
Abstract
Background:
The field of Traditional, Complementary, and Integrative Medicine (TCIM) is complex, comprising a diverse range of ethnomedical and non-ethnomedical therapeutic systems and practices whose primary shared characteristic is that they fall outside of the boundaries of Biomedicine’s standard of care in a particular context. To date, however, there has been no rigorously elaborated classification system to support scholars, educators, policymakers, and clinicians to meaningfully delineate the field’s features. This work, an operational typology of TCIM, fills that gap.
Methods:
Operational typologies are one form of operational definition in which a series of “ideal types” group phenomena with shared attributes into theoretically defined categories. As detailed in the first article of this three-part series (of which the current work is the second), the typology presented in the current article is built on a conceptual analysis of TCIM-related definitional indications provided by the World Health Organization (WHO). The WHO has for decades recognized the vital role of TCIM knowledges and practices in primary health care worldwide and continues to call for TCIM’s greater integration within national health systems. In addition, conceptual insights from sociological and anthropological scholarship support the typology’s design.
Results:
The typology has six primary “types”: (A) Orally Transmitted Ethnomedical Systems and Practices, (B) Codified Ethnomedical Systems and Practices, (C) Non-Ethnomedical Whole Systems, (D) Complementary Therapeutics, (E) Community-Based Therapeutics, and (F) Integrative Therapeutics. These types, which are understood as dynamic and permeable (rather than static and fixed), each have their own subtypes, meant to support more nuanced classifications.
Conclusion:
Readers interested in a more detailed account of the typology’s applications will refer to the third and fourth articles in this series.
Keywords
Preamble
This article, the second in a four-part series, presents an operational typology of Traditional, Complementary, and Integrative Medicine (TCIM). Operational typologies are classification systems 1 that “identify and cluster phenomena with shared characteristics and dimensions within groups, so as to clearly differentiate between groups, based on carefully-articulated theoretical foundations.” 2 TCIM is a diverse field that includes a wide and in many ways disparate range of therapeutic approaches whose primary shared characteristic is that they fall outside of the boundaries of Biomedicine’s i standard of care in a particular context. To date, no international classification system has offered conceptually rigorous tools to meaningfully classify the TCIM field’s diverse knowledge systems and therapeutic approaches in a way useful to scholars, educators, decision-makers, practitioners, and members of the public. This typology, theoretically built upon definitional indications provided by the World Health Organization (WHO), and informed by social science scholarship, aims to fill that gap.
The first article in the series 3 provides a detailed overview of the typology’s theoretical foundations, elaborating on three major conceptual domains upon which the typology is built (see the section “Conceptual Domains” of this article). Table 1 offers readers brief definitions of related key concepts. The current article presents the TCIM typology itself (made up of six TCIM types, each with its own subtypes). The third 30 and fourth articles 4 deepen discussion of the typology’s applications across a range of contexts. Readers may choose to read all four articles in sequence, or to engage with one or more of the articles as stand-alone scholarly works.
Glossary of Key Concepts in an Operational Typology of Traditional, Complementary, and Integrative Medicine
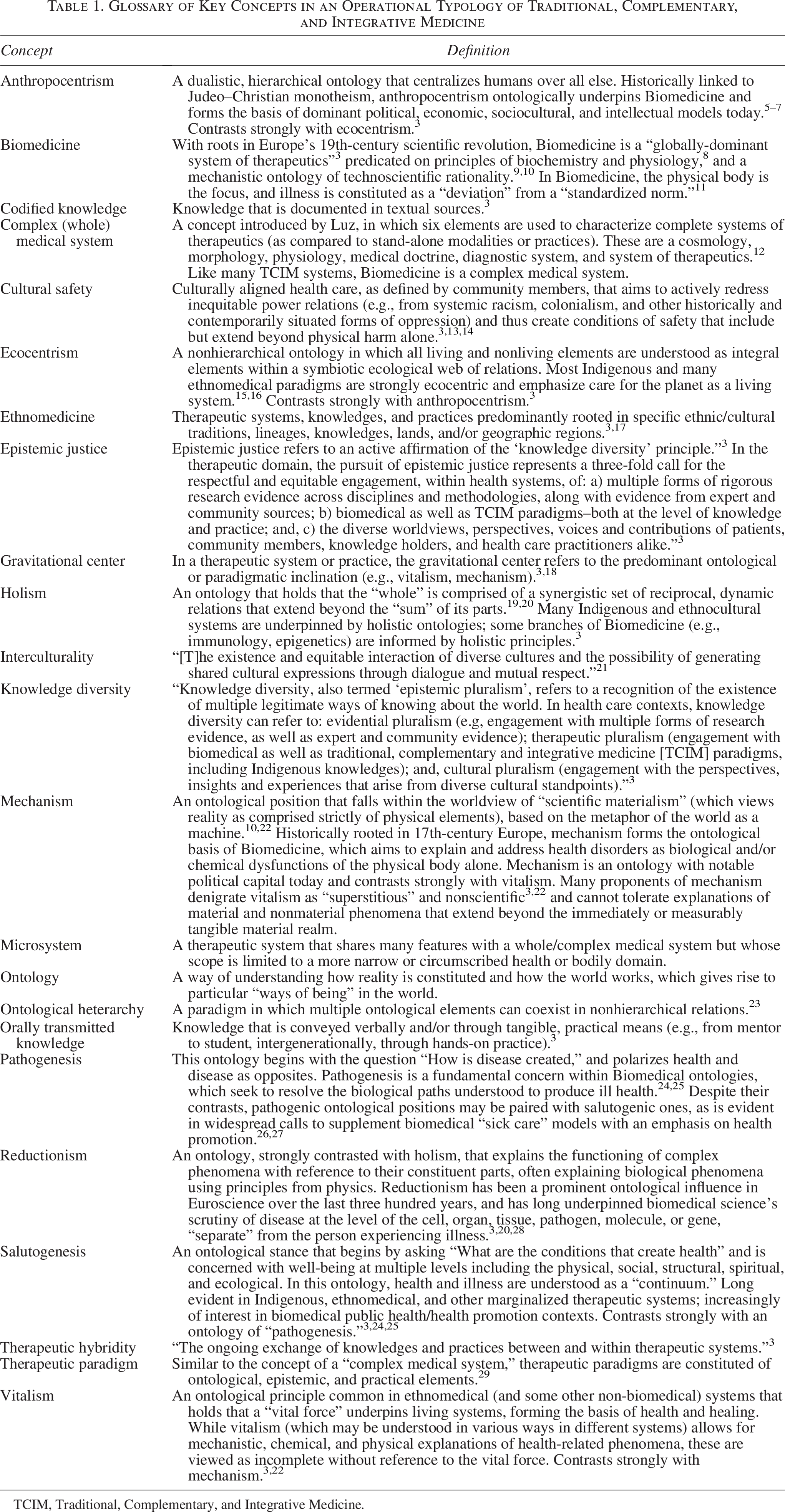
TCIM, Traditional, Complementary, and Integrative Medicine.
Overview: An Operational Typology of TCIM
An operational typology is one kind of operational definition. 1 The purpose of an operational definition is to make clear “whether a specific instance is or is not a member of [a] construct through a series of criteria.” 31 While the term “taxonomy” is sometimes used as a synonym for “typology,” “a typology is conceptual while a taxonomy is empirical.” 1 In other words, rigorously developed scholarly typologies: “a) subdivide a larger construct…into smaller sub-units, for classification purposes; b) have a strong theoretical, or conceptual basis (rather than being developed, as are taxonomies, on the basis of empirical research datasets).” 3
The construct being defined in the current work’s typology is TCIM: a large and internally diverse category that encompasses a wide range of notably different therapeutic approaches. These include, for example: Indigenous healing ceremonies, herbal teas as well as standardized herbal extracts, dietary supplements, acupuncture delivered alongside herbs and massage with reference to a Chinese medicine diagnosis, as well as biomedical styles of acupuncture.
How do such therapeutics relate to one another? How may researchers, decision-makers, health systems administrators, clinicians, or community members understand what these therapeutics may have in common and how they differ, what may unite or divide the field, and how to make sense of it all?
The operational typology presented in this work is meant to clarify these issues, providing meaningful categories that support various interest holders in critically navigating complex TCIM-related questions across the research, education, practice, and governance spheres. The typology is also meant to make visible, in a respectful and inclusive way, the diverse range of sociopolitically marginalized therapeutic knowledges and practices that continue to make important contributions to peoples’ health and well-being around the world.
To lend rigor to the typology’s construction, it must be made explicit from the outset that as a construct, neither the notion of TCIM—nor that of its referent, Biomedicine—is absolute or unproblematic. On one hand, the TCIM construct is essentially “a signifier of sociopolitical marginalization” 3 : a category that groups together all therapeutic approaches that fall outside Biomedicine’s boundaries (whether in a given context or more globally). This point does not, however, tell readers much about what the TCIM category may actually entail, in itself. In that regard, as elaborated in the previous article in this series, many TCIM approaches “are based on paradigmatic tenets that differ dramatically” from those that have historically underpinned Biomedicine 3 (e.g., ecocentrism, vitalism, holism, salutogenesis; see Table 1). The world of therapeutics, however, is dynamic and evolving. Today, the principle of holism is increasingly informing work in such biomedical fields as “epigenetics, immunology, network pharmacology,” and there are widespread calls within the public health field for an increased emphasis on salutogenesis. 3 Furthermore, there is a growing body of TCIM approaches that are philosophically inclining toward the kinds of mechanistic premises that have long underpinned Biomedicine. At a moment when the boundaries between therapeutic systems across the globe are increasingly breaking down, the need for a common language to discuss the nuances of therapeutic pluralism—such as proposed in this typology—is arguably greater than ever.
