
Abstract
Background:
Xuebijing injection was approved for treating sepsis; however, the efficacy and safety of Xuebijing injection in population with sepsis need further evaluation. We aimed to evaluate the safety and efficacy of Xuebijing injection on sepsis.
Materials and Methods:
We searched for potential randomized controlled trials about Xuebijing injection and sepsis from six public databases. Primary outcomes included the 28-day mortality and mortality during treatment. Our secondary outcomes were body temperature, APACHE Ⅱ score, and adverse events or reactions. All data were synthesized by the meta package.
Results:
A total of 3007 patients (1551 patients receiving the conventional treatment combined with Xuebijing injection and 1456 patients receiving the conventional treatment only) were included. We found Xuebijing injection reduced the 28-day mortality (risk ratio = 0.69 [0.60–0.78], p < 0.0001), mortality during treatment (risk ratio = 0.74 [0.62–0.88], p = 0.0009), APACHE II score (mean difference = 3.91 [2.45–5.38], p < 0.0001), and body temperature (mean difference = 0.43 [0.31–0.55], p < 0.0001) without obvious adverse events (risk ratio = 0.91 [0.77–1.07], p = 0.2405).
Conclusions:
Xuebijing injection is effective and safe for treating sepsis. Additional methodologically sound trials with long-term mortality as an outcome measure could provide further insights into whether Xuebijing injection offers an enhanced therapeutic effect for sepsis.
Introduction
Sepsis is a serious condition with high morbidity and mortality for which treatment advancements are desperately needed. 1 Early identification and immediate treatment can reduce the mortality of sepsis. 2 Management of patients with established sepsis includes hemodynamic management, corticosteroids (such as hydrocortisone), and adjunctive therapies (anti-inflammatory and immune stimulation strategies [such as interleukin-7 and checkpoint inhibitors], renal replacement therapy, cytokine removal, and general intensive care management [such as positive pressure mechanical ventilation and extracorporeal membrane oxygenation]).3,4 Traditional Chinese Medicine for treating diseases is gradually being accepted by more and more people due to its unique advantages.5–7 Xuebijing injection (a Chinese patent) is prepared from a combination of Carthamus tinctorius flowers (Honghua), Paeonia lactiflora roots (Chishao), Ligusticum chuanxiong rhizomes (Chuanxiong), Angelica sinensis roots (Danggui), and Salvia miltiorrhiza roots (Danshen). Xuebijing injection is prescribed for various diseases, including sepsis, 8 acute pancreatitis, 9 spontaneous bacterial peritonitis in liver cirrhosis, 10 severe community-acquired pneumonia, 11 as well as Corona Virus Disease 2019-induced cardiac dysfunction. 12
Xuebijing injection has been used for the treatment of sepsis for a long time. Previous studies have systematically evaluated the safety and efficacy of Xuebijing injection in treating sepsis, but the sample size included was very small. A previous meta-analysis that included 16 randomized controlled trials (1144 patients) showed that add-on therapy with Xuebijing injection not only improves the 28-day mortality but also reduces body temperature, white blood cell count, and APACHE Ⅱ score without serious adverse events among patients with sepsis. 13 Nevertheless, due to the relatively low quality of included randomized controlled trials, the clinical routine application of Xuebijing injection is limited. In recent years, high-quality clinical trials have emerged one after another, such as the EXIT-SEP randomized clinical trial, 14 so we here conducted an updated systematic review and meta-analysis of randomized controlled trials with 3007 patients to provide a more reliable evidence-based medical solution for Xuebijing injection treatment of sepsis.
Methods
Our study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. We followed a structured approach to ensure transparency and reproducibility, including the development of a predefined protocol, a comprehensive literature search, study selection, data extraction, and quality assessment.
Population
Patients who were diagnosed with sepsis, including severe sepsis and septic shock, according to recognized diagnostic criteria15,16 were included in our analysis.
