. Therefore, effective management is crucial. The benefits of the treat-to-target approach must be carefully balanced against the risk of adverse events, heightened by the prevalence of comorbidities in elderly patients. Polypharmacy is also common among elderly RA patients, complicating treatment protocols and increasing the likelihood of drug interactions, adverse events, and contraindications due to hepatic and renal dysfunction.
Despite these complexities, the effects of DMARDs in elderly RA patients have not been a primary research focus. Methotrexate is the gold standard for treating RA, but it may not always be the best option for older patients. Leflunomide may be more preferable in certain cases. To date, comparative data on the effectiveness and safety of these drugs in elderly patients are limited.
Effective treatment strategies and the choice of effective DMARDs may improve clinical outcomes in older patients. However, evidence to support the safety and feasibility of using different DMARDs in elderly RA patients is required. Current treatment guidelines are based on limited evidence, and gaps in knowledge remain, especially for older adults with RA. This study aimed to compare the efficacy and safety of methotrexate and leflunomide in treating patients aged ⩾65 years with RA who started treatment with either drug.
Methods
This retrospective cohort study was conducted at the Balıkesir Ataturk City Hospital. Data (2024–2025) were collected from the medical records of the rheumatology clinic. This study was reviewed and approved by the Institutional Review Board for Ethics in Human Research (protocol number: 2025/08/89).
DMARD-naive patients with RA aged ⩾65 years, who fulfilled the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) 2010 classification criteria for RA, 9 were recruited between January 2024 and January 2025. The inclusion criteria were DMARD-naïve patients with RA aged ⩾65 years who initiated treatment with methotrexate or leflunomide and maintained treatment for at least 6 months. The exclusion criteria were concomitant use of methotrexate and leflunomide, previous use of DMARDs, GFR <30 mL/min/1.73 m2, and additional autoimmune rheumatological disease diagnosis, such as Sjögren’s disease, systemic lupus erythematosus, vasculitis, scleroderma, and RA. Low-dose prednisone (⩽5 mg/day) and non-steroidal anti-inflammatory drugs were administered during the study period. Concomitant medications had to be stable for ⩾3 months.
The study groups were not individually or frequency-matched. Instead, the analysis adjusted for age and sex as covariates in the multivariable regression models to control for any potential imbalance, as their distributions were comparable at baseline.
The number of tender and swollen joints, visual analog scale (VAS) scores, and physician global assessment of the disease were analyzed. The swollen joint count (SJC) and tender joint count (TJC) each constitute 28 joint counts. The VAS and Patient Global Assessment of Disease Activity were assessed using a 10-cm scale.
Rheumatoid factor (RF) levels were measured using nephelometric analysis (Siemens Dade Behring N2, Marburg, Germany), and values of >20 IU/mL were considered positive. Anti-cyclic citrullinated peptide (anti-CCP) antibodies were measured using an enzyme-linked immunosorbent assay (Cobas e411, Roche Diagnostics, Mannheim, Germany). According to the manufacturer’s reference range for this assay, levels >17 IU/mL were defined as positive. C-reactive protein (CRP) was measured using a high-sensitivity immunoturbidimetric assay (Roche Diagnostics), with results expressed in mg/dL. The specific assay manufacturer and reference ranges are based on our institution's standard laboratory protocols. Seropositive RA was defined as patients with positive results for either RF or CCP.
Laboratory assessments included complete blood counts, liver tests (aspartate aminotransferase and alanine aminotransferase), serum creatinine/GFR, and CRP levels. Laboratory data were recorded at baseline and at 4th, 12th, and 24th weeks.
Radiographs of the hands and feet were obtained at the first visit. The term “erosive disease” indicates that an erosion is seen in at least three separate joints at any of the following sites: the proximal interphalangeal, metacarpophalangeal, wrist (counted as one joint), and metatarsophalangeal joints on radiographs of both hands and feet, as defined in the 2010 ACR/EULAR RA classification criteria. 10
By the 4th week, all patients on methotrexate had reached a dose of 15 mg/week (with folate supplementation), and those on leflunomide had reached 20 mg/day. Both groups were maintained at these doses and monitored.
Disease activity was measured using the Disease Activity Score 28 (DAS28)-CRP 11 scores. Remission and low disease activity (LDA) were assessed using American College of Rheumatology criteria in both groups after 24 weeks. 12 Disease activity was categorized by remission as DAS28-CRP < 2.6 and LDA as DAS28-CRP 2.6–3.2 at the 24th week of treatment.
