
Abstract
Aim:
This study was conducted to determine the effect of footbath on premenstrual syndrome (PMS), sleep quality, and quality of life in university students with PMS.
Materials and Methods:
This randomized controlled trial was conducted during the 2021–2022 academic year with students from the Faculty of Education at a university in the Black Sea Region of Turkey. Data were collected between November 2021 and June 2022. Following screening with the Premenstrual Syndrome Scale (PMSS), 78 students were randomly assigned to the intervention (n = 39) and control (n = 39) groups using a computer-generated sequence (1:1 ratio). Before starting the intervention, the Pittsburgh Sleep Quality Index (PSQI) and the SF-36 Quality of Life Scale (SF-36) were applied to both groups. Students in the intervention group received footbaths with water at 38°C–42°C every night for 7–10 days during the premenstrual phase of each cycle for three menstrual cycles. The control group received no intervention. The PMSS, PSQI, and SF-36 were readministered at the end of each cycle. The primary outcome was the change in PMSS scores; secondary outcomes included PSQI and SF-36 subscales. Data were analyzed using descriptive statistics, the Shapiro–Wilk test, and a two-way mixed ANOVA.
Results:
Post-test mean scores of the PMSS and its subscales (depressive mood, anxiety, fatigue, irritability, depressive thoughts, pain, and sleep changes) showed statistically significant differences between the intervention and control groups (p < 0.05). While a significant within-group improvement in PSQI scores was observed in the intervention group, no statistically significant between-group difference in sleep quality was found (p > 0.05). For the SF-36 subscales, bodily pain, vitality (energy), role emotional, and mental health scores significantly improved in the intervention group compared with the control group (p < 0.05).
Conclusion:
Footbath was found to reduce PMS symptoms and improve quality of life in students with PMS. However, it did not lead to a statistically significant improvement in sleep quality when compared with the control group.
Introduction
Premenstrual syndrome is a recurrent condition characterized by a variety of physical, emotional, behavioral, and cognitive symptoms that typically appear during the late luteal phase of the menstrual cycle and subside within a few days after the onset of menstruation. 1 Clinical manifestations include physical symptoms such as breast tenderness, bloating, headaches, heart palpitations, and increased appetite, as well as behavioral and psychological symptoms such as aggression, irritability, depression, fatigue, suicidal ideation, mood swings, poor concentration, and social withdrawal. 2 The prevalence of PMS is difficult to determine due to the heterogeneity of its symptoms. 3 Reported prevalence rates range from 7.1% to 99.5%.2,4–10 PMS can significantly affect women’s mental, physical, and functional capacities, thereby impairing their work performance and social interactions.
Sleep disturbances are a critical factor associated with PMS and have the potential to impair cognitive and psychomotor performance. 11 Studies among university students indicate that individuals with PMS are more likely to experience poor sleep quality11–13 and a diminished quality of life14–16 due to their symptoms.
Nonpharmacologic interventions for PMS management include cognitive behavioral therapy, exercise, yoga, reflexology, massage, aromatherapy, phytotherapy, chiropractic care, acupuncture, and acupressure.17–25 One such intervention is a warm footbath, a simple and accessible practice that can be applied at any time. 26 Warm footbaths have been shown to reduce sympathetic nervous system activity while enhancing parasympathetic activity in healthy individuals. This modulation of autonomic nervous system function may improve sleep quality and overall quality of life, providing both relaxation and physical comfort. 27 Furthermore, the application of warm or hot water to the whole body or specific areas, such as during showering, has been reported to relieve nervous tension associated with PMS. 28
Although some studies have compared the effects of hot footbaths and foot reflexology in alleviating PMS symptoms, 29 there remains a notable gap in the literature regarding the impact of footbaths on premenstrual symptom severity, sleep quality, and quality of life among university students diagnosed with PMS.
Study hypotheses
Students with PMS in the footbath intervention group during the premenstrual period will exhibit lower PMS symptom severity compared with students in the control group.
Students with PMS in the footbath intervention group during the premenstrual period will experience improved sleep quality in comparison with students in the control group.
The physical function of quality of life in students with PMS in the footbath intervention group during the premenstrual period will be better than those in the control group.
The social function of quality of life in students with PMS in the footbath intervention group during the premenstrual period will be better than that of students in the control group.
The pain level of quality of life in students with PMS in the footbath intervention group during the premenstrual period will be lower than that of students in the control group.
The vitality (energy) level of quality of life in students with PMS from the footbath intervention group during the premenstrual period will be higher than that of students in the control group.
The role limitation (emotional) level of quality of life in students with PMS from the footbath intervention group during the premenstrual period will be better than that of students in the control group.
The role limitation (physical) level of quality of life in students with PMS from the footbath intervention group during the premenstrual period will be better than that of students in the control group.
The mental health level of quality of life in students with PMS in the footbath intervention group during the premenstrual period will be higher than that of students in the control group.
Students with PMS in the footbath intervention group during the premenstrual period will exhibit better quality of life and an overall perception of health than students in the control group.
Methods
Design and participants
This study employed a single-blind, randomized controlled experimental design. It was conducted among female students enrolled at the Faculty of Education in a state university located in the Black Sea Region of Türkiye during the academic year 2021–2022. Initially, 747 female students volunteered for the study and underwent screening involving sociodemographic questions and the PMSS. Out of the 510 students who expressed a willingness to proceed to the next phase of the study, 151 students who scored 111 points or more on the PMSS were randomly selected based on predefined inclusion and exclusion criteria (see Fig. 1).
