
Abstract
Introduction:
This work presents an analytic framework for describing the unique features of Traditional, Complementary, and Integrative Medicine (TCIM) governance, based on datasets from across the Americas, a region globally notable for its cultural and legal pluralism. In response to World Health Organization (WHO) guidance, the Pan American Health Organization expanded its TCIM technical cooperation, investing in governance-related research and fostering a TCIM regional network.
Methods:
Using the Framework method developed by Richie and Spencer, the authors iteratively constructed the framework with reference to over 500 TCIM-related policy instruments, court cases, and other governance approaches.
Results:
Seven primary analytic categories comprise the framework: (1) jurisdiction, (2) governance type, (3) specificity, (4) TCIM type, (5) health systems elements, (6) intersectoral dimensions, and (7) TCIM aspects addressed. Together, these categories (along with related subcategories and analytic tags) enable systematic tracking of diverse Indigenous, state, civil society, and private sector governance approaches applied to TCIM systems, practitioners, practices, and products. The framework facilitates detailed monitoring of numerous TCIM governance issues (e.g., financing, human resources, service provision, information management, biodiversity, traditional knowledge protection). It also accounts for the influence of international and regional governance instruments and recognizes the intersectoral character of TCIM governance in many settings.
Conclusion:
The framework offers a harmonized analytic approach to tracking TCIM governance and may be transferable to other regions. As such, it provides a preliminary architecture for a future digital online repository of global TCIM governance. This kind of resource, aligned with WHO recommendations, would help to close expertise gaps—such as those related to regulatory frameworks, health systems integration, and culturally responsive practices—identified by countries as barriers to TCIM governance. It also has the potential to support horizontal cooperation among diverse interest-holders, including policymakers, health professionals, private sector representatives, researchers, Indigenous peoples, and community-based actors.
Keywords
Introduction
For over four decades, the World Health Organization (WHO) has formally recognized that traditional, complementary, and integrative medicine (TCIM) practitioners, practices, and products, as well as their affiliated systems of knowledge, have important roles to play in advancing primary health care around the world. The WHO’s commitment to advancing public health through TCIM’s inclusion in national health systems has been evident in its Declarations of Alma Ata (1978), 1 Beijing (2008), 2 Astana (2018), 3 and Gujarat (2023), 4 as well as three Traditional Medicine Strategies (2002–2005, 5 2014–2023, 6 2025–2034 7 ) As these and other related WHO documents recognize, TCIM’s widespread worldwide use in primary health care includes jurisdictions where TCIM “practitioners are the first contact and sometimes the only health providers available.” 8 As an important source of culturally responsive, people-centered care in many settings, TCIM is especially relevant to historically marginalized communities, including but not limited to Indigenous peoples, ethnospecific groups, and rural or underserved populations. TCIM’s interface with health systems offers transformative opportunities to advance health equity and well-being-focused societies.
While the number of WHO member states implementing national policies related to TCIM, as well as regulations governing related practitioners and products, has steadily increased in recent decades, many governance-related challenges remain. Although “lack of research data” has been identified as the primary difficulty faced with regard to TCIM regulatory issues, member states also highlight numerous specific challenges directly related to TCIM governance. 9 These include a “lack of expertise within national health authorities and control agencies”; a “lack of appropriate mechanisms” for governing TCIM practitioners, practices, and products; and a “lack of cooperation channels” between countries for information sharing about TCIM governance.
The WHO’s most recent Traditional Medicine Strategy (2015–2034) prioritizes the advancement of TCIM-related governance of various kinds around the world, as well as related research and information sharing. 7 Echoing earlier versions,5,6 the current strategy prioritizes the regulation of TCIM practitioners, practices, and products to support the safe inclusion of related services within primary health care. 7 Expanding on the scope of what was stipulated in previous strategies, this document also recognizes that TCIM governance takes place at the international, national, and subnational levels, and across multiple sectors, requiring coordinated action. It recognizes that TCIM governance must be context-appropriate and calls for the involvement of diverse stakeholders in policy development. It also emphasizes cross-sectoral dialogue and policy action across the health care system, with the education and private sectors, and regarding such matters as biodiversity, traditional knowledge protection and benefit sharing, well-being, cultural appropriateness, and affordability. To monitor countries’ success in achieving these aims and to identify contextually transferable best practices, a systematic, rigorous approach will be needed.