Patients whose treatment was discontinued owing to adverse events within 6 months of treatment were identified, and the adverse events leading to drug discontinuation were recorded. Drug survival was calculated for the period between the start of treatment and the 24th week.
We followed patients for drug-related adverse events, such as nausea, vomiting, elevated liver enzymes, mucosal ulcers, hair loss, rash, anemia, lymphopenia, thrombocytopenia, interstitial pneumonitis, hypertension, neuropathy, and renal impairment, which are the most common causes of drug withdrawal.
This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 13 Statement (Supplemental Table 1).
Statistical analysis
Statistical analysis was performed using SPSS Statistics (version 20.0; SPSS Inc., Chicago, IL, USA). Chi-square, Fisher’s exact, t-test, and Wilcoxon rank-sum tests were performed to compare demographic data, efficacy, and adverse events. Significant independent variables in univariate analyses were tested using multivariate stepwise regression models. The results are expressed as odds ratios (ORs) in logistic regression models and regression coefficients in linear regression models. The 95% confidence interval (95% CI) was calculated, and a p-value <0.05 was considered significant.
A post hoc power analysis was performed based on the final cohort of 167 patients (80 treated with leflunomide and 87 treated with methotrexate). The post hoc power for the primary comparison (discontinuation rate) was 42% based on Cohen’s h = 0.257.
Binary logistic regression was used to identify the factors associated with discontinuation at 24 weeks (yes/no). Time-to-event analysis was performed using Kaplan–Meier and Cox proportional hazards regression for drug survival.
The proportional hazard assumption was tested using Schoenfeld residuals.
Missing data were handled using a complete-case analysis. No imputation methods were employed as the missingness was minimal (<5% for all variables).
Results
Study population and baseline characteristics
A total of 167 elderly patients with RA were included in this cohort. Of these, 80 patients received leflunomide and 87 received methotrexate. The baseline characteristics of the study population are summarized in Table 1. The median age of the patients in the leflunomide and methotrexate groups was 65 years (interquartile range [IQR]: 65–71.5) and 67 years (IQR: 