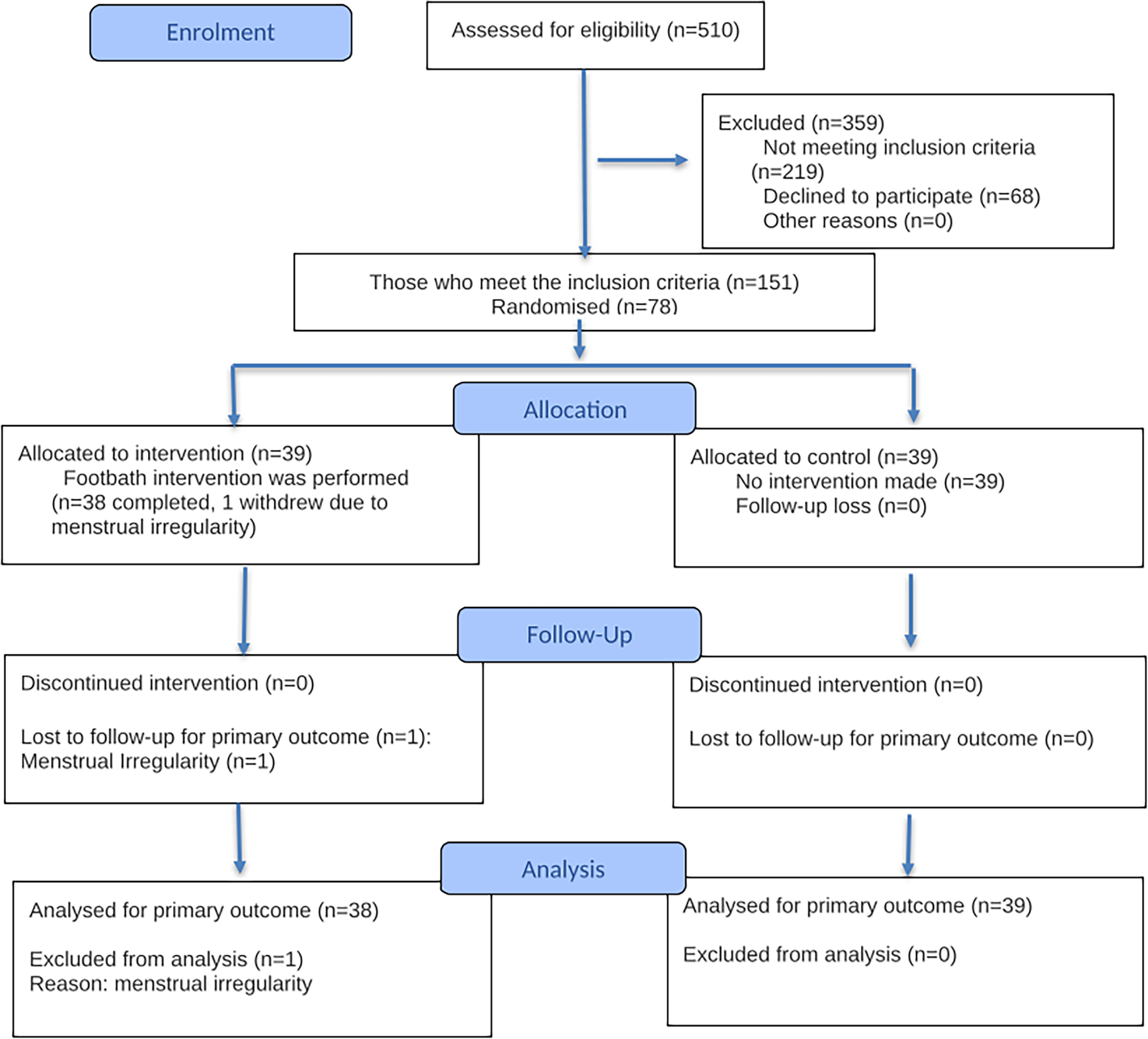
Shows the recruitment flowchart.
Study group size and power analysis
The sample size of this randomized controlled trial was determined through power analysis using the G-Power 3.1.9.7 software program (with an effect size of 0.8, a significance level of α = 0.05, and a power of 0.95). Based on power analysis, the minimum required sample size was calculated as 70. Taking into account potential data loss, 78 students were randomized (39 intervention, 39 control) (see Fig. 1). Randomization was performed via computer.
During the study period, one student from the intervention group was withdrawn from the study due to menstrual irregularity. Thus, 77 students (38 intervention, 39 control) completed the study. Compliance with the intervention group was monitored daily via WhatsApp, and it was confirmed that all participants performed the footbath as specified in the protocol.
Analyses were conducted on participants who completed the protocol; therefore, the study was conducted using a per-protocol (PP) analysis. One student from the intervention group who withdrew from the study due to menstrual irregularity corresponds to a very low dropout rate of 1.3% (1/78). Therefore, missing data are not considered to be significant enough to affect the study results.
Inclusion criteria
Participants were required to be 18 years or older, score 111 points or higher on the PMSS, be single, have a regular menstrual cycle (menstruation occurring every 21–35 days with no intermittent bleeding complaints) for the past 6 months, have a body mass index (BMI) ranging from 19 to 24.9, not smoke or consume alcohol, have not received medical treatment for PMS, have not been treated for insomnia, and express a willingness to participate in the study.
Exclusion criteria
Participants with a psychiatric diagnosis, gynecologic disease, regular exercise habits, and those using hormonal contraception (e.g., oral contraceptives and injections) were excluded from the study.
While the study was continuing, one student from the intervention group was excluded from the study due to menstrual irregularity. The study resulted in 38 students in the experimental group and 39 students in the control group.
Randomization and blinding randomization
To reduce selection bias and control variables that could affect the results, 78 students were randomly assigned to the experimental and control groups by a statistician who did not know the names and characteristics of the students. Which group was the intervention or control group was determined by drawing lots. The data of the intervention and control groups were coded as A and B and recorded in the statistical package program. The data were entered into the statistics program by someone else under the control of the thesis advisor, who had no role in the interventions and measurements. The statistician analyzed the data without knowing which group the data belonged to (see Fig. 1).
Data collection tools
Descriptive information form
The descriptive information form includes questions about sociodemographic characteristics, menstrual traits, daily habits, and the overall health status of the students.
Premenstrual Syndrome Scale
Premenstrual Syndrome Scale, developed by Gençdoğan in 2006, 30 utilizes a five-point Likert scale with 44 items. The scale comprises nine subdimensions, namely “depressive sensation,” “anxiety,” “fatigue,” “irritability,” “depressive thoughts,” “pain,” “appetite changes,” “sleep changes,” and “bloating.” Scoring on the PMSS involves summing up scores from all subdimensions, ranging from a minimum of 44 to a maximum of 220. The presence or absence of PMS is determined by surpassing 50% of the PMSS total score, with an additional criterion of a total score of 111 points and above indicating the presence of PMS. 30 The reliability of the scale is measured by Cronbach’s alpha, with an overall scale value of 0.75 and subdimension values ranging from 0.75 to 0.91. Specific to this study, Cronbach’s alpha values were found to be 0.916, 0.938, 0.942, and 0.964 during the pretest and all follow-ups, respectively. Subdimension Cronbach alpha values varied between 0.651 and 0.910 in the T1, 0.738 and 0.892 in the T2, 0.734 and 0.888 in the T3, and 0.787 and 0.911 in the T4.