Interventions and comparisons
Trials comparing Xuebijing injection used for sepsis versus whether a placebo or no treatment were eligible for inclusion. Xuebijing injection could be an add-on therapy. The studies comparing the efficacy and/or safety of Xuebijing injection and other drugs were excluded. The conventional treatment for sepsis included nutritional support, fluid resuscitation and vasopressors (maintenance of arterial blood pressure), antibiotics application, early treatment of the source of infection, and necessary mechanical ventilation. 17
Outcomes
Trials with at least one of the following outcomes were eligible for inclusion. Primary outcomes included mortality during treatment and 28-day mortality. Secondary outcomes were body temperature, APACHE Ⅱ score, and adverse events or reactions. Consistent with the guidance provided in CONSORT Harms 2004,18,19 We defined adverse events or reactions as the totality of possible adverse consequences of Xuebijing injection, which might be assessed systematically by measuring variables using standardized clinical examinations, questionnaires, and medical instruments.
Study design
Published randomized controlled trials were eligible for inclusion. We excluded nonrandomized studies as they were associated with a high risk of bias. The methodological quality of literature was evaluated with the Cochrane Risk of Bias Tool (version 2), 20 which is structured into a fixed set of domains of bias, including randomization, deviations from intended interventions, missing data, outcome measurement, and selection of the reported result.
Data source
Some electronic databases (PubMed, Embase, Cochrane, CNKI, Wanfang Databases, and Chinese Scientific Journal Database) were searched with the keywords of “Xuebijing,” “sepsis,” and “randomized.” We further searched the reference lists for relevant studies. We searched for literature from the inception until July 31, 2023.
Study selection and evaluation
Two reviewers independently screened the literature based on predetermined criteria. Detailedly, first, we detected and deleted the duplications from the retrial results. Second, we deleted the obviously irrelevant literature after reading the corresponding title and abstract. Finally, we only included the relevant literature after reading the full texts. After that, two reviewers independently assessed the bias risk of the included literature to evaluate the methodological quality. Any disagreement was discussed and consulted by the third reviewer.21,22
Data extraction
Data from the included literature were independently extracted by another two reviewers. The extracted data included the characteristics of the literature and characteristics of the study design (disease type, interventions, treatment duration, and outcomes). For the continuous indicators, means and standard deviations were extracted. For the dichotomous indicators, frequencies and rates were extracted. We contacted the authors for incomplete data, if applicable.
Statistical analysis
All data were analyzed by the meta package 23 (version 6.0-0) in R. All data were presented as the risk ratios or mean differences with 95% confidence intervals. We selected the fixed or random effect models based on study characteristics. We chose the random effect models if the studies were too heterogeneous based on selected characteristics; otherwise, we chose the fixed effect models. If heterogeneity was found, subgroup analysis was conducted to find the source. When more than 10 trials were included, a funnel was conducted to detect the publication bias. Multiple imputation was performed if necessary. Finally, sensitivity analysis was applied to test the robustness and reliability.
Results
Study selection
In total, 1954 publications were identified in the literature search, and 812 duplicated citations were excluded. After screening the titles and abstracts, 1019 irrelevant publications describing animal experiments, case reports, or reviews were excluded. After reading the full text of the remaining studies, 105 records were excluded. Finally, 18 trials were included in our study (Supplementary Fig. S1).
Study characteristics
We identified 1954 records, and 18 trials were included, covering 3007 participants (1551 patients receiving the conventional treatment combined with Xuebijing injection and 1456 patients receiving the conventional treatment only).14,24–40 One trial was separated into three studies containing a low dosage (50 mL b.i.d.), a moderate dosage (100 mL b.i.d.), and a high dosage (100 mL q.i.d.) Xuebijing injection 36 and one trial was separated into two studies containing a low dosage (100 mL q12h) and a high dosage (100 mL q8h) Xuebijing injection. 40 All the included randomized controlled trials were conducted in China and were mostly published in Chinese (one trial was published in English 14 ). The details of the included studies are shown in Supplementary Table S1.
Methodological quality
According to the Cochrane Risk of Bias Tool (version 2), the methodological quality of all included literature was acceptable (Supplementary Fig. S2), although two studies27,37 were classified as high-risk, overall assessment was still mainly low-risk.