65–70; p = 0.897), respectively. Sex distribution was similar between the groups, with females accounting for 76.3% of the leflunomide group and 70.1% of the methotrexate group (p = 0.237). The median symptom duration was 3 years (IQR: 1–7) in the leflunomide group and 3 years (IQR: 1–5) in the methotrexate group (p = 0.373). The two groups were comparable in terms of seropositivity rate and the proportion of patients with erosive disease at baseline. At baseline, the SJC, TJC, and VAS scores were similar between the groups.
Baseline characteristics of the study population.
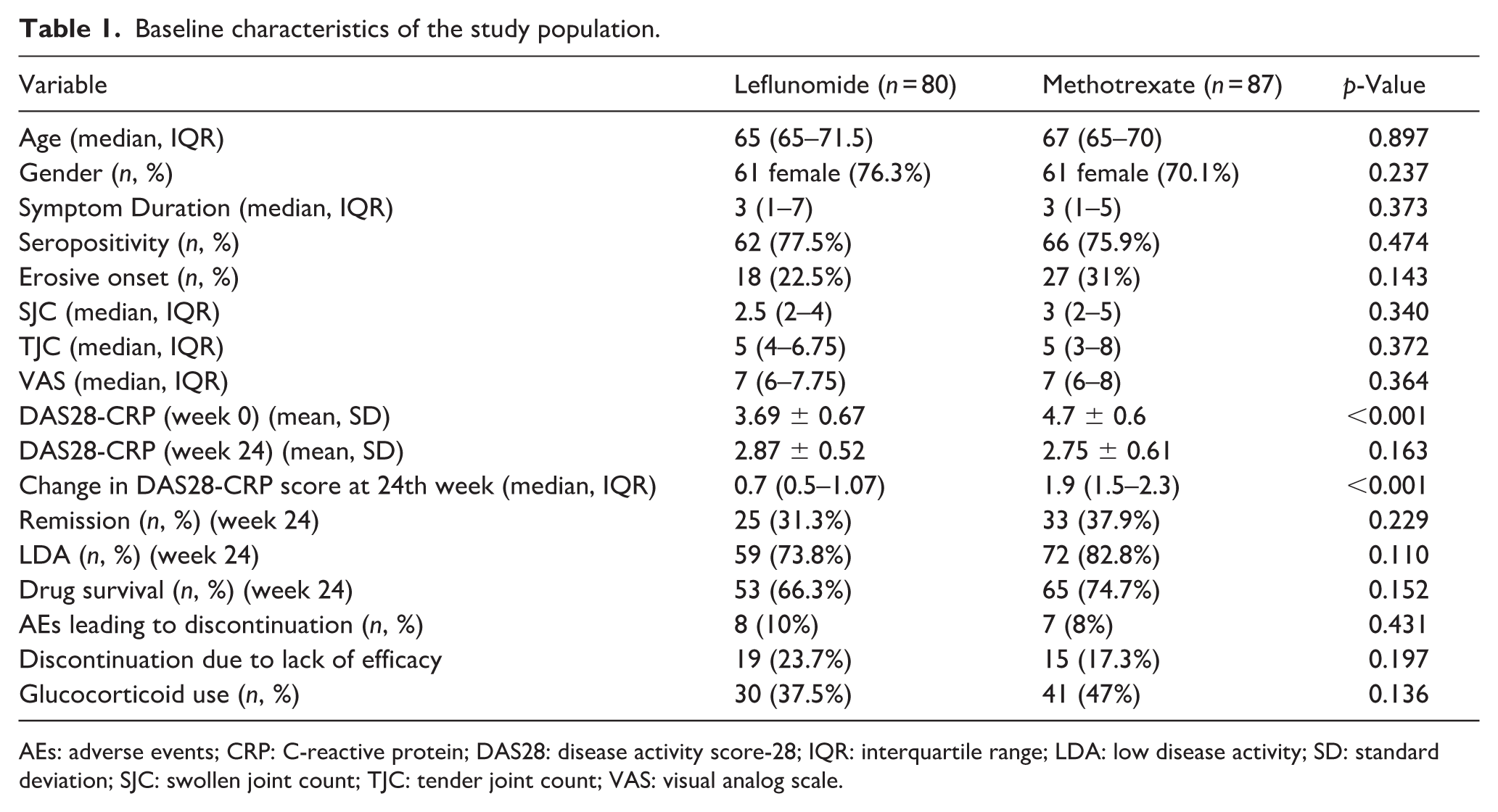
AEs: adverse events; CRP: C-reactive protein; DAS28: disease activity score-28; IQR: interquartile range; LDA: low disease activity; SD: standard deviation; SJC: swollen joint count; TJC: tender joint count; VAS: visual analog scale.
Over a median follow-up of 24 weeks, 33.7% (27/80) of the leflunomide-treated patients and 25.3% (22/87) of the methotrexate-treated patients discontinued treatment. The absolute difference in the 24-week discontinuation rate was 8.4% in favor of methotrexate (95% CI 5.1% to +21.9%, p = 0.23). Reasons for discontinuation included lack of efficacy (23% for leflunomide and 17% for methotrexate) and adverse events (10% for leflunomide and 8% for methotrexate).
Disease activity and treatment effectiveness
The baseline DAS28-CRP scores were significantly different between the two groups. The leflunomide group had a mean score of 3.69 ± 0.67, while the methotrexate group scored 4.7 ± 0.6 (p < 0.001). Over 24 weeks, the change in DAS28-CRP scores was higher in the methotrexate group, with a median reduction of 1.9 (IQR: 1.5–2.3) compared to 0.7 (IQR: 0.5–1.07) in the leflunomide group (p < 0.001). Although not statistically significant, the rates of remission (31.3% vs 37.9%, p = 0.229) and LDA (73.8% vs 82.8%, p = 0.110) at 24 weeks were higher in the methotrexate group.
Multistep regression analysis was used to predict remission and LDA scores. In both groups, SJC was significantly associated with remission (p < 0.001), with ORs of 3.984 and 1.447. In the leflunomide group, higher baseline DAS28-CRP scores were associated with LDA (p = 0.0034, OR = 6.901) (Table 2).
Univariate and multivariable logistic regression analyses of factors associated with remission and LDA in elderly RA patients treated with methotrexate and leflunomide.