The WHO currently monitors just three types of governance mechanisms for TCIM: National Policies, National Legislation, and National Regulation on Herbal Medicines. 9 However, as the WHO’s Traditional Medicine Strategy 2015–2034 recognizes,9,10 TCIM governance across the globe is complex. For example, at the state level, it spans the entire spectrum of states’ hierarchy of the law, from the constitution down to regional, municipal, and institutional mechanisms. 11 Moreover, TCIM governance approaches extend well beyond statal mechanisms and are evident in Indigenous communities, the private sector, and civil society. 12 To date, however, there are few guidance resources available for decision makers seeking to govern TCIM and its elements (e.g., practitioners, practices, products, devices).11–13 Nor are there rigorous analytic tools available for scholars that are specific to TCIM governance and address the sphere’s complexity. To help fill these gaps, and with reference to TCIM governance-related datasets from the Americas region, this work proposes a descriptive analytic tool for classifying diverse TCIM governance approaches, including and beyond statal mechanisms.
Methods
Because this research involved only document review and no human participants, no ethics review was required. In developing this work’s analytic framework for TCIM governance, the authors engaged with an applied policy research method called “Framework,” introduced by Ritchie and Spencer. 14 Applied policy research can take various forms, including “contextual” research (such as the current work) focused on “identifying the form and nature” of a particular domain’s elements. According to Ritchie and Spencer, some advantages of the Framework method are that it is “grounded” (in data), “dynamic” (in the sense that the resulting analytic model, that is, framework may be iteratively amended), and “systematic” (in that the framework may be repeatedly applied to similarly treat related units of analysis).
The Framework method consists of a series of five stages characterized together by a “systematic process of sifting, charting, and sorting materials according to key issues and themes” of interest in relation to a particular area of inquiry. Framework’s five stages are: (a) data familiarization, (b) identification of a thematic framework, (c) indexing, (d) charting, and (e) mapping and interpretation. In developing the analytic framework presented in this work, the authorship team engaged primarily with the first three stages of the Framework method. However, all five stages are relevant to the authors’ larger scholarly project of tracking and analyzing TCIM governance approaches from around the world. The authorship team’s work engaging with Framework’s fourth and fifth stages (through which the authors are actively conducting in-depth analyses of TCIM governance approaches in specific countries and regions) is ongoing and will be reported elsewhere.
Below, the authors present a detailed account of the methods used to develop the analytic framework and to detail the specifics of this tool’s concomitant elements and their application utility. This account is intended to provide knowledge users with sufficient information to not only engage with the tool themselves, but also to evaluate future reporting of the tool’s application.
As Ritchie and Spencer indicate, the Framework method’s stages are “highly interconnected” and may proceed in an iterative, recursive (rather than prescriptive, linear) manner. This was very much the authors’ experience with this methodological approach. The project’s origins are multiple, initially arising from separate bodies of policy analytic work in the Americas region by Gallego-Perez and Ijaz, respectively. In a doctoral dissertation, Gallego-Perez had proposed a set of policy analytic parameters for TCIM practitioners and practices with respect to the civil law contexts of Latin America.11,15 This work applied the construct of the “hierarchy of laws” 16 to characterize the wide range of state governance approaches at play across the analyzed contexts, ranging from national constitutions and laws to a wide range of (formal and informal) policy-setting mechanisms, including national policies, regulations, and position documents without administrative sanction.
Independently but in tandem, Ijaz had been conducting analyses of TCIM governance within the hybrid civil/common law contexts of Canada and the United States of America.12,17–20 These analyses not only addressed statutory governance in terms of national and subnational policy making, but also with respect to governance taking place within civil society and the private sector. Like the work of Gallego-Perez, Ijaz’s research drew attention to the limitations of current WHO reporting around global TCIM governance. In dialogue, these authors began a collaborative process, aligned with the framework method, aimed at developing an analytic model capable of comprehensively describing the wide range of TCIM governance approaches in use across the Americas region. From the outset, the intention was to create a data-driven analytic model that could ultimately be used around the world.
Following the Framework method’s first stage (data familiarization), 14 the lead authors immersed themselves in their respective TCIM governance datasets (some published, some unpublished) from Latin America, Canada, and the United States. They also familiarized themselves with the contents of an expanded database of TCIM governance instruments from Latin American and Caribbean countries, which extended Gallego-Perez’s compilations to include TCIM products and intercultural health instruments. This expanded database was developed by coauthor de la Ossa as part of a consultancy with the Pan American Health Organization, supervised by coauthors Bascolo and Rosell De Almeida. Altogether, these datasets tracked over 550 distinct TCIM-related governance mechanisms across the region. In this process of data familiarization, the authors iteratively and collaboratively engaged with the framework’s second stage (identification of a thematic framework), seeking to construct analytic parameters capable of classifying the wide range of TCIM governance approaches in the engaged datasets.