The TCIM category is globally recognized, including and in particular by influential bodies like the WHO. The WHO has long called for greater inclusion of TCIM knowledges and practices within national health systems, in recognition of TCIM therapeutics’ concurrent therapeutic and cultural importance around the world, including as a major form of primary health care.32–36 Further, as elaborated in the first article in this series, the WHO’s own TCIM-related theoretical definitions (“traditional and complementary medicine” and “Indigenous traditional medicine” 37 ) and definitional indications (for “integrative medicine” 35 ) incline away from biomedical dominance toward epistemic justice (defined in Table 1). 3 This is one central reason why the author has chosen to engage the WHO’s definitional work as a strong conceptual basis for this operational typology of TCIM. Other advantages for this approach are that the WHO definitions are: (1) “well-known to, and widely-cited by a large range of stakeholders worldwide”; (2) have “clear global applicability, rather than being limited to a particular region or context”; (3) are “inclusive enough to account for a wide range of therapeutic approaches that fall outside of Biomedicine’s standard of care”; and (4) are “conceptually rich…providing clear indications as to how” they might be “meaningfully operationalized.” 3
Informed by TCIM-related critical social science scholarship, the section “Conceptual Domains” of this article summarizes the detailed analysis of the WHO’s definitional indications which form the conceptual basis of this work’s operational typology. First, however, some brief additional notes about the typology’s specific features are needed here.
Typically, the categories or classes advanced in a conceptually driven operational typology are “both exhaustive and mutually exclusive,” with clear explanations of their theoretical dimensions and inclusion parameters provided. Further, as ideal types, typological classes may be further elaborated into subtypes (as they are in this work’s TCIM typology). However, as Weber has elaborated, ideal types rarely provide “perfect” representations of the cases classified within them, offering instead an approximation of such cases’ shared characteristics. 38 Between these approximations, there may well be gray areas between discrete types or subtypes that defy unequivocal categorization. Indeed, as anthropologists and sociologists have observed, efforts to statically “impose a bounded way of understanding the world” are characteristic of Eurocentric intellectual logics, 23 and permeable, interconnected categorizations are more evident in “epistemologies of the South” (from which many TCIM therapeutic approaches originate). 39 As such, this work’s typology conceptualizes its categories—its ideal types—as both interconnected and permeable. This approach recognizes that particular therapeutic systems, knowledges, and practices may dynamically occupy multiple spaces within the typology—at different temporal moments, in distinct contexts, and in the various forms they take.
The TCIM typology is meant to have broad and inclusive utility across diverse global contexts. This includes settings (such as those in many low- and middle-income countries) wherein TCIM therapeutics represent a primary form of accessible, affordable health care, including where biomedical care remains unavailable. 35 It also includes contexts (often but not exclusively in higher-income countries) in which TCIM therapeutics are preferentially used alone, or as a preventive or therapeutic supplement to Biomedicine, and sometimes as “elite medicine for the worried well.” 40
The typology is ultimately a tool intended to support work across various facets of the evidence-to-policy cycle in the TCIM field, including regulatory engagements, research designs, literature reviews, critical sociological and anthropological analyses, health services and workforce studies, as well as clinically focused investigations. It is meant to complement and inform (rather than replace) use of other operational tools in the field. Together, these tools may be fruitfully deployed to lend deepened rigor, integrity, and nuance to TCIM scholarship and governance. As an educational resource, the typology also provides a conceptually nuanced and historically informed basis for teaching and learning about the diverse worlds of global therapeutics. Let us now turn briefly to the typology’s conceptual foundations.
Conceptual Domains
The operational typology of TCIM presented in this series of articles is explicitly built with reference to four primary conceptual domains, which reflect the theoretical underpinnings of the WHO’s TCIM-related definitional indications, and related critical social science scholarship. The typology, presented in the current article and meant to support classification of a wide range of TCIM approaches, is built with explicit reference to the first three of these conceptual domains (Historical Factors, Paradigmatic and Cultural Features, and Knowledge Transmission Modes). As explained further below, the fourth domain, Health Systems Contexts, and its relevance to the typology’s application, is elaborated in more detail in the final article in this series. For a deeper discussion of the construction of the theoretical context of these domains, readers may return to the previous article.
The first domain, Historical Factors, recognizes that contemporary forms of TCIM arise out of a series of defined historical (and related political) factors.41,42 Although such factors will necessarily differ for each TCIM approach, and across regions, there are some common historical trends to recognize that support this work’s typological classifications. These include European colonization’s impacts, resulting in the globalized establishment of Biomedicine (and its affiliated knowledge system) as a politically dominant mode of health care around the world. These issues will be briefly discussed across the narratives explaining the typology’s various TCIM types and subtypes.
The second domain, Paradigmatic and Cultural Features, recognizes that all therapeutic approaches—including Biomedicine—have distinct affiliated worldviews, diagnostic and therapeutic practices, and cultural affiliations. 41 Accounting for these features, the typology categorically differentiates between ethnomedical and non-ethnomedical TCIM approaches (Table 1). This approach recognizes (among other issues) that some (ethnomedical) therapeutic approaches remain strongly connected to (though at times displaced from) particular lands, ecosystems, and/or ethnocultural communities. The typology also distinguishes between therapeutic approaches with a historical or contemporary conceptual gravitational center in ecocentric/vitalistic versus anthropocentric/mechanistic ontologies (Table 1). Related, the typology accounts for the fact that all therapeutic knowledges and systems (Table 1) are dynamic and evolving, inter-hybridizing with others in varying degrees. 42 Furthermore, the typology calls attention to the place of spiritual and religious perspectives, which have, historically speaking, played a central role in many ethnomedical paradigms. 43
The third domain, Knowledge Transmission Modes, characterizes the ways in which different forms of TCIM are contemporarily shared, taught, and/or disseminated. In particular, this domain draws attention to the degree of textual codification and knowledge standardization evident with respect to diverse TCIM approaches. It also delineates the extent to which oral, community-based modes of knowledge transmission (e.g., apprenticeship, family or community lineage) and/or institutional training modes may be at play. 44 Finally, this domain attends to questions of “expert”45,46,ii versus community-based knowledge and to their interface.
The fourth domain, Health Systems Contexts, refers to structural considerations that inform the ways in which health care is delivered and received around the world. The typology presented in the current article is implicitly informed by this domain, as reflected most strongly in two of the six TCIM types (Community-Based Care and Integrative Therapeutics). Furthermore, the TCIM construct itself is very much a product of health systems contexts around the world. The final two articles of this series 30 more fulsomely address the fourth domain’s importance in understanding, and applying, the typology.