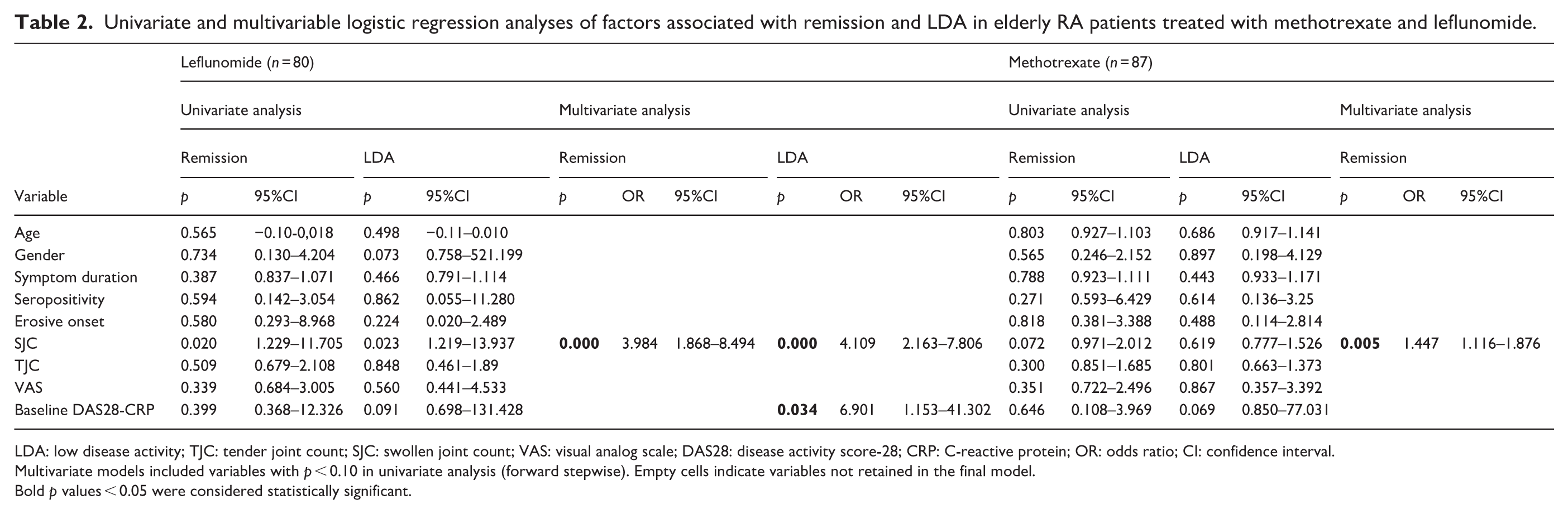
LDA: low disease activity; TJC: tender joint count; SJC: swollen joint count; VAS: visual analog scale; DAS28: disease activity score-28; CRP: C-reactive protein; OR: odds ratio; CI: confidence interval.
Multivariate models included variables with p < 0.10 in univariate analysis (forward stepwise). Empty cells indicate variables not retained in the final model.
Bold p values < 0.05 were considered statistically significant.
Drug survival and adverse events
Drug survival, defined as the proportion of patients remaining on the initial treatment, was comparable between the leflunomide and methotrexate groups (66.3% vs 74.7%, p = 0.152). Drug survival analysis indicated that SJC (p < 0.001, OR = 2.132) and VAS (p = 0.043, OR = 2.017) scores were associated with drug survival in the leflunomide group. In the methotrexate group, baseline DAS28-CRP score was associated with drug survival (p = 0.02, OR = 3.928) (Table 3).
Univariate and multivariable logistic regression analyses of factors associated with drug discontinuation at week 24.
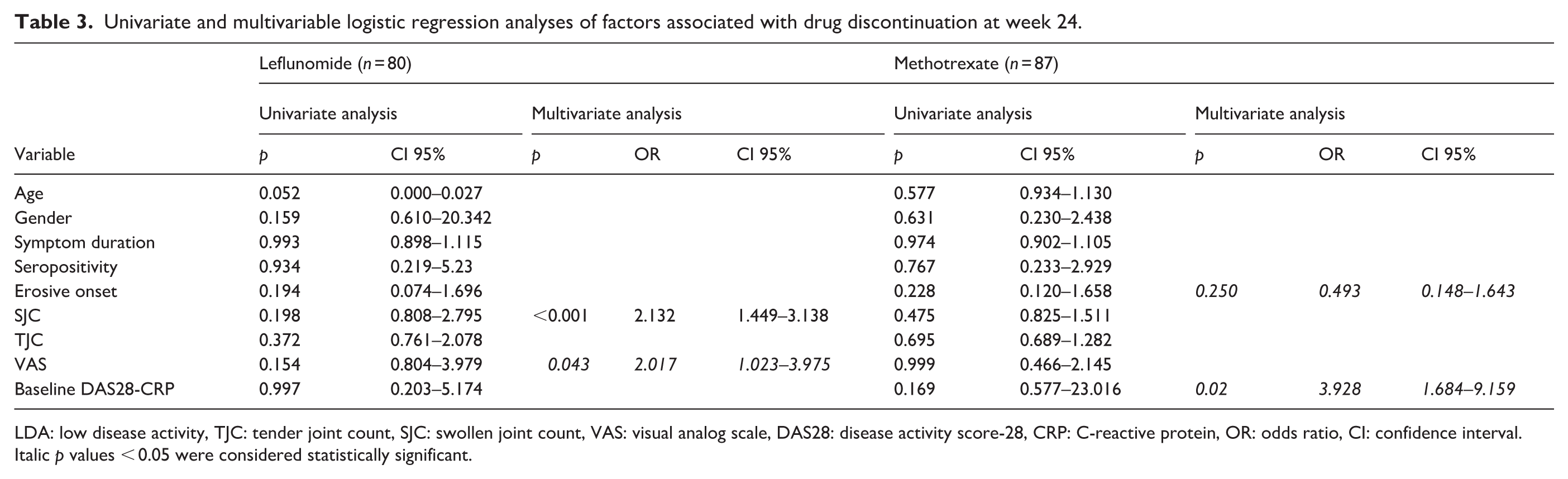