Primary outcomes
In total, 14 trials with 2774 participants (1394 participants in the Xuebijing injection group and 1380 participants in the control group) reported the primary outcome of 28-day mortality (Supplementary Table S1). As shown in Figure 1, compared with the conventional treatment, Xuebijing injection therapy combined with the conventional treatment decreased the 28-day mortality rate by 31% (risk ratio = 0.69, 95% confidence interval = 0.60–0.78, p < 0.0001) with no heterogeneity (I2 = 0%, p = 0.9935).
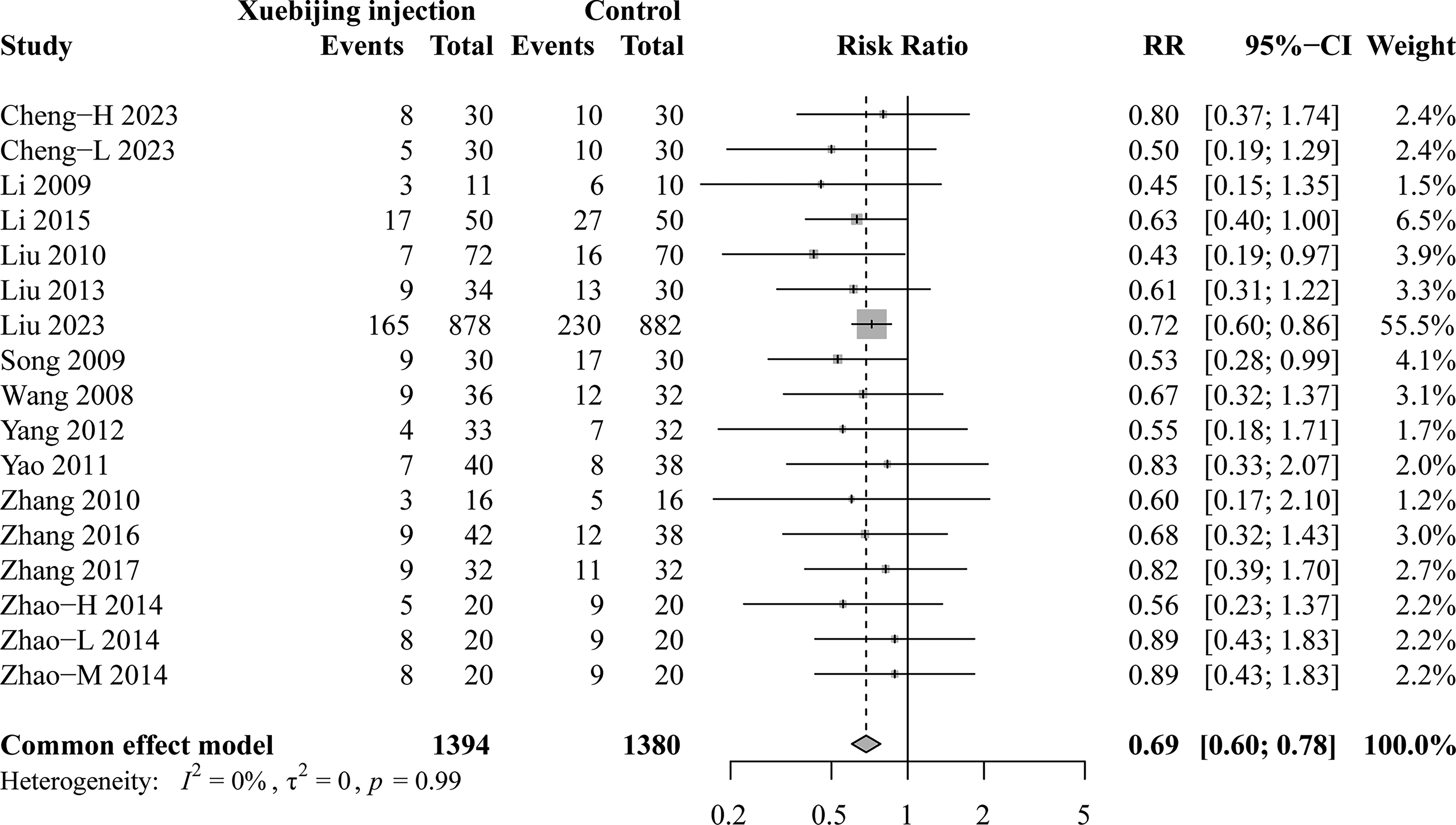
Xuebijing injection treatment compared with conventional treatment for 28-day mortality.