Pittsburgh Sleep Quality Index
Pittsburgh Sleep Quality Index developed by Buysse et al. 31 and adapted into Turkish by Ağargün et al. 32 comprises seven subdimensions. Each subdimension score, indicating symptom severity, ranges 0–3. The PSQI total score, obtained by summing the subscales, ranges from 0 to 21 points. A PSQI score of five points and below suggests “good sleep” quality, while six points and above indicate “poor sleep” quality. The original Turkish study reported a Cronbach’s alpha of 0.80, 32 and in this study, Cronbach’s alpha values for T1 PSQI were 0.702, 0.750 in the T2, 0.783 in the T3, and 0.827 in the T4.
SF-36 Quality of Life Scale
The SF-36 developed by Ware et al. 33 and adapted into Turkish by Koçyiğit et al. 34 consists of eight subscales and 36 questions. Subscales include “physical functioning,” “role physical,” “bodily pain,” “general health,” “vitality (energy),” “social functioning,” “role emotional,” and “mental health.” Each subscale is scored independently between 0 and 100 points, with higher scores indicating better health status. In the original study, Cronbach alpha values for subscales ranged between 0.7324 and 0.7610. 34 In the present study, Cronbach’s alpha values ranged between 0.552 and 0.848 in the T1, 0.640 and 0.855 in the T2, 0.717 and 0.825 in the T3, and 0.560 and 0.853 in the T4.
Data collection
The data were collected between November 2021 and June 2022. The students were first informed about the study, and their informed consent was obtained. After the students were screened for PMS, random assignments were made to the groups among the students who met the inclusion criteria. The researcher conducted individual interviews with the students in the groups to get information about the research and to have them sign the informed consent forms. During the interviews, the estimated menstruation dates of the students in both groups were recorded. The students were administered the PSQI and the SF-36 to complete the pretest data before the intervention. Each student in the intervention group received a foot bathtub, a liquid thermometer, a paper towel, and a footbath follow-up chart. PMSS, PSQI, and SF-36 were administered to the students in both groups during three menstrual cycles and at the end of each menstruation.
Footbath equipment
For the footbath application, a nonelectric, plastic bathtub with a width of 35 × 35 cm and a depth of 15 cm, a liquid thermometer to measure the temperature of the water, paper towels to dry the feet, and a footbath follow-up chart to record the application information were used.
Interventions
The footbath application phase of the research was carried out between January 1 and June 30, 2022. In separate interviews with each student, students were given training on how to apply the footbath. The application was performed by the students during 7–10 days in the premenstrual period by bathing their feet in warm water with a temperature between 38°C and 42°C for 20 min before going to bed at night. The depth of water was 10 cm above the ankle of the participants. The students were sent a reminder WhatsApp message every day by the researcher, 7–10 days before their estimated menstruation dates. The students notified the researcher that they applied the footbath via WhatsApp message, recorded the application information in the follow-up chart, and submitted it to the researcher. Students in the intervention group applied footbaths in the luteal phase for three menstrual cycles. At the end of each menstrual period, PMSS, PSQI, and SF-36 scales were applied to the students. Thus, after receiving pretest data from the students, they were monitored for three menstrual cycles. No application was made to the students in the control group. After obtaining pretest data from the students in the control group, they were monitored for three menstrual cycles.
Ethical considerations
Written permission was obtained from the authors of the scales used in this study via e-mail and from the Faculty of Education where the research was conducted (date: 5.10.2021 and number E.0654653). Approval was obtained from the Ordu University Clinical Research Ethics Committee (date: November 5, 2022, and number 2022/236) for research applications. Students who agreed to participate in the study were informed about the research, and their written consent was obtained. The research was conducted in accordance with the principles of the Declaration of Helsinki. Clinicaltrials.gov was registered for the research (NCT05264519).
Data analysis
The data analysis involved the application of descriptive statistical methods to both numerical and categorical data. For numerical data, measures such as mean, standard deviation, and median were employed, while categorical data were assessed using frequency and percentage. The normal distribution of the data was examined through the Shapiro–Wilk test.
The primary outcome of the study was the change in PMSS scores. The secondary outcomes included the PSQI scores and the SF-36 subscales. The analysis plan was prespecified, and the primary outcome was prioritized in hypothesis testing. While multiple comparisons were performed across scales and subscales, no formal correction (e.g., Bonferroni or Benjamini–Hochberg) was applied beyond Bonferroni-adjusted post hoc tests in simple main effects analyses, as the primary outcome was clearly designated and secondary analyses were exploratory.
The PMSS was predefined as the primary outcome, while the PSQI and SF-36 subscales were designated as secondary outcomes. Exploratory analyses were limited to examining the subscales of the PMSS and SF-36, interpreted as hypothesis-generating rather than confirmatory. No subgroup, adjusted, or sensitivity analyses were conducted beyond these prespecified analyses. A Bonferroni correction was applied for multiple time comparisons within groups.
Inferential statistics were conducted using the two-way mixed ANOVA model, with careful consideration of the necessary assumptions. The analysis employed SPSS v24 and R package programs, with a significance level set at p < 0.05. Effect size statistics were utilized for interpreting hypothesis test results in comparing the mean scores of scales. The study included two nearly equal groups, and any assumption violations in relevant test statistics were disregarded, adhering to the results of the two-way mixed ANOVA model. In cases where a statistically significant group*time interaction effect was observed, the total effect of these variables was ignored, even if the effect of only time and only group variables was statistically significant. If the joint effect was significant, the mean values varied across time for the control or intervention groups. Interpretations were based on simple main effects analyses in this context. Differences in the time variable were determined using Bonferroni-corrected multiple comparison tests for each group.
Results
A total of 78 students were randomized (39 intervention, 39 control). During the study, one participant in the intervention group withdrew due to menstrual irregularity, resulting in 77 students (38 intervention, 39 control) completing the study. All analyses were conducted on a PP basis, including only participants who completed the intervention as assigned. For each outcome, the number of participants analyzed was identical (n = 38 in the intervention group and n = 39 in the control group) at all four measurement points (T1–T4), as no missing data occurred for any of the primary or secondary outcomes (PMSS, PSQI, SF-36). Therefore, no data imputation was required.
According to the results, there were no statistically significant differences between the intervention and control groups concerning various factors such as age, BMI, age at menarche, grade, place of residence, maternal education level, income level, presence of diagnosed anemia, coffee and acidic beverage consumption, duration, and frequency of menstruation (p > 0.05) (Table 1).