As a team, the authors iteratively constructed a thematic classification model from their analytic codes and categories to account for the distinct features of TCIM governance across the Americas region. To this end, they engaged with the Framework method’s third stage, indexing, which enabled consistent labeling and categorization of governance mechanisms for systematic analysis.” In data immersion, the authors used a descriptive content analysis approach of data coding and categorization to classify the range of policy approaches in their datasets. Using the qualitative research principle of saturation (rather than an exhaustive coding process), the authors determined that the framework was robust once the team’s existing categories consistently accounted for the features of the wide range of governance approaches in the project datasets.
Overall, the authors privileged an inductive approach to category building. However, in areas where relevant classification systems existed, the authors took them into consideration in constituting the otherwise inductively derived categories. Where this was the case, the authors make it explicit in the Results section. Further, some design decisions were made with an inclusive view to supporting the framework’s transferability to other regions moving forward. All coauthors validated the analytic model based on their specialized expertise in health governance and regional knowledge of the Americas. The framework described in what follows is the result of this process. Illustrative exemplars of TCIM governance from the engaged datasets support the overview provided of each of the framework’s thematic categories.
Results: The Framework
This framework is designed as a descriptive analytic tool for classifying the range and characteristics of diverse TCIM governance mechanisms. To track the specific governance mechanism being classified, the framework invites users to begin by collecting that mechanism’s basic identifying details (name, year enacted, instrument number, etc.) along with a synthetic narrative account of its objectives and TCIM-related scope. As shown in Table 1, the framework itself is comprised of seven primary thematic categories (each of which has subcategories and/or additional descriptive “tags”). These categories are: (1) jurisdiction, (2) governance type, (3) specificity, (4) TCIM type, (5) health systems elements, (6) intersectoral dimensions, and (7) TCIM aspects addressed. The sections that follow provide a brief overview of each category’s aims and primary features, along with illustrative exemplars for each, drawn from the authors’ Americas regional datasets. Where elements of the framework draw upon or represent modifications of other analytic instruments, this is made explicit.
TCIM Governance Framework Map: Categories and Subcategories
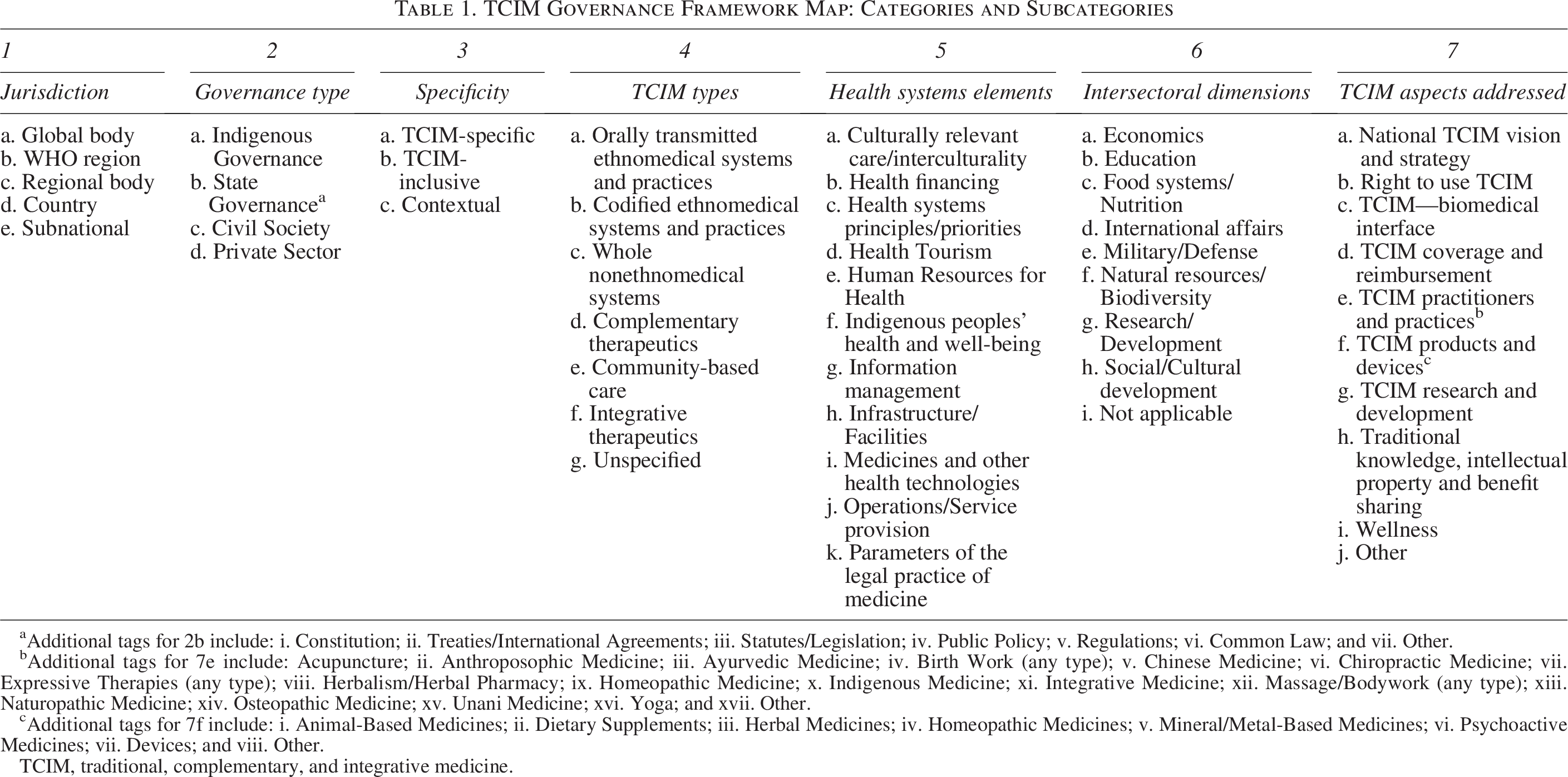
Additional tags for 2b include: i. Constitution; ii. Treaties/International Agreements; iii. Statutes/Legislation; iv. Public Policy; v. Regulations; vi. Common Law; and vii. Other.