Among 18 trials, 6 trials14,25,26,34,35,39 with 2070 participants (1034 participants in the Xuebijing injection group and 1036 participants in the control group) reported mortality during treatment (Supplementary Table S1). Xuebijing injection therapy combined with the conventional treatment decreased the mortality during treatment by 26% (risk ratio = 0.74, 95% confidence interval = 0.62–0.88, p = 0.0009) with no heterogeneity (I2 = 0%, p = 0.5053) compared with the conventional treatment alone (Fig. 2).
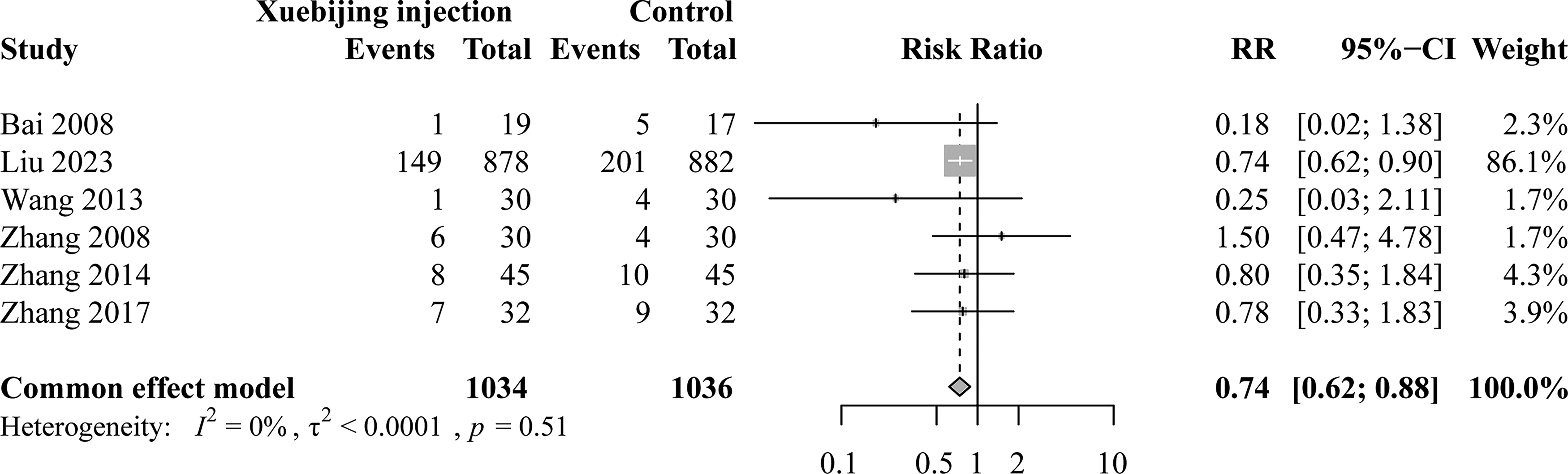
Xuebijing injection treatment compared with conventional treatment for mortality during treatment.