LDA: low disease activity, TJC: tender joint count, SJC: swollen joint count, VAS: visual analog scale, DAS28: disease activity score-28, CRP: C-reactive protein, OR: odds ratio, CI: confidence interval.
Italic p values < 0.05 were considered statistically significant.
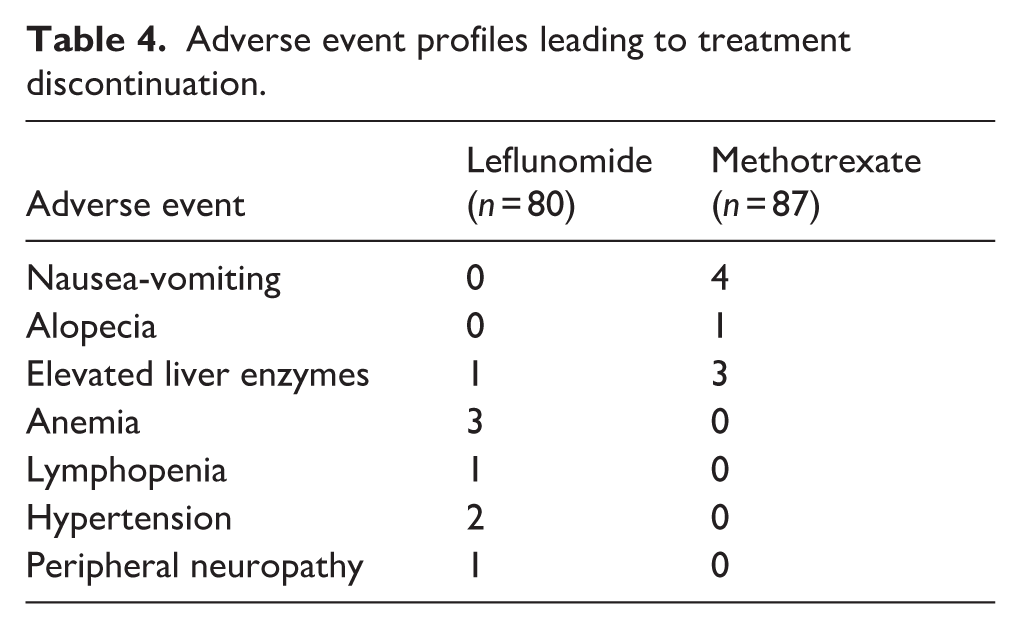
Adverse events leading to treatment discontinuation were similar between groups (p = 0.431). Treatment-specific adverse events that caused drug discontinuation included nausea and vomiting (four patients on methotrexate), elevated liver enzymes (one on leflunomide and three on methotrexate), and anemia (three on leflunomide; Table 4).
Adverse event profiles leading to treatment discontinuation.
Unadjusted survival analysis
Kaplan–Meier analysis revealed a non-significant trend toward better drug survival with methotrexate (log-rank p = 0.407) (Figure 1). Univariate Cox regression yielded a hazard ratio (HR) of 0.80 (95% CI 0.46–1.40, p = 0.43), indicating a 20% reduction in discontinuation hazard with methotrexate compared to leflunomide, but did not reach statistical significance.