Additional tags for 7e include: Acupuncture; ii. Anthroposophic Medicine; iii. Ayurvedic Medicine; iv. Birth Work (any type); v. Chinese Medicine; vi. Chiropractic Medicine; vii. Expressive Therapies (any type); viii. Herbalism/Herbal Pharmacy; ix. Homeopathic Medicine; x. Indigenous Medicine; xi. Integrative Medicine; xii. Massage/Bodywork (any type); xiii. Naturopathic Medicine; xiv. Osteopathic Medicine; xv. Unani Medicine; xvi. Yoga; and xvii. Other.
Additional tags for 7f include: i. Animal-Based Medicines; ii. Dietary Supplements; iii. Herbal Medicines; iv. Homeopathic Medicines; v. Mineral/Metal-Based Medicines; vi. Psychoactive Medicines; vii. Devices; and viii. Other.
TCIM, traditional, complementary, and integrative medicine.
Jurisdiction
This category classifies TCIM governance approaches according to their territorial jurisdiction, beginning with their affiliated WHO region, country, and (where relevant) subnational jurisdiction (e.g., state, province, municipality).
Because TCIM governance in specific regions and countries is impacted by larger global policy contexts, the framework also tracks instruments put in place by a global body, which bear on how countries govern TCIM within their borders.
The framework similarly documents governance instruments produced by a regional body, which impact nations’ specific TCIM governance approaches.
Governance type
In recognition of the multisectoral nature of public health governance, this category enables classifications of the sector in which a TCIM governance mechanism is being enacted, with reference to four primary domains: Indigenous governance, state governance, civil society, and the private sector. In addition to being data-driven, the first domains are informed by the JuriGlobe classification model of legal systems around the world
22
; the second two derive from PAHO’s recognition in its Essential Public Health Functions framework,
23
of the range of stakeholders involved in health systems governance. Because the authors identified governance mechanisms in the region with overlapping sectoral domains, the framework permits multiple classifications for a single governance mechanism.
To account for the wide range of state mechanisms used to govern TCIM, this category also includes a second classification layer involving seven subcategories. These are: constitution, treaties/international agreements, legislation, public policy, regulations, common law, and other governance instruments. These categories were informed by the hierarchy of laws model developed by the International Foundation for Electoral Systems
16
and modified to better account for TCIM governance approaches identified in the project datasets. In this framework, state policy instruments are classified into the highest applicable level within the hierarchy of laws. For example, an instrument titled “National Policy,” issued or enacted through a law, is classified as “Legislation” rather than “Public Policy.”
Further, there are various examples of public policy across the region, such as Haiti’s National Health Policy (2012) and National Pharmaceutical Policy (2014), which both address the governance of traditional Haitian medicine as a central element of the country’s health care. With respect to common law (established through judicial precedent), there are court rulings in some US states (e.g., Oregon, 2014) that have determined in which licensed professions’ scopes the use of acupuncture needles is permitted.