An Operational Typology of TCIM
TCIM is a broad construct that includes a wide and diverse range of therapeutic systems, knowledges, practices, products, and devices, as well as the interface between them and with Biomedicine. The construct has evolved in relation to the emergence and dominance of Biomedicine, which necessarily also conditions the typology. Theoretically, the operational typology of TCIM presented in this work is informed by a detailed analysis of the WHO’s definitions of traditional and complementary medicine, and Indigenous traditional medicine, WHO indications as to how the concept of integrative medicine might be understood, and related critical social science scholarship. Underpinned by that analytic work, outlined in the section “Conceptual Domains,” and as illustrated in Figure 1, the typology introduces six primary TCIM types, as follows:
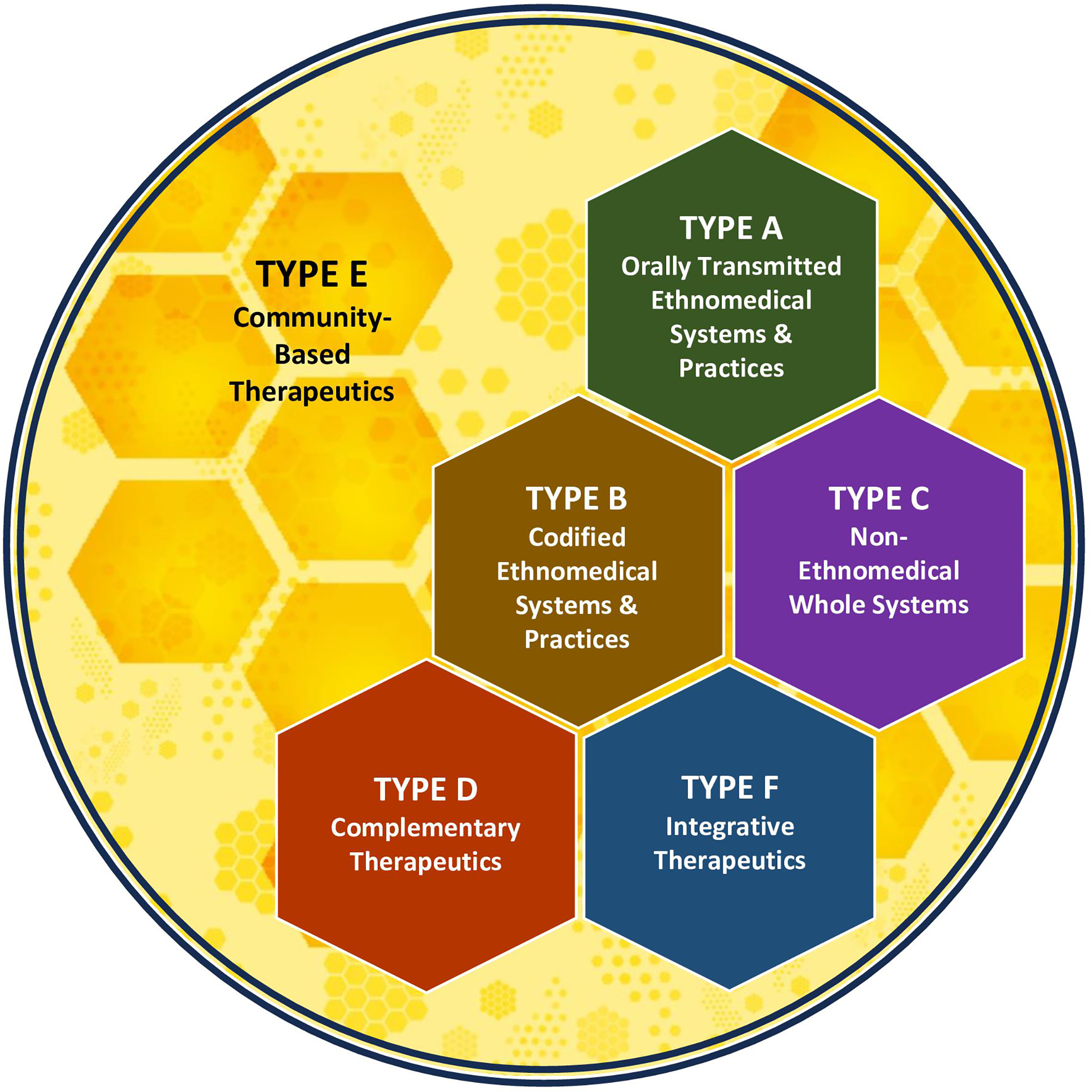
Operational typology of traditional, complementary, and integrative medicine. This figure provides a graphical overview of the six primary types in an operational typology of traditional, complementary, and integrative medicine.
Orally Transmitted Ethnomedical Systems and Practices;
Codified Ethnomedical Systems and Practices;
Non-Ethnomedical Whole Systems;
Complementary Therapeutics;
Community-Based Therapeutics; and
Integrative Therapeutics.
These six TCIM types (along with their respective subtypes) are elaborated in what follows and summarized in Table 2. With reference to the three conceptual domains outlined in the section “Conceptual Domains” of this article (Historical Factors, Paradigmatic and Cultural Features, and Knowledge Transmission Modes), Table 3 provides a detailed account of the conceptual features of each of the typology’s types and subtypes, which together provide a comprehensive framework for understanding, classifying, and analyzing the diverse therapeutic approaches that fall outside the boundaries of Biomedicine’s standard of care.
Overview of Types and Subtypes in an Operational Typology of Traditional, Complementary, and Integrative Medicine
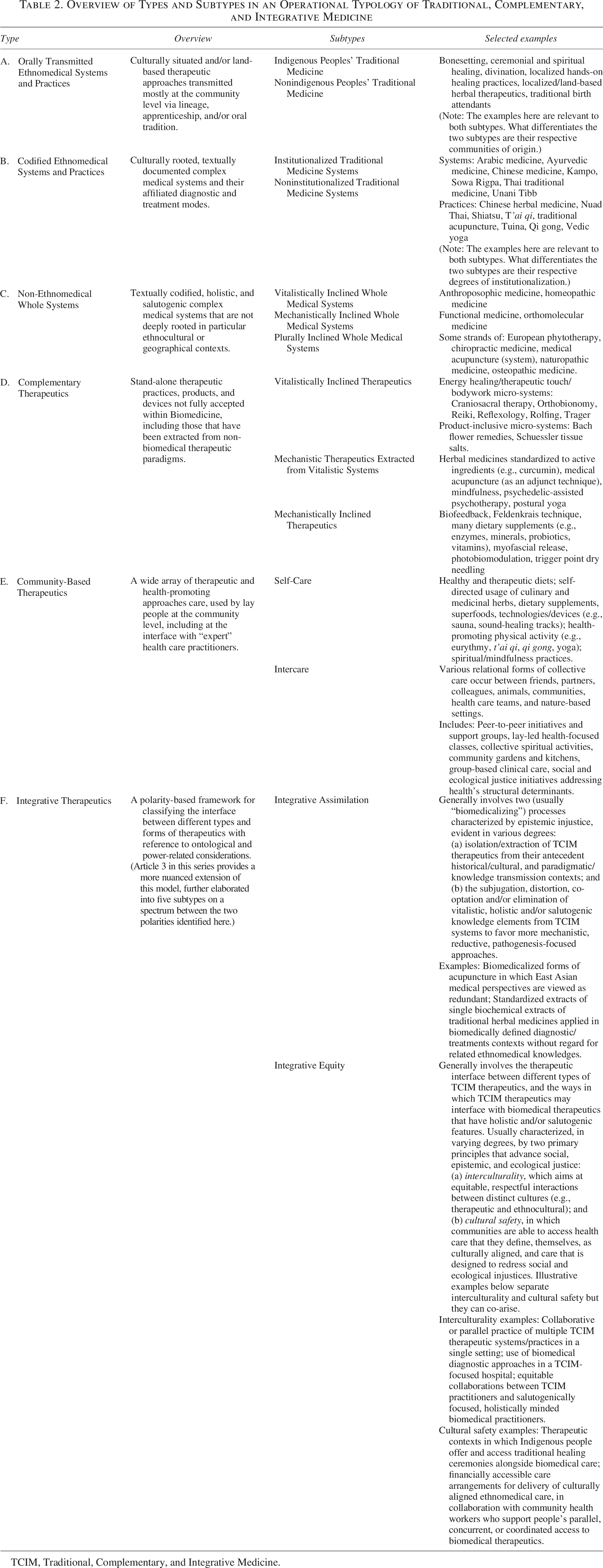
TCIM, Traditional, Complementary, and Integrative Medicine.
Conceptual Features of Types and Subtypes in an Operational Typology of Traditional, Complementary, and Integrative Medicine

Type A: Orally transmitted ethnomedical systems and practices
The first TCIM type includes a wide range of ethnomedical therapeutic knowledges and practices that are: (a) primarily transmitted at the community level through expertise constituted as oral tradition, family lineage, and/or apprenticeship (though some of their elements may be textually documented); (b) explicitly anchored to particular lands and communities in any world region (though they may have become displaced or exported); (c) characterized by a high degree of internal diversity (rather than standardization of knowledge and practice), whether at the level of family, village, community, or nation; and (d) in many cases, include an explicit focus on spirituality, wherein humans (along with other life forms) are understood as sacred elements within complex, interconnected ecological systems. Although either weak or strong therapeutic hybridizations with other knowledge forms may be evident, Type A therapeutics typically retain orally transmitted knowledges as their gravitational center.
Key examples of Type A therapeutic approaches may include highly localized approaches to herbal therapeutics, divination, ceremonial healing practices, and the work of traditional birth attendants. Some but not all Type A systems and practices may also align with Foster’s anthropological category of a “personalistic medical system…in which disease is explained as due to the active, purposeful intervention of an agent, who may be human…nonhuman (a ghost, an ancestor, an evil spirit), or supernatural (a deity or other very powerful being).” 47 However, as with all types, the determination of whether a therapeutic approach falls within Type A should be based on the type’s primary characteristics (rather than a provisional “list” of included healing approaches).
It is useful to differentiate two subtypes within Type A: Indigenous Peoples’ Traditional Medicine and Non-Indigenous Peoples’ Traditional Medicine.
Indigenous peoples’ traditional medicine
This subtype refers to Type A therapeutic approaches that have strong ties to Indigenous peoples, lands, and ways of life. The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) does not provide a singular definition of Indigeneity, based on the principle that Indigenous peoples’ self-determination and self-definition should be honored. 48 However, a widely cited working definition, offered by United Nations Special Rapporteur Martinez Cobo, is useful 49 :
Indigenous communities, peoples and nations are those which, having a historical continuity with pre-invasion and pre-colonial societies that developed on their territories, consider themselves distinct from other sectors of the societies now prevailing on those territories, or parts of them. They form at present non-dominant sectors of society and are determined to preserve, develop and transmit to future generations their ancestral territories, and their ethnic identity, as the basis of their continued existence as peoples, in accordance with their own cultural patterns, social institutions and legal system.