Comparison of Students’ Basic Characteristics (Sociodemographic, Habit, Menstrual) (n = 77)
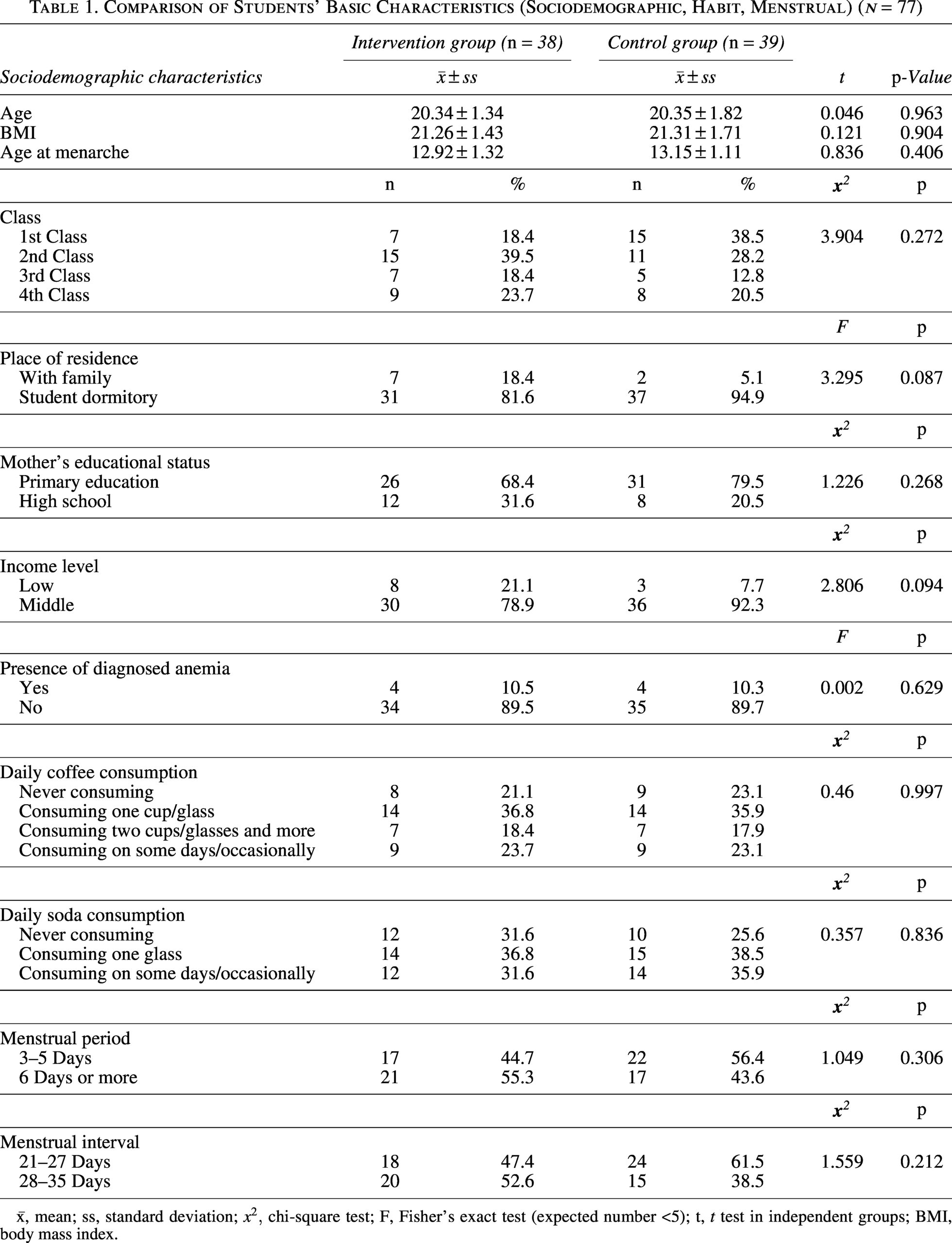
x̄, mean; ss, standard deviation;
The intra- and intergroup comparison of the mean scores of the PMSS and its subscales
In the study, it was determined that the group*time joint effect was statistically significant for the total mean PMSS score (p < 0.01, η2 = 0.10). A statistically significant difference was observed between the means of the intervention and control groups in terms of the time variable (p < 0.01, η2 = 0.47 and p < 0.01, η2 = 0.17). It was determined that the intervention group PMSS mean score was significantly lower than the control group at T4 (p < 0.01, η2 = 0.12) (H1 accepted) (Table 2).
Comparison of Premenstrual Syndrome Scale Score Mean of Students Within and Between Groups
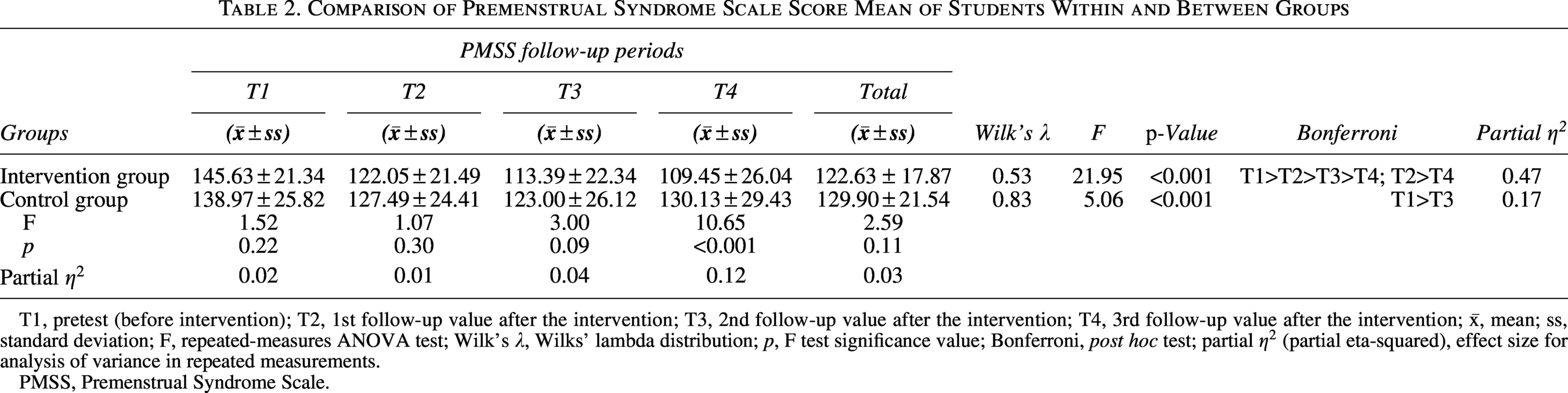
T1, pretest (before intervention); T2, 1st follow-up value after the intervention; T3, 2nd follow-up value after the intervention; T4, 3rd follow-up value after the intervention; x̄, mean; ss, standard deviation; F, repeated-measures ANOVA test; Wilk’s λ, Wilks’ lambda distribution; p, F test significance value; Bonferroni, post hoc test; partial
PMSS, Premenstrual Syndrome Scale.