Specificity
This category classifies TCIM governance approaches by their degree of TCIM-specificity, that is, according to whether they “only” address TCIM (TCIM-specific), address TCIM as well as other matters (TCIM-inclusive), or bear indirectly on TCIM’s governance in a nonexplicit way (contextual). A particular governance approach may only be classified with reference to one of the three subcategories of specificity.
TCIM types
The purpose of this category is to permit analytic differentiation between the mechanisms used to govern a wide range of TCIM approaches in use around the world. To this end, the framework engages (in an unmodified form) the six “types” elaborated in Ijaz’s operational typology of TCIM,
24
which differentiates between diverse TCIM systems, practices, products, and devices based on their historical, cultural, and paradigmatic features. There are countries where a single governance approach may encompass multiple TCIM types; in other cases, specific TCIM elements are addressed through individual governance mechanisms.
Health systems elements
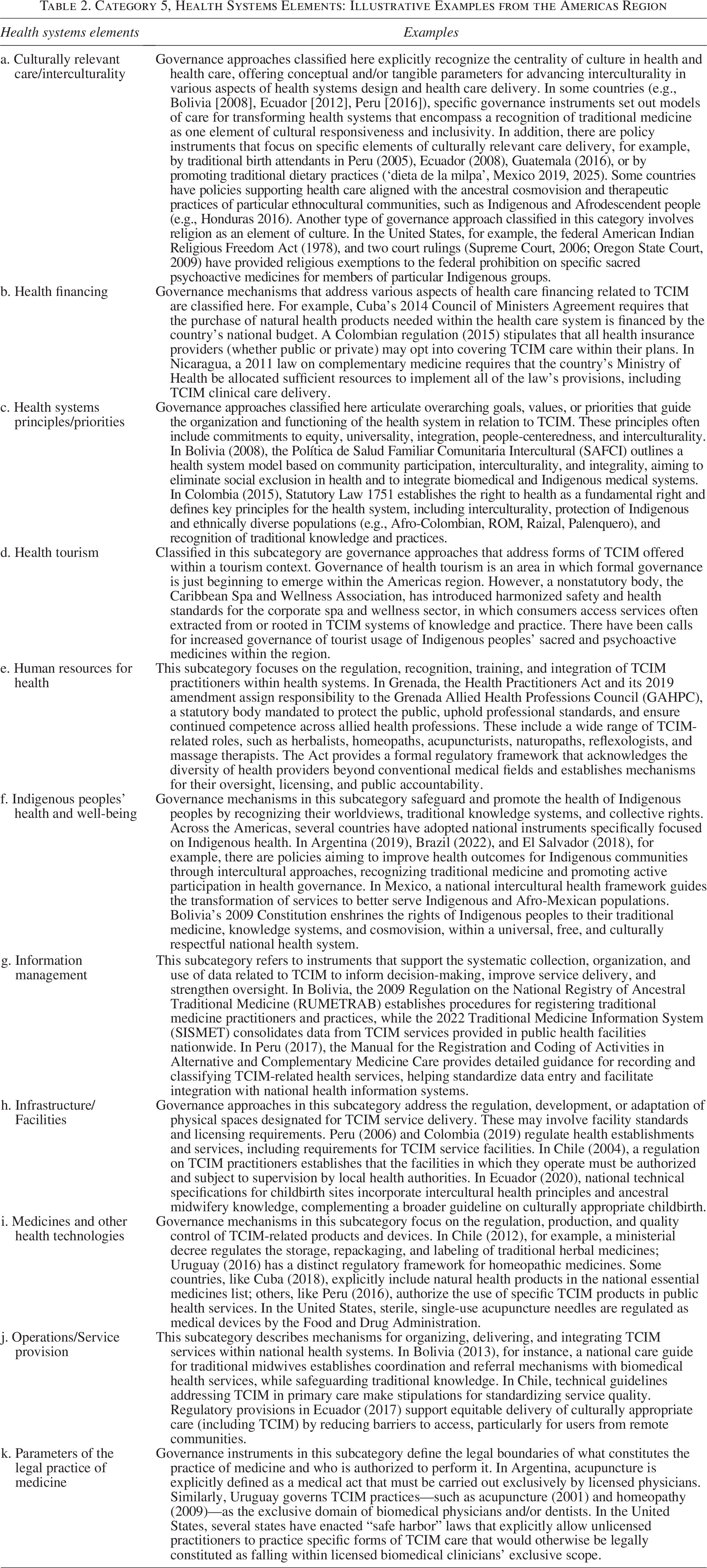
This category aims to contextualize particular TCIM governance approaches by identifying which elements of a jurisdiction’s health system they address. The 11 subcategories used for this purpose were dually informed by an iterative coding and classification process using data from the Americas region. In addition, some elements of the Pan American Health Organization’s Essential Public Health Functions framework, 23 —in particular, its conceptualization of resource allocation as an essential public health function—informed the narrative framing of three of the subcategories* outlined below. These are: culturally relevant care/interculturality, health financing*, health systems principles/priorities, health tourism, human resources for health*, Indigenous peoples’ health and well-being, information management, infrastructure/facilities, medicines and other health technologies*, operations/service provision, and parameters of the legal practice of medicine. Table 2 briefly explains each subcategory’s scope and provides illustrative examples.
