
Abstract
Introduction:
Chronic pain is a prevalent condition in the United States, and multimodal treatment approaches are the hallmark of management. Yoga therapy is a targeted, systematic approach for treating patients with specific conditions, using focused breathing and relaxation techniques. The purpose of this observational study was to evaluate the impact of yoga therapy on periprocedural pain, anxiety, and satisfaction in patients with chronic pain undergoing interventional procedures.
Materials and Methods:
A total of 36 voluntary subjects participated in this prospective study. Nineteen had a yoga therapist guide them through periprocedural yoga therapy techniques, and 17 underwent the procedure without a yoga therapist. Periprocedural vital signs and pre- and postsurvey responses relating to patient-reported severity of pain, anxiety, and satisfaction were collected and compared between the two groups.
Results:
The mean difference in Visual Facial Anxiety Scale anxiety rating of patients receiving yoga therapy was 1.12 (95% confidence interval [CI]: −2.11 to −0.12, p = 0.029) points lower than that of patients without therapy. The mean difference in Numeric Rating Scale-10 pain score of patients receiving yoga therapy was 1.93 (95% CI: −3.78 to −0.07, p = 0.042) points lower than that of patients without therapy, controlling for procedural sedation. There were no significant differences in vital signs or overall patient satisfaction (Patient Global Impression of Change-7) following the procedure.
Discussion:
In patients with chronic pain undergoing interventional procedures, participation in yoga therapy may be associated with a significant reduction in periprocedural anxiety and pain. Further investigation through a randomized controlled trial is necessary to verify these preliminary findings.
Conclusion:
Yoga therapy may be considered in a multimodal approach to perioperative pain and anxiety management.
Introduction
Background
Chronic pain is one of the most prevalent chronic conditions in the United States, and one of the most common reasons adults seek medical care. 1 Its importance cannot be understated, both in terms of its economic cost as well as its morbidity, with links to restrictions in activities of daily living, depression, dependence on opioids, and reduced perception of quality of life. 1 Multimodal treatment approaches are the hallmark of both acute and chronic pain management. 2 While pain management includes conventional medical modalities, such as medication and interventional pain procedures, nonpharmacological modalities are increasingly important in the management of chronic pain. 2 Nevertheless, interventional pain procedures, such as nerve blocks, ablations, and steroid injections, comprise a significant and effective aspect of treatment options for people living with chronic pain. 3
Perioperative and periprocedural anxiety has been associated with a variety of negative clinical outcomes that can have adverse effects on recovery and healing. Anxiety has been shown to significantly impair patients’ sense of well-being, hindering cooperation with self-care activities and ongoing self-management of pain. In addition, anxiety may adversely contribute to emotional uncertainty, loss of control, decreased self-esteem, and anticipation of increased pain. 4 Physical problems impacted by periprocedural patient anxiety not only include refractory postoperative pain and dissatisfaction with surgery but also issues that slow wound healing, such as elevated blood pressure, elevated cortisol levels, decreased immune response, and increased risk of infection.5,6 As such, intravenous sedatives are often used in the periprocedural setting. Although sedation can calm the patient, this is not without additional risk. Depending on the sedative used, patients may require longer postoperative recovery time and are more prone to risks such as respiratory depression, risk of aspiration, loss of airway, hypotension, disinhibition, and cardiac suppression. 7 Sedative effects are temporary by design and limited to when the sedative agent was administered; intravenous sedation confers neither long-term anxiolysis nor increased patient self-management of their symptoms.