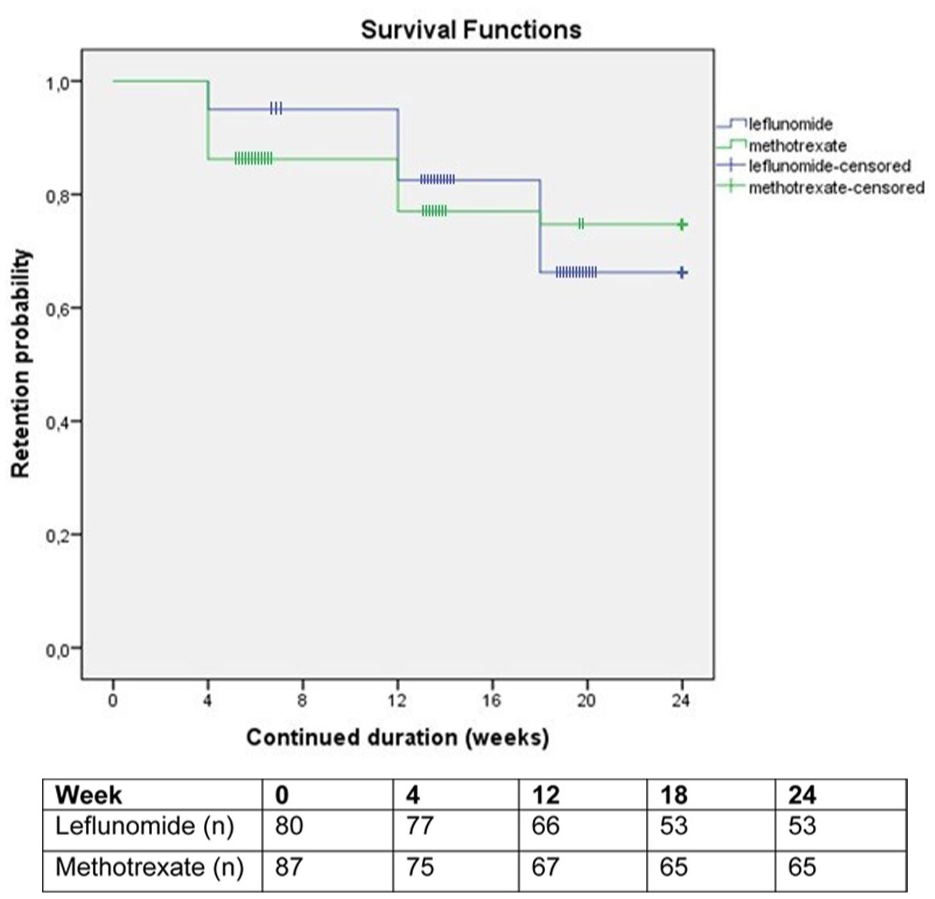
Kaplan–Meier curve showing the drug retention rates.
Adjusted Cox proportional hazards model
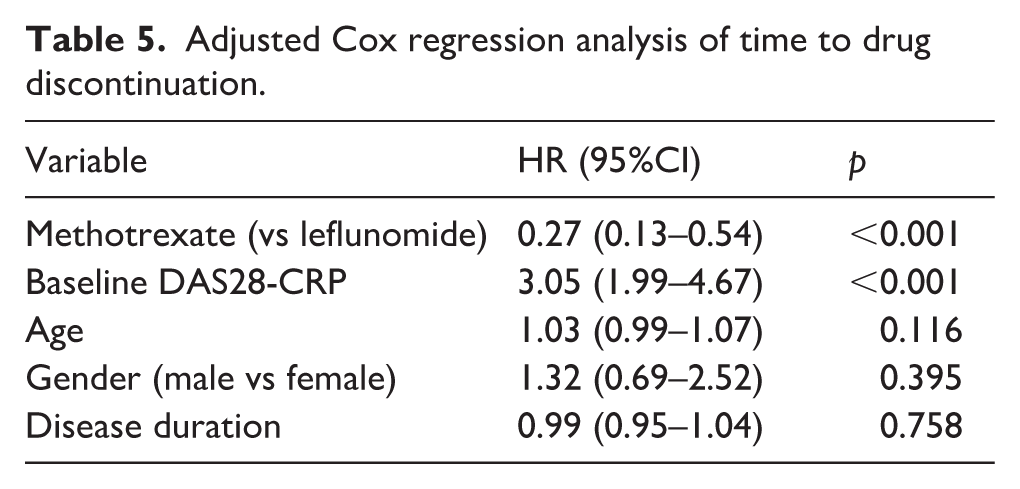
After adjusting for age, sex, disease duration, and baseline DAS28-CRP in a multivariate Cox model, methotrexate was associated with a 73% reduction in discontinuation hazard compared to leflunomide (adjusted HR 0.27, 95% CI 0.13–0.54, p < 0.001). Baseline DAS28-CRP was the strongest independent predictor of discontinuation, with each 1-unit increase associated with a 3.05-fold higher hazard of discontinuation (95% CI 1.99–4.67, p < 0.001). Age, sex, and disease duration were not significant predictors of discontinuation (Table 5). The proportional hazards assumption was not violated (global Schoenfeld test, p = 0.32).