Category 5, Health Systems Elements: Illustrative Examples from the Americas Region
Intersectoral dimensions
This category and its subcategories emerged inductively as it became clear that some governance approaches addressing TCIM do not limit their scope to the health care sector alone. The resulting seven data-driven subcategories are: economics, education, food systems/nutrition, international affairs, military/defense, natural resources/biodiversity, research/development, and social/cultural development. Importantly, many TCIM governance approaches are not explicitly intersectoral and may be classified here using the “not applicable” category.
TCIM aspect addressed
This category uses 10 subcategories that identify the specific thematic aspect or facet of TCIM being governed. Developed through a thematic coding process, these subcategories, shown in Table 1, address (among others) TCIM-related national visions/strategies, practitioners and practices, products and devices, and coverage and reimbursement, as well as issues related to wellness, intellectual property rights, research and development, the TCIM-biomedical interface, and the right to use TCIM. Table 3 provides illustrative exemplars for each of these subcategories.
Category 7, TCIM Aspects Addressed: Illustrative Examples from the Americas Region
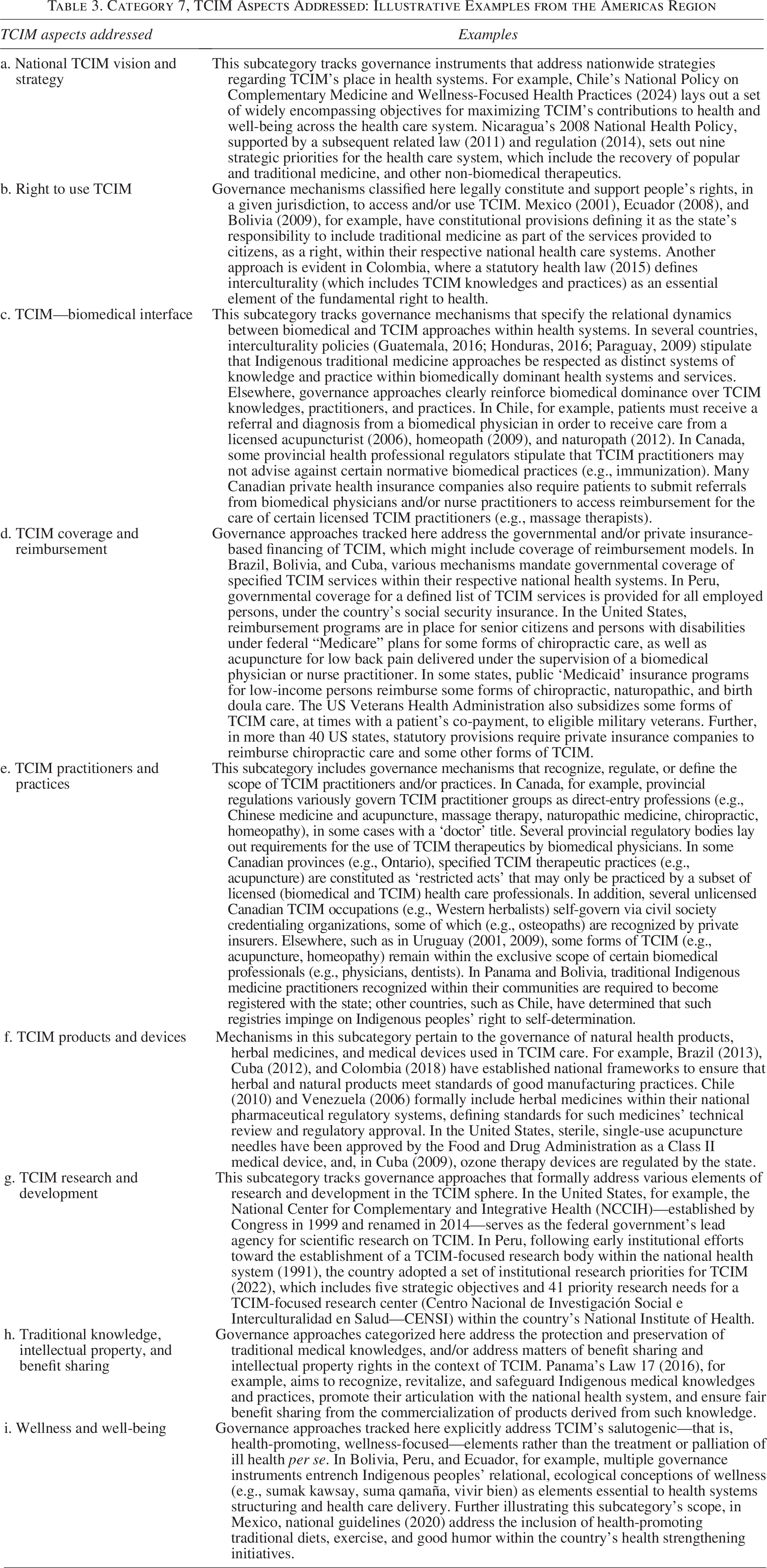
To permit further analytic nuance, the framework uses additional “tags” for two of the most widely used subcategories in the authors’ experience to date (see Table 1). In the first case (TCIM practitioners/practices), a pragmatic decision was made to explicitly list particular TCIM practitioner types for which the authors had identified more than seven country examples in our datasets (or around the world). In the second case (TCIM products/devices), the principle of comprehensiveness was used to iteratively create, with reference to the project datasets, seven distinct tags that could account for the range of TCIM medicinal products being governed.
Discussion
This work’s data-driven analytic framework provides, for the first time, a systematic classification model for describing the unique features of TCIM governance across diverse contexts, national and legal constructs, and governance mechanisms. Iteratively constructed with reference to over five hundred TCIM-related policy instruments, court cases, and other governance approaches tracked across the Americas region, the framework is comprised of seven primary analytic categories. These categories, along with their concomitant subcategories and analytic tags, permit detailed tracking of a wide range of Indigenous, state, civil society, and private sector governance approaches used across countries to govern diverse TCIM