Yoga therapy is a targeted and systematic approach for treating patients with specific conditions, using focused breathing, relaxation techniques, and meditation. Movement, while not generally applied in the periprocedural environments, may also be introduced on a small and modified basis. Yoga therapists are certified yoga instructors who have completed postgraduate coursework on the underlying physiology of various disease states, taught by physicians and other specialists in the field, and understand how to use breathing, meditation, and limited movement to treat patients with specific medical conditions. There is a breadth of evidence indicating the effectiveness of yoga therapy on breast cancer; improvements in sleep, fatigue, and cognition; as well as improvements in biomarkers of stress, inflammation, and immune function.8–10 There have been studies showing the benefit of yoga therapy and other comparable mindfulness and breathing exercises in certain periprocedural settings.11–13 However, there are limited data that evaluate the use of yoga therapy specifically in the acute, intraprocedural setting of patients who are being treated for chronic pain.14,15 Longitudinal mindfulness, yoga, and breathing modules have shown some promise in improving awareness and psychological perception of pain among patients with chronic, nonmalignant pain, though pain intensity ratings and use of opioid medications have been similar across groups in prior studies.2,16–19 Patients with chronic pain often have elevated anxiety and negative perceptions about their upcoming procedures, sometimes due to previous experiences when procedures were painful and/or ineffective.18–20 Pharmacological sedation is used more frequently for periprocedural anxiety in this patient population but also carries risk, requires the patient to be nothing by mouth prior to the procedure, precludes them from operating a motor vehicle after the procedure, and does not confer any long-term self-efficacy for symptom management. 20
Objectives
The purpose of this observational study was to evaluate the impact of yoga therapy on pain, anxiety, hemodynamics, and patient satisfaction when undergoing interventional pain procedures. It was hypothesized that patients undergoing periprocedural yoga therapy would demonstrate decreased pain and anxiety scores, as well as increased overall satisfaction with their procedure.
Materials and Methods
Design, setting, and participants
This was a prospective, observational, pilot study. Inclusion criteria consisted of patients scheduled for any interventional pain procedure to treat their chronic pain at two Henry Ford Health pain clinics in Royal Oak, Michigan, and Dearborn, Michigan, between March 31 and May 16, 2023. Patients were excluded if they were unable to complete the survey, were non-English speakers, or were unwilling to provide consent for this study. Informed consent was obtained from all patients involved in the study.
Yoga therapy is available to all patients scheduled for interventional pain procedures at the Royal Oak and Dearborn pain clinics twice a week on a predetermined schedule based on the availability of trained yoga therapists. The first group of patients included in this study consisted of patients seen in the clinic on days when yoga therapy was not offered. These patients received standard-of-care treatment, including intravenous sedation when applicable. The second group of patients was scheduled on a day when yoga therapists were available in the clinic and agreed to have a yoga therapist guide them before, during, and after their interventional procedure to treat their chronic pain. Participation in yoga therapy at these clinics is free, voluntary, and in no way changes the care that patients otherwise receive. Patients who elect to have yoga therapy are not excluded from also receiving intravenous sedation if eligible. All procedures are performed by two interventional pain specialists familiar with working with the yoga therapists.
Each yoga therapist follows the guidelines set forth by the International Institute of Yoga Therapy (IIYT) while guiding each patient before, during, and after their procedure. The continuous intervention began in the preoperative holding area for approximately 10 min, and the yoga therapists accompanied patients into the procedure suite and then into the recovery area for an additional 5 min. As part of their standard practice, the yoga therapists document their activities with the patients. The yoga therapy clinical coordinator oversees the therapy provided to ensure consistency and appropriateness through the use of a fidelity checklist. In this setting, yoga therapy primarily consists of focused breathwork and guided relaxation techniques rather than movement exercises. Patients were coached to focus on each of their breaths and concentrate on individual parts of their body when beginning the intervention, and this continued throughout their procedure. During the actual procedure, the study participants continued these breathing exercises and other relaxation techniques at the discretion of yoga therapists. They were also asked beforehand what may have been causing their procedural anxiety, if applicable, and asked to reflect on it postoperatively while concluding the intervention.
Variables, data sources, and bias
This prospective observational study was approved by the Institutional Review Board of Henry Ford Health System on March 16, 2023 (IRB# 16272). Primary sources of data that were later analyzed include electronic health record data from study subjects as well as survey responses. Data collected from the patients included their responses to a questionnaire that was administered both pre- and postprocedurally, as well as information about their procedure (date, type, administration of intravenous sedatives/analgesics, provider name), demographics (age, gender, race), and periprocedural vital signs (blood pressure, heart rate, respiratory rate, oxygen saturation) from the electronic medical record. The questionnaires were administered solely on the day of the procedure, both pre- and postprocedurally. Preintervention data were collected before the yoga therapists met any of the participants, and postintervention results were collected following the conclusion of yoga therapy in the recovery area. The questionnaires included the Patient Global Impression of Change (PGIC-7) scale assessing overall satisfaction, patients’ pre- and postprocedural Numeric Rating Scale (NRS-10) pain scores, and patients’ pre- and postprocedural Visual Facial Anxiety Scale (VFAS).21–23 Patients were also asked if they had ever received yoga therapy at a Henry Ford Health facility before the date of their scheduled procedure. Vital sign measurements consisted of one set of preoperative vitals, one set of intraprocedural vitals (taken closest to the middle of their procedure based on the length of time), and the first set of postprocedure vitals. The primary outcome of interest was the difference in patients’ pain scores based on the validated NRS-10, ranging from 0 (no pain) to 10 (worst imaginable pain). Secondary outcomes included anxiety based on patients’ VFAS scores and overall satisfaction based on PGIC-7 scores. Outcome assessors were blinded to the intervention arm of the participants, including all self-reported survey data as well as vital signs.