Adjusted Cox regression analysis of time to drug discontinuation.
Discussion
To our knowledge, this is the first real-world study to compare the effectiveness and safety data between leflunomide and methotrexate in DMARD-naïve patients with RA aged ⩾65 years. Our findings indicate that while methotrexate demonstrated a significantly greater reduction in disease activity scores, both treatments achieved key clinical outcomes such as remission, LDA, and drug survival at 24 weeks. Furthermore, the safety profiles of both drugs were acceptable and consistent with their known toxicity spectra.
The significantly greater reduction in DAS28-CRP among those on methotrexate is noteworthy. This finding aligned with methotrexate’s established position as a first-line anchor drug in RA treatment guidelines. 14 However, the clinical relevance of this difference was tempered by the fact that the final disease activity scores at 24 weeks and the rates of remission and LDA were not significantly different between the two groups. The higher baseline DAS28-CRP level in the methotrexate group may have contributed to the larger observed reduction due to regression to the mean, a phenomenon that could partly explain the between-group differences in absolute change scores. Nevertheless, after adjusting for baseline disease activity, methotrexate was associated with better adjusted drug survival. This suggested that leflunomide may be an effective therapeutic alternative for the elderly patient population, particularly when methotrexate is not tolerated or is contraindicated. Moreover, the higher baseline disease activity in the methotrexate group may have contributed to the larger observed change in the DAS28-CRP level, a phenomenon known as regression to the mean. In a comparative study by Emery et al., methotrexate appeared to be more effective in the first year of RA treatment, whereas no difference was observed between the two treatment arms by the end of the second year, which is similar to the data in our study. 15 This may reflect varying patient responses and the multifactorial nature of achieving remission in patients with RA.
One of the key findings of our study was the identification of baseline SJC as a strong and consistent predictor of positive treatment response and improved drug survival, specifically for leflunomide. Patients with a higher baseline SJC were significantly more likely to achieve remission in both treatment groups. In addition, a higher baseline DAS28-CRP score was associated with LDA levels in the leflunomide group. This differential predictive value could aid in personalizing treatment choices for elderly patients with RA.
Observational studies have shown that the disease activity and treatment responses are similar in elderly and young patients with RA.16,17 A pooled analysis of 11 methotrexate clinical trials showed that advanced age and renal impairment had no effect on the efficacy of methotrexate. 18 The Swedish Farmacotherapy (SWEFOT) trial showed that the likelihood of an EULAR response to methotrexate in patients with new-onset RA increased with age. 19 Another study on patients with rheumatoid and psoriatic arthritis showed that advancing age had no impact on the efficiency of leflunomide treatment. 20 Consistent with previous data, in our study, patients with RA treated with methotrexate and leflunomide appeared to have a higher rate of remission or LDA. These results indicated that the effectiveness of the drug did not decrease with advancing age.
Although efficacy studies of methotrexate in elderly RA patients have not shown a difference compared to younger patients,21–23 there have always been concerns about adverse events.24–26 Safety analysis revealed that both drugs were generally well tolerated, with low and comparable rates of discontinuation due to adverse events. The adverse event profile of methotrexate is dominated by gastrointestinal intolerance (nausea/vomiting) and hepatotoxicity, which have been well documented. 27 The observed adverse events of leflunomide, including hypertension, anemia, and cytopenia, were consistent with known safety profiles. 28 The occurrence of these events underscores the importance of regular monitoring of blood pressure, complete blood count, and liver function tests in elderly patients receiving DMARDs. In a population-based study, increased age was associated with an increased risk of methotrexate discontinuation in patients newly diagnosed with RA. 24 Sugihara et al. found that methotrexate-associated adverse events were observed in 60.5% of patients with late-onset RA during the 3 years of observation. 29 In a retrospective series of patients with RA treated with leflunomide with 2 years of follow-up, the adverse events and survival rates were similar between patients aged <65 years and those aged ⩾65 years. 20 In our study, the rate of adverse events leading to drug discontinuation was very low in both drug groups during the 24-week treatment period.