As Martinez Cobo further elaborates, Indigenous Peoples’ “historical continuity” is linked to their “occupation of ancestral lands. . . culture [and] language.” Furthermore, Indigenous Peoples across all global regions often have “[a]n experience of subjugation, marginalization, dispossession, exclusion or discrimination.” 48 Therapeutic approaches linked to Indigenous Peoples as described above may be characterized within the present subtype, whether they are constituted as complex medical systems, fragments thereof, or as standalone practices. This positioning is meant to recognize and honor the distinct knowledges that underpin these varied therapeutic approaches, as Indigenous communities work to revitalize their knowledges and practices and transform colonization’s extensive harms.
As noted in a 2023 United Nations study, “Indigenous Peoples tend to approach health as an equilibrium of spirituality, traditional medicine, biodiversity and the interconnectedness of all that exists…address[ing] the entire person within the context of past, present and unborn generations.” 50 Furthermore, as Redvers (an Indigenous global health scholar) indicates, “the health of the planet is intrinsically tied to the wellbeing of Indigenous Peoples. When Indigenous Peoples have their Land, culture, and sovereignty, they are more likely to have greater wellbeing.” 15 This fundamentally involves the preservation of Indigenous languages and Indigenous knowledges as part of a “holistic lens that acknowledges cultural and Land-based practices as being crucial for human health and for the health of the planet.” However, Indigenous Peoples around the world disproportionately experience health inequities that “originated during the colonization era…[and] have been perpetuated by neocolonial systems” of governance today. 50
Furthermore, a range of factors—European colonization foremost among them—have contributed to the erosion, denigration, and loss of living lineages of many Indigenous therapeutic knowledges and practices, which may later emerge in regenerated forms. Many such therapeutic approaches have been historically outlawed (and in some cases continue to be outlawed) across some parts of the world, interrupting their free and continuous transmission. 41 Today, many Indigenous communities continue the work of reclaiming, reconstructing, and revitalizing these approaches.51,52 Marshall et al.—Indigenous Elders and scholars with expertise in traditional knowledge systems—write, for example, of the need to “relearn to use the proper herbs, plants, and trees for our good health and well-being” as a means to “recover from the cultural starvation” of colonization’s impacts. 52
In terms of knowledge transmission, it further warrants note that while such therapeutics may sometimes be incorporated into national health systems in various forms, 53 it is not usually in a standardized or professionalized format. 52 Indigenous-led health care partnerships in such contexts often centralize the principle of “culture as cure.” 54 Furthermore, as Indigenous scholars repeatedly observe, the persistence of many forms of Indigenous Peoples’ Traditional Medicine as internally diverse, noninstitutionalized approaches that resist Eurocentric organizational modes is not accidental. Kovach, for example, writes, “Indigenous knowledges can never be standardized” 55 ; and Martin-Hill cautions against “transforming [traditional medicine] practice from cultures to institutions.” 51
Regulators contending with the interface between Indigenous Peoples’ Traditional Medicine and state health systems may refer to stipulations made within UNDRIP. 48 In particular, Section 11 affirms Indigenous Peoples’ “right to practise and revitalize their cultural traditions and customs,” which includes therapeutic knowledges and practices. Section 11 also affirms Indigenous Peoples’ right to state restitution “with respect to their cultural, intellectual, religious, and spiritual property taken without their free, prior and informed consent or in violation of their laws, traditions and customs.” The latter point is of particular relevance with respect to the widespread globalized extraction and misappropriation of Indigenous therapeutic practices and products, including traditional herbal medicines. Sections 24 and 31 of UNDRIP furthermore address Indigenous Peoples’ right to health, including the maintenance and preservation of traditional health care knowledges, practices, and resources as key elements of Indigenous peoples’ self-determination.
Non-Indigenous Peoples’ Traditional Medicine
Type A’s second subtype refers to orally transmitted ethnomedical systems and practices that are not specifically affiliated with Indigenous peoples. Some such therapeutic approaches may once have been forms of Indigenous Peoples’ Traditional Medicine but, having become historically displaced from their lands of origin (at times through violent means), are now practiced in other regions. One key example here would be the diverse (and variously hybridized) systems and practices of Afro-descendent traditional medicine that have persisted and inter-hybridized across the Americas region following African peoples’ forced enslavement there. 56 Other examples include a wide range of highly localized, orally transmitted ethnomedical approaches in practice across all world regions but especially across the global South that are sometimes termed “folk” medicine by anthropologists. iii Such therapeutics are largely practiced by trusted, community-defined expert practitioners (e.g., herbalists, hands-on healing practitioners, birth workers, spiritual healers, and others). As in the Indigenous Peoples’ Traditional Medicine subtype, the question of expertise here, and the determinations of what knowledges and practices are constituted as valid and who may legitimately transmit and enact such, are determined within noninstitutional, community, and cultural contexts. 57
Type B: Codified Ethnomedical Systems and Practices
Type B refers to a wide range of complex ethnomedical systems (along with their associated therapeutic elements) that are characterized by a high degree of textual codification. This codification might take the form of: (a) associated historical texts that continue to inform contemporary practice; and/or (b) more contemporary textual documentation of a system and its affiliated practices, informed by historical fragments and/or culturally situated elements. Globally speaking, codified ethnomedical systems and practices may be employed within their cultures and/or geographies of origin, as well as in diasporic contexts. Ecocentric, vitalistic ethnomedical sciences remain the dominant paradigmatic frameworks within which this category’s therapeutics are employed. The ecocentricity of such systems is evident, for example, in conceptual models that conceptualize health and its balances in relation to fire, earth, water, and other elements from the natural world. Today, many such systems may be characterized by weak hybridization with mechanistic knowledges (e.g., the inclusion of biomedical scientific elements in training curricula). There may also be evidence of strong or weak inter-hybridization between multiple ethnomedical knowledges (as the example of Arabic medicine, detailed further on, shows). However, only those hybridizations that retain codified ethnomedical knowledges at their gravitational center are to be classified within Type B.
Key examples include such ethnomedical systems as Chinese medicine, Ayurveda, Unani Tibb, Kampo, Persian Medicine, Korean medicine, Sowa Rigpa, traditional Arabic and Islamic medicine, Thai traditional medicine, and forms of traditional European herbal medicine that have strongly retained ethnomedical paradigmatic elements, such as elemental constitutional diagnosis. 58 Critically, Type B includes ethnomedical systems’ associated knowledges, vitalistic diagnostic approaches, and treatment frameworks, as well as their affiliated therapeutic practices, tools, and products. For example, “traditional” acupuncture practiced from within an East Asian ethnomedical framework would be included in this type, whether practiced alone or in combination with other therapeutic elements from that ethnomedical system (e.g., moxibustion and herbal medicine). Many Type B systems furthermore overlap at least partly within Foster’s anthropological category of a “naturalistic” medical system, in which illness is explained “in impersonal systemic terms,” resulting “from such natural forces or conditions as cold, heat, winds, dampness, and, above all, by an upset in the balance of the basic body elements…[or] humors.” 47
As in Type A, ethnomedical systems and practices with a strong historical basis are neither internally singular nor unequivocally “ancient.” Further, while many such systems and practices may have historically included spiritual or religious epistemic elements (e.g., Chinese medicine and Taoism, Ayurveda and Hinduism), such elements may have become minimized in contemporary variants. Conversely, other systems—such as traditional Arabic and Islamic medicine—continue to retain explicitly religious elements. 59 The latter case also shows how multiple ethnomedical systems may inter-hybridize into new systems. Indeed, Arabic medicine represents an “amalgam of indigenous medical knowledge” with “Islamic medical and Prophetic influences, as well as regional healing practices emerging from specific geographic and cultural origins,” including from Ayurvedic, Chinese, Persian, and Unani medicine.
Type B may be broadly categorized into two primary subtypes: (a) Institutionalized Traditional Medicine Systems and Practices and (b) Non-Institutionalized Traditional Medicine Systems and Practices.
Institutionalized Traditional Medicine Systems and Practices
Over the last century, a particular, strongly institutionalized configuration of codified ethnomedical systems has emerged that Hardiman and Mukharji refer to as “syndicated traditions.” 42 In such institutionally sanctioned “syndications,” long-standing ethnomedical traditions and their affiliated practices have some of their paradigmatic and technical elements selectively standardized, at times recodified, transmitted through formal educational institutions, professionalized, and in several jurisdictions governed via statutory regulation.