The group*time joint effect was statistically significant for the depressive sensation, anxiety, fatigue, irritability, and depressive thoughts subdimensions of the PMSS. However, it was not significant for appetite changes, pain, sleep changes, or bloating subdimensions.
For the PMSS “depressive mood” subdimension, the within-group mean score differences in terms of time variable in the control and intervention groups were found to be statistically significant (p < 0.05, η2 = 0.13 and p < 0.01, η2 = 0.37, respectively), while there was a significant difference between the groups only at T4 (p < 0.01, η2 = 0.10) (Table 3).
Comparison of Premenstrual Syndrome Scale Subdimension Score Mean of Students Within and Between Groups
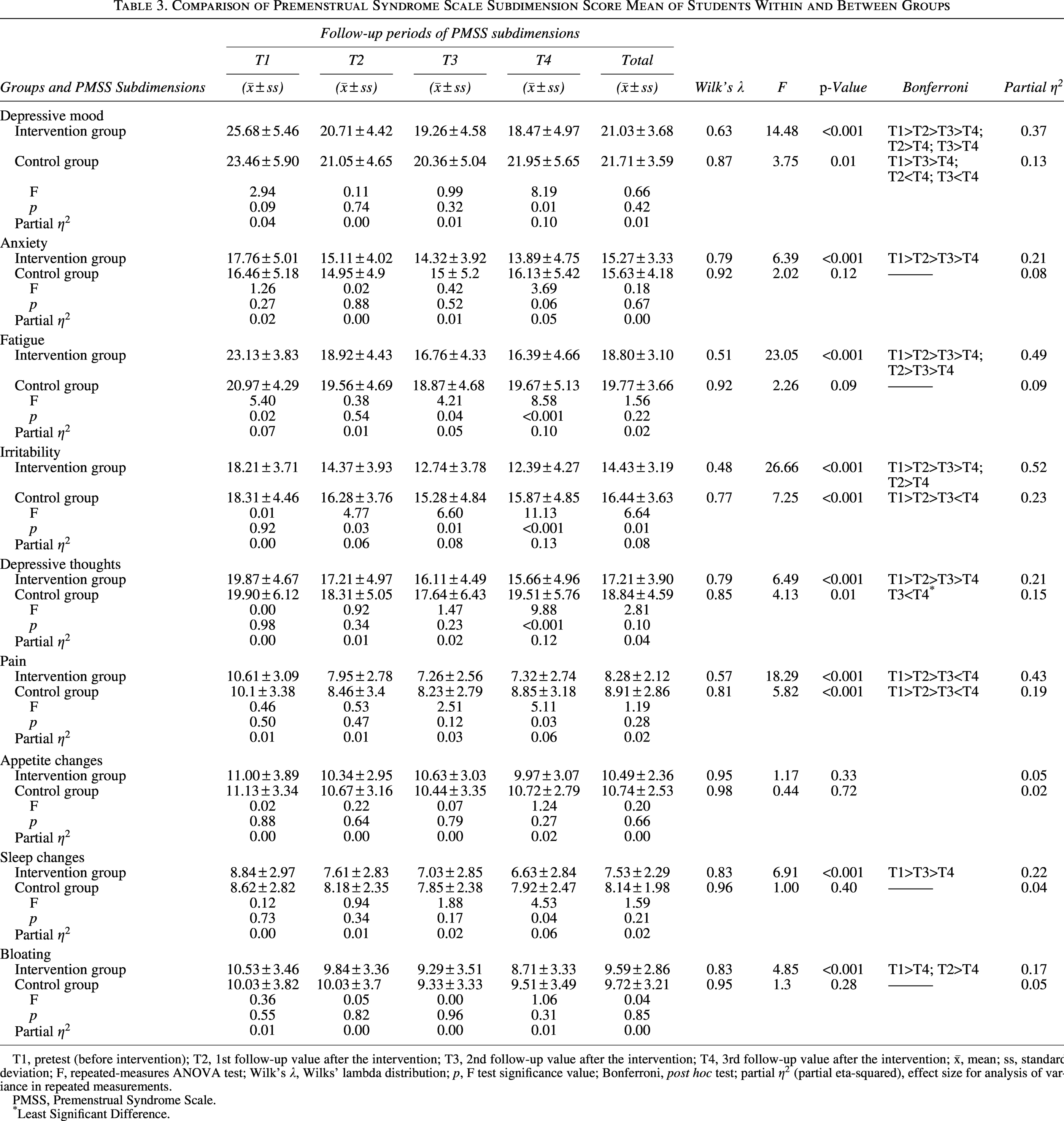
T1, pretest (before intervention); T2, 1st follow-up value after the intervention; T3, 2nd follow-up value after the intervention; T4, 3rd follow-up value after the intervention; x̄, mean; ss, standard deviation; F, repeated-measures ANOVA test; Wilk’s λ, Wilks’ lambda distribution; p, F test significance value; Bonferroni, post hoc test; partial
PMSS, Premenstrual Syndrome Scale.
Least Significant Difference.
For the “anxiety” subdimension of PMSS, intragroup (time) variability was observed only in the intervention group (p < 0.01, η2 = 0.21), and there was no significant difference between the groups (p > 0.05) (Table 3).
For the “fatigue” subdimension of the PMSS, within-group (time) variability was found only in the intervention group (p < 0.01, η2 = 0.49), with significant differences between groups at T1, T3, and T4 (p < 0.05, η2 = 0.05, and p < 0.01, η2 = 0.10, respectively) (Table 3).
A statistically significant difference was observed between the mean scores of the “irritability” subdimension of PMSS in terms of the within-group time variable of the intervention and control groups (p < 0.01, η2 = 0.23 and p < 0.01, η2 = 0.52, respectively). A significant difference was determined between the groups at T2, T3, and T4 (T2: p < 0.05, η2 = 0.06; T3: p < 0.05, η2 = 0.08; T4: p < 0.05, η2 = 0.13) (Table 3).
A statistically significant difference was observed between the mean scores of the “depressive thoughts” subdimension of PMSS in terms of the within-group time variable of the intervention and control groups (p < 0.05, η2 = 0.15 and p < 0.01, η2 = 0.21, respectively). A significant intergroup difference was found only at T4 (p < 0.01, η2 = 0.12) (Table 3).