Study size and statistical methods
All data were de-identified prior to analysis. Assuming an effect size of 1, it was determined that each study group would need at least 17 subjects to detect a difference with 80% power using an alpha of 0.05 and two-sided testing, based on the primary outcome of interest and a priori power analysis. Initial descriptive statistics were presented with mean and standard deviation for continuous variables and counts and percentages for categorical variables. For group comparisons, the Wilcox rank-sum test was conducted for continuous variables, the chi-square test of independence for categorical variables, or Fisher’s exact test (*) when conditions were not met. Univariate and multivariate linear regression models were fit to examine the association between yoga therapy and the difference in pre- and postprocedural outcomes. The former included only yoga therapy as the dependent variable, and the latter further adjusted for intravenous sedation. All statistical tests were two-sided with an α (significance) level of 0.05. All data were analyzed using R version 4.1.2.
Results
A total of 36 study subjects were enrolled in the study, of which 19 (52.7%) received yoga therapy, and 17 (47.3%) did not receive yoga therapy (Table 1). The types of procedures patients in both groups underwent included medial branch blocks in both the cervical and lumbar spine, radiofrequency ablations in both the cervical and lumbar spine, epidural steroid injections in both the cervical and lumbar spine, intra-articular and bursal steroid injections throughout the lower extremities, and spinal cord stimulator implant trials. There was no missing data from any participants. Intention-to-treat analysis was performed on the collected data. When comparing these two groups of patients, there were significant differences in the change in anxiety and pain ratings, but not in vital signs (Tables 2 and 3, and Supplementary Table S1).
Patient Characteristics
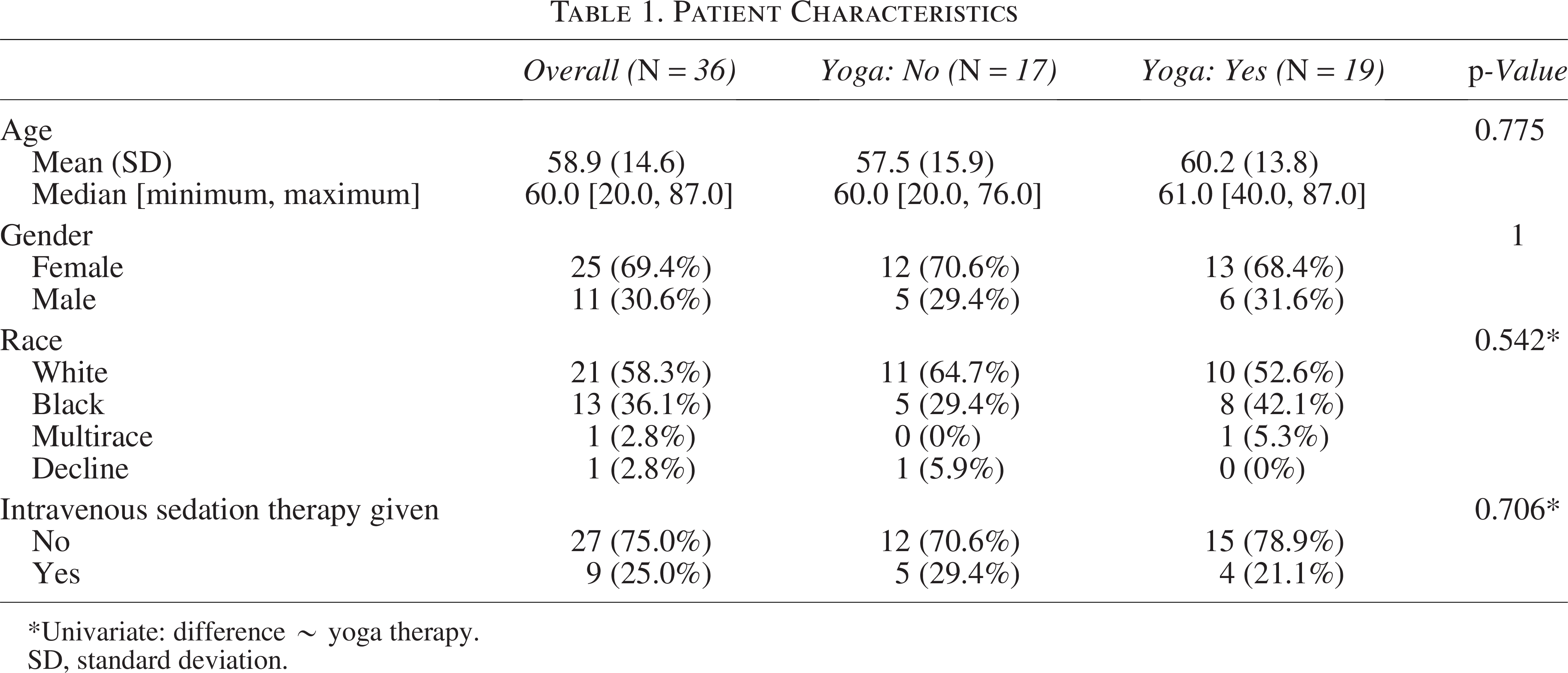
Univariate: difference ∼ yoga therapy.
SD, standard deviation.
Patient Survey Scores
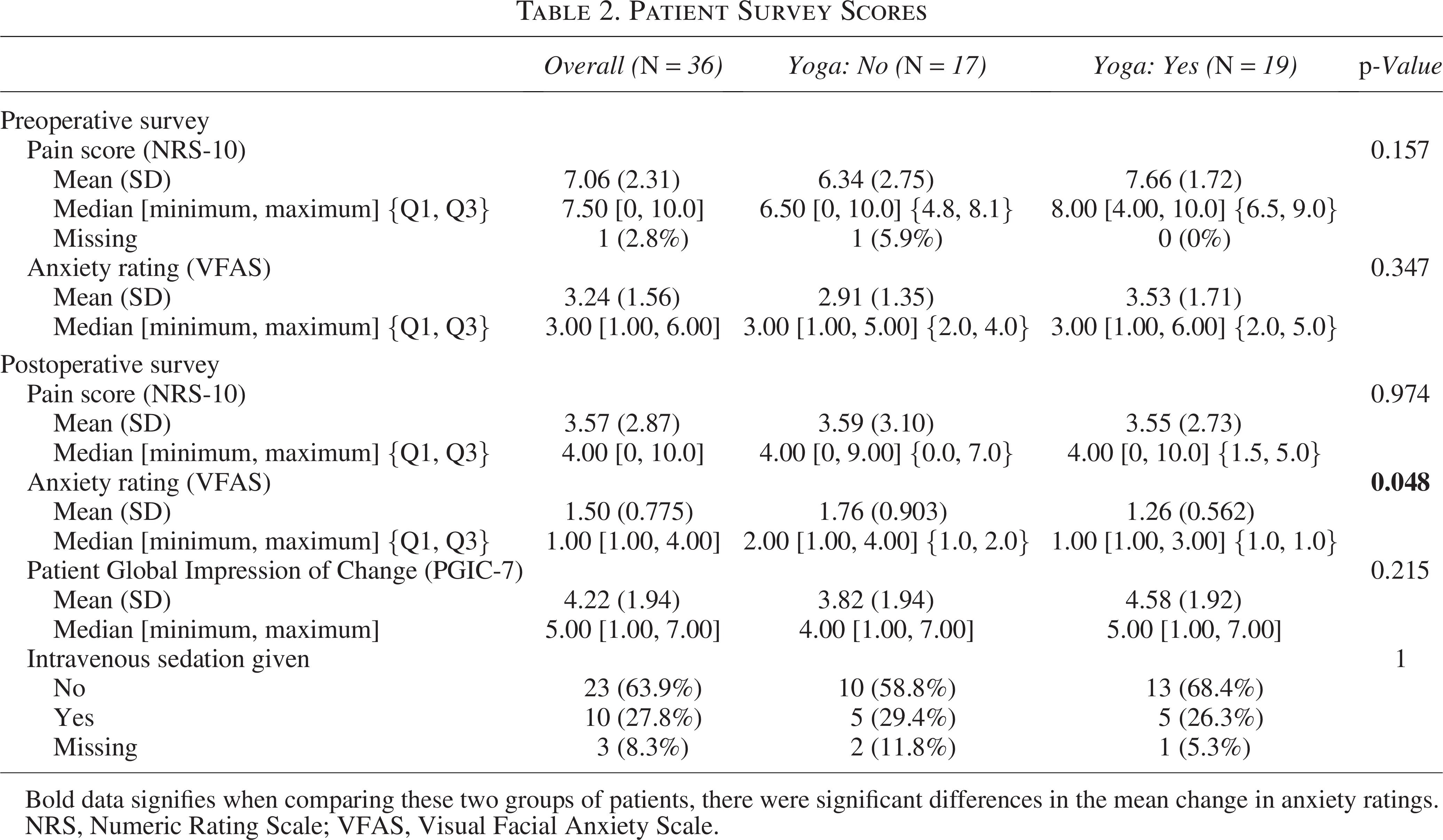
Bold data signifies when comparing these two groups of patients, there were significant differences in the mean change in anxiety ratings.