Secondary outcomes
Fourteen trials with 2674 participants (1338 participants in the Xuebijing injection group and 1336 participants in the control group) reported APACHE Ⅱ score (Supplementary Table S1). Xuebijing injection therapy combined with the conventional treatment decreased APACHE Ⅱ score by 3.91 (95% confidence interval = 2.45–5.38, p < 0.0001) with heterogeneity (I2 = 96%, p < 0.0001) compared with the conventional treatment alone (Fig. 3). The subgroup analysis was conducted by sample size and Xuebijing injection dosage. Compared with the conventional treatment alone, Xuebijing injection therapy combined with the conventional treatment decreased APACHE Ⅱ score by 3.79 (95% confidence interval = 2.56–5.01, p < 0.0001) without heterogeneity (I2 = 28%, p = 0.20) for sample size of less than 70 and 3.98 (95% confidence interval = 1.21–6.75, p < 0.0001) with heterogeneity (I2 = 98%, p < 0.01) for sample size of more than 70 (Supplementary Fig. S3A). Compared with the conventional treatment alone, Xuebijing injection therapy combined with the conventional treatment decreased APACHE Ⅱ score by 5.21 (95% confidence interval = 0.98–9.44, p < 0.0001) with heterogeneity (I2 = 99%, p < 0.01) for 100 mL b.i.d., 4.11 (95% confidence interval = 2.43–5.79, p < 0.0001) without heterogeneity (I2 = 41%, p = 0.16) for 100 mL q.i.d., and 3.03 (95% confidence interval = 1.97–4.09, p < 0.0001) without heterogeneity (I2 = 51%, p = 0.07) for 50 mL b.i.d., respectively (Supplementary Fig. S3B).
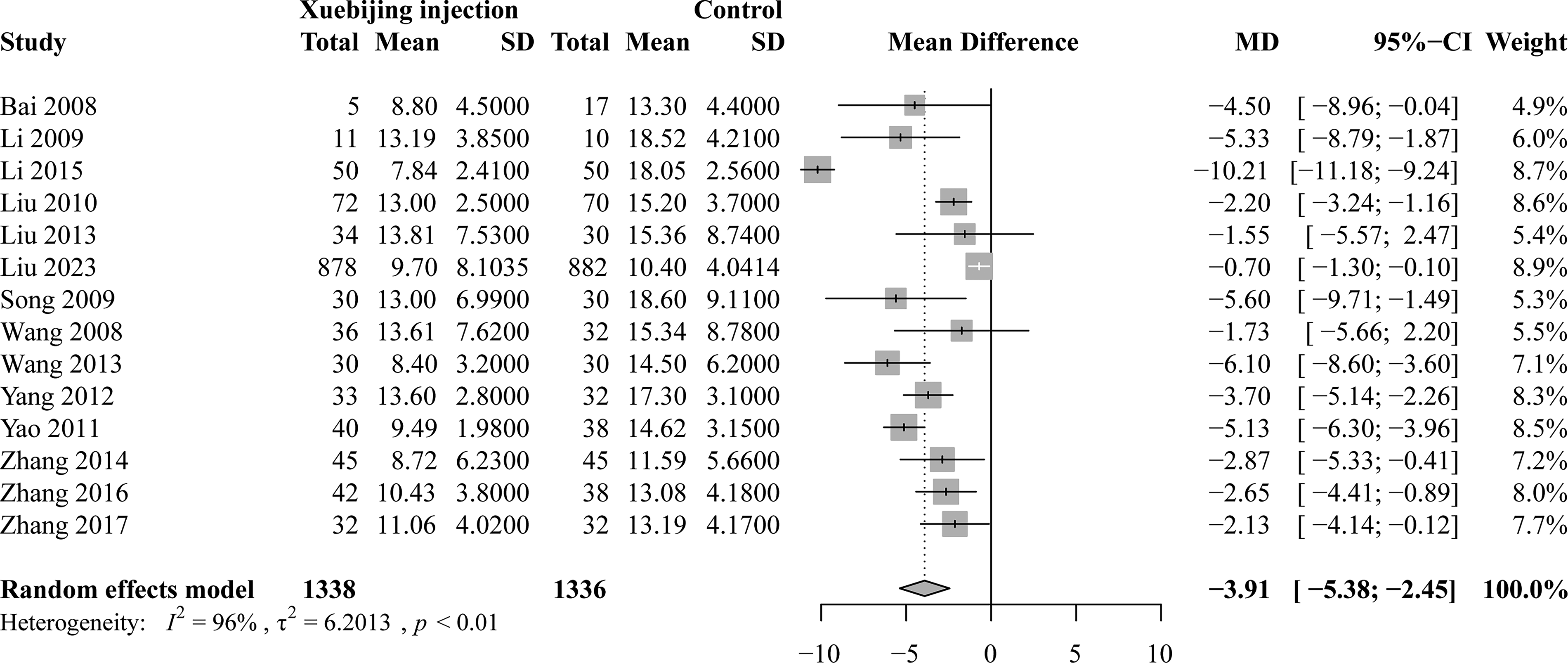
Xuebijing injection treatment compared with conventional treatment for APACHE II score.