systems, practitioners, practices, products, and devices. Importantly, the framework reflects the cross-sectoral and multilevel nature of TCIM governance, extending well beyond what has been previously tracked by the WHO. As illustrated through numerous regional exemplars, TCIM governance may be enacted across the entire hierarchy of state law, from national constitutions to nonstatutory administrative documents. While some countries may govern TCIM strictly in relation to service provision and product safety, others engage TCIM approaches, including Indigenous knowledge, to foundationally inform health systems design. The framework also recognizes the range of substantive issues that TCIM governance may address, from culturally relevant care delivery and Indigenous peoples’ health and intellectual property rights to reimbursement, health tourism, and information management. Further reflected in the framework are the influences of international and regional governance instruments on the ways in which countries govern various aspects of TCIM.
The authors’ primary aim in this work was to use the Framework method to construct a thematic framework capable of tracking the range of TCIM-related governance approaches in the Americas region. The authorial team is currently applying this framework in a systematic way to their existing datasets. The results of these analyses will be published elsewhere, further illustrating the framework’s utility. For example, the framework’s capacity to track the range of TCIM governance approaches in a single country will permit multilayered, multisectoral analyses that account for statal and nonstatal mechanisms. This includes “ecological” analyses of the ways in which a country’s range of TCIM governance mechanisms intersect to produce a broader TCIM governance ecosystem. Such analyses may specifically illuminate the ways in which Indigenous and state governance may be interfacing, and how civil society and private sector actors may be intervening to address state governance gaps. At the subregional or regional level, the framework’s categories can support comparative studies of different approaches to governing similar TCIM elements (e.g., service coverage/reimbursement, practitioners, products). It could also enable analyses of the value of specific governance instruments (e.g., constitutional provisions, national policies) in supporting health systems transformations that center on TCIM knowledges and practices. Likewise, the framework allows for comparative analyses of how specific TCIM systems (e.g., Indigenous traditional medicine, Ayurvedic medicine, Chinese medicine), practices (e.g., massage therapy, mindfulness), or products (e.g., psychoactive herbal medicines) are being governed across jurisdictions.