In particular, in East and South Asia, such ethnomedical institutionalization trajectories have unfolded at least partly as a political means to bolster national identity. This is the case, for example, for traditional Chinese medicine, Ayurveda, and Unani Tibb, for each of which the WHO has also articulated institutional “training benchmarks.”60,61 In each case, these systems’ politicized “syndications” emerged at least partly in response to broader conditions of European colonization and biomedical dominance. Relatedly, they have gained political capital as a result of a strategic engagement with historically European modes of health professionalization (e.g., educational standardization, statutory regulation) and the adoption of biomedical scientific elements (e.g., curricular components, evidentiary modes) as key elements.62–64 In some cases, as in post-Soviet Uzbekistan, “syndicated” ethnomedical systems may also be built around “a body of local traditions that draw their substance from long-forgotten beliefs,” which become reconstituted as a new “invented tradition.” 65
The institutionalization of ethnomedical systems has several important ramifications. Their standardized forms may lend these systems heightened paradigmatic alignment 29 with biomedical research approaches (like randomized controlled trials), which typically emphasize investigations of standardized therapeutics. Research conducted in adherence to such biomedical norms may, in turn, act as a kind of politial capital that may support uptake of institutionalized ethnomedical therapeutics within dominant health systems. 66 Their adherence to dominant professionalization norms can also support trajectories leading to these systems’ uptake within “public medical systems,” where they may be “considered legitimate reimbursable services by insurers.” 67 However, as Fruehauf—a scholar of East Asian medicine—has argued, 68 the transformation of ethnomedical knowledges and practices into institutionalized forms may also profoundly alter their paradigmatic character, extracting “the traditional art…out of the hands of its lineage holders and assigning it to the control of modern science.” In other words, such institutionalizations may be viewed as therapeutic hybridizations that risk, over time, shifting the gravitational centers of ethnomedical systems from more vitalistic to more mechanistic ontologies. As Janes, a medical anthropologist, asserts, “alternative systems may become so much like biomedicine, so rationalized and ‘sanitized’ of their alternative epistemological tenets that they may not be able to meet the human and social needs of the rapidly approaching health crises” within which they might otherwise have the capacity to fruitfully intervene. 67
Non-Institutionalized Traditional Medicine Systems and Practices
As the medical anthropologist Lambert has observed, the “selective processes of legitimation…whereby particular traditions of [I]ndigenous medicine undergo reformulation into professionalized and accredited knowledge systems” produce “hierarchies of legitimacy” that marginalize ethnomedical practitioner communities who “practice without official [state] sanction.” 62 Although less institutionalized variants of codified ethnomedical systems—including those that have “syndicated” iterations—continue to be practiced across many countries and regions, this typically occurs without state backing and with lesser sociopolitical standing than their “syndicated” counterparts. This subtype characterizes such noninstitutionalized ethnomedical therapeutic approaches. These are often characterized by a combination of codified and orally transmitted knowledges, and institutional as well as more community-based training modes (including apprenticeship and family lineage). Two brief examples, with reference to Chinese medicine and Ayurveda, illustrate the complex and marginalized positionalities of such therapeutics.
As Taylor (a medical historian) and other social scientists have documented, the institutionalized (“syndicated”) system known as Traditional Chinese Medicine (TCM) took shape in 1950, in China, under Mao Zedong’s regime.64,68,69 At the time, following state licensure examinations that many people failed, “[t]he large majority of Chinese medical practitioners…[were] banned from practice…[and] unable to practice Chinese medicine legally.” 64 Fruehauf recounts, from that time 68 : “TCM departments were established in many city hospitals…[but] the doctors in charge were ‘Western doctors with Chinese knowledge’,” which had the effect of further infusing the emerging TCM system with biomedical paradigmatic elements. Over time, TCM’s institutionalization and its subsequent globalization have had the persistent effect of marginalizing many “classical” and Taoist (rather than Maoist) variants of Chinese ethnomedical knowledge and practice. Critically, however, all these approaches share a common textual basis as well as links to orally transmitted, local, and regional lineages.
Another example, from India, makes visible how legislative regimes that lift up ethnomedical syndication strategies based on Eurocentric professionalization norms may marginalize non-institutionalized therapeutic lineages. There, non-professionalized “bone doctors,” whose work has “historical and epistemological links with Ayurveda,” treat “a wide range of complaints…[but primarily] sprains, fractures, injuries to limbs, or musculo-skeletal pain.” 62 These practitioners’ knowledges of medicinal plant preparations, as well as physical manipulative techniques, are transmitted via familial lineage as well as textually. But bone doctors do not share institutionalized Ayurvedic medicine’s state backing in India. 62 Although Indian state governments had initially valorized “experience-based registration” of bone doctors and other ethnomedical practitioners in the 1940s and 1950s as part of early efforts to “regulate indigenous medical forms,” these statutory pathways were subsequently phased out. Although today “[b]one doctors have expertise in the eyes of the patients they treat…they are not authorized to provide care, since the modern State takes formal qualifications to be the sole criterion for recognition of expert status.”
Type C: Non-Ethnomedical Whole Systems
The typology’s third type encompasses textually codified, complex medical systems that are neither predominantly ethnomedical nor well-accepted within Biomedicine.70,iv On the whole, these systems are underpinned by therapeutic paradigms that centralize holism and salutogenesis, either—in a first subtype—with a more vitalistic ontological inclination, or—in a second subtype—with reference to a mechanistic gravitational center. Like Type B systems, Type C systems are often internally diverse (with subcommunities of knowledge and practice within them) and may be institutionalized and standardized in varying degrees. Type C systems also have their own distinct conceptual and diagnostic models, as well as therapeutic modes, sometimes produced via hybridizations with other ethnomedical, non-ethnomedical, and biomedical systems. However, what distinguishes Type C systems from Type B is that their paradigmatic gravitational centers are not predominantly ethnomedical. In varying degrees, Type C systems remain sociopolitically marginalized in relation to Biomedicine. This may be due to a range of historical, economic, epistemic, political, and sociocultural factors, but not predominantly because of European colonialism, as in Type B. Type C’s two subtypes are elaborated below.
Vitalistically Inclined Whole Medical Systems
This subtype involves complex medical systems that take as their gravitational center an ontological heterarchy (Table 1) characterized by vitalism, along with holism and salutogenesis, as well as other system-specific paradigmatic elements. Ecocentricity may be implicit or explicit in varying degrees within such systems. Salient examples of such systems include homeopathic medicine and anthroposophic medicine, as well as vitalistically oriented strands within European phytotherapy, naturopathic medicine, chiropractic medicine, and osteopathic medicine.
Homeopathic medicine, a system conceptually based on “the principle of ‘like curing like’,” 70 is one example of a vitalistically inclined, holistic, salutogenic system. Classical (Hahnemannian) homeopathy originated in late 18th-century Germany 71 and has been notably globalized across many nations, for example,72,73 with many variants worldwide today. On the whole, homeopathic medicine’s vitalistic inclinations are evident both in its diagnostic and therapeutic modes, which contrast strongly with the tenets of scientific materialism. Indeed, its diagnostic model centers “the concept of an individualized ‘constitutional’ prescription,” which considers physical, emotional, and temperamental traits, and its therapeutic modes rely on “the use of remedies prepared by ‘infinitesimally’ diluting particular substances.” 70
Anthroposophic medicine is another system that exemplifies this subtype’s complex potential characteristics, fusing ethnomedical, non-ethnomedical, and biomedical elements into a vitalistic, holistic, salutogenic whole. Anthroposophy’s conceptual model draws on elements from Greco–Roman ethnomedicine (e.g., its four-element cosmology) 74 and includes other vitalistic constructs (e.g., four “formative forces,” and a threefold structural/functional model of the human organism). 74 The system concurrently incorporates biomedical diagnostic and treatment approaches, ethnomedical European herbal medicines, and non-ethnomedical therapeutic approaches such as eurythmy therapeutic movement and homeopathically informed remedies.
Mechanistically Inclined Whole Medical Systems
Type C’s second subtype characterizes complex medical systems with a mechanistic gravitational center informed by holistic, salutogenic principles and other system-specific paradigmatic elements. Key exemplars include functional medicine and orthomolecular medicine.
In some cases, systems in this subtype have their origins in mechanistic ontologies. Functional medicine (a mechanistic, holistic, salutogenic system) is a key exemplar, characterized by a “paradigm shift from the body-as-machine model to a systems biology approach.…This involves exploring patients’ biochemical individuality[,]…may incorporate [diagnostic] tools such as gut microbiome testing and genomic testing,” and offers “lifestyle medicine prescriptions” and other non-pharmacological therapeutic approaches to restore health. 75
As the case of chiropractic medicine shows, some therapeutic systems that have historical roots in a vitalistically inclined ontology may, over time, have shifted their paradigmatic gravitational centers toward mechanism. Over the last 50 years, the “vertebral subluxation theory”—a vitalistic construct at the heart of early chiropractic medicine, but one that is difficult to reconcile with mechanistic/biomedical explanatory models—has been increasingly de-emphasized (and even disavowed) across much of the chiropractic field.76–78 As the next subtype further illustrates, such biomedicalizing paradigmatic shifts have also been documented as taking place as part of the professionalization trajectories of several other non-biomedical therapeutic occupations (e.g., osteopathy, naturopathy, midwifery), as a means to advance their sociopolitical and economic standing.77–82
Plurally Inclined Whole Medical Systems
There are several examples of complex medical systems that may straddle the previous two subtypes, at once illustrating the internal diversity of many therapeutic systems, the dynamism and hybridity of therapeutics, and the permeability of this typology’s categories. Such systems—which include subcommunities of practice with distinct (and sometimes conflicting) ontological inclinations—include European phytotherapy (sometimes termed “Western herbal medicine”), naturopathic medicine, osteopathic medicine, and chiropractic medicine. As Nissen, a medical anthropologist, has shown in a case study of Western herbal medicine practitioners in the United Kingdom, their occupation unites around the principle of holism. 83 But subcommunities within that occupation diverge as to their alignment with vitalistic perspectives, with some relying instead on more biomedical (mechanistic) diagnostic constructs and a biopsychosocial approach in their use of herbal medicines.