A total three trials with 362 participants (182 participants in the Xuebijing injection group and 180 participants in the control group) reported body temperature (Supplementary Table S1) and compared with the conventional treatment alone, Xuebijing injection therapy combined with the conventional treatment decreased body temperature (mean difference = 0.43, 95% confidence interval = 0.31–0.55, p < 0.0001) with no heterogeneity (I2 = 0%, p = 0.5963) (Fig. 4).
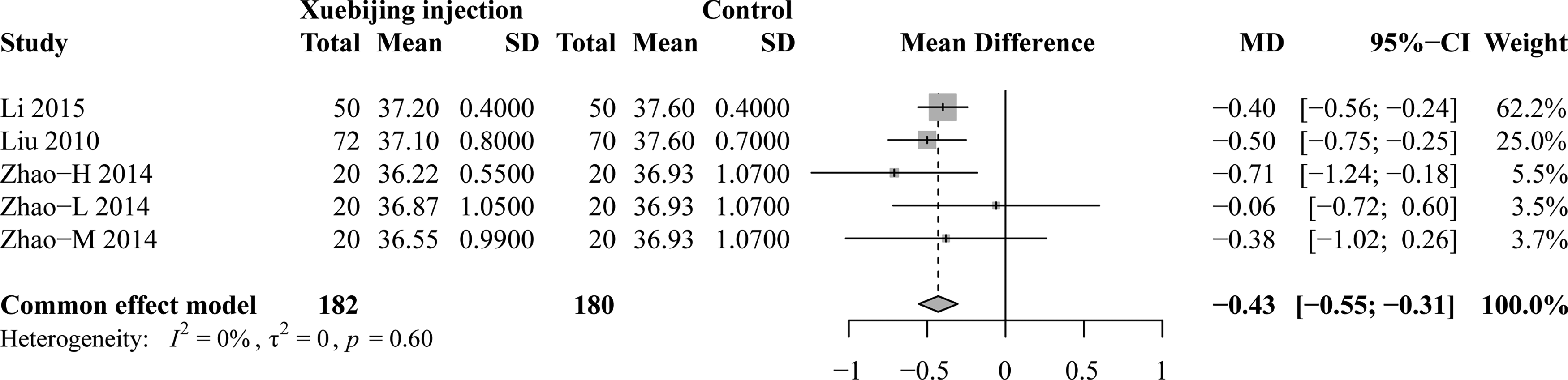
Xuebijing injection treatment compared with conventional treatment for reported body temperature.
In total, 17 trials with 2914 participants (1499 participants in the Xuebijing injection group and 1415 participants in the control group) reported adverse events or reactions (Supplementary Table S1). Compared with the conventional treatment, Xuebijing injection therapy combined with the conventional treatment mildly decreased adverse events or reactions without a statistical difference (risk ratio = 0.91, 95% confidence interval = 0.77–1.07, p = 0.2405) (Supplementary Fig. S4).
Publication bias
The funnel analysis indicated a complete symmetry in 28-day mortality (Supplementary Fig. S5), exhibiting that publication bias might not exist. Moreover, the Peters test confirmed our result (p = 0.2591). Among APACHE Ⅱ score, the funnel plot exhibited a complete symmetry (Supplementary Fig. S6). Moreover, after trim and fill, Xuebijing injection therapy combined with the conventional treatment decreased APACHE Ⅱ score by 1.54 (95% confidence interval = −0.28–3.36, p = 0.0962) compared with the conventional treatment alone (Supplementary Fig. S7). For adverse events or reactions, there was no publication bias (Supplementary Fig. S8).
Sensitivity analysis
Then the leave-one-out analysis was conducted to confirm the robustness and reliability of results for 28-day mortality (Supplementary Fig. S9), mortality during treatment (Supplementary Fig. S10), APACHE Ⅱ score (Supplementary Fig. S11), body temperature (Supplementary Fig. S12), and adverse events or reactions (Supplementary Fig. S13).