NRS, Numeric Rating Scale; VFAS, Visual Facial Anxiety Scale.
Net Change of Pre- and Postprocedural Survey Scores
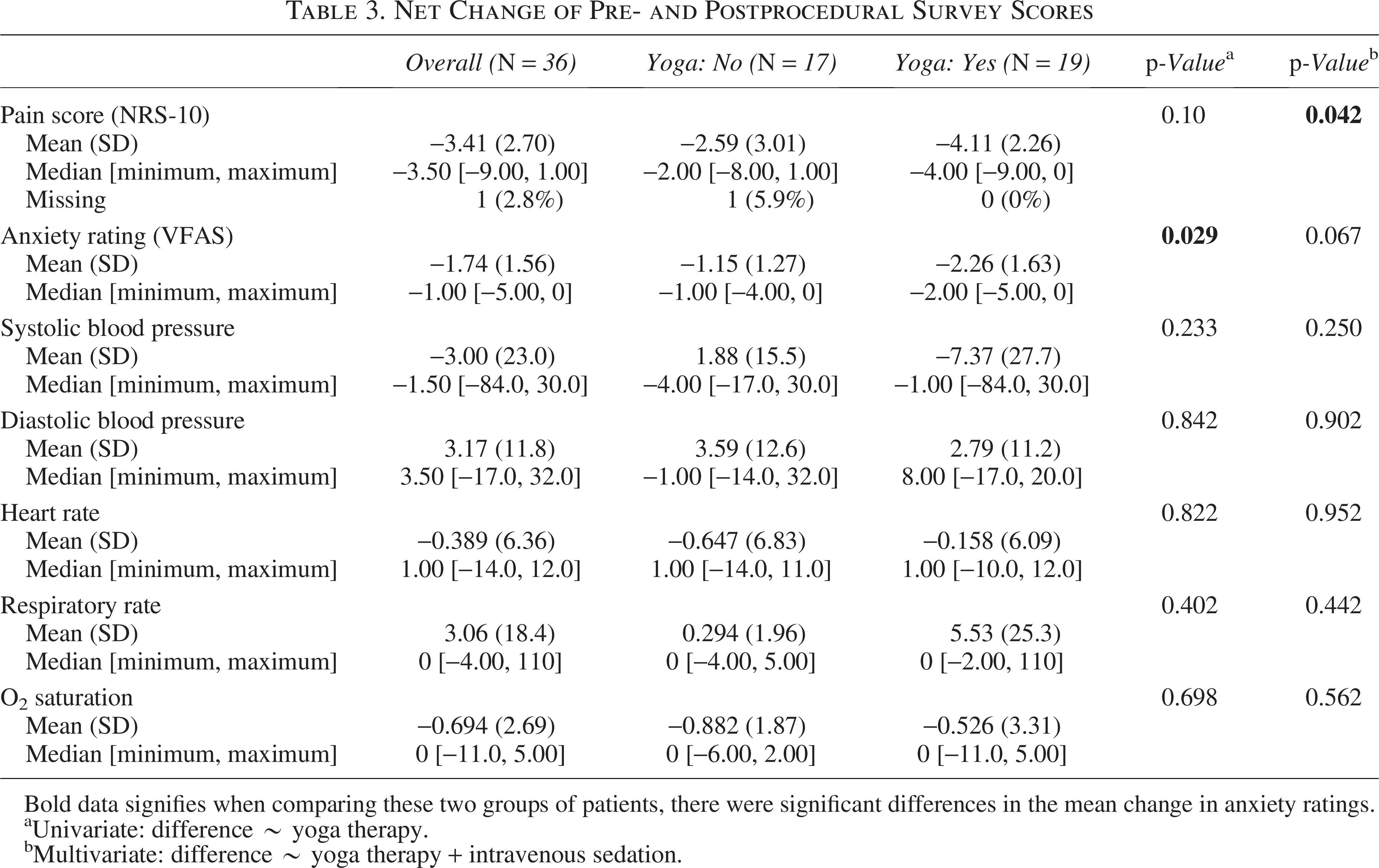
Bold data signifies when comparing these two groups of patients, there were significant differences in the mean change in anxiety ratings.