A similar phenomenon has been documented within naturopathic medicine, a therapeutic system historically underpinned by an ecocentric, vitalistic principle termed the Vis Medicatrix Naturae (“nature’s healing power”). Casting “the Vis” as a metaphor, Coulter and colleagues argue that it is simply the interpretation of this fundamental vitalistic principle that varies across the contemporary naturopathic occupation. 22 However, as Ijaz et al. have shown with reference to the Canadian context, there remains a substantial subcommunity of naturopathic practitioners “who adhere more strictly to biomedical epistemology and bioscientific evidentiary constructs in their clinical activities.” 79 Like Nissen’s herbalists, these naturopaths appear to “reject…notions of vitalism,” 83 despite an overarching commitment to holism and salutogenesis within their work. 79
The case of naturopaths illustrates another important feature of this subtype: the existence of “syndicated” and “non-syndicated” subcommunities within a single therapeutic system. In the United States, for example, an institutionalized naturopathic medicine profession is built upon a standardized 4-year curriculum offered at several formally accredited institutions across the country and has achieved licensure in 26 of the country’s states and territories. 79 However, so-called traditional naturopaths (who share many paradigmatic elements with professionalized naturopathic doctors) train within less institutionalized contexts and continue to practice in many U.S. jurisdictions 84 without explicit state sanction or the socioeconomic capital that institutionalization entails.
Type D: Complementary Therapeutics
The therapeutic approaches included in Type D have three defining characteristics: (a) they are therapeutic micro-systems (Table 1), practices, products, or devices that “stand alone,” that is, they do not, in themselves, comprise complex medical systems (although they may have historical origins or antecedents in such systems); (b) they are not fully accepted within Biomedicine’s standard of care (in a particular context, which may vary from place to place); and, finally, (c) they are often practiced as a “complement” or adjunct to another defined complex medical system, biomedical or otherwise.85–87,v It is useful to categorize Type D into three subtypes, which reference their predominant ontological inclinations.
Vitalistically Inclined Therapeutics
Type D’s first subtype refers to a wide range of stand-alone therapeutics that have historically emerged and continue to be practiced with reference to vitalistic perspectives. This includes such energy medicine approaches as Reiki; vitalistic therapeutic touch techniques like foot reflexology, the Trager Method, and Craniosacral or Structural Integration (Rolfing) therapies; and product-inclusive approaches like Bach flower remedies and Schuessler tissue salts. Such approaches, notably, may comprise a therapeutic micro-system with its own internal logics, diagnostic, and treatment approaches. But, the therapeutic scope and range of such micro-systems are considerably more limited than “whole” complex medical systems as characterized by Luz, 12 which typically include knowledge frameworks and tools that address a more comprehensive range of health-related considerations. At times, approaches within this subtype may be applied in the form of “this-for-that” or “cookbook-style” therapeutics, in which a particular remedy is “matched” to one or more (vitalistically constituted) symptoms without the fulsome diagnostic assessment that would take place within the context of a Type A, B, or C vitalistic system.
Mechanistic Therapeutics Extracted from Vitalistic Systems
This subtype refers to therapeutic approaches that have origins in a vitalistic Type A, B, or C system, but have been “extracted” and isolated from their vitalistic paradigms to be used with reference to a more mechanistic perspective. Key examples include some forms of biomedical acupuncture; extracts of traditional herbal medicines standardized to optimize a particular “active ingredient” (e.g., curcumin, derived from turmeric); homeopathic remedies used for biomedically constituted diagnoses without reference to a homeopathic diagnostic process; “secular” mindfulness (originating in Buddhist meditative traditions); “secular” postural yoga; and various psychoactive therapeutics practiced outside of their originating Indigenous ceremonial and/or ethnomedical contexts (e.g., psilocybin-assisted psychotherapy).
The mechanistic refashioning of once-vitalistic therapeutics has certain recognizable hallmarks. For example, ethnomedical herbal preparations often undergo (at least some part of) a threefold process involving “constituent isolation, compound standardization, and constituent synthesis” 88 as they are reformulated to “suit the biomedical paradigm.” “Biopiracy” (so termed by the physicist-ecologist Vandana Shiva), involving the nonconsensual extraction and commercialization of Indigenous plants,89,vi Complex sociopolitical and ethical issues, including cultural misappropriation, commodification, intellectual property rights, and social and ecological injustice, are key considerations relevant to this subtype, especially with respect to therapeutic approaches extracted from ethnomedical systems. 90
Mechanistically Inclined Therapeutics
Therapeutics within this final subtype have primarily originated within, and are currently practiced with reference to, a mechanistic therapeutic ontology. vii Included approaches, which are often also inclined toward holism and salutogenesis, include some art and music therapies; some body-based therapies (e.g., the Alexander Technique, Feldenkrais, Myofascial Release); a range of nutritional supplements and their combinations that are being used in ways not currently accepted as biomedical standard practice (e.g., some vitamin, mineral, enzyme, and probiotic products); pharmaceutical drugs that are used “off label” in ways that diverge from conventional biomedical practice standards; and various therapeutic approaches that rely on medical devices (e.g., biofeedback, photobiomodulation, and “others”).
Notably, while some such therapeutics (e.g., vitamin supplements) are widely characterized as “natural” or “alternative” compared with pharmaceutical drugs—and they may be food-derived or food-inspired—they carry the conceptual hallmarks of mechanistic biomedical science, which emphasizes isolation and synthetic production of so-called active ingredients. 88 In some cases, therapeutic approaches in this category may also represent therapeutic hybrids that include influences from ethnomedical (or other vitalistic) therapeutic systems. Trigger point dry needling, for example, involves the therapeutic insertion of acupuncture needles (originating in East Asian medicine), but originated in the work of biomedical physician Janet Travell, who initially used hypodermic needles to inject anesthetic and saline solutions into painful bodily sites from a mechanistic standpoint.91–93
Type E: Community-Based Therapeutics
The next type to be characterized in this work, Community-Based Therapeutics, is qualitatively different from Types A through D, which emphasize externally validated (and sometimes monopolistic) forms of expertise. Indeed, all therapeutic approaches, whether institutionalized or community-based, rely on culturally determined forms of validation and expertise. Here, in Type E, one finds TCIM therapeutics practiced across community settings, typically by and for “lay” people (and validated with reference to local cultural conventions of knowledge transmission), though also in coordination with organizationally or institutionally sanctioned health care practitioners. Depicted as the “background zone” within the typology’s graphical representation, Type E may thus be understood as a space that encompasses but extends beyond the other types, a zone of interface between the other types, and ultimately as an overarching backdrop within which the other types are housed. On the whole, this type represents a sphere of health democratization, illustrating lay peoples’ autonomous capacity to engage, with and/or without “expert” inputs, the therapeutic knowledges and practices that address their needs and preferences. People may engage in community-based therapeutics for various reasons, whether salutogenic/preventive, to treat active ailments, to palliate discomfort, and/or to build healthy relationships and communities. Ultimately, this TCIM type may be understood as a space advancing what the WHO has termed “well-being societies,” in which a “whole-of-government” and “whole-of-society” approach intersect to promote
a positive vision of health that integrates physical, mental, psychological, emotional, spiritual and social well-being; the principles of human rights, social and environmental justice, solidarity, gender, inter-generational equity, and peace; new indicators of success, beyond gross domestic product, that take account of individual and societal well-being…[and] the focus of health promotion on empowerment, inclusivity, equity and meaningful participation. 94
Type E, Community-Based Therapeutics, is constituted here within two subtypes: Self-Care and Intercare.
Self-Care
The WHO has characterized self-care as “the ability of individuals, families and communities to promote health, prevent disease, maintain health and to cope with illness and disability with or without the support of a health worker.” 95 As “the primary health resource in the health system,” self-care is an essential element of the human right to health, encompassing health’s “personal determinants…situational, economic, emotional and social determinants…[and] health systems determinants.” It has been shown, at least in some jurisdictions, that “CAM [complementary and alternative medicine] self-care constitutes the bulk of self-care…and represents the single largest area of modern CAM consumption.” 96
This subtype refers to forms of remedial or salutogenic self-care practices at the level of the individual. This includes such over-the-counter TCIM therapeutics as self-administered herbal remedies, which may have cultural as well as therapeutic significance. Other examples address what the WHO calls health’s “personal determinants” (e.g., the actions that individuals take in caring for themselves, based on their own knowledge and health literacy). 95 These may include healthy dietary patterns (including traditional and Indigenous dietary practices, the avoidance of industrially processed foods, and therapeutic diets that fall outside the standard of biomedical dietetic care); the consumption of nutrient-dense “super”-foods (e.g., bee pollen, spirulina, nutritional yeast); the preventive and therapeutic use of culinary spices and medicinal herbs (e.g., in cooking or as teas); the use of dietary supplements (e.g., vitamins, minerals, probiotics, digestive enzymes, and essential fatty acid products); health-promoting physical activity (including such approaches as yoga, t’ai chi, qigong, dance, or eurythmy); spiritual and mindfulness-focused practices (such as prayer and meditation); and engagement with health-promoting technologies or devices (e.g., sauna, mindfulness “apps,” sound-healing musical tracks). At times, individual self-care activities may include an associated financial transaction (e.g., participation in a paid t’ai chi class); and although these may take place in group settings, they may still be conceptualized as self-care at the level of the individual. However, as the next subtype—intercare—illustrates, self-care always takes place within a larger socioecological context.