Discussion
Sepsis remains the leading cause of death in intensive care patients. Despite the use of combination antibiotics, good supportive therapy, and care, treatment for sepsis remains unsatisfactory. The results of our study revealed that Xuebijing injection combined with conventional treatment may reduce 28-day mortality, mortality during treatment, decreased APACHE Ⅱ score, and body temperature compared with conventional treatment alone (Fig. 5). Moreover, there are no obvious adverse events.
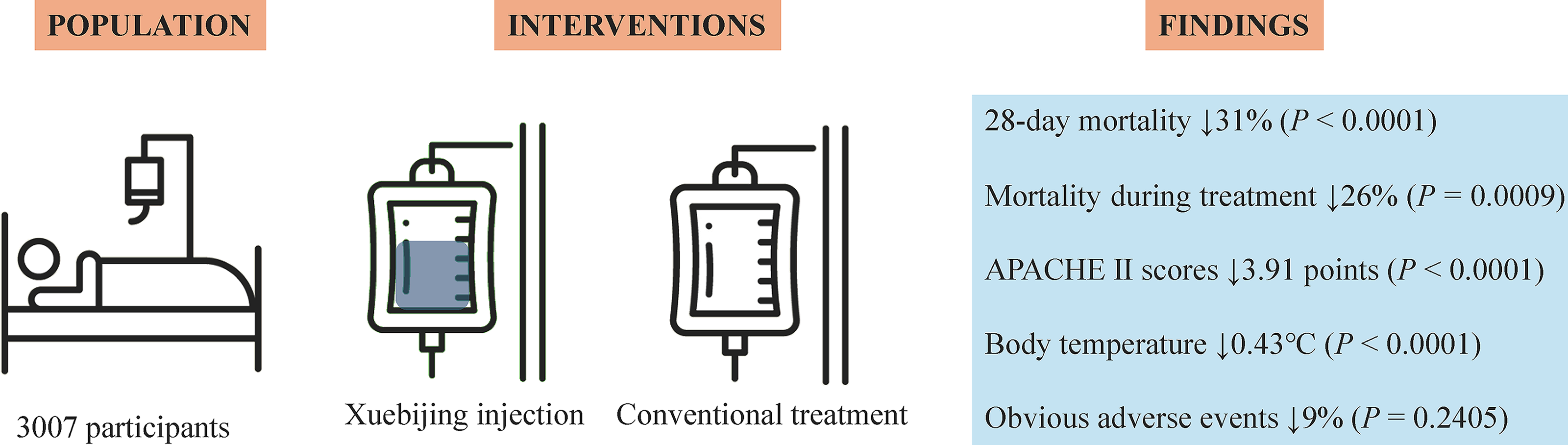
Efficacy and safety of Xuebijing injection in patients with sepsis.
The pathogenesis of sepsis includes uncontrolled inflammation, immune dysregulation, and coagulation dysfunction. 41 Pharmacological studies showed that Xuebijing injection acts as an anti-inflammatory, immune regulation, and anti-coagulation role in sepsis.8,42 Detailly, benzoyl paeoniflorin, a bioactive component of Xuebijing injection, dose-dependently inhibited the production of C-X-C motif chemokine ligand 1, tumor necrosis factor-α, and interleukin-6 in septic conditions, 43 Xuebijing injection prevented the inflammatory cytokine storm in septic mice. 44 Xuebijing injection normalized Tregs Th17 population in septic mice 44 and in patients with sepsis. 45 Xuebijing injection strongly reversed alterations in tissue-type plasminogen activator and circulating active protein C in septic rats, 46 Xuebijing injection significantly shortened thrombin time, prothrombin time, and activated partial thromboplastin time as well as improved platelets in patients with sepsis. 47 Moreover, Xuebijing injection antagonized endotoxin and protected organ damage. Xuebijing injection markedly down-regulated the synthesis and release of high mobility group box 1 and attenuated multiorgan pathological damage in septic rates. 48 Taken together, Xuebijing injection has an integrated and comprehensive regulatory effect in sepsis.