While unadjusted analyses showed only a modest, non-significant advantage for methotrexate, multivariate adjustment revealed a pronounced and statistically significant benefit, with methotrexate being associated with a 73% lower risk of discontinuation than leflunomide. This dramatic shift in the magnitude of the effect after adjustment highlights substantial confounding by indication, whereby patients with higher baseline disease activity, a strong predictor of discontinuation, were more likely to receive methotrexate.
The marked change in the hazard ratio after multivariate adjustment, from a non-significant 0.80 in the unadjusted analysis to a significant 0.27 in the adjusted model, warrants careful interpretation. This substantial shift strongly suggests the presence of confounding by indication, where clinicians preferentially prescribed methotrexate to patients with higher baseline disease activity, a factor strongly associated with discontinuation. While our model adjusted for key measured covariates, including baseline DAS28-CRP, we cannot fully exclude the possibility of residual confounding from unmeasured variables, such as frailty, cognitive status, or detailed comorbidity burden, which may influence both treatment choice and outcomes in this elderly population.
Our finding that the baseline DAS28-CRP level was the strongest predictor of drug discontinuation (HR 3.05 per unit) aligns with previous evidence that higher disease activity correlates with poorer treatment persistence.30–32 This may reflect either reduced efficacy or greater susceptibility to adverse events in patients with more active diseases. Importantly, after accounting for this and other covariates, methotrexate demonstrated better adjusted drug survival, which is consistent with some prior comparative trials in general RA populations, although our effect size was larger than previously reported. 20
Our study has some limitations. First, the retrospective design could increase the potential for selection bias and confounding factors between the groups. Although we employed regression analyses to control these factors, residual confounding factors could not be entirely ruled out. Second, the sample size, although reasonable, may have been insufficient to detect small but clinically meaningful differences in secondary outcomes, such as the remission rate. Non-significant differences between remission and LDA may be due to insufficient power (type II error) rather than true equivalence. Third, our follow-up of 24 weeks to assess long-term drug survival and late-onset adverse events was relatively short. Extended observations are required to confirm whether the superior adjusted drug survival of methotrexate persists beyond 6 months. A longer observation period would provide more robust data on drug survival and late-onset adverse events. Fourth, the substantial baseline difference in DAS28-CRP between the groups limited the direct comparison of absolute change in scores. Although multivariate adjustment was applied, residual confounding and regression of the mean could not be fully excluded. Therefore, in the future, studies using propensity score matching are warranted. Fifth, our adverse event reporting was limited to events that led to treatment discontinuation. Mild or moderate adverse events that did not result in drug cessation were not systematically collected from patient records, which may underestimate the total burden of treatment-related toxicity. This represents a limitation inherent to the retrospective design.
Conclusion
This study demonstrated that both leflunomide and methotrexate are viable treatment options for elderly RA patients. While methotrexate was associated with a greater reduction in DAS28-CRP, both drugs achieved similar rates of remission and low disease activity at 24 weeks. After adjusting for baseline disease activity, methotrexate demonstrated better adjusted drug survival. However, due to the notable baseline differences in disease activity and the lack of statistical significance for key clinical endpoints, clinicians should consider methotrexate as a reasonable first-line option for RA patients aged 65 and older in the absence of contraindications, with vigilant monitoring. Leflunomide remains a valuable alternative when methotrexate is not suitable.
Supplemental Material
sj-doc-1-taj-10.1177_27558428261463661 – Supplemental material for Comparative effectiveness and safety of leflunomide versus methotrexate in the treatment of elderly rheumatoid arthritis patients: A retrospective cohort study
Supplemental material, sj-doc-1-taj-10.1177_27558428261463661 for Comparative effectiveness and safety of leflunomide versus methotrexate in the treatment of elderly rheumatoid arthritis patients: A retrospective cohort study by Esra Dilsat Imrak, Ilknur Aktas and Alev Cetin Duran in Sage Open Chronic Disease
Footnotes
Ethical considerations
The protocol was approved by the institutional ethics review board of Balıkesir Ataturk City Hospital (protocol number: 2025/08/89, date:21/08/2025).
Consent to participate
In line with the approval of the institutional ethics review board of Balıkesir Ataturk City Hospital, a waiver of informed consent was granted. Consequently, no direct patient contact was made, and individual consent was not required.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, E.D. Imrak, upon reasonable request.*
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.