As social scientists have observed, predominant self-care narratives in global North countries tend to emphasize the well-being of the individual rather than the collective or the planet. 97 This emphasis may reproduce Eurocentric tenets of individualism, at odds with “the cultural focus on collectivism” 97 that underpins many Indigenous and global South cultures, as well as communities of color across the North.98,99 Further, “individualizing” self-care narratives have at times been critiqued as potentially “reproducing neoliberal moralities of health and illness” 100 that inappropriately “blame” individuals for poor health outcomes that should be attributed to health’s social and structural determinants.100,101 Moreover, some self-care narratives, in particular those that call for use of costly commercial products (e.g., dietary supplements) or services (e.g., expensive yoga classes), can reproduce patterns of sociopolitical marginalization, in which the “poor and most vulnerable” 96 are less likely to have access.96,102 The dire ecological impacts associated with “overexploitation” of medicinal plants popularized on the open marketplace represent another critical consideration in the self-care domain. 103 The inclusion of the next subtype—intercare—aims in part to redress such problems.
Intercare
The concept of “intercare,” elaborated in a 2019 report by the Pan American Health Organization, recognizes that the health-related concept of “care…refers not only to self-care, because people to do not care for themselves entirely on their own.” 104 Rather, “[h]ealth is the product of intercare that people provide to each other every day, while creating the conditions for a dignified life.” As that report elaborates, “[u]nlike the self-care approach, [intercare] values the relational and collective perspective,” explicitly recognizing “the support networks that are not yet considered part of health systems, but without which no health system can function.” Intercare, thus, is a synergistic, ecological principle, at once incorporating the role of self-care at the individual level as well as treatment offered by health care practitioners. Intercare also makes visible the complex, symbiotic, and reciprocal relations of care that exist among people and other living beings, and with place: between and within friendships and intimate partnerships, families, communities, health care teams, and health care institutions, with plants and nonhuman animals, and within broader ecosystems.
On any scale, Intercare includes certain features akin to what has elsewhere been termed “collective care”105,106 or “mutual aid.” 107 As Downe, a medical anthropologist, explains, “collective care represents an ethos of social interconnectedness…It is a cultural touchstone” in many communities, not only in families where people share “biological connections but [also in] the ties among those who share…histories, and a similar ethic of care.” 106 Therapeutically speaking, Intercare thus includes the many informal ways in which families and friends may mutually support one another in their health-related self-care. It also encompasses the wide range of “peer-to-peer” initiatives, lay-led educational classes (e.g., yoga, t’ai chi, mindfulness, nutrition), and health-focused support groups that emphasize non-biomedical therapeutics; community kitchens, community gardens, and farmers’ markets (including those emphasizing traditional and Indigenous foodways); nature-based and animal-engaged therapeutic encounters; and a range of communal spiritual activities. Intercare further extends to institutional health care settings in which the patient–provider relationship plays an integral role in the healing process, and to group-based clinical initiatives.
Finally, as Spade (a legal studies scholar) argues, mutual aid as a form of collective care also includes a wide range of social and ecological justice initiatives that address health’s structural and planetary determinants through “(a) work to dismantle existing harmful systems and/or beat back their expansion, (b) work to directly provide for people targeted by such systems and institutions, and (c) work to build an alternative infrastructure through which people can get their needs met.” 107 Intercare of all the aforementioned kinds is not only a survival imperative for many but can play an important therapeutic role within communities that, for a range of historical reasons, may have come to distrust mainstream health care institutions and that suffer collective traumas arising from epistemic, social and ecological injustices. As Page and Woodland, a community organizer and psychotherapist, respectively, together affirm, 106 “[c]ollective trauma is transformed collectively…just as harm is collective, healing is not an individual act.…Our collective histories are filled with practices and traditions used to heal our people and ensure our survival.” Ultimately, Intercare represents the space of the therapeutic commons, where health-related knowledges and healing practices dwell in social, ecological, and epistemic justice as a shared, communal resource.
Ultimately, Intercare represents the most comprehensive category within this TCIM typology, subsuming and encompassing the many and diverse ways in which all other types and subtypes interrelate within a larger socioecological fabric. In this sense, Intercare may be understood to draw attention to the health systems contexts of TCIM therapeutics, which as readers will recall, is one of the four conceptual domains around which this typology is built. The specifics and implications of that fourth domain, both with respect to Intercare and the typology’s other types, will be addressed in the final article in this series.
Type F: Integrative Therapeutics
Like Type E, Type F is conceptually different from Types A through D. Somewhat akin to Type E’s second subtype (Intercare), Integrative Therapeutics108,109,viii is a relational category, pointing to the interface between forms of health care. However, where the emphasis of Intercare is on the reciprocal relations of care that are evident within communities, Integrative Therapeutics is a type whose purpose is to characterize the ways in which multiple therapeutic knowledges and practices may intersect or interface—that is, integrate—with one another across health care ecosystems. This kind of integration is often conceptualized as the combination of TCIM therapeutics with conventional biomedical care, and such integration indeed represents an important sociocultural trend globally. However, in this typology, which aims at comprehensiveness, the interface between multiple forms of TCIM, with or without Biomedicine, is also encompassed in Type F.
Like all other types in this typology, as shown in Table 3, Type F accounts for the paradigmatic, cultural, and knowledge transmission features of different integrative scenarios. As elaborated in the first article in this series, the power relations expressed in integrative therapeutic contexts ix (sometimes called “integrative medicine”) may be conceptualized in relation to two polarities. These two integrative polarities—first, assimilation and second, equity,—form the basis of Type F’s two subtypes.
Integrative Assimilation
As part of the previous article’s analysis of WHO indications as to the meaning of integrative medicine, two primary interpretive possibilities were identified. In the first—the focus of this subtype—integration is constituted as a “biomedicalizing process, that is, a unidirectional assimilative process of incorporating non-biomedical practices (separated from their concomitant knowledges) into existing biomedically-dominant health systems.” The dynamics of such Integrative Assimilation have been repeatedly described by social scientists as characterizing the encounter between TCIM and biomedical therapeutics.90,110–113
Shuval et al., for example, report that TCIM practitioners working in Israeli hospitals experienced a “dual process of simultaneous acceptance and marginalization” in which “their marginality was made clear by a variety of visible structural, symbolic and geographical cues.” 114 In a study of two Canadian integrative health care settings, Hollenberg describes multiple ways in which biomedical physicians exerted “professional dominance” over TCIM practitioners, even as the latter “resisted” such. 110 In another sociological study of the integration of Indigenous traditional medicine practitioners within a Bolivian biomedical health center, several related problems were reported. 115 For example, the program “claimed to be culturally sensitive [but] overlooked important [I]ndigenous beliefs”; there was a “lack of professional recognition of T[raditional] H[ealers], who did not receive monetary payment for their services”; and “relationships between THs and biomedical staff [were]…hindered by the presence of preconceived ideas about the alleged ‘superiority’ of the biomedical system.” 115
Integrative Assimilation would be most commonly evident in contexts wherein one or more TCIM approaches interface with forms of Biomedicine characterized concurrently by mechanistic, reductionist, and pathogenic ontologies. As elaborated in the first article in this series, those three ontologies seem to have a low capacity to “tolerat[e] alternative paradigms.” While Integrative Assimilation may take a wide range of different forms, its “mechanics” would be characterized by two primary processes: (a) the isolation and extraction (in varying degrees) of TCIM therapeutics from their broader historical, paradigmatic, cultural, and knowledge transmission contexts; and (b) the distortion, co-optation, subjugation, or elimination of TCIM knowledge perspectives with reference to Biomedicine’s mechanism, reductionism, and pathogenesis. Put another way, Integrative Assimilation represents a range of forms of epistemic injustice.
It is also possible that one form of TCIM might exert Integrative Assimilation over another TCIM approach in some contexts. This might be especially evident in contexts in which a more mechanistically inclined, professionalized, and/or institutionally sanctioned TCIM approach interfaces with more vitalistically inclined, less professionalized, and/or institutionally sanctioned TCIM therapeutics.
Hollenberg and Muzzin, critical social scientists, have notably advanced two concepts—paradigm appropriation and paradigm assimilation—to characterize integrative therapeutic contexts or processes that may fall broadly under this subtype. Although paradigm appropriation and paradigm assimilation differ by a matter of degree, they follow the same overarching principle of reinforcing biomedical dominance and devaluing non-biomedical knowledges. These phenomena may take place inadvertently, as long-term sequelae of the historical institutionalization of colonial worldviews—even when actors involved in institutions today do not sanction colonial values.