Here, we performed an updated systematic review and meta-analysis only including randomized controlled trials about Xuebijing injection for sepsis with no blinding limitation and publication language limitation and demonstrated that Xuebijing injection is effective and safe for patients with sepsis. Our results are acceptable because of no heterogeneity, except for the secondary outcome of APACHE Ⅱ score. We conducted subgroup analysis (sample size and Xuebijing injection dosage) on APACHE Ⅱ score to identify the source of heterogeneity and we found that heterogeneity might come from large sample size (more than 70) and high dosage (100 mL b.i.d.). This reminds us that we need to design more rigorous randomized controlled trials or real-world studies to re-evaluate the effectiveness and safety of different doses of Xuebijing injection for sepsis. Furthermore, the funnel analysis demonstrated there was no publication bias among various outcomes. A previous study that included 306 participants (165 participants in the Xuebijing injection group and 141 participants in the control group) found that Xuebijing injection effectively reduced the mortality among patients with sepsis. 49 A later large-scale study that included 1144 participants showed that add-on therapy with Xuebijing injection improved the 28-day mortality, body temperature, white blood cell count, and APACHE II score of patients with sepsis without serious adverse events, but Xuebijing injection did not reduce mortality during treatment. 13 In another word, the effect of Xuebijing injection on mortality during treatment is inconsistent. Here, we included 3007 participants (1551 participants in the Xuebijing injection group and 1456 participants in the control group), especially including a high-quality trial, 14 and discovered that Xuebijing injection decreased the mortality during treatment by 26%, which confirmed the recent effects of Xuebijing injection on sepsis.
There are some limitations in the present study. First, since Xuebijing injection is a kind of Traditional Chinese Medicine, all included trials were completed in China. More national and racial data may be needed for the global promotion and application of Xuebijing injection. Moreover, the overall quality of the included literature still needs to be improved, which is also an area that needs improvement in current clinical research of Traditional Chinese Medicine. Finally, we only compared the efficacy and safety of Xuebijing injection as an add-on therapy and did not pay attention to the dosage relationship of Xuebijing injection. Such as, the two included trials used different Xuebijing injection doses (50 mL b.i.d./100 mL b.i.d./100 mL q.i.d. Xuebijing injection in a trial 36 and 100 mL q12h/100 mL q8h Xuebijing injection in another trial), 40 we simply split them into different doses (five studies) during analysis. A previous clinical trial on specialized Xuebijing injection dosage showed that 50 mL b.i.d./100 mL q.i.d. Xuebijing injection improves overall treatment effectiveness, reduces APACHE II score and inflammation levels, and 100 mL q.i.d. Xuebijing injection has clearer effects. 50 Another previous research indicated that the time for onset of therapeutic effect in 100 mL q.i.d. Xuebijing injection was short and significantly reduced inflammatory cytokines levels and improved the prognosis of sepsis patients. 36 100 mL q12h/100 mL q8h Xuebijing injection significantly reduced the inflammation level, shortened the duration of blood purification and mechanical ventilation, improved the prognosis of patients with sepsis, and the effect was more obvious in the 100 mL q8h group, without affecting the safety of treatment. 40 These data demonstrate that high-dose Xuebijing injection seems to be clinically feasible. However this study did not set up a blank control group, 50 and more rigorous trials may need to be designed in the future to further elucidate the dose–response effect of Xuebijing injection while ensuring safety.
Conclusions
In conclusion, Xuebijing injection significantly decreased the 28-day mortality rate, mortality during treatment, APACHE Ⅱ score, and body temperature without adverse events or reactions.
Authors’ Contributions
B.L. and R.W. conceived, designed, or planned the idea. G.C., L.L., X.H., R.W., and B.L. collected the data. G.C., L.L., and X.H. analyzed the data. B.L. and R.W. interpreted the data. G.C. drafted the article. B.L. and R.W. revised the article. All authors read and approved the final article.
Footnotes
Acknowledgment
The authors thank all participants and researchers involved in Xuebijing injection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.