A statistically significant difference was observed between the mean scores of the PMSS “pain” subdimension of the intervention and control groups in terms of the within-group time variable (p < 0.05, η2 = 0.15 and p < 0.01, η2 = 0.21, respectively). A significant difference was found between the groups only at T4 (p < 0.01, η^2 = 0.06) (Table 3).
No statistically significant intergroup difference was observed for the “sleep changes” subdimension of the PMSS (p > 0.05, η2 = 0.02). However, the time effect was found to be statistically significant regardless of the group variable (p < 0.01, η2 = 0.11) (Table 3).
No statistically significant intergroup difference was observed for the “bloating” subdimension of the PMSS (p > 0.05, η2 = 0.00); however, the time effect was statistically significant independent of the group variable (p < 0.01, η2 = 0.07) (Table 3).
Intra- and intergroup comparison of PSQI mean scores
The combined effect of time*group and the independent group effect on PSQI mean scores was found to be statistically insignificant (p > 0.05). In the control group, no significant change in PSQI scores was observed over time (p > 0.05, η2 = 0.10). However, a significant within-group time effect was found in the intervention group (p < 0.05, η2 = 0.16), where the mean score at T1 was significantly higher than the scores at T3 and T4 (p < 0.05). Despite this within-group improvement, the absence of a significant time*group interaction indicates that the intervention did not produce a statistically significant effect on sleep quality compared with the control group (H2: rejected) (Table 4).
Comparison of Pittsburgh Sleep Quality Index Score Mean of Students Within and Between Groups
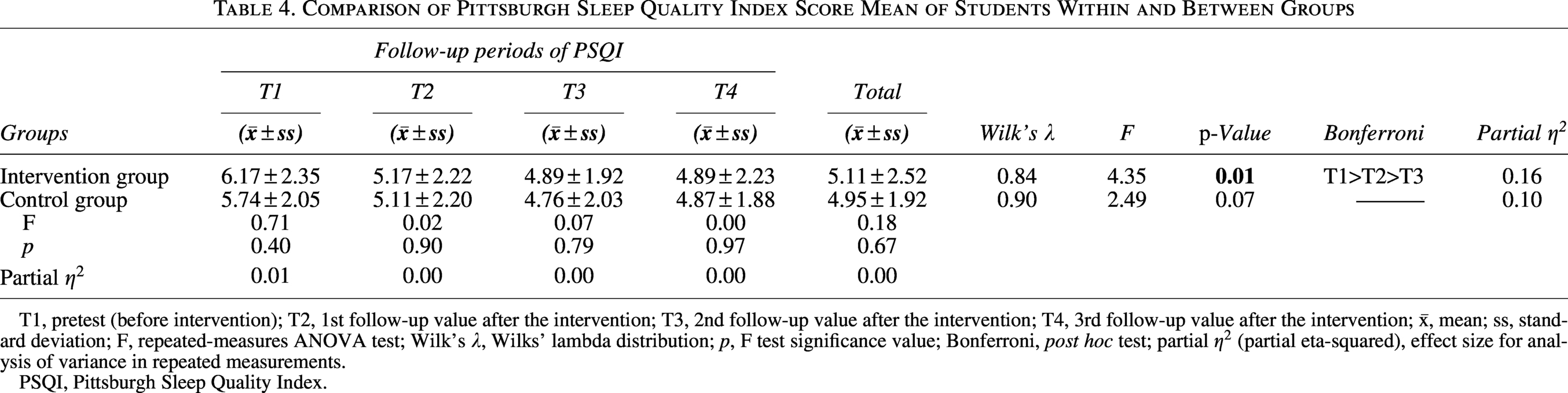
T1, pretest (before intervention); T2, 1st follow-up value after the intervention; T3, 2nd follow-up value after the intervention; T4, 3rd follow-up value after the intervention; x̄, mean; ss, standard deviation; F, repeated-measures ANOVA test; Wilk’s λ, Wilks’ lambda distribution; p, F test significance value; Bonferroni, post hoc test; partial
PSQI, Pittsburgh Sleep Quality Index.
Intra- and intergroup comparisons of the SF-36 mean scores
In this study, it was observed that the joint effects of time, group, and time*group on the means of the “physical function” and “social function” subscales of the SF-36 were not statistically significant (p > 0.05) (H3: rejected, H4: rejected) (Table 5).
Comparison of SF-36 Quality of Life Subscale Score Mean of Students Within and Between Groups
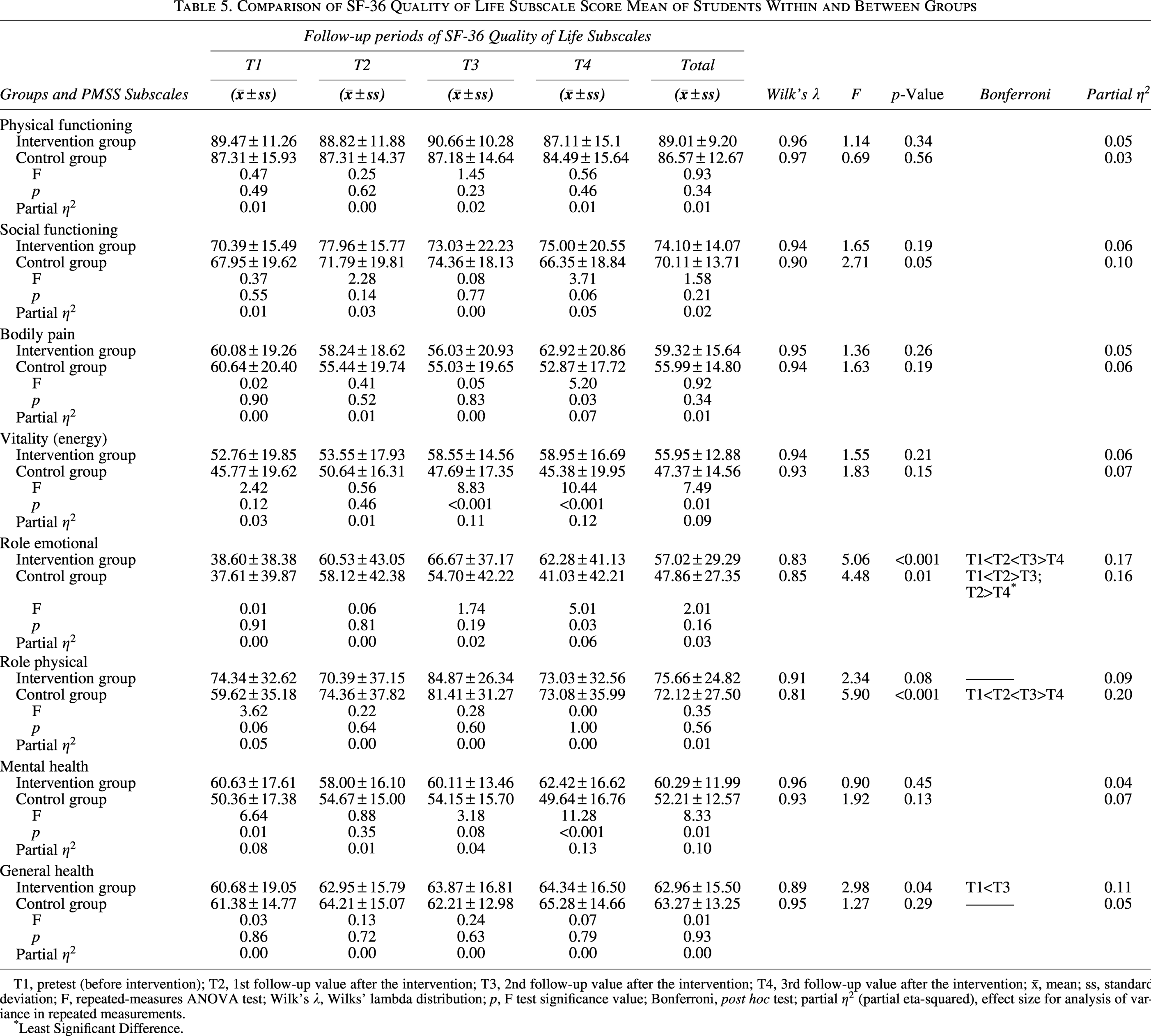
T1, pretest (before intervention); T2, 1st follow-up value after the intervention; T3, 2nd follow-up value after the intervention; T4, 3rd follow-up value after the intervention; x̄, mean; ss, standard deviation; F, repeated-measures ANOVA test; Wilk’s λ, Wilks’ lambda distribution; p, F test significance value; Bonferroni, post hoc test; partial
Least Significant Difference.
The joint effect of group, time, and group*time on the mean scores of the “bodily pain” subscale of the SF-36 was not statistically significant (p > 0.05). Regarding the main effects of the group variable on a time basis, although there was no statistically significant effect of the group variable in total, a statistically significant difference was observed between the groups in T4 means (p < 0.05, η2 = 0.07) (H5: accepted) (Table 5).
In the SF-36 “vitality (energy)” subscale mean scores, it was observed that the time*group joint effect and the time effect independent of the group variable were statistically insignificant (p > 0.05), but the group effect independent of time was statistically significant (p < 0.05, η2 = 0.09). Accordingly, the mean of the intervention group was found to be statistically significant and higher than the mean of the control group in terms of total (p < 0.05). The simple main-effect analyses were examined for the group variable based on time, and the basis of the difference observed in terms of total was that the control group mean scores were statistically significantly lower than the intervention group mean scores at T3 and T4 (T3: p < 0.01, η2 = 0.11, T4: p < 0.01, η2 = 0.12) (H6: accepted) (Table 5).