In paradigm appropriation, “biomedicine appropriates certain aspects from other healing systems or traditions without fully acknowledging the paradigmatic worldview from which the particular treatment aspect was taken.” 90 One example might involve the therapeutic application of a traditional herbal medicine “product” (e.g., turmeric) for joint pain without consideration of the traditional medicine paradigms from which related knowledge may derive. 116 x Turning to a TCIM “practice,” clinical settings that include the clinical application of forms of acupuncture in which East Asian medical principles are viewed as “redundant or not necessary for the practice of acupuncture itself” might represent another example. Finally, illustrating the phenomenon with reference to “practitioners,” this phenomenon would be evident in some cases involving traditional midwives. In such cases, midwives who initially learned to attend home births in ethnomedical contexts—where they engaged in culturally specified approaches (such as song, prayer, specific herbal preparations) and used ethnomedical conceptual frameworks to explain their work—become “grandparented” into a licensed midwifery profession predicated primarily on biomedical knowledges. That profession, historically, would have emerged on the basis of traditional ethnomedical knowledges. But, its contemporary practitioners (who might continue to attend home births and offer family centered care) might now be expected to work (and explain their work) primarily from a biomedical standpoint, abandoning those elements of practice that are more explicitly non-biomedical.
Paradigm assimilation goes further than paradigm appropriation, with Biomedicine “not only appropriat[ing] or tak[ing] over another entire healing paradigm or system but reinterpret[ing] it,” a process through which “theoretical attributes and characteristics of the appropriated paradigm are then eliminated.” This phenomenon may be perceived in the therapeutic application of a standardized extract of curcumin (a biochemical constituent biomedically characterized as turmeric’s “active ingredient” but removed from the traditional whole plant application) for a specific biomedical diagnosis (e.g., rheumatoid arthritis). In fact, as biomedical scientific evidence has now reaffirmed, traditional culinary combinations of turmeric root with black pepper potentiate its therapeutic action. 117 Further, the curcumin contained within turmeric is known to be a fat-soluble compound, lending additional support to traditional culinary practices in which turmeric is used not only with other spices but also with cooking oils. 118
As Hollenberg and Muzzin further explain, paradigm assimilation might also be exemplified with reference to the practice of acupuncture. Understood in East Asian medical systems as “stimulating the flow of Qi along the body’s meridians to resolve Qi obstruction and to promote healing,” acupuncture might become entirely reframed, via paradigm assimilation, as “the stimulation of cells to release pain-relieving endorphins.” Finally, the same kinds of traditional birth workers described in the preceding section might come to work as nurse-midwives—members of a profession strictly framed in biomedical terms whose care is primarily delivered in hospital settings.
Integrative Equity
The second subtype in Type F refers to a wide range of therapeutic interactions among multiple TCIM therapeutics, and also between TCIM therapeutics and a range of forms of Biomedicine that have some salutogenic and/or holistic ontological features. This subtype, in notable contrast to Integrative Assimilation, is thematically encapsulated by the construct of Integrative Equity, which brings together two principles: interculturality and cultural safety. Overall, integrative therapeutic models that tend toward Integrative Equity may be understood as supporting social, epistemic, and ecological justice goals. 119 ,x
Interculturality, as described by the United Nations Educational, Social and Cultural Organization (UNESCO), refers to “the existence and equitable interaction of diverse cultures and the possibility of generating shared cultural expressions through dialogue and mutual respect.” 21 Interculturality might be expressed in a wide range of ways in integrative therapeutic contexts. However, such expressions would on the whole be characterized, in varying degrees, by an impulse toward epistemic justice wherein multiple “therapeutic cultures,” that is, forms of therapeutic knowledge and practice, might interface in ways that seek to honor their respective paradigmatic and knowledge transmission features.
Cultural safety, in turn, refers to forms of health care with two main characteristics (though, again, in varying degrees). First, they are culturally appropriate as “[d]etermined from the patient/community’s perspective” 13 ; and second, they proactively strive “to address the power imbalances inherent in the healthcare system [including] current and historical and colonial impact and…structural racism and discrimination.” 14 In this sense culturally safe iterations of therapeutic integration would—in relation to this typology’s primary conceptual features—be characterized by explicit efforts to redress long-standing inequities in health care. The principle of cultural safety is widely used to furthermore account for gender equity considerations, including in an intersectional way with ethnicity, ability, age, and other categories of identity.120,121
Returning to the examples of turmeric, acupuncture, and birth work discussed in the previous section, the actualization of the aforementioned principles may be made visible. One might turn, for example, to an Ayurveda- or Unani-focused hospital setting in a South Asian country where biomedical diagnostic techniques are actively used with the support of biomedically trained clinicians. There, traditional medicine practitioners use turmeric in clinical practice in line with ethnomedical therapeutic indications, either as a single plant (perhaps in a preparation with clarified butter or as a topical application) or in complex formulations with other herbal medicines. In the same setting, patients might receive traditionally prepared, culturally situated meals that deliberately include turmeric as a therapeutic culinary spice.
Or, one might turn to a community center in a European country where medically underserved East Asian immigrant seniors with low English language proficiency receive culturally concordant traditional acupuncture care alongside biomedical care stewarded by a community health worker with extensive knowledge of local social services. The acupuncture element of that care might be offered in an East Asian language and paired with traditional herbal medicine prescribing and culturally specified dietary recommendations aligned with ethnomedical principles, as well as access to t’ai chi, qigong (or similar gentle martial arts) classes at the same community center.
Finally, one might envision a birthing center in a Latin American country in which community-based, traditional midwives are reimbursed by the state to attend births in alignment with culturally specified traditional knowledge and practice. That birthing center might have a formalized agreement with a local biomedical hospital to facilitate seamless transport and transfer of birthing families on an as-needed basis, with traditional midwives authorized to continue offering culturally relevant supportive care in that context.
Overall, the increasing engagement of holistic, salutogenic, as well as social justice principles within some biomedical circles might be seen as conducive to therapeutic integration that falls within the present subtype. As readers familiarize themselves with the two subtypes described—Integrative Equity and Integrative Assimilation—it may become clear that further analytic granularity would prove helpful in terms of classifying a wide range of integrative therapeutic encounters within health systems. In the fourth article in this series, Type F is thus further elaborated within an expanded analytic framework that supports its practical application. That framework positions the two Integrative Therapeutics subtypes presented above as polarities on a spectrum along which five distinct “forms” of therapeutic integration are further elaborated, with additional examples. These are (beginning from the “assimilative” polarity and moving progressively toward integrative equity): Melting Pot, Co-optation, Multiculturalism, Transculturation, and Third Space. This five-part Integrative Therapeutics framework is ultimately meant to inform applications of the typology with reference to real-world settings across health systems contexts, in which multiple therapeutic approaches typically intersect. In this sense, the framework synthetically brings together the typology’s conceptual and practical elements.
Conclusion
The operational typology of TCIM presented in this work is a conceptual and practical tool constructed to support a range of interest holders (including students, practitioners, scholars, and policymakers) in making sense of the diverse and complex landscape of therapeutic practices that fall outside of, and/or have historical, cultural, and paradigmatic origins outside of, Biomedicine’s boundaries. Salient features of this typology include its strong theoretical basis in the WHO’s globally relevant, broadly inclusive definitional work; its explicitly articulated conceptual foundations informed by related critical scholarship 3 ; and its capacity to engage with a wide range of contextual considerations. In this sense, this operational typology of TCIM—with its six primary types and concomitant subtypes—represents the first comprehensive scholarly classification tool of its kind in the field with strong international relevance.
The typology represents a crucial step forward for scholars and policymakers working across the evidence-to-policy cycle and has the potential to inform a wide range of scholarly investigations and support the use of other operational tools in the field. For scholars and policy makers alike, the typology clarifies the distinct and common characteristics of diverse TCIM systems, practices, practitioners, products, and devices, in turn supporting the development and implementation of more paradigmatically aligned research approaches, critical analyses, and governance models. As a dynamic tool, the typology’s benefits are optimized when users actively engage with the concepts underlying the classification model proposed. The typology may also be fruitfully employed as a teaching tool meant to deepen critical engagement with the complex contextual issues at play with respect to therapeutic pluralism across global contexts. Readers interested in additional guidance as to the typology’s applications will refer to the third 30 and final article in this series. 4 Ultimately, this work is a resource designed to consolidate many strands of activity in the TCIM field within an inclusive, rigorously elaborated conceptual framework that honors knowledge diversity and aims toward greater health and well-being for all.
Footnotes
Acknowledgment
The author is grateful to Anne Taillefer, to readers of the SSRN preprint, and to the respected journal peer reviewers for their valuable critical feedback and questions on earlier versions of this work. Jenny Jaeckel provided artistic advice and support on ![]() , which the author deeply appreciates. The author would also be remiss not to recognize the fluffy companionship of her ginger cats and the compassionate guidance of her community of plant beings throughout the many phases of this work’s choreography.
, which the author deeply appreciates. The author would also be remiss not to recognize the fluffy companionship of her ginger cats and the compassionate guidance of her community of plant beings throughout the many phases of this work’s choreography.
Author Disclosure Statement
No interests to declare.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability
No data were generated or collected for the present article.