Univariate: difference ∼ yoga therapy.
Multivariate: difference ∼ yoga therapy + intravenous sedation.
The postsurvey anxiety ratings of patients who received yoga therapy were significantly lower in patients who received yoga therapy than those who did not (p = 0.048, Table 2). When comparing the change in pre- and postoperative anxiety ratings, patients who received yoga therapy had a significantly larger decrease in anxiety than patients without therapy (95% confidence interval [CI]: −2.11 to −0.12, p = 0.029, Table 3).
There was not a significant difference in the postsurvey pain scores for patients who received yoga therapy and patients without yoga therapy (p = 0.974, Table 2). However, when comparing the average difference in pre- and postoperative pain scores, patients who received yoga therapy had a larger decrease in pain than those who did not receive yoga therapy (95% CI: −3.78 to −0.07, p = 0.042, Table 3). It is important to note that the effect of intravenous sedation was controlled for in these calculations.
There were no significant differences in the mean or median pre-, intra-, or postprocedural vital signs (blood pressure, heart rate, respiratory rate, or oxygen saturation) between the two groups, based on both univariate and multivariate analyses (Supplementary Table S1). There was no difference in overall satisfaction between the two groups of patients, based on the PGIC-7 scores collected postprocedure (p = 0.215). The sample size was not adequate to determine the effect of demographic variables, such as gender, age, or race on pain, anxiety, or satisfaction in patients who received yoga therapy.
Discussion
This prospective observational study compared the self-reported anxiety, pain, and satisfaction levels in adults undergoing interventional procedures for chronic pain with the guidance of a yoga therapist periprocedurally with those of patients who did not receive yoga therapy. The use of yoga therapy was associated with a greater decrease in self-reported pain (NRS-10, p = 0.042) and anxiety (VFAS, p = 0.029) when comparing the difference in pre- and postprocedure ratings. Postoperative anxiety ratings of patients who received yoga therapy were significantly lower than those who did not receive yoga therapy (p = 0.048). There was no significant difference in the patients’ overall satisfaction following the procedure or in any of the vital signs collected. Prior studies have shown no difference in pain intensity ratings in patients undergoing longitudinal mindfulness, yoga, and breathing modules, although improvements in the psychological perception of pain have been observed.2,16–20 Our study is novel in that it focused on pain only in the acute, perioperative setting, rather than chronically.
Periprocedural patient anxiety has been linked to many other underlying psychological and physical manifestations that can affect the technical success of a procedure, as well as patient satisfaction.4–6 Yoga therapy may provide an integrative and novel modality to other commonly used anxiolytics, such as intravenous midazolam, in helping patients during the periprocedural period and beyond to find ways to combat elevated anxiety levels and negative perceptions about procedures.5,6 Through the focused breathing and mindfulness exercises as described in previous studies and similarly applied in this study, yoga therapy may impact the psychological perception of pain and allow patients to engage in self-management of their pain, rather than relying on external sources, such as medication, to mitigate the distressing symptoms of pain and anxiety.
Patients having to manage chronic pain may benefit from psychotherapy and other nonpharmacological approaches that may prove to be more helpful in reducing stress, anxiety, and pain perception.16,24 The exercises that patients learn from yoga therapists may be extended outside of the perioperative setting into their daily lives to help with long-term anxiety management. Furthermore, mindfulness training in the acute setting may be able to reduce the need for opioids in patients with intolerable pain levels. This may help lead to an overall reduction in perceived pain levels and patients’ desire for opioids for chronic pain management.25,26 This pilot study focused on the acute benefits of yoga therapy in the periprocedural setting and lacks follow-up data from clinic visits postoperatively. Future studies surveying the long-lasting effects of exposure to yoga therapy in the acute, interventional setting may be of interest in examining the durability of these findings in stress, anxiety, and pain reduction.