In the SF-36 “role emotional” subscale mean scores, the time*group joint effect was not statistically significant (p > 0.05, η2 = 0.02). Similarly, no statistically significant differences were observed between the control and intervention groups (p > 0.05, η2 = 0.03). When the main effects of the time variable were analyzed on a group basis, the overall differences indicated that the mean score at T1 in the intervention group was lower than at other time points (p < 0.01, η2 = 0.17), whereas in the control group, a statistically significant difference was observed only between the T1 and T2 mean scores (p < 0.05, η2 = 0.16). Regarding the main effects of the group variable based on time, although the overall test statistic between the groups was not statistically significant, a statistically significant difference was found between groups at the T4 mean scores (p < 0.05, η2 = 0.06) (H7: accepted) (Table 5).
The joint effect of time*group on the mean scores of the “role physical” subscale of the SF-36 was found to be statistically insignificant (p > 0.05, η2 = 0.03). Similarly, no statistically significant difference was observed in the means between the control and intervention groups (p > 0.05, η2 = 0.01). When the main effects of the time variable were examined on a group basis, no difference was observed between the mean scores of the “role physical” subscale for the time variable in the intervention group overall (p > 0.05, η2 = 0.09), while the means in the control group were found to be statistically significantly different in terms of the time variable (p < 0.01, η2 = 0.20) (H8: rejected) (Table 5).
In the SF-36 “mental health” subscale mean scores, it was observed that the time*group joint effect and the time effect, independent of the group variable, were statistically insignificant (p > 0.05), but the group effect, independent of time, was statistically significant (p < 0.05, η2 = 0.10). Accordingly, it was determined that the overall mean of the intervention group was statistically significant and higher compared with the control group mean (p < 0.05). When simple main-effect analyses for the group variable on a time basis were examined, the basis of the observed difference in terms of overall was the fact that the mean of the intervention group at T1 was statistically significantly higher compared with the control group mean (p < 0.05, η2 = 0.08). It was also observed that the mean of the intervention group at T4 was statistically significantly higher compared with the control group mean (p < 0.01, η2 = 0.13) (H9: accepted) (Table 5).
The joint effect of time*group on the mean scores of the “general health” subscale of the SF-36 was found to be statistically insignificant (p > 0.05, η2 = 0.01). Similarly, no statistically significant difference was observed in the means between the control and intervention groups (p > 0.05, η2 = 0.00). However, while no difference was observed between the means for the time variable in the control group (p > 0.05, η2 = 0.05), a statistically significant difference was determined between the means in the intervention group (p < 0.05, η2 = 0.11) (H10: rejected) (Table 5).
Discussion
This study aimed to investigate the effects of a footbath administered during the premenstrual period on PMS, sleep quality, and quality of life in university students with PMS. The study found that footbaths were effective in reducing the severity of PMS symptoms. Specifically, footbaths were found to alleviate symptoms such as depressed mood, anxiety, fatigue, irritability, depressive thoughts, pain, and sleep disturbances. These findings are consistent with the results reported by Abdeesso and Aruna, 29 a study focusing directly on PMS. This study demonstrated that a hot footbath was more effective than foot reflexology in reducing PMS symptoms. Furthermore, a study conducted by Wu et al. 27 on university students found that a footbath administered during the first days of menstruation reduced the severity of dysmenorrhea pain and improved autonomic nervous system activity. Although the study by Wu et al. 27 was not conducted directly on PMS, given the shared mechanisms between PMS and dysmenorrhea (e.g., pain and autonomic nervous system regulation), these findings indirectly support the results of the current study.