Consistent with the Framework method’s iterative character, the authors consider this analytic framework for TCIM governance to be an adaptive tool and anticipate that additional subcategories and tags may be added as the framework gets applied across contexts. This includes applications to other regions, which some of the authorship team members are currently undertaking in an effort to determine the framework’s potential transferability beyond the Americas. The authors are aware, for example, that in the Eastern Mediterranean and African regions, there are a number of countries in which religious law is a key component of the legal system, which the authors anticipate may have implications for TCIM governance that were not evident in the Americas region. This may require adaptations or additions to the framework in the future. Nevertheless, the Americas region is uniquely diverse among global regions in its multifaceted representation of low-, middle-, and high-income countries, as well as the presence and combination of different legal frameworks (e.g., civil and common law, centralized and federal states). In addition, the region’s strong presence of Indigenous peoples, who have actively and effectively struggled for recognition of their self-determination, including their healing traditions, has strongly impacted TCIM governance across the region. Together, these factors, which are reflected in the datasets that informed the framework’s design, lend robustness to the prospect of its potential relevance for tracking TCIM governance more globally.
The WHO’s Traditional Medicine Strategy 2025–2034 has called for global information sharing about TCIM governance. 7 This work’s framework has the potential to advance that goal by offering a preliminary architecture for a searchable digital repository of TCIM governance approaches around the world. This vision aligns closely with calls within the 2023 Gujarat Declaration of the WHO’s first Global Summit on Traditional Medicine for “digital health resources on TCIM” to be used in advancing “people’s health and well-being supported by the development of comprehensive governance models, policies, [and] regulatory frameworks.” 4 There have to date been several global and regional efforts to track TCIM governance, each with strengths and limitations. Globally, the WHO has, since 2005, disseminated the results of three global surveys tracking national policies and legislation on TCIM, as well as herbal medicine regulations.9,10,25 While valuable, governance approaches outside of these three categories have not been systematically monitored in that process. At the regional level, there have been focused efforts to more comprehensively track a broader range of statal TCIM governance instruments,11,12,26–30 including as part of a virtual health library in the Americas region. 31 However, the authors are unaware of efforts to track the important place of non-statal TCIM governance (e.g., Indigenous, civil society, private sector) around the world. Nor has there been, to date, a centralized platform where decision makers might access, in a searchable, indexed format, the kinds of TCIM governance approaches being adopted across jurisdictions.
The WHO is currently developing an online Global Traditional Medicine Library to make available a range of informational resources relevant to TCIM stakeholders. 32 Sharing of governance-related information on this platform would strongly support efforts to advance TCIM governance across jurisdictions. The categories, subcategories, and tags that constitute this work’s analytic framework offer a rigorous basis for an indexed online compilation of TCIM governance around the world. Such a resource would enable decision makers, researchers, occupational groups, and civil society actors to systematically sort, filter, and cross-reference information relevant to specific governance needs. A digital database of this kind would help knowledge users to better understand how countries around the world are addressing similar issues. It could also help close the expertise gaps identified by WHO member states as barriers to TCIM governance. Critically, the tool could promote horizontal cooperation between countries (among other stakeholders) by making accessible the range of instruments and strategies deployed in TCIM governance across contexts. By identifying exemplars of TCIM governance addressing particular issues, decision makers could, in turn, conduct more detailed analytic reviews and meaningful experience exchanges. In this way, as multisectoral stakeholders seek to transform health systems in culturally relevant, people-centered ways, the authors hope that this work may support a more encompassing understanding of the role of TCIM governance in advancing universal health and well-being.
In conclusion, this framework addresses critical gaps in the systematic analysis and classification of TCIM governance mechanisms. By enabling consistent tracking and comparison of governance approaches, the tool can guide policymakers, researchers, and practitioners toward more coherent, context-sensitive, and integrated health systems.
Authors’ Contributions
Conceptualization: D.F.G.P. and N.I. Data curation: D.F.G.P., N.I., and M.D.O. Formal analysis: D.F.G.P., N.I., and M.D.O. Investigation: D.F.G.P., N.I., and M.D.O. Methodology: D.F.G.P. and N.I. Supervision: G.R.A. and E.B. Validation: D.F.G.P., N.I., M.D.O., G.R.A., and E.B. Writing—original draft: D.F.G.P., N.I., and M.D.O. Writing—review and editing: D.F.G.P., N.I., M.D.O., G.R.A., and E.B.
Footnotes
Author Disclosure Statement
The authors have no conflicts to declare.
Funding Information
The Pan American Health Organization/World Health Organization (PAHO/WHO) partly funded time on this project for D.F.G.P., M.D.O., G.R.A., and E.B. N.I. was partly funded by a Project Grant [PJT-175030] from the Canadian Institutes of Health Research.