There were a few limitations in the design of this study. It is possible that there was selection bias for the group of patients who did receive yoga therapy, as they were given the choice of whether they wanted to receive the yoga therapy or not. Only those who made the choice to receive yoga therapy were included in the study. It is possible that they had a preconceived notion that yoga therapy would be beneficial for their anxiety and pain or were more open to receiving such complementary therapies in the first place. Therefore, these biases may have influenced survey results both pre- and postprocedurally from some patients. Furthermore, patients often receive local anesthesia at the site of the procedure that may affect their pain levels in the immediate postoperative period, thus impacting their perception of pain. A major inherent challenge of most pain research is that pain levels can be notably subjective, producing variability even when validated rating tools like the NRS-10 are used. In addition, this study did not account for other comorbid conditions of patients or the length of procedure when comparing pre-, intra-, and postprocedural vital sign measurements. Both factors can influence periprocedural vital signs and should be incorporated in future analyses. The participants in the study were primarily female, though with no statistically significant difference between genders on analysis. The participants were also from two clinics within one health system. The analysis also included a small sample size (n = 36), which does reduce the statistical power in interpreting the results and generalizing them to a larger population, especially when performing subgroup analysis. We did not register this observational study in a public trial registry, given its nature as a pilot study with a small sample size, but prior to enrolling patients, the authors obtained Institutional Review Board approval, and patients provided informed consent to participate. A larger sample in a more formal randomized controlled trial is needed to evaluate the potential influence of patient demographics and other potentially confounding variables following this prospective, observational single-institution pilot study.
There are a few other considerations for future work in this field. Managing the psychological components of pain and anxiety in the perioperative setting is multifaceted, and interventions like yoga therapy demand some level of “buy-in” from the patient. Studies have shown that patients’ perceived treatment helpfulness has a significant effect on treatment outcomes. 27 Patients who had otherwise participated in yoga therapy outside of this clinical context may have been a confounding variable in interpreting the results of this study. Another factor to consider is the clinical feasibility of having yoga therapists involved in the perioperative pathway. Maintaining the workflow of a surgical center to ensure patients are seen on schedule is vital, and busy clinical practices may be deterred from adding another step to the patient experience. However, this needs to be weighed with the significant potential benefits for patients in decreasing their pain and anxiety levels, increasing their overall satisfaction, and improving outcomes. 28 Combining anxiolytic modalities to improve patient anxiety scores and procedure satisfaction can be a focus of future studies in this arena. For example, other studies have shown that aromatherapy improves patient satisfaction and decreases the need for intraoperative anxiolytics in awake patients undergoing procedures like cesarean section under spinal anesthesia, as well as interventional spine procedures, such as the ones the subjects in this study underwent.29,30
Conclusions
This study suggests that periprocedural yoga therapy may be associated with a greater decrease in anxiety and pain ratings following interventional pain management procedures like epidural steroid injections and radiofrequency ablations, and no differences in periprocedural vital signs or overall patient satisfaction, as compared to interventional procedures taking place without periprocedural yoga therapy. Further studies are needed to analyze not only the reduction in immediate postoperative pain and anxiety but also the long-term effects of periprocedural yoga therapy, as well as evaluate the influence of other factors, including patient comorbidities, on the efficacy of this therapy. Confirmation of this study’s findings through a proper randomized controlled trial is essential in verifying the role of yoga therapy in the periprocedural context.
Authors’ Contributions
Y.M.S.: Methodology, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, and visualization. L.Z.: Conceptualization, methodology, validation, formal analysis, investigation, resources, writing—review and editing, supervision, project administration, and funding acquisition. S.M., V.Z., R.H., N.S., and C.E.G.-L.: Resources and writing—review and editing. K.N.: Software, formal analysis, resources, data curation, writing—review and editing, and visualization.
Footnotes
Acknowledgments
The authors of this article would like to express their gratitude to each of the yoga therapists from the IIYT who made this study possible. Their assistance has significantly contributed to the success of this endeavor and is dearly appreciated.
Author Disclosure Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Support was provided solely from institutional and/or departmental sources. The authors declare no competing interests.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.