In this study, it was determined that while footbaths administered during the premenstrual period were effective in improving sleep quality over time in the intervention group, they did not improve sleep quality compared with the control group. In the literature, some studies conducted on healthy women have observed the positive effects of footbaths on sleep. For example, Hosona and Kano 35 reported significant improvements in the quality of awakening in the group that used hot water footbaths to a depth of 5 cm and in the ease of falling asleep in the group that used hot water footbaths to a depth of 15 cm in a study with healthy female university students; however, no significant difference was found between the two groups. Sung and Tochihara 36 reported that hot footbaths administered before bed in healthy women facilitated earlier sleep onset. These studies were not conducted on university students with PMS and were obtained from populations with different physiologic and psychological states. Therefore, these findings cannot be directly compared with the results of the current study. However, these results in the literature provide insight into the potential mechanisms of action on sleep quality and provide a contextual framework to explain the limited effect of footbaths in students with PMS.
PMS can negatively impact a woman’s physical and social activities, interfering with her interpersonal relationships and work productivity and affecting her quality of life. 37 This study found that footbaths administered to university students with PMS during the premenstrual period were effective in improving quality of life in terms of pain, vitality (energy), role emotional, and mental health. In particular, the significantly higher vitality (energy), mental health, pain, and role emotional scores in the intervention group compared with the control group indicate that footbaths may have positive effects not only on physical symptoms during the PMS period but also on mental well-being, emotional functioning, and energy levels. This result demonstrates that PMS affects quality of life in both its physical and psychological dimensions. However, footbaths were not effective in improving quality of life in terms of the physical function, social function, role physical, and general perception of health subscales of the SF-36. This result suggests that footbaths may have a limited effect on quality of life in these areas. Consistent with the findings of this study, a study by Park and Park 38 found that footbaths applied to patients with chemotherapy-induced peripheral neuropathy were more effective than foot massage in improving quality of life. A study by Kito and Suzuki 39 on patients with residual schizophrenia also found that footbaths and foot massages were effective in reducing daily life difficulties caused by psychiatric symptoms and improving quality-of-life scores.
Therefore, while the findings of the current study are consistent with the literature, it is important to note that the comparisons are indirect because they were made across different populations, and the mechanism of action may not be equally applicable to young women with PMS.
However, it is important to evaluate the results not only statistically but also clinically. Some of the changes in PMS symptom severity and quality-of-life subscales indicate small-to-moderate effect sizes based on η2 values. This suggests that, while statistically significant, they may have limited clinical impact on some subscales. There is currently no clearly defined minimal clinically meaningful change (MCID) for PMS; therefore, the clinical significance of the findings should be interpreted in the context of the implications of the observed mean differences for daily life. For example, improvements observed in symptoms such as depressed mood, anxiety, fatigue, and sleep disturbances may facilitate students’ social and academic functioning and thus provide clinically significant benefits. However, the lack of significant differences observed in areas such as social function or general health perception suggests that the intervention’s spectrum of effect may be limited.
In conclusion, the current study findings suggest that footbaths may be a useful nonpharmacologic method for reducing PMS symptoms and improving some quality-of-life domains. However, due to low effect sizes in some subscales and the lack of MCID data, the clinical generalizability of the results should be interpreted with caution. Future studies with larger samples and longer follow-up periods will more clearly demonstrate the clinical value of footbaths in the management of PMS.
Conclusion
This study explored the impact of footbaths applied during the premenstrual period on PMS, sleep quality, and overall quality of life in university students experiencing PMS. The findings revealed that footbath application led to a reduction in PMS symptoms and a significant improvement in overall quality of life. Although an improvement in sleep quality was observed within the intervention group, no statistically significant difference in sleep quality was found between the intervention and control groups.
The study suggests that footbath applications can serve as a self-administered and relaxing intervention for women dealing with PMS, which is not only user-friendly but also cost-effective and time efficient. In light of these findings, it is recommended that health care professionals, particularly nurses, inform students about the symptoms, prevalence, and coping strategies related to PMS; empower students to effectively cope with PMS; improve sleep quality; and enhance their overall quality of life through simple and accessible self-care practices.
Limitations
This study has several limitations. These include the following: The study results are valid only for the student group studied, and their generalizability to different regions or more heterogeneous groups is limited. Assessments of PMS, sleep quality, and quality of life were based on self-reported scales completed by students. This may pose a risk of recall and social desirability bias. The fact that students self-administered the footbath at home/dormitory may have led to incomplete compliance with variables such as application duration and water temperature. Because the measurements were limited to three menstrual cycles, long-term effects were not assessed. No intervention or placebo-equivalent activity was applied to the control group. This increases the risk of performance bias and makes it difficult to determine whether the improvements were due to the thermal component of the footbath or to nonspecific effects such as relaxation, expectancy, or increased attention. In future studies, the use of an active control group—such as a sham or placebo intervention—would be preferable to better control for these potential confounding factors.
In addition, this study involved multiple comparisons across different scales and subscales. While the PMSS was predefined as the primary outcome, no adjustment for multiple testing was applied for secondary outcomes and exploratory subscales. Therefore, significant findings in the PSQI and SF-36 domains should be interpreted with caution and considered exploratory.
Harms/adverse events
No adverse events or harms were reported by any participants during the study period. The footbath intervention was well tolerated, and none of the participants experienced discomfort, burns, skin irritation, or any other adverse reactions related to the procedure. Participants were informed that they could discontinue the intervention at any time in case of discomfort; however, no such cases occurred. Thus, no harm was observed or recorded throughout the study.
This finding is consistent with the safety expectations described in the prespecified protocol (NCT05264519).
Footnotes
Acknowledgments
The authors thank the students who participated in this study. They also thank Ordu University Scientific Research Projects Coordination Department for financial support. This study was submitted as an oral presentation at the 3rd International and 5th National Nursing History Congress, November 2–4, 2023, Izmir, Türkiye.
Author Disclosure Statement
No potential conflict of interest was reported by the authors.
Funding Information
The study was supported by funding from the Ordu University Scientific Research Projects Coordination Department with B-2140 project number.
Ethical Issues
Written permission was obtained from the authors for the scales used in this study via e-mail and from the Faculty of Education where the research was conducted (date: 5.10.2021 and number E.0654653). Approval was obtained from the Ordu University Clinical Research Ethics Committee (date: November 5, 2022, and number 2022/236) for research applications. Students who agreed to participate in the study were informed about the research, and their written consent was obtained. The research was conducted in accordance with the principles of the Declaration of Helsinki. Clinicaltrials.gov was registered for the research (